-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
1/57
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
2/57
2
A paradigm shift: role of dopamine in behavior
Effect of L-DOPA in
dopamine-depleted rabbits
A. Carlsson (1960)
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
3/57
3
Emotional responses activate the same brain
regions as actual sensory stimuli
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
4/57
Contents
Basic principles of neuropharmacology and
classification of brain diseases Monamines: properties and
relevance for neuro- and
psychopharmacology
Antipsychotic drugs Experimental approaches to study brain
diseases:
Molecular basis of the sedative and anxiolytic action of
benzodiazepines
4
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
5/57
5
Basic principles of neuropharmacology
CNS diseases affect a large fraction of the general
population and have a very high social cost The
pathophysiological mechanisms underlying most
brain disorders are poorly understood
Many CNS disorders have a genetic basis. The
elucidation of mutations in familial forms of thesediseases
contributes markedly to our understanding oftheir
pathophysiology
Pharmacological treatments are mainly symptomatic
and the mechanism of drug action is often unknown
Neuropsychiatric disorders are difficult to reproduce inanimal
models
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
6/57
Experimental approaches to study brain diseases
Genetic screening of familial forms of disease to
identify genes contributing to the pathophysiology
Large scale genetic screening for identifying disease-
susceptibility genes
Molecular and cell biological studies in vitro to
understand the function of implicated genes In vivo animal
models (lesion, pharmacological
treatment, targeted gene mutations)
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
7/57
Classification of brain diseases (1)
1. Psychiatric diseases
Neurodevelopmental disorders (autism, Rettsyndrome, X-linked
mental retardation, attention-
deficit disorders)
Anxiety (panic, generalized anxiety, phobia, post-
traumatic stress disorder)
Mood disorders (depression, bipolar disorder)
Schizophrenia, Tourettes disease
Drug dependence
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
8/57
Classification of brain diseases (2)
2. Neurological diseases
Stroke and ischemia Brain lesions (trauma, tumors,
infections)
Epilepsy
Chronic pain Sleep disorders
Movement disorders (dystonia; tremor)
3. Autoimmune diseases Multiple Sclerosis (MS)
Myasthenia gravis
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
9/57
Classification of brain diseases (3)
4. Neurodegenerative diseases
Alzheimer Parkinson
Huntington
Fronto-temporal lobe dementia (FTLD) Amyotrophic lateral
sclerosis (ALS)
Prion diseases (Creutzfeld-Jacob)
The cause of neurodegeneration is not established but is
oftenlinked to the production of protein aggregates (e.g.
-amyloids),
due to abnormal proteolytic processing or to mutations
(e.g.,
trinucleotide repeats)
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
10/57
Examples of diseases caused by trinucleotide repeats
Disease Repeat
Fragile X syndrome (CGG)n in FMR1 gene
Myotonic dystrophy (CTG)n in myotonin-protein
kinase gene
Spinobulbar muscle
dystrophy
(CAG)n in androgen-receptor
gene
Huntington (CAG)n in Huntingtin gene
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
11/57
11
Huntingtons disease
Autosomal dominant disorder causes by mutation in
the huntingtin gene (short arm of chromosome 4)
Onset in middle adulthood (minor motor coordination
problems, involuntary jerking progressing towards
major deterioration)
Cognitive alterations and changes in personality(impulsivity,
depression, psychotic symptoms)
Molecular basis: presence of tri-nucleotide repeats
(37 86) coding for glutamine (CAG). Longer repeats
lead to early onset and more severe symptoms
Physiological role of huntingtin is unknown
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
12/57
12
Pathophysiology of Huntingtons disease
Progredient loss of
GABAergic
neurons inputamen and
caudate nucleus
Upregulation ofGABAA receptors
in target regions
(globus pallidus)
Selectivity ofdegeneration is not
explained
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
13/57
Lessons from Huntingtons disease
Power of reverse genetics: the affected gene could
be identified without knowledge about ist function The
pathophysiology of the disease is not due to anobvious dysfunction
in the striatum
The selectivity of neurodegeneration remainsunexplained
The path to therapy is very long and no goal is insight
In the case of complex genetic diseases, such aspsychiatric
diseases, the development of novel
therapies based on genetic information might beeven more
difficult
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
14/57
14
Monoamines: relevance to psycho- and
neuropharmacology
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
15/57
15
Monoamines
Catecholamines (dopamine, noradrenaline, and
adrenaline) are derived from tyrosine Serotonin (an indolamine)
is derived from tryptophan
They are the neurotransmitter of small groups ofneurons in the
brainstem that innervate most of the
brain Monoaminergic neurons regulate brain state and
function (neuroendocrine systems, sleep-wake cycle,motor
functions, sensory perception, emotions,
attention, memory)
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
16/57
Catecholamine synthesis
16
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
17/57
Common principles of monoaminergic transmission
Local synthesis and storage in vesicles
Ca++-dependent release
Termination of synaptic transmission by re-uptake.
The transporter proteins are a major drug target
Action on a multitude of receptors (mainly 7 TM
domain receptors coupled to G-proteins)
Presence of pre- and postsynaptic receptors
Complex metabolism, in neurons, glial cells, and
other tissues (Monoamine oxidase A and B);metabolites can be
toxic
17
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
18/57
18
Significance of monoaminergic transmission in
neuro- and psychopharmacology
Monoaminergic transmission is the target of many
psychoactive drugs (antidepressants, antipsychotic
drugs, some psychostimulant and psychotropicdrugs, and
anti-parkinson drugs)
Many unwanted side effects of psychopharma-
cological treatment arise from interactions withmonoaminergic
transmission
Dysfunction of dopaminergic systems underlie
multiple neurological and psychiatric disorders, as
well as drug addiction
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
19/57
19
Complex pharmacology of monoaminergic systems
Direct drug effects by receptor activation/inhibition(agonist,
antagonist)
Indirect effects by enhancing effects of endogenoustransmitter
(increased release (e.g., amphetamin,inhibition of re-uptake (e.g.
cocain), inhibition ofcatabolism)
Complex interactions with precursor (e.g., L-Dopa)
orpseudo-transmitters (e.g., -Methyl-Tyrosin)
Inhibition of catabolism can affect pseudo-transmitterspresent
in food
Complex regulation of receptors
(super-sensitivity,desensitization, opposite action of pre- and
post-synaptic receptors
Importance of target selectivity
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
20/57
A dopaminergic synapse
20
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
21/57
Dopamine receptors
21
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
22/57
22
Dopamine
Major dopaminergic projections
Mesostriatal projection Mesolimbic projection
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
23/57
Thalamus
Ca
Pu
GPe
GPi
ic
STN
SNr
SNc
Hypoth
Hip
Insula
cc
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
24/57
24
DA receptor agonist-induced rotation in lesioned
animals
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
25/57
25
Opposite rotation effects caused by amphetamine
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
26/57
26
Serotonin (5-Hydroxytryptamine)
Source:Enterochromaffin cells, thrombocytes,
neurotransmitter in centralneurons (raphe nuclei)
EffectsPeriphery: complex actions on thecardiovascular system,
increasedmotility of the gastrointestinal
tract,vasoconstriction
CNS: Regulation of blood pressure,
temperature, appetite, sleep-weakcycle, motor activity, pain
perception,emotional behavior (serotoninreuptake inhibitors
areantidepressants)
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
27/57
27
Serotonergic neurons
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
28/57
Functional and pharmacological relevance of
the serotonergic system
Serotonin exerts multiple, complex actions by
activating pre- and postsynaptic receptors coupled to
various signal transduction pathways
Serotonin regulates mood, attention, sleep-wake
cycle, descending pain control, motor systems,
autonomic functions, neuroendocrine systems Selective 5-HT
reuptake inhibitors (SSRI) are widely
used antidepressants
Psychostimulants, recreational drugs, and
hallucinogens have mixed actions of theserotonergic,
noradrenergic, and dopaminergic
system.
28
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
29/57
29
Noradrenergic neurons: Locus coeruleus
Immunhistochemistry of dopamine--hydroxylase Nissl staining
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
30/57
30
Noradrenergic projections from the locus coeruleus
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
31/57
Scheme of serotonergic and adrenergic synapses
31
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
32/57
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
33/57
Pharmacotherapy of Parkinsons disease
Dopamine receptor agonists (D1 and D2)
Apomorphin, Bromocriptin, Cabergolin, Lisurid,
Dihydroergocriptin, Pergolid, Ropinirol, etc.
L-Dopa
Mode of action: L-Dopa is transported across the
blood-brain barrier and converted into dopamine(mainly in
dopaminergic neurons)
Is given in combination with inhibitors of Dopa-decarboxylase
(Carbidopa, Benserazid) to minimizeperipheral side effects
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
34/57
Metabolism of L-Dopa
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
35/57
35
Antipsychotic drugs
Treatment of schizophrenia
Typical (Dopamine D2 receptor antagonists) Phenothiazine
derivatives (Chlorpromazine)
Butyrophenone (Haloperidol)
Numerous side-effects (blockade of Ach, NA, 5-HT
receptors): sedation, autonomic dysfunction,
involuntary movements
Atypical (mechanism of action unknown)
Clozapine
Risperidone
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
36/57
36
Effects of antipsychotics on the DA system
Location Clinical effects (due to blockade of D2 receptors)
Mesolimbic,mesocortical
pathway
Antipsychotic action by modulation of neuronal circuitsand
regulation of excitatory-inhibitory balance (only
positive symptoms)
Nigrostriatal
pathway
Extrapyramidal motor symptoms (EPS): Parkinson-like
symptoms and dyskinesia
Tuberoinfundibular
projection
Gynaecomasty, milk secretion (due to increased prolactin
secretion)
Medulla oblongata
(area postrema)
Anti-emetic effects
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
37/57
37
Extrapyramidal motor symptoms
Syndrom Symptoms Prevalence,
duration
Treatment
Early dyskinesia Head and neck muscle spasms 5%, at start of
therapy
Anti-cholinergic
drugs
Parkinsonoid Akinesis, rigor, tremor, hyper-
salivation
20-30%
up to 8 weeks
Dose,
anti-cholinergic
drugs
Akathisia Agitation, restlessness 25%
up to12 weeks
Dose
benzodiazepines
Late dyskinesia Chronic hyperkinetic syndrome
(irreversible); stereotypic
movements of the lips, tongue,jaws
20%
After
months/years
Change to clozapin;
no anti-cholinergic
drugs
Malignant
neuroleptic
syndrom
Acute emergency (rigor, akinesis,
high fever, tachycardia, coma)
rare
before 2 weeks
Stop therapy;
dentrolene
Relationship between wanted and unwanted effects
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
38/57
38
Relationship between wanted and unwanted effects
of neuroleptics
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
39/57
Tests for cognitive function
39
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
40/57
40
Predicting schizophrenia: a longitudinal study
Differences in gray matter volume prior to first
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
41/57
41
Differences in gray matter volume prior to first
psychosis
Differences in gray matter volume after onset of
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
42/57
42
Differences in gray matter volume after onset of
psychosis
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
43/57
43
New hypotheses about the pathophysiology of schizophrenia
Structural anomalies in the brain can be shown priorto the first
psychosis
Functional disturbances occur selectively in prefrontalcortex
(thought and memory disorders)
NMDA-Receptor antagonists (e.g. PCP) producepsychoses in healthy
volunteers
Schizophrenia may be related to alteredglutamatergic
neurotransmission
Selective deficit of GABAergic transmission inprefrontal
cortex
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
44/57
44
Further hypotheses
Selective glutathion deficit (protection against
oxidative stress) in prefrontal cortex
Altered function of oligodendrocytes ( possible
disturbance of myelination)
Abnormal neuronal migration during formation of theneocortex
(reelin hypothesis)
Consequences of a prenatal production of
inflammatory cytokines (disturbance of braindevelopment during a
critical period)
Evidence for synaptic alterations in the prefrontal
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
45/57
45
Evidence for synaptic alterations in the prefrontal
cortex of schizophrenia patients
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
46/57
Altered regulation of dopaminergic function in schizophrenia
46
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
47/57
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
48/57
Allosteric modulation of GABAergic
transmission by benzodiazepines
48
Benzodiazepines
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
49/57
Benzodiazepines
49
Benzodiazepines are drugs with a high affinity and
selectivity for GABAA receptors. They differ mainly in
their pharmacokinetic profile (half-life, activemetabolites)
Clinical applications of benzodiazepine agonists Sleep disorders
(sedation, hypnosis)
Anxiety disorders (tranquillizer) Muscle spams, dystonia (muscle
relaxant)
Status epilepticus (anticonvulsants)
Side effects
Motor incoordination Anterograde amnesia
Ethanol potentiation
Tolerance
GABA receptors
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
50/57
GABAA receptors
50
Allosteric modulation by benzodiazepines
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
51/57
Allosteric modulation by benzodiazepines
51
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
52/57
Diazepam sensitive GABA receptor subtypes
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
53/57
Diazepam-sensitive GABAA receptor subtypes
53
1
2
3
5
diazepam
H101R: a molecular switch for diazepam sensitivity
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
54/57
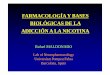
H101R: a molecular switch for diazepam sensitivity
54
Wieland and Lddens, 1992
Diazepam-insensitive receptors in 1(H101R) mutants
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
55/57
Diazepam-insensitive receptors in 1(H101R) mutants
55
3H Ro15 4513 + diazepam
wt
1(H101R) 1 subunit immunostaining
3H Ro15 4513 is a ligand bindingto all benzodiazepine sites; it
can
be displaced only from diazepam-
sensitive sites
Lack of sedative effect of diazepam in 1(H101R) mutants
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
56/57
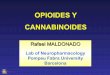
Lack of sedative effect of diazepam in 1(H101R) mutants
56
WT 1(H101R)
Further reading
-
8/13/2019 02042012 Fritschy Neuropharmacology FS2012
57/57
57
Further reading
Books:
The biochemical basis of neuropharmacology
(Cooper, Bloom, Roth)
A primer of drug action (R.M. Julien; Freeman and
company, New York)
Molecular Neuropharmacology (E.J. Nestler, S. E.Hyman, R.C.
Malenka; The McGraw-Hill
Companies, Inc., New York)