Embed Size (px)
Citation preview

Yonathan HasinYaakov Hasin
PCI is a good alternative to CABG in patients with HF and viable
myocardium
Conflict of interests:I am an interventional cardiologist

Rationale• Revascularization of viable myocardium may:
– Improve LV function, reverse remodeling– Improve QOL, improve survival
• Viability diagnosis– Scar (wall thickness, gadolinium)– Induced contraction– Metabolism
– Echo– PET– MRI

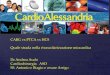
Figure 1 Diagrammatic representation of postulated progressive changes in a patient with hibernating myocardium and ( A ) no remodeling ( B ), mild to moderate remodeling ( C and D ), and end stage ( E ) of the disorder. WMA , Wal...
Harry R. Phillips , Christopher M. O'Connor , Joseph Rogers
Revascularization for heart failure
American Heart Journal, Volume 153, Issue 4, Supplement, 2007, 65 - 73
Concept of reverse remodeling

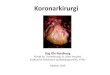
Cardiac events (cardiac death, myocardial infarction, and hospitalization for heart failure) at 3-year follow-up for four different patient categories with ischaemic left ventricular dysfunction
according to the presence of substantial viable myocardium (>4 segments) at dobutamine stress echo and the left ventricular end-systolic volume.
Lauro Cortigiani et al. Eur Heart J Cardiovasc Imaging 2012;13:219-226

Results of two meta-analysis on 3088 and 2217 patients with ischaemic cardiomyopathy, respectively, assessing the effect of revascularization and medical therapy according to the
presence or absence of viability at dobutamine stress echo or nuclear techniques.
Lauro Cortigiani et al. Eur Heart J Cardiovasc Imaging 2012;13:219-226

Modes of revascularization
• CABG:– Technically straight forward, – Durable– Evidence based– Increased risk in heart failure
• PCI:– Technically challenging (CTO)– Restenosis– Paucity of evidence

ESC Guidelines Heart failure 2012

ESC Guidelines Myocardial Revascularization 2014

ESC Guidelines Heart failure 2012

ESC Guidelines Heart failure 2012

ESC Guidelines Myocardial Revascularization 2014

Guideline summary• Conditional revascularization for HF
– Angina– Proximal anatomy– Viability/Ischemia
• In Acute heart failure (ACS)– PCI is preferred over CABG
• In Chronic heart failure– CABG is preferred over PCI

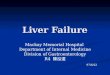
Figure 5 Management algorithm for patients with LV dysfunction and suspected coronary disease. SPECT , Single-photon emission computed tomography; Echo , echocardiography; CABG , coron...
Harry R. Phillips , Christopher M. O'Connor , Joseph Rogers
Revascularization for heart failure
American Heart Journal, Volume 153, Issue 4, Supplement, 2007, 65 - 73
Flow chart of ischemic cardiomyopathy

Revascularization for chronic HF Prospective randomized trials
• CABG Vs. Medical: STICH trial
• PCI Vs. Medical: None
• CABG Vs. PCI: None

1212
RandomizedCABG
Randomized MED only
610602
STICH Revascularization Hypothesis
•• 99 clinical sites in 22 countries99 clinical sites in 22 countries
•• Enrollment: July 2002 – May 2007Enrollment: July 2002 – May 2007

All-Cause Mortality — As Randomized

Death or Cardiovascular Hospitalization — As Randomized

Time-varying Hazard Ratios — As Randomized
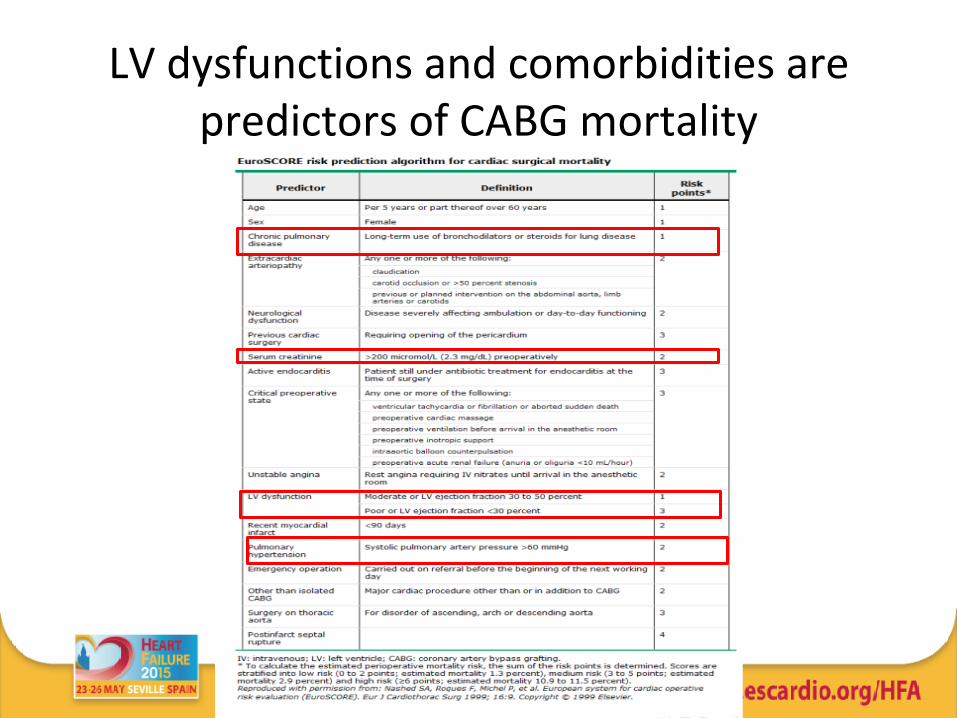
LV dysfunctions and comorbidities are predictors of CABG mortality

Post STICH clarifications
• The concept of re-vascularizing viable myocardium is viable.
• CABG – may be hazardous• PCI – a possible alternative
- Paucity of evidence

PCI can be effective in ischemic cardiomyopathy
Facilitation of LV functional recovery post PCI by levosimendan
Oct 2012.J Cardiol D… Hasin Y. Int Qarawani
Poria:No cardiac surgery

P=0.79 P=0.78
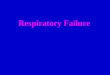
LVEF before and after revascularization+ Levosimendan and after 6 months follow-up
In group A : Improvement in LVEF at discharge (after) relatively to the baseline( before) (P<.0001) and at 6 months follow up relatively to the discharge (P<0001)In group B1: Improvement in LVEF at discharge relatively to the baseline (P<0.001); but there is no significant improvement in LVEF at follow up relatively to the discharge (P=0.485) In group B2: No improvement in LVEF at discharge relatively to the baseline (P=0.79); and at follow up relatively to the discharge (P=0.78)
P=0.48
P<0.001 P<0.001
P<0.001

A,B1 P=0.845
A,B2 P=0.019B1,B2 P=0.038
Kaplan Meier survival curves
There is no difference in survival between group A (improved LV function post revascularization) and B1 (improved LV function post revascularization and levosimendan (P=0.8475),The survival of group B2 (no improvement in LV post revascularization and Levosimendan) is significantly reduced
B1
A
B2

CABG or PCI for heart failure
Revascularization in patients with heart failure
Tsuyuki, Ross T., et al. "Revascularization in patients with heart failure."Canadian Medical Association Journal 175.4 (2006): 361-365.
A retrospective analysis of 2538 patients with Heart failure, ≈ 25% with EF ≤ 35%, 48.5% PCI

Park, Seung-Jung, et al. New England Journal of Medicine 372.13 (2015): 1204-1212.
Trial of Everolimus-Eluting Stents or Bypass Surgery for Coronary Disease (BEST)

Predicting Benefit From Revascularization in Patients With Ischemic Heart Failure
Orla Buckley, MD; Marcelo Di Carli, MD Circulation.2011; 123: 444-450
Current practice
Case report and contemporary review
“The incorporation of an assessment of ischemia with viability assessment can provide valuable additional information for patient selection for revascularization.”
“In light of the dilated LV, severe LV dysfunction, and potential surgical morbidity and mortality, our patient received percutaneous therapy, with successful stenting of the left anterior descending and right coronary arteries. ”

Conclusions• Revascularization for HF is appropriate provided
significant viable (yet stunned or hibernated) myocardium
• PCI is preferred for acute HF (ACS)• CABG in the presence of HF is associated with
increased risk• Paucity of evidence for PCI in chronic HF • A RCT comparing CABG VS PCI is needed • Individual assessment (Patient characteristics, local
expertise) should determine the method of revascularization in chronic HF