Embed Size (px)
Citation preview

PENAPISAN TEKNOLOGI DIAGNOSTIK
Bambang Udji Djoko Rianto

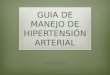
The technology assesment iterative loop
Efficiency
Burden of illness
Efficacy
Screening & diagnosis
Community Effectiveness
Synthesis & implementation
Monitoring &reassessment

TUJUAN
Memahami berbagai masalah terkait dg penggunaan teknologi diagnostik bidang kedokteran/kesehatan
Melakukan penilaian kritis thd penggunaan suatu teknologi diagnostik

PENDAHULUAN
Ketepatan diagnosis: kunci sukses penanganan pasien
Pengembangan teknologi diagnostik membawa manfaat dan dampak

Disease/non diseaseDisease/non disease
TEKNOLOGI DIAGNOSTIKTEKNOLOGI DIAGNOSTIK
AccurateAccurate SafeSafe Therapeutic impactTherapeutic impact
Pendahuluan

Jumlah & rerata CT-scanner/1 juta penduduk
Jumlah CT Scanner
CT scanner/juta penduduk
Negara
1986 1988 1986 1988 AS Jepang Perancis Belgia Jerman Barat Denmark Belanda Inggris Itali
3000 3300 264 64
423 23 45
149 210
4991 5448 350 118 595
? 83
204 338
12.8 27.5 4.7 6.4 6.9 4.6 3.2 2.7 3.5
21.7 44.3 6.3
12.1 9.8 ?
5.7 3.6 5.9

Jumlah & rerata MRI/ 1 juta penduduk
Jumlah MRI Rerata MRI/juta penduduk
Negara
1986 1988 1986 1988
AS Jepang Perancis Belgia Jerman Barat Belanda Inggris Itali
110 10 29 7 41 2 14 13
1150 256 34 7
91 7
28 29
0.5 0.1 0.5 0.7 0.7 0.4 0.3 0.2
5.0 2.0 0.6 0.7 1.5 0.5 0.5 0.5

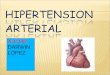
Test-treatment thresholds
Prevalence (pre-test probability) of target disoreder
0 .10 .20 .30 .40 .50 .60 .70 .80 .90
Do not test
Do not treat
Test, & treat on the basis of the
test’s results
Do not test
Get on with treatment
A B

Penilaian teknologi diagnostik
Tingkat akurasi Tingkat ketelitian Peruntukan teknologi diagnostik Evaluasi teknis Peranan dalam proses pengambilan keputusan
terapetik Peranan dalam penurunan morbiditas dan
mortalitas Keuntungan bagi klinisi Keuntungan bagi pasien


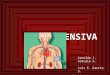
Diagnostic accuracy Sensitivitas Spesifisitas Likelihood ratio

+ -
+
Penyakit
Test
Truepositive
Falsepositive
Falsenegative
Truenegative
-

DEFINISI
Sensitivity: proporsi hasil test positif pada kelompok penderita
Specificity: proporsi hasil test negatif pada kelompok orang tanpa penyakit
Positive PV: probabilitas penyakit pada penderita dengan hasil test positif
Negative PV: probabilitas seseorang dengan hasil test negatif untuk benar-benar bebas dari penyakit

Sensitivity = a / (a+c)Specificity = d / (b+d)Accuracy = (a+d) / N
+ PV = a / (a+b)- PV = d/ (c+d)Prevalence = (a+c) / N
+ -
+
Gold Standard
Hasiltest
a b
c d-
a+b
c+d
a+c b+d N

2 Pendekatan ttg penampilan diagnosis
Prevalensi Sensitivitas/Spesifisitas
Nilai ramal
Pre-testprobability
Rasiokemungkinan
Post-testprobability

Likelihood Ratio Likelihood ratio positif: rasio hasil tes
positip yang dijumpai pada kelompok sakit dan kelompok tidak sakit
Likelihood ratio negatif: rasio hasil tes negatip yang dijumpai pada kelompok sakit dan kelompok tidak sakit

a/a+cLR (+) = --------
b/b+d
c/a+cLR (-) = --------
d/b+d
+ -
+
Gold Standard
Hasiltest
a b
c d-
a+b
c+d
a+c b+d N


Lieklihood ratio
>10 atau < 0,1, menghasilkan perubahan yg besar dari pre dan post test probability. Dan sering conclusive
5-10 dan 0,1-0,2, perubahan sedang 2-5 daan 0,2-0,5 perubahan kecil (kadang-
kadang penting) 1-2 dan 0,5-1, mengubah probability kecil
sekali (dan jarang penting)

Ketelitian diagnosis
Skala nominal: un-weighted kappa Skala ordinal: weighted kappa Skala interval/rasio: intra-class coefficient
correlation (ICC), CV

Peruntukan teknologi diagnostik Menegakkan diagnosis Menyingkirkan diagnosis Skrining

Technical evaluation
Prosedur sederhana Risiko minimal Interpretasi jelas (risiko false positive rendah) Risiko kesalahan pembacaan akibat kesalahan
prosedur operasional kecil Ketergantungan terhadap rekonfirmasi diagnosis
atau second opinion kecil

Diagnostic impact
Mendeteksi penyakit pada fase dini Rekonfirmasi terhadap prosedur diagnostik
sebelumnya Hasil mempengaruhi prognosis Mengurangi risiko keraguan

Therapeutic impact
Mensupport therapeutic decision making process
Early treatment Mengubah kebijakan terapi yang sudah
diputuskan

Health impact
Early warning system Morbiditas & mortalitas turun Quality of health care Reassurance

Seberapa besar kontribusinya terhadap therapeutic decision making process
Prompt action
Keuntungan yang diperoleh melebihi cost yang dikeluarkan
Membantu menetapkan terapi yang lebih do
more good than harm

Prompt treatmentPrompt treatment
Early diagnosisEarly diagnosis
morbiditasmortalitasmorbiditasmortalitas
Seberapa besar kontribusinya terhadap penurunan mortalitas dan morbiditas

Apa keuntungannya bagi klinisi
Menghilangkan keraguan diagnosis Improving confidence Lebih terfokus pada pilihan terapi Mengurangi risiko malpractice Improving quality of care

Morbidity/mortalityMorbidity/mortality
Quality of lifeQuality of life
DisabilityDisability
Opportunity costOpportunity cost
Patient satisfactionPatient satisfaction
Apa keuntungannya bagi pasien

Should general practitioner perform diagnostic tests on patients before prescribing antibiotics?,BMJ 318, 799-802 Kendali resistensi thd antibiotik tergantung
perilaku peresepan yg rassional oleh dokter umum.
Pemeriksaan mikrobiologis merupakan dasar pemberian antibiotik yg rasional. Tetapi hal ini memiliki kendala
Salah satu cara untuk mengatasi masalah ini di Denmark melakukan pemeriksaan mikrobiologis menggunakan mikroskop fase kontras dan kit diagnostik sederhana (near patient testing)

Keuntungan near patient testing Hasil pemeriksaan lebih cepat tersedia
dan keputusan dapat segeraa diambil Birokrasi dikurangi. Menghemat waktu,
mengurangi problem komunikasi, menghemat uang, lebih murah dan mendapat tambahan pendapatan.

Isu tentang mutu
Baku pemeriksaan ditempat praktek harus seimbang dg yg di laboratorium
Syarat pemeriksaan: sederhana, cepat, handal, mudah dibaca dan diinterpretasikan
Contoh: pemeriksaan mikroskopis fase kontras untuk ISK, vaginitis/vaginosis, pharyngotonsilitis, dermatophytosis, perianal pruritus, mononukleosis

Kepentingan near patient tests
Paling penting dilakukan untuk discharge vagina, dysuria, pharyngitis.
Pemeriksaan mikroskopis fase kontras di tempat praktek umum lebih teliti dibanding di laboratorium
Berfungsi sbg skrining pemeriksaan berikutnya, misalnya biakan, pemeriksaan Chlamydia, athropic vaginitis

Aspek uji diagnosis dalam praktek dokter umum Apakah uji/pemeriksaan layak dan valid?
Perlu selektif, pelatihan dan kendali mutu. Grup A streptococcus vs ASTO. Test strip vs metode skoring klinis.
Apakah uji/pemeriksaan mempercepat kesembuhan? Penurunan keluhan vs kekambuhan; 50% bakteriuria akan sembuh dlm waktu 3 hari tanpa antibiotik

Aspek-aspek uji diagnosis dalam praktek dokter umum
Apakah uji/pemeriksaan mencegah komplikasi?
Apakah pasien diuntungkan? Apakah uji/pemeriksaan cost-effective?

Kesimpulan
Pemeriksaan diagnosis untuk infeksi akut dilakukan jika ada bukti yg kuat ttg validitas, kelayakan, dan cost-effectivenes
Sebelum ada bukti yg kuat dokter umum dianjurkaan untuk memberikan obat simtomatis untuk infeksi yg paling sering dijumpai tanpa tergantung pd pemeriksaan diagnosis maupun antibiotik

The impact of medical imaging on physician’s diagnostic and therapeutic thinking Eur. Radiol. 8: 488-90

Pendahuluan
Ada perubahan kecenderungan bahwa pemeriksaan radiologi “requested” dari pada “ordered”
Permintaan pemeriksaan sering didiskusikan dalam pertemuan antara dokter klinis dan radiolog dengan memperhatikan kondisi klinis pasien, penampilan diagnosis dari bbrp pilihan, biaya, ketersediaan, daan expertise.

5 tahap dalam penilaian teknologi radiologi
1. Technical performance
2. Diagnostic performance
3. Diagnostic impact – keputusan diagnostik
4. Diagnostic impact – keputusan terapi
5. Impact on health

Diagnostic thinking
Dulu diagnosis pd pasien rawat jalan dpt ditegakkan dg anamnesis yg baik dan pemeriksaan fisik
Modern radiologi mungkin dpt mengubah fenomena ini
Radiolog dpt bekerja sama dg klinisi dlm penatalaksanaan pasien

Diagnostic thinking
Diagnosis klinis: peran radiologi kurang tampak apabila klinisi memberikan diagnosis klinis terlalu luas, begitu juga sebaliknya
Diagnostic confidence, ditetapkaan dg bbrp cara: pre-test probability, hasil V/Q scan, 10 point scale, VAS, LR, diagnostic entropy

Diagnostic thinking
Displacement of other investigations: pemeriksaan alat lama dan alat baru, alat baru dpt menggantikan alat lama, misalnya MRI pada meatus auditorius interna menggantikan pemeriksaan neurofisiologis
Health economists and statisticians

Therapeutic thinking
Pilihan terapi tersedia setelah diagnosis ditegakkan. Pilihan ini juga tergantung dari kwalifikasi pengirim
Pengembangan algoritme

How Often Should We Screen for Cervical Cancer? AU: Sarah Feldman, M.D., M.P.H. SO: New Eng J of Med, Volume 349, Number 16; October 16,
2003 Over the past 60 years, the mortality from cervical
cancer has decreased dramatically. Much of the reduction has been due to the widespread use of the Papanicolaou test, which has enabled clinicians to detect cervical intraepithelial neoplasia before it progresses to cervical cancer and to detect cervical cancer at an early stage.
When cervical cancer is detected early, the five-year survival rate is more than 90 %

PAP Smear test
> 80 % of women undergoing screening in any two-year period and > 90 % having been screened at least once.
Questions remain about optimal screening strategies. One key question is the optimal frequency of testing.
Cost–benefit analyses have suggested that lifelong annual screening may not result in substantially better outcomes than less frequent screening and is much more costly. With this in mind, the American Cancer Society recently revised its guidelines for screening

PAP Smear test
Recommending intervals between screenings ranging from one to three years, depending on several factors, such as age, screening history, type of Papanicolaou smear, and history of immunosuppression.
Other guidelines have also suggested screening less frequently than annually after three consecutive normal annual Papanicolaou tests and pelvic examinations. Yet there are not many data to support these recommendations.

Risk of Cervical Cancer Associated with Extending the Interval between Cervical-Cancer Screenings
AU: Sawaya et al
SO: New Eng J of Medicine, Volume 349, Number 16; October 16, 2003

Methods
We determined the prevalence of biopsy-proven cervical neoplasia among 938,576 women younger than 65 years of age, stratified according to the number of previous consecutive negative Papanicolaou tests. Using a Markov model that estimates the rate at which dysplasia will progress to cancer, we estimated the risk of cancer within three years after one or more negative Papanicolaou tests, as well as the number of additional
Papanicolaou tests and colposcopic examinations that would be required to avert one case of cancer given a particular interval between screenings.

Result
Among 31,728 women 30 to 64 years of age who had had three or more consecutive negative tests
The prevalence of biopsy-proven cervical intraepithelial neoplasia of grade 2 was 0.028 %
The prevalence of grade 3 neoplasia was 0.019 % None of the women had invasive cervical cancer

Result
According to our model, the estimated risk of cancer
with annual Papanicolaou tests for three years :
2 in 100,000 among women 30 to 44 years of age,
1 in 100,000 among women 45 to 59 years of age,
1 in 100,000 among women 60 to 64 years of age;
these risks would be 5 in 100,000, 2 in 100,000, and 1
in 100,000, respectively, if screening were performed
once three years after the last negative test.

Result
To avert one additional case of cancer by screening 100,000 women annually for three years rather than once three years after the last negative test, an average of 69,665 additional Papanicolaou tests and 3861 colposcopic examinations would be needed in women 30 to 44 years of age and an average of 209,324 additional Papanicolaou tests and 11,502 colposcopic examinations in women 45 to 59 years of age.

Conclusion
As compared with annual screening for three years, screening performed once three years after the last negative test in women 30 to 64 years of age who have had three or more consecutive negative Papanicolaou tests is associated with an average excess risk of cervical cancer of approximately 3 in 100,000.

Colorectal cancer screening: an overview of available and current recommendations
Early DS, Southern Medical Journal, 92 (3):258-265

Colorectal cancer screening
Skrining pd asimtomatik dpt menurunkan insidensi dan kematian
Database medline: artikel yg memuat rasional skrining kanker colorectal, metode yg digunakan, hasil guna dan rekomendasi yg digunakan saat ini
Hasil: metode: flexible sigmoidoscopy, fecal blood test, barium enema, colonoscopy. Metode yg digunakan dan frekwensi skrining tergantung dr risiko

Colorectal cancer screening
Penerimaan skrining oleh pasien dan dokter belum optimal
Masih diperdebatkan: Potensi skrining untuk mencegah
kematian dari ca colorectal, Cost effectiveness jika digunakan
untuk populasi umum.

Terima Kasih