Embed Size (px)
DESCRIPTION
A brief description of the Brazilian Lung Cancer status and an update on new procedures in Thoracic Surgery
Citation preview

“Estado Atual, da Arte e dos Ânimos”
Grupo Paulistano de Apoio ao Tratamento do Câncer de Pulmão
Instituto Brasileiro de Cancerologia Torácica (IBCT)Instituto Paulista de Cancerologia (IPC)
Instituto TóraxCentro de Cirurgia Torácica Minimamente Invasiva (CTMI)
Dr. Ricardo Sales dos SantosCoordenador, Centro de Cirurgia Torácica Minimamente Invasiva
Hospital Israelita Albert Einstein
Maio, 2010

Albert Einstein Jewish Hospital
Research & Education Institute
Social Responsability Institute
Diagnostic & Preventive Medicine

ONCOLOGY

INTERVENÇÃO CARDIOTORÁCICA MINIMAMENTE INVASIVA
Intervenção Cardiovascular
Percutânea
Cirurgia Cardíaca Minimamente
InvasivaDr. Marco Perin Dr. Robinson Poffo
Cirurgia Torácica Minimamente
InvasivaDr. Ricardo Santos
•CARDIOLOGIA INTERVENCIONISTA Intervenção Coronária percutânea Implante de Valva Aórtica Correções de Cardiopatias congênitas Implante de Dispositivos de Assistência Circulatória (Impella)
CENTRO DE ARRITMIA CARDÍACA Tratamento de Arritmias (Centro de Arritmia)
• Cirurgia Cardíaca Robótica Cirurgia vídeo-assistida - Troca valvar - Revascularização miocárdica - Correção de Cardiopatia congênitas - Tratamento de FA
•Cirurgia Torácica Video-Assistida (VATS) & Robótica (RATS) nas doenças do mediastino, pulmao e esofago
Terapia oncologica ablativa por via endoscopica ou percutanea guiada por imagem
Endoscopia respiratoria e digestiva intervencionista (Stent, laser, crioterapia)
Cirurgia estereotactica (Cyberknife)
Procedimentos multidisciplinares
•TERAPIAS COMBINADAS Revascularização do miocárdio Tratamento combinado de FA

1 - To present the big picture 2 - Deficiency of equipment 3 - Lack of multidisciplinary approach
– Conflict of interest among specialties?4 - Delay on the diagnosis of cancer
– Mistreatment is also related to the high incidence of tuberculosis
Challenges for the Brazilian Thoracic Oncologists

1 -To present the big picture
Challenges for the Brazilian Thoracic Oncologists

Population Economy 1 China 1,338,612,968
2 India 1,166,079,217
3 European Union 491,582,852 4 United States 307,212,123.
5 Indonesia 240,271,522
6 Brazil 198,739,269
7 Pakistan 176,242,949
8 Bangladesh 156,050,883
9 Nigeria 149,229,090
10 Russia 140,041,247
11 Japan 127,078,679
12 Mexico 111,211,789
https://www.cia.gov/library/publications/the-world-factbook/geos/br.html
1 European Union $ 14,910,000,000,000
2 United States $ 14,260,000,000,000
3 China $ 7,973,000,000,000
4 Japan $ 4,329,000,000,000. 5 India $ 3,297,000,000,000
6 Germany $ 2,918,000,000,000
7 Russia $ 2,266,000,000,000 8 United Kingdom $ 2,226,000,000,000
9 France $ 2,128,000,000,000
10 Brazil $ 1,993,000,000,000
12 Mexico $ 1, 563,000,000,000
24 Argentina $ 573,900,000,000
World Economy

Thoracic Oncology
• Early detection– Expensive– Less effective than prevention
- Tobacco control - Comprehensive programs and policies to reduce
tobacco consumption.

Tobacco use

Global Warming
• 1.3 billion of smokers• 80 % living in under developing countries• Every day , there are 100,000 new smokers
worldwide

Tobacco use – USA • In the United States, an estimated 25.6 million men (25.2 percent) and 22.6 million women
(20.7 percent) are smokers. These people are at higher risk of heart attack and stroke. The latest estimates for persons age 18 and older show...
• Among whites, 25.1 percent of men and 21.7 percent of women smoke
• Among black or African Americans, 27.6 percent of men and 18.0 percent of women smoke
• Among Hispanics/Latinos, 23.2 percent of men and 12.5 percent of women smoke
• Among Asians (only), 21.3 percent of men and 6.9 percent of women smoke
• Among American Indians/Alaska Natives (only), 32.0 percent of men and 36.9 percent of women smoke
• Studies show that smoking prevalence is higher among those with 9-11 years of education (35.4 percent) compared with those with more than 16 years of education (11.6 percent).
• It's highest among persons living below the poverty level (33.3 percent).

Tobacco use – Brazil
Tobacco prevalence in 15 Brazilian Capitals
MenWomen

Lung Cancer - Massachusetts

Lung Cancer in Brazil by region(Rates per 100,000)
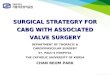
Incidence of cancer – Brazil 2008

Challenge – understand the differences
• Smoking • USA – 20 to 30 % Brazil
– same
• Cancer • USA – 215,000 new
cases• Brazil – less than 25,000
new cases/year
Population in Brazil is about 2/3 US population
Official lung CA in Brazil is near 10% of US cases

Lung Cancer in Brazil
SEXO
68%
32%
Masculino Feminino

Lung Cancer in Brazil
31 23
38 196
133 498
259
670
262
531
214
12154
51
<30 30-39 40-49 50-59 60-69 70-79 80-89 > 89
FAIXA ETÁRIA - MASCULINO E FEMININO
F
M
3009 patients from January 2000 to December 2007 – One major cancer center

Lung Cancer in Brazil
772 227502 306
37 46217 139
15 1048 18
414 1938828 12
8 1
CEC
ADENO CBA
IPC /CARCINÓIDES
INDETERMINADO
OUTROS
TIPO HISTOLÓGICO
M
F
•3009 patients from January 2000 to December 2007 – One major cancer center•Squamous cell is still more frequent than adenocarcinoma; •High incidence of undetermined NSCLC
Courtey Dr José Pereira

Courtesy from Dr Jose Pereira.
Lung Cancer in Brazil
> 20 % were classified as undetermined NSCLC, further evaluation after this study was completed

Lung Cancer in BrazilHow about Staging ?
Courtesy from Dr Jose Rodrigues Pereira
I/IIIII
IV

Showing respect to the cop

Treatment and survival
564 patients with Stage IV NSCLC

Survival Stage IV
• Median survival = 8.3 months
• 1 year survival = 37 %

• 47 types of chemotherapy combination in 4 institutes
• Media # cycles = 4• Almost 30% received 3
drugs • 83.5% cisplatinum /
Carbotaxol564 patients with Stage IV NSCLC


2 - Deficiency of equipment
– What is going on in Minimally Invasive Thoracic Surgery ?– Is it important ? – At least we hope so...
Challenges for the Brazilian Thoracic Oncologists

Deficiency of equipment
• Assessment of technology • Cost effectiveness analysis• When and how to implement

3 - Lack of multidisciplinary (MD) approach- Small number of hospitals with tumor board- Resistance “to share” patient care ?– Why is MD important ?
Challenges for the Brazilian Thoracic Oncologists
Lack of multidisciplinary approach


4 - Delay on the diagnosis of cancer
Challenges for the Brazilian Thoracic Oncologists

Lung Cancer in Brazil
Delay on the diagnosis of cancer– Is mistreatment also related to the high incidence of
tuberculosis ? • It is not uncommon for Cancer patients to receive Tb
drugs. Is it true ?
–Is the delay related to Medical education or related to the health system?

Instituto Israelita de Responsabilidade Social

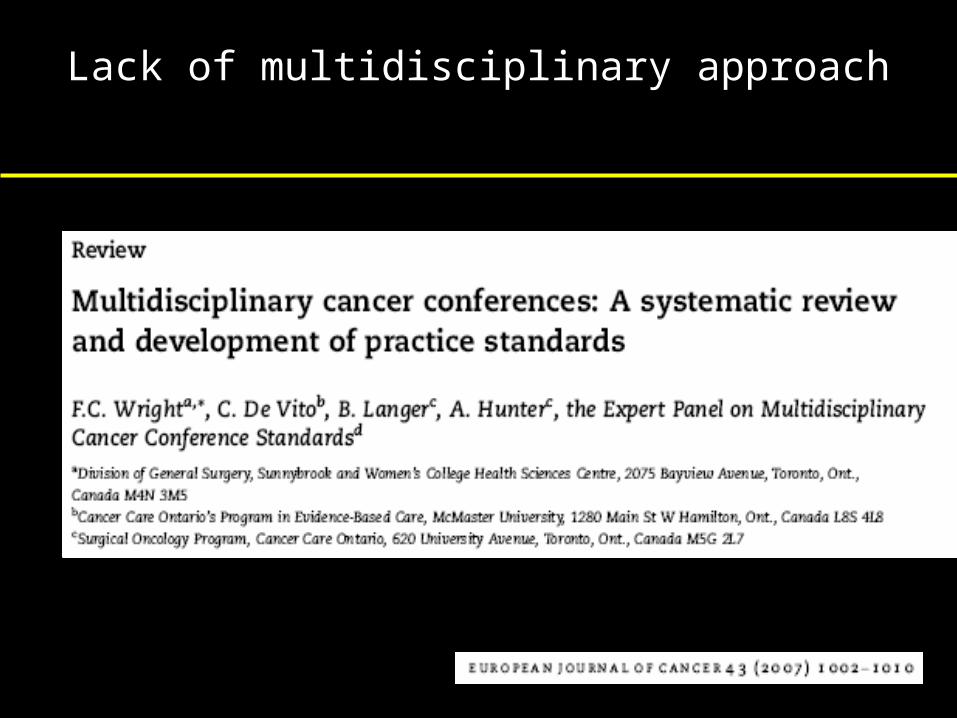
EXCESSIVA DEMORA NO DIAGNÓSTICO CLÍNICO DO CÂNCER DE PULMÃO. DEPENDE DO MÉDICO, DO PACIENTE OU DO SISTEMA?
Mariana Lista, Fernanda C. Bes, José Rodrigues Pereira, Flora Kazumi Ikari, Sueli M.Nikaedo.Instituto do Câncer Arnaldo Vieira de Carvalho (ICAVC) – Santa Casa de Misericórdia de São Paulo.
São Paulo. Brasil.
• Prolonged delay of the diagnosis of Lung Cancer in Brazil.
• Is it the Patient, Physician or Health system fault ?
• Method : Prospective questionnaire applied to 372 patients treated for lung cancer at the ICAVC – Sao Paulo
EXCESSIVA DEMORA NO DIAGNÓSTICO CLÍNICO DO CÂNCER DE PULMÃO. DEPENDE DO MÉDICO, DO PACIENTE OU DO SISTEMA?
Mariana Lista, Fernanda C. Bes, José Rodrigues Pereira, Flora Kazumi Ikari, Sueli M.Nikaedo.Instituto do Câncer Arnaldo Vieira de Carvalho (ICAVC) – Santa Casa de Misericórdia de São Paulo.
São Paulo. Brasil.
0.0
10.0
20.0
30.0
40.0
% de pacientes
1 - 7 8 - 30 31 - 90 > 90
dias
Graphic 1: Delay before looking for Medical assistance
• 29 % < 1 week• 61.5% < 30 days • 81.4% < 90 days • 18.5% > 90 days
Patient’s delay
Slide Courtesy Dr Pereira – Pulmonary Oncologist

EXCESSIVA DEMORA NO DIAGNÓSTICO CLÍNICO DO CÂNCER DE PULMÃO. DEPENDE DO MÉDICO, DO PACIENTE OU DO SISTEMA?
Mariana Lista, Fernanda C. Bes, José Rodrigues Pereira, Flora Kazumi Ikari, Sueli M.Nikaedo.Instituto do Câncer Arnaldo Vieira de Carvalho (ICAVC) – Santa Casa de Misericórdia de São Paulo.
São Paulo. Brasil.
Gráfico 2: Main symptoms (n=372)
31%
13%16%8%
32% tosse
dispnéia
dor torácica
hemoptise
outros
0%
50%
100%% de
pacientes
Tosse Dispnéia Dortorácica
Hemoptise
Gráfico 7: Tempo para procura de assistência, segundo sintomas
>90 dias31 - 90 dias8 - 30 diasaté 7 dias
Cough
SOBChest Pain
Hemoptysis
Other symptoms
Cough SOB Chest Pain
Hemoptysis
Hemoptysis
Time for looking for medical assistance X symptoms

EXCESSIVA DEMORA NO DIAGNÓSTICO CLÍNICO DO CÂNCER DE PULMÃO. DEPENDE DO MÉDICO, DO PACIENTE OU DO SISTEMA?
Mariana Lista, Fernanda C. Bes, José Rodrigues Pereira, Flora Kazumi Ikari, Sueli M.Nikaedo.Instituto do Câncer Arnaldo Vieira de Carvalho (ICAVC) – Santa Casa de Misericórdia de São Paulo.
São Paulo. Brasil.
3061
47
234
050
100150200250300
nº de pacientes
particular público
tipo de serviço
Graphic 5: First consult diagnosis based on type of service: Private or Public
outros
câncer
• 79.3% received a non cancer diagnosis at the first consult
Other diagnosis
Cancer suspicious
Private Public

EXCESSIVA DEMORA NO DIAGNÓSTICO CLÍNICO DO CÂNCER DE PULMÃO. DEPENDE DO MÉDICO, DO PACIENTE OU DO SISTEMA?
Mariana Lista, Fernanda C. Bes, José Rodrigues Pereira, Flora Kazumi Ikari, Sueli M.Nikaedo.Instituto do Câncer Arnaldo Vieira de Carvalho (ICAVC) – Santa Casa de Misericórdia de São Paulo.
São Paulo. Brasil.
• 11.8% - visited one physician before the diagnosis
• 24.5 % - visited 2 physicians • 45.4% - 3 or more physicians were necessary
to obtain a diagnosis

EXCESSIVA DEMORA NO DIAGNÓSTICO CLÍNICO DO CÂNCER DE PULMÃO. DEPENDE DO MÉDICO, DO PACIENTE OU DO SISTEMA?
Mariana Lista, Fernanda C. Bes, José Rodrigues Pereira, Flora Kazumi Ikari, Sueli M.Nikaedo.Instituto do Câncer Arnaldo Vieira de Carvalho (ICAVC) – Santa Casa de Misericórdia de São Paulo.
São Paulo. Brasil.
Gráfico 3: Primeiro diagnóstico obtido pelo paciente
7%28%
5%
10%5%
21%
12%12%
resfriado
pneumonia
bronquite
tuberculose
ortopédico
câncer
outros
sem diagnóstico
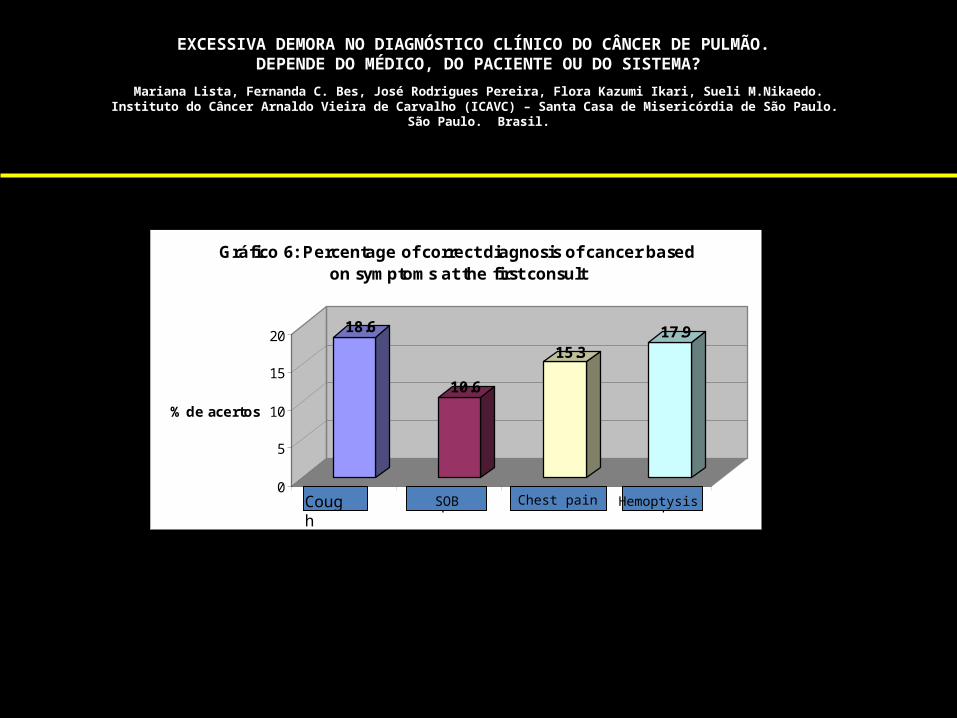
• only 20.7% suspicious for cancer at first
• 28% were treated for pneumonia
EXCESSIVA DEMORA NO DIAGNÓSTICO CLÍNICO DO CÂNCER DE PULMÃO. DEPENDE DO MÉDICO, DO PACIENTE OU DO SISTEMA?
Mariana Lista, Fernanda C. Bes, José Rodrigues Pereira, Flora Kazumi Ikari, Sueli M.Nikaedo.Instituto do Câncer Arnaldo Vieira de Carvalho (ICAVC) – Santa Casa de Misericórdia de São Paulo.
São Paulo. Brasil.
18.6
10.6
15.317.9
0
5
10
15
20
% de acertos
tosse dispnéia dor torácica hemoptise
Gráfico 6: Percentage of correct diagnosis of cancer based on symptoms at the first consult
Cough
SOB Chest pain Hemoptysis
EXCESSIVA DEMORA NO DIAGNÓSTICO CLÍNICO DO CÂNCER DE PULMÃO. DEPENDE DO MÉDICO, DO PACIENTE OU DO SISTEMA?
Mariana Lista, Fernanda C. Bes, José Rodrigues Pereira, Flora Kazumi Ikari, Sueli M.Nikaedo.Instituto do Câncer Arnaldo Vieira de Carvalho (ICAVC) – Santa Casa de Misericórdia de São Paulo.
São Paulo. Brasil.
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
% de pacientes
≤ 30 31-90 91-180 181-365 >365
dias
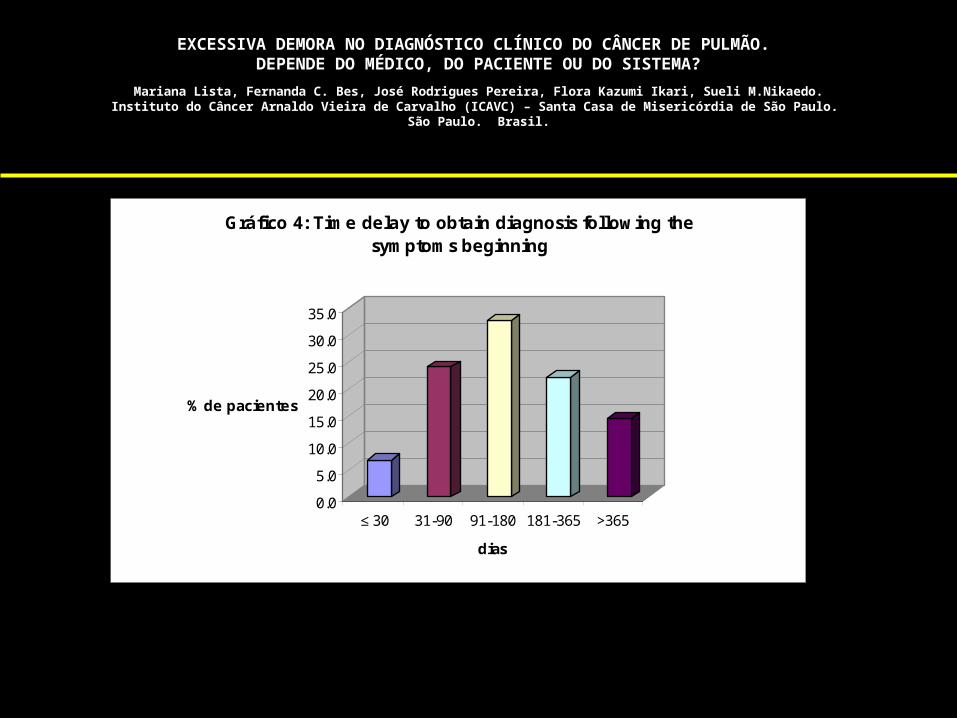
Gráfico 4: Time delay to obtain diagnosis following the symptoms beginning

CONCLUSIONS
• 80% of patients had a non neoplastic diagnosis at the fisrt consult
• 18.5% never sought medical assistance before 3 months from the onset of symptoms
• In almost 40% , diagnosis was obtained after 6 months following the onset of symptoms, which is evidence that medical practioners and/or health system play an important role contributing to this major delay.

ESTADO DA ARTE



Robótica em esôfago
MWA em pulmão
RFA em Esôfago
Robótica em pulmão
Crioterapia sp
ray
100
2736
42
126
79
128
RFA em esôfago
200
1000
Hiperidrose
10000
2295
VATS
3592
5000
Drenagem Pleural
4370
Empiema
8425
Toracotomia
16845
9087
Ablação por radiofrequência (RFA)
Cirurgia Robótica2850
723
Ablação por micro-ondas (MWA)
485
Lobectomia por VATS
423
Radiofrequência em pulmão (RFA)●
●
●
●
●
●●
●●●●
●
●
●
●
●
Procedimentos
Usuários de vanguargaÁrea de inovação
“Late adopters” Usuários comuns (alvo)
Publicações até setembro de 2009

Lobectomia video assistida

ROBÓTICA
Cirurgia Video Assistida - Robótica

Standard instrumentation Open /close and rotation only
Lobectomia video assistidaInstrumentação

Estadiamento Mediastinal

Broncoscópio com US (EBUS)
• Broncoscópio com ultrassom na extremidade
• Permite ao usuário avaliar além da parede do brônquio; vasos em tempo real.
Estadiamento Mediastinal

EBUS
Estadiamento Mediastinal

EBUS
No presente momento EBUS não substitui e sim complementa a mediastinoscopia no estadiamento mediastinal

Estadiamento Biológico
• Terapia alvo – Marcadores • ERCC1 , RRM1, BRCA 1, P53, KRAS, P27, EGFR
• Platina, Gencitabina, Erlotinibe, Cetuximab
• LACE – Lung Adjuvant Cisplatinum Trial
• ITACA – International Tailored Chemotherapy Adjuvant Trial
• TASTE – Tailored Post Surgical Therapy in Early Stage NSCLC
• SCAT – Spanish Customised Adjuvant Treatment
– Necessidade de biópsias - antes, durante ou após o tratamento
Lancet Oncol Oct, 2009; 10:1001-10

DPOC, ICC, IAM, IRA, DM , baixa reserva cardiopulmonar, etc, etc........

Diminuir a recidiva local
125 Iodine radio-active seeds into the sutures
Braquiterapia intra-operatória

Implante da Braquiterapia

Ablação pulmonar (RFA)

RF & MW Circuit Diagrams
RFAVia circuitoEletrodo passa corrente
MWASem fluxo de corrente
pelo pacienteRadiação pela antena

Ablação pulmonar - Microondas

Ablação pulmonar - Microondas
Santos et al , STS 2010, Fort Lauderdale USA

Navegação eletromagnética
Electromagnetic navigation to aid radiofrequency ablation and biopsy of lung tumors.Santos RS, Gupta A, Fernando HC et al. Ann Thorac Surg. 2010 Jan;89(1):265-8.

Ablação guiada por imagem
Electromagnetic navigation to aid radiofrequency ablation and biopsy of lung tumors.Santos RS, Gupta A, Fernando HC et al. Ann Thorac Surg. 2010 Jan;89(1):265-8.

Navegação eletromagnética
Superdimension bronchoscopy

Endoscopia Torácica Intervencionista

Centro Cirúrgico BWH - Harvard

Endoscopia Torácica Intervencionista

Pre-Treatment 6 Weeks Post-Treatment
Glottic Stricture (Web)
74 yr old female with laryngeal cancer treated with external beam radiation therapy (EBRT) Laryngoscopy demonstrated a severe, circumferential glottic web
Treatment
Currently 8-months out with no recurrent symptoms

CRIOTERAPIA ENDOBRÔNQUICA
ESTADO DOS ÂNIMOS

Building the Future

IX Curso Internacional da Sociedade Brasileira de Cancerologia Boston Medical Center
6-11 de setembro de 2010
Coordenadores– Benedict Daly, MD.
– Chrish Fernando, MD– Dr. Ricardo Antunes– Dr. Ricardo Santos– Dr. Roberto Gomes







![OSTETRICIA E GINECOLOGIA [332-368] - gomrc.it. 39 ter profilassi antibiotica in chirurgia...Soriano E, Sanchez-Lloret J. Antibiotic prophylaxis in non-cardiac thoracic surgery: cefazolin](https://img.pdfslide.tips/doc/110x75/5e0b89deaf608c5bcb2c8149/ostetricia-e-ginecologia-332-368-gomrcit-39-ter-profilassi-antibiotica-in.jpg)














![[原著]Usefulness of video-assisted thoracic surgery in the ...okinawa-repo.lib.u-ryukyu.ac.jp/bitstream/20.500.12001/3379/1/v17p… · Tomoharu Kuda*, Keiichirou Genka…, Kiyoshi](https://img.pdfslide.tips/doc/110x75/605f608883981a564e2a7c4f/eusefulness-of-video-assisted-thoracic-surgery-in-the-okinawa-repolibu-.jpg)