Embed Size (px)
Citation preview

Interesting casePAWARIS WANGKIAT

History
Case ผปวยหญง อาย 40 ปCC: โดนทำาราย 3 hr pta

PI : 3 hr pta ผปวยใหประวตวาดมเหลาผปวยไม เมา จำา
เหตการณไดหมด เกดการทะเลาะววาท โดนทำารายดวยแทง
เหลกทมตะขอฟาดเขาทแขนขวา มอาการบวม มาก และมอซาย โดนตะขอเกยวมอซาย มแผล เปด แขนขวาสามารถขยบหวไหล
ขอศอก ขอมอ นวมอไดด แขนซาย ขยบขอมอ ไมได ไมชา ไม ออนแรง ทง 2 ขาง จงมา รพ.

Past history - ไมมประวตแพยา แพอาหาร - เปน HT มยาทานอย -NPO time 18.30

Physical ExaminationV/S:BT 37 degrees PR 100 /min RR 20 /min BP 137/73 mmHgGA:good consciousHEENT:no pale conjunctivae ,aniteric sclerae ,no woundHeart:WNLLungs:WNLAbdomen:soft ,not tenderExt:Rt armSwelling tenderness at forearm ,LW 1 cm ,full ROM ,distal neurovascular intact Lt armswelling and tenderness at ulnar side ,limit ROM due to pain at wrist ,LW 2 cm at palmar side ,LW 1 cm at dorsal side

Rt forearm

Lt hand

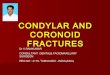
Film:Rt forearm AP ,lat

Film:Left hand AP ,Oblique

Film:Comminuted Fracture at 5th metacarpal bone Lt hand
Dx:Open fracture at fifth metacarpal bone
Lt hand

Management Admit NPO Dressing wound Preop lab ,CXR ,EKG IV fluid:5%DN/2 1000 ml iv 80 ml/hr Cefazolin 1 g IV stat then q 6 hr Set or for Excisional debridement + K-wire

Operation: Excisional debridement + K-wire

Post-op

Metacarpal Fracture

Anatomy

concave on palmar surface 1st, 4th, and 5th digits form mobile borders The second and third metacarpals are fixed rigidly at their bases,
while the fourth and fifth carpometacarpal (CMC) joints are capable of at least 15° and 25° of motion
three palmar and four dorsal interossei muscles arise from metacarpal shafts

Epidermology incidence
metacarpal fractures account for 40% of all hand injuries demographics
men aged 10-29 have highest incidence of metacarpal injuries location
metacarpal neck is most common site of fracture fifth metacarpal is most commonly injured

Mechanism of injury
direct blow to hand or rotational injury with axial load high energy injuries (ie. automobile) may result in multiple fractures

Management
Depend on location ,acceptable angulation ,no degree of deformities Surgical indication Displaced Intraarticular frature Unstable diaphyseal fracture :long oblique ,spiral ,comminuted Rotation deformity Open fracture Tendon injury association Unaccept angulation Multiple fracture Cosmetic Fail reduction

Nonoperative management Immobilization indications
must be stable pattern no rotational deformity acceptable angulation & shortening (see table)
Acceptable Shaft angulation
Shortening (mm) Acceptable neck angulation
Index&long finger 10-20 5 10-20
Ring finger 30 5 40
Little finger 40 5 50

Metacarpal head fracture Undisplace ,Stable fracture -immobilization in save position Displaced fracture (Intraarticular fracture) -ORIF

Metacarpal neck fracture Nonoperative reduction and short arm AP slab
acceptable degrees of apex dorsal angulation immobilize safe position include PIP joint Short arm AP slab for 3 weeks reduce using Jahss technique
90 degrees MCP flexion, dorsal pressure through proximal phalanx while stabilizing metacarpal shaft

Operative reduction and fixation
indications unacceptable angulation (see above table) open fractures any malrotation intraarticular fractures Cosmetic Fail reduction

Metacarpal shaft fracture Nonoperative immobilization
indications nondisplaced metacarpal neck fractures acceptable angulation (see above table) no malrotation shortening (aesthetic problem only)
immobilize MCP joints in 70-90 degrees of flexion Short arm AP slab in safe position for 3 weeks

Operative ORIF indications
open fractures unacceptable angulation any malrotation multiple fractures Cosmetic Fail reduction

Metacarpal base fracture Mostly nondisplaced Short arm AP slab in safe position and check rotation follow up 3 week

Reference
http://www.orthobullets.com/hand/6037/metacarpal-fractures http://emedicine.medscape.com/article/1239721-treatment

Thank You