-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
1/31
INTRODUCTION
A clavicle fracture is a bone fracture in the clavicle, or
collarbone.Claviclefractures involve approximately 5% of all
fractures seen in hospital emergency
admissions. Clavicles are the most common broken bone in the
human body. It ismost often fractured in the middle third of its
length. Children and infants areparticularly prone to it. Newborns
often present clavicle fractures following adifficult delivery.
After fracture of the clavicle, the sternocleidomastoid
muscleelevates the proximal fragment of the bone. The trapezius
muscle is unable tohold up the distal fragment owing to the weight
of the upper limb, and thus theshoulder droops.
A rib fracture is a break orfracture in one or more of the bones
making upthe rib cage. The middle ribs are the ones most commonly
fractured. Fracturesusually occur from direct blows or from
indirect crushing injuries. The weakest
part of a rib is just anterior to its angle, but a fracture can
occur anywhere. Themost commonly fractured ribs are the 7th and
10th. Rib fractures are usuallyquite painful because the ribs have
to move to allow forbreathing. Even a smallcrack can inflame a
tendon and cripple an arm.Rib fractures can occur withoutdirect
trauma and have been reported after sustained coughing and in
varioussports for example, rowing and golf often in elite athletes.
They can alsooccur as a consequence of diseases such as cancer or
infections (pathologicalfracture).
Cirrhosis is a consequence of chronic liver disease
characterized byreplacement of livertissue by fibrous scartissue as
well as regenerative nodules
(lumps that occur as a result of a process in which damaged
tissue isregenerated), leading to progressive loss of liver
function. Cirrhosis is mostcommonly caused by alcoholism, hepatitis
B and C, and fatty liver disease buthas many other possible causes.
Some cases are idiopathic, i.e., of unknowncause.The word
"cirrhosis" derives from Greek, meaning tawny (the orange-yellow
colour of the diseased liver).
Diabetes mellitus type 2 or type 2 diabetes (formerly called
[non-[insulin]]-dependent diabetes mellitus (NIDDM), or adult-onset
diabetes) is a disorder thatis characterized by high blood glucose
in the context of insulin resistance andrelative insulin
deficiency.While it is often initially managed by
increasingexercise and dietary modification, medications are
typically needed as thedisease progresses. There are an estimated
23.6 million people in the U.S.(7.8% of the population) with
diabetes with 17.9 million being diagnosed, 90% ofwhom are type
2.With prevalence rates doubling between 1990 and 2005, CDChas
characterized the increase as an epidemic. Traditionally considered
adisease of adults, type 2 diabetes is increasingly diagnosed in
children in parallelto rising obesity rates due to alterations in
dietary patterns as well as in life stylesduring childhood.
1
http://en.wikipedia.org/wiki/Bone_fracturehttp://en.wikipedia.org/wiki/Claviclehttp://en.wikipedia.org/wiki/Childrenhttp://en.wikipedia.org/wiki/Infantshttp://en.wikipedia.org/wiki/Newbornshttp://en.wikipedia.org/wiki/Childbirthhttp://en.wikipedia.org/wiki/Sternocleidomastoid_musclehttp://en.wikipedia.org/wiki/Trapezius_musclehttp://en.wikipedia.org/wiki/Bone_fracturehttp://en.wikipedia.org/wiki/Bonehttp://en.wikipedia.org/wiki/Rib_cagehttp://en.wikipedia.org/wiki/Breathhttp://en.wikipedia.org/wiki/Coughhttp://en.wikipedia.org/wiki/Sporthttp://en.wikipedia.org/wiki/Rowing_(sport)http://en.wikipedia.org/wiki/Golfhttp://en.wikipedia.org/wiki/Sportspersonhttp://en.wikipedia.org/w/index.php?title=Pathological_fracture&action=edit&redlink=1http://en.wikipedia.org/w/index.php?title=Pathological_fracture&action=edit&redlink=1http://en.wikipedia.org/wiki/Liverhttp://en.wikipedia.org/wiki/Diseasehttp://en.wikipedia.org/wiki/Tissue_(biology)http://en.wikipedia.org/wiki/Scarhttp://en.wikipedia.org/wiki/Nodule_(medicine)http://en.wikipedia.org/wiki/Alcoholismhttp://en.wikipedia.org/wiki/Hepatitis_Bhttp://en.wikipedia.org/wiki/Hepatitis_Chttp://en.wikipedia.org/wiki/Non-alcoholic_fatty_liver_diseasehttp://en.wikipedia.org/wiki/Idiopathichttp://en.wikipedia.org/wiki/Diabetes_mellitushttp://en.wikipedia.org/wiki/Metabolic_disorderhttp://en.wikipedia.org/wiki/Insulin_resistancehttp://en.wikipedia.org/wiki/Physical_exercisehttp://en.wikipedia.org/wiki/Dietinghttp://en.wikipedia.org/wiki/Centers_for_Disease_Control_and_Preventionhttp://en.wikipedia.org/wiki/Epidemichttp://en.wikipedia.org/wiki/Bone_fracturehttp://en.wikipedia.org/wiki/Claviclehttp://en.wikipedia.org/wiki/Childrenhttp://en.wikipedia.org/wiki/Infantshttp://en.wikipedia.org/wiki/Newbornshttp://en.wikipedia.org/wiki/Childbirthhttp://en.wikipedia.org/wiki/Sternocleidomastoid_musclehttp://en.wikipedia.org/wiki/Trapezius_musclehttp://en.wikipedia.org/wiki/Bone_fracturehttp://en.wikipedia.org/wiki/Bonehttp://en.wikipedia.org/wiki/Rib_cagehttp://en.wikipedia.org/wiki/Breathhttp://en.wikipedia.org/wiki/Coughhttp://en.wikipedia.org/wiki/Sporthttp://en.wikipedia.org/wiki/Rowing_(sport)http://en.wikipedia.org/wiki/Golfhttp://en.wikipedia.org/wiki/Sportspersonhttp://en.wikipedia.org/w/index.php?title=Pathological_fracture&action=edit&redlink=1http://en.wikipedia.org/w/index.php?title=Pathological_fracture&action=edit&redlink=1http://en.wikipedia.org/wiki/Liverhttp://en.wikipedia.org/wiki/Diseasehttp://en.wikipedia.org/wiki/Tissue_(biology)http://en.wikipedia.org/wiki/Scarhttp://en.wikipedia.org/wiki/Nodule_(medicine)http://en.wikipedia.org/wiki/Alcoholismhttp://en.wikipedia.org/wiki/Hepatitis_Bhttp://en.wikipedia.org/wiki/Hepatitis_Chttp://en.wikipedia.org/wiki/Non-alcoholic_fatty_liver_diseasehttp://en.wikipedia.org/wiki/Idiopathichttp://en.wikipedia.org/wiki/Diabetes_mellitushttp://en.wikipedia.org/wiki/Metabolic_disorderhttp://en.wikipedia.org/wiki/Insulin_resistancehttp://en.wikipedia.org/wiki/Physical_exercisehttp://en.wikipedia.org/wiki/Dietinghttp://en.wikipedia.org/wiki/Centers_for_Disease_Control_and_Preventionhttp://en.wikipedia.org/wiki/Epidemic
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
2/31
B. Objectives of the Study
The study aims to further analyze a patients condition providing
the
students of NCM501204 a definite idea on how it is to care for a
patient with the
same disease condition and how to interconnect all the other
laboratory and
significant findings of the physician to associate to the
patients current state and
condition. Proper assessment and nursing interventions are also
given priority to
emphasize the importance of nursing care to an ill patient. The
study also has an
objective of assessing and assisting the patient from her
present condition
towards the patients improvement in a higher level of
wellness.
C. Scope and Limitation of the Study
The study covers 2 days of assessment and care during our
exposure at
Cagayan de Oro Medical Center (COMC) and rendered our care to
the patient at
Station 4 (Private room) these includes thorough assessment,
giving of nursing
interventions, analyzing of the laboratory results, relating the
disease condition to
the Anatomy and Physiology of the Human body and the
Pathophysiology of the
disease.
The focus of the study is limited to the time that we had our
duty at
COMC, the span of time for the assessment of the patient has
limited since we
had only 2 days to assess and for our nursing interventions.
Also the hand writing
of the doctors at the doctors order are not legible.
2
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
3/31
II. PATIENTS PROFILE
Name: C.B.P
Age: 79 years old
Sex: Female
Birth date: January 12, 1930
Birth place: Zamboanga De l Sur
Occupation: Housewife
Income: 300 pesos/month
Civil status: Widower
Nationality: Filipino
Informant: Patient and SonsReligion: Roman Catholic
Address: Balucot, Tambulig, Zamboanga Del Sur
Number of children 5 children
CLINICAL PROFILE
Date of admission: August 1, 2009
Time of admission: 11:35 AM
Attending physician: Dr. Chang, Dr. Sison, Dr. Tia, Dr.
Pagdilao
Chief Complaint: Body malaise
Admitting diagnosis: DM, Fracture Left 8th Rib minimally
displaced
Fracture of Distal Left Clavicle
Diet: Soft Diabetic Diet
Vital Signs upon Assessment: BP: 140/80mmHg
T: 36.60 C
RR: 22 cpm
3
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
4/31
PR: 85 bpm
Patients Health History
In 2008, patient C.B.P. was admitted at Cebu and was diagnosed
to have
liver cirrhosis 2004, this is because of her diet since she was
young, she was
fond of eating street foods. She had been on Godex and
Essentiale Natural
Meds for several years.
History of Present Illness
A case of 79 year old, female, widower, Filipino fromBalucot,
Tambulig,
Zamboanga Del Sur, was admitted at Cagayan de Oro Medical Center
on august1, 2009 at exactly 11:35AM accompanied by her daugther. 2
weeks prior to
admission, the patient experienced a fall at there stairs (4
steps), she was
admitted at Zamboanga by then. Due to insufficiency of the
equipments of their
hospital, her children decided to transfer her at COMC here in
Cagayan de Oro
City and was diagnose DM, Fracture Left 8th Rib minimally
displaced Fracture of
Distal Left Clavicle.
4
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
5/31
III. GROWTH AND DEVELOPMENT
Developmental Task Theory of Robert Havighurst
A developmental task is a task which arises at or about a
certain period in
the life of an individual.
Basing on Havighurst theory our patient C.B.P. belongs in the
later
maturity 79 years old stage wherein she has adjusted to
decreasing physical
strength and health and the patient also has settled for a
reduced income.
Psychosexual Theory of Sigmund Freud
The psychosexual stage of Sigmund Freud has five
developmental
periods during which the individual seeks pleasure from
different areas of the
body associated with sexual feelings.
Basing in this theory, C.B.P. belongs to the genital stage
wherein she has
already achieved sexual desires. She has five children.
Fortunately, She has a
good personal relationship with her children. She has fully
achieved the
implications of this stage because she was able to raise a
family, making a livingand doing it independently apart from her
parents. The value of decision making
has already matured in the patient, upon making many decisions
for herself and
her family.
Psychosocial Theory of Erik Erickson
Erik Erickson envisioned life has a sequence of levels of
achievements.
Each stage signals tasks that must achieved. He believed that
the greater the
task achievement, the healthier the personality of the person.
Failure to achieve
the tasks influences the persons ability to achieve the next
tasks.
Basing on this theory, C.B.P. belongs to the maturity Stage
wherein she
has already achieved sexual desires he has 5 children at
present. The patient
5
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
6/31
feels that she has already lived longer to see her children grow
up and live a life
of their own. She thinks that she already has served her purpose
in this life and
found uniqueness in the life that she is leading. She accepted
that all life forms
has their own end and has accepted that sooner she will have to
leave his
children behind, because she is open in the concept of death but
she has also
fear from it.
Cognitive Theory of Jean Piaget
Cognitive development refers to how a person perceives, thinks,
and
gains understanding of his or her world through the interaction
and influence of
genetics and learning factors.Basing on this theory C.B.P.
belongs to the Formal Operational Phase
wherein she has solved previously encountered problems in a
logical manner
and has used rational thinking. This includes overcoming
financial problems and
her personal family problems.
6
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
7/31
IV. MEDICAL MANAGEMENT
A. Medical Orders and Rationale
Doctors Order RationaleAugust 1, 200911:35 AM
Pls. admit under the serviceof Dr. Chang
Secure consent of care
TPR q4
Soft Diabetic Diet
Labs: CBC, U/A, Chest x-rayPA view, Ultrasound of theliver and
gallbladder,NA+ K+
Start venoclysis with PNSS IL @ 10gtts/min
O2 2-3L/min
Med: Celecoxib 200mg BID
Intake and output monitor qshift
August 2, 2009
8:00 AM Request for FBS, crea, NA+
K+
IVF to follow PNSS 1L atsame rate.
For proper management/care.
For legal purposes
To monitor any changes in TPR
Diet for patient to provide proper
nutritionTo determine deviation and to knowany abnormalities
.
To provide fluid and electrolytes andserves as a channel for any
drug thatcan be administer through it (IVTT).
Provide enough oxygen.
For management of moderate tosevere pain.
To determine fluid balance going in andout from the body.
To re-evaluate the values of the result.
To provide fluid and electrolytes andserves as a channel for any
drug thatcan be administer through it (IVTT).
7
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
8/31
For Rehabilitation
Informed Dr. Sison for co-management
Meds: Kalimate 2 sachets TID
NaHCO3 650mg 1 tab TID
Lactulose 30ml OD
Continue Celecoxib 200mgBID
Refer accordingly
August 3, 20098:50 AM
Side drip Aminoleban 500 @20cc/hr.
Repeat for FBS, crea, NA+K+
Continue Rehabilitation
Informed Dra. Tia for co-management
Turn to sides q 2 hours
Moderate high back rest
Provide footboardMeds: Amoxiclav 500 I tab TID
Itopride 50 mg TID
Pancreatin 50mg BID
For management of the fracture
For co-management
For electrolytes balance in the bodyAntacid; neutralize secreted
acid.
Laxative: Prevent/treatment forconstipation.
Management of pain.
Refer any abnormalities/ anusualities.
For hepatic encelopathy due to chronicliver disease.
To monitor blood glucose level and toto check for electrolyte
imbalance.
For proper managementFor co-management
To prevent bed sore.
To facilitate proper breathing
To provide comfort.
For lower tract infections.
To prevent nausea and vomiting.
For bloating and flatulence as inpancreatic insufficiency.
Refer any abnormalities/ anusualities.
8
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
9/31
Refer accordingly
August 4, 20099:15AM
Ventolin 1 neb now
IVF to follow PNSS @10gtts/min
Treatment and prevention of asthma.
To provide fluid and electrolytes andserves as a channel for any
drug thatcan be administer through it (IVTT).
DRUG STUDY
SODIUM BICARBONATE
Classification: Acidifiers and AlkalinizersDosage/route: 650mg
TID , poMechanism of Action: Restores buffering capacity of the
body and neutralizerexcess acid.Specific Indication: Cardiac
Arrest, Metabolic Acidosis, Systemic or UrinaryAlkalinization and
AntacidContraindications: Patients who are losing chlorides because
of vomiting,continuous GI suction and in those receiving diuretics
that producehypochloremic alkalosis. Oral sodium bicarbonate is
contraindicated for patientswith acute ingestion of strong mineral
acids.
Side Effects: Tetany, Edema, Gastric Distention, Belching, and
Flatulence.Nursing Precaution: To avoid risk of alkalosis, obtain
blood pH, partial pressure of arterial
oxygen, partial pressure of partial carbon dioxide, and
electrolyte levels.Keep prescriber informed of laboratory
results.
KALIMATE
Classification: ElectrolytesMechanism of Action: After
administration of Kalimate via oral, calcium ion of
Kalimate is exchanged for potassium ion in the intestinal tract,
particularly aroundthe colon, and Kalimate is excreted as unchanged
polystyrene sulfonate resininto the feces without digestion and
absorption. In consequence, potassium inthe intestinal tract is
excreted outside the body.Dosage/route: 2 sachets TID, poSpecific
Indication: Prevention & treatment of hyperkalemia resulting
fromacute or chronic renal failure.Contraindications: Patients w/
intestinal obstruction & stenosis, constipation.
9
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
10/31
Side Effects: Constipation, anorexia & nausea.
Hypopotassemia.Nursing Precaution: Careful administration in
patients with hyperparathyroidism(blood concentration of calcium
may be increased by ion exchange) and patientswith multiple myeloma
(blood concentration of calcium may be increased by
ionexchange).
Important: Kalimate should be administered while measuring the
serumpotassium and serum calcium levels regularly to prevent
overdose. If anyabnormal findings are observed, appropriate
measures eg, reduction of dose orwithdrawal of the drug should be
taken.
FUROSEMIDE
Classification: Loop diuretic
Dosage/route: 40 mg BID, poMechanism of Action: Inhibits the
reabsorption of sodium and chloride from theascending limb of the
loop of Henle, leading to a sodium-rich diuresis.
Specific Indication: Furosemide is a "water pill" (diuretic)
that increases theamount of urine you make, which causes your body
to get rid of excess water.This drug is used to treat high blood
pressure. Lowering high blood pressurehelps prevent strokes, heart
attacks, and kidney problems. This medication alsoreduces
swelling/fluid retention (edema) which can result from conditions
such ascongestive heart failure, liver disease, or kidney disease.
This can help toimprove symptoms such as trouble breathing.
Contraindications: Contraindicated with allergy to furosemide,
sulfonamides;allergy to tartrazine (in oral solution); anuria,
severe renal failure; hepatic coma;pregnancy; lactation.
Side Effects: CNS: Dizziness, vertigo, paresthesias, xanthopsia,
weakness,headache, drowsiness, fatigue, blurred vision, tinnitus,
irreversible hearing loss
CV: Orthostatic hypotension, volume depletion, cardiac
arrhythmias,thrombophlebitis
Dermatologic: Photosensitivity, rash, pruritus, urticaria,
purpura,exfoliative dermatitis, erythema multiforme
GI: Nausea, anorexia, vomiting, oral and gastric irritation,
constipation,
diarrhea, acute pancreatitis, jaundice GU: Polyuria, nocturia,
glycosuria, urinary bladder spasm Hematologic: Leukopenia, anemia,
thrombocytopenia, fluid and
electrolyte imbalances, hyperglycemia, hyperuricemia Other:
Muscle cramps and muscle spasms
Nursing Precaution: Use cautiously with SLE, gout, diabetes
mellitus.
10
http://www.medicinenet.com/script/main/art.asp?articlekey=378http://www.medicinenet.com/script/main/art.asp?articlekey=12699http://www.medicinenet.com/script/main/art.asp?articlekey=1930http://www.medicinenet.com/script/main/art.asp?articlekey=42000http://www.medicinenet.com/script/main/art.asp?articlekey=378http://www.medicinenet.com/script/main/art.asp?articlekey=12699http://www.medicinenet.com/script/main/art.asp?articlekey=1930http://www.medicinenet.com/script/main/art.asp?articlekey=42000
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
11/31
Give early in the day so that increased urination will not
disturb sleep. Administer with food or milk to prevent GI upset.
Reduce dosage if given with other antihypertensives; readjust
dosage
gradually as BP responds. Measure and record weight to monitor
fluid changes.
CELECOXIB
Classification:Nonsteroidal Antiinflammatory drugMechanism of
Action: This medication is a nonsteroidal anti-inflammatory
drug(NSAID), specifically a COX-2 inhibitor, which relieves pain
and swelling(inflammation). It is used to treat arthritis, acute
pain, and menstrual pain anddiscomfort. Celecoxib is also used to
decrease growths found in the intestines(colon polyps) of persons
with a family history of this condition. This drug worksby blocking
the enzyme in your body that makes prostaglandins. Decreasing
prostaglandins helps to reduce pain and swelling.Dosage/route:
200 mg BID, poSpecific Indication: Celecoxib is licensed for use in
osteoarthritis, rheumatoidarthritis, acute pain, painful
menstruation and menstrual symptoms, and toreduce the number of
colon and rectal polyps in patients with familialadenomatous
polyposis. It was originally intended to relieve pain
whileminimizing the gastrointestinal adverse effects usually seen
with conventionalNSAIDs. In practice, its primary indication is in
patients who need regular andlong term pain relief: there is
probably no advantage to using celecoxib for shortterm or acute
pain relief over conventional NSAIDs. In addition, the pain
reliefoffered by celecoxib is similar to that offered by
paracetamol.[1]
Contraindications: Hypersensitivity including those in whom
attacks ofangioedema, rhinitis and urticaria have been precipitated
by aspirin, NSAIDs orsulfonamides. Severe hepatic impairment;
severe heart failure; inflammatorybowel disease; peptic ulcer;
renal impairment.Side Effects: The most common adverse effects are
headache, abdominal pain,dyspepsia, diarrhea, nausea, flatulence,
and insomnia. Other side effects includefainting, kidney failure,
heart failure, aggravation of hypertension, chest pain,ringing in
the ears, deafness, stomach and intestinal ulcers, bleeding,
blurredvision, anxiety, photosensitivity, weight gain, water
retention, flu-like symptoms,drowsiness and weakness.Nursing
Precaution:
History of GI bleeding; renal/hepatic insufficiency; asthma or
allergic disorders;hypertension; monitor haemoglobin or haematocrit
levels for signs of anaemia.History of cerebrovascular disease or
ischaemic heart disease.
11
http://www.medicinenet.com/script/main/art.asp?articlekey=9520http://www.medicinenet.com/script/main/art.asp?articlekey=7776http://www.medicinenet.com/script/main/art.asp?articlekey=7761http://en.wikipedia.org/wiki/Osteoarthritishttp://en.wikipedia.org/wiki/Rheumatoid_arthritishttp://en.wikipedia.org/wiki/Rheumatoid_arthritishttp://en.wikipedia.org/wiki/Acute_painhttp://en.wikipedia.org/wiki/Menstruationhttp://en.wikipedia.org/wiki/Familial_adenomatous_polyposishttp://en.wikipedia.org/wiki/Familial_adenomatous_polyposishttp://en.wikipedia.org/wiki/Non-steroidal_anti-inflammatory_drughttp://en.wikipedia.org/wiki/Paracetamolhttp://en.wikipedia.org/wiki/Celebrex#cite_note-Yelland-0http://www.medicinenet.com/script/main/art.asp?articlekey=20628http://www.medicinenet.com/script/main/art.asp?articlekey=1908http://www.medicinenet.com/script/main/art.asp?articlekey=24745http://www.medicinenet.com/script/main/art.asp?articlekey=1900http://www.medicinenet.com/script/main/art.asp?articlekey=24732http://www.medicinenet.com/script/main/art.asp?articlekey=370http://www.medicinenet.com/script/main/art.asp?articlekey=47466http://www.medicinenet.com/script/main/art.asp?articlekey=1945http://www.medicinenet.com/script/main/art.asp?articlekey=10419http://www.medicinenet.com/script/main/art.asp?articlekey=42321http://www.medicinenet.com/script/main/art.asp?articlekey=378http://www.medicinenet.com/script/main/art.asp?articlekey=24705http://www.medicinenet.com/script/main/art.asp?articlekey=496http://www.medicinenet.com/script/main/art.asp?articlekey=24720http://www.medicinenet.com/script/main/art.asp?articlekey=42985http://www.medicinenet.com/script/main/art.asp?articlekey=10049http://www.medicinenet.com/script/main/art.asp?articlekey=24750http://www.medicinenet.com/script/main/art.asp?articlekey=64119http://www.medicinenet.com/script/main/art.asp?articlekey=9520http://www.medicinenet.com/script/main/art.asp?articlekey=7776http://www.medicinenet.com/script/main/art.asp?articlekey=7761http://en.wikipedia.org/wiki/Osteoarthritishttp://en.wikipedia.org/wiki/Rheumatoid_arthritishttp://en.wikipedia.org/wiki/Rheumatoid_arthritishttp://en.wikipedia.org/wiki/Acute_painhttp://en.wikipedia.org/wiki/Menstruationhttp://en.wikipedia.org/wiki/Familial_adenomatous_polyposishttp://en.wikipedia.org/wiki/Familial_adenomatous_polyposishttp://en.wikipedia.org/wiki/Non-steroidal_anti-inflammatory_drughttp://en.wikipedia.org/wiki/Paracetamolhttp://en.wikipedia.org/wiki/Celebrex#cite_note-Yelland-0http://www.medicinenet.com/script/main/art.asp?articlekey=20628http://www.medicinenet.com/script/main/art.asp?articlekey=1908http://www.medicinenet.com/script/main/art.asp?articlekey=24745http://www.medicinenet.com/script/main/art.asp?articlekey=1900http://www.medicinenet.com/script/main/art.asp?articlekey=24732http://www.medicinenet.com/script/main/art.asp?articlekey=370http://www.medicinenet.com/script/main/art.asp?articlekey=47466http://www.medicinenet.com/script/main/art.asp?articlekey=1945http://www.medicinenet.com/script/main/art.asp?articlekey=10419http://www.medicinenet.com/script/main/art.asp?articlekey=42321http://www.medicinenet.com/script/main/art.asp?articlekey=378http://www.medicinenet.com/script/main/art.asp?articlekey=24705http://www.medicinenet.com/script/main/art.asp?articlekey=496http://www.medicinenet.com/script/main/art.asp?articlekey=24720http://www.medicinenet.com/script/main/art.asp?articlekey=42985http://www.medicinenet.com/script/main/art.asp?articlekey=10049http://www.medicinenet.com/script/main/art.asp?articlekey=24750http://www.medicinenet.com/script/main/art.asp?articlekey=64119
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
12/31
LACTULOSE
Classification: LaxativesMechanism of Action: Lactulose promotes
peristalsis by producing an osmoticeffect in the colon with
resultant distention. In hepatic encephalopathy, it reduces
absorption of ammonium ions and toxic nitrogenous compounds,
resulting inreduced blood ammonia concentrations.Dosage/route: 30
ml ODSpecific Indication: Used to treat
constipation.Contraindications: Galactosaemia, intestinal
obstruction. Patients on lowgalactose diet.Side Effects: This
medication may cause gas, belching or stomach cramps. Ifthese
effects continue or become bothersome, inform your doctor. Notify
yourdoctor if you develop any of these effects while taking this
medication: diarrhea,nausea, vomiting. If you notice other effects
not listed above, contact your doctoror pharmacist.
Nursing Precaution:Monitor electrolyte imbalance. Lactose
intolerance; diabetics.
Laboratory Exams:
Urinalysis Date: August 1, 2009,
Test Result SignificanceColor Yellow Normal
Transparency Clear NormalPus cells 10-21hpf Normal
RBC 5-12hpf NormalEpithelium Few NormalAmorphous Few Normal
Complete Blood Count Date: August 1, 2009
Test Result Normal Value SignificanceWBC 10,800 5,000-
10,000/mm
Increase infection,dehydration, leukemia,trauma polycythemia
vera
Hemoglobin 13.8 13.7-16.7 g/dl Hemoglobin is the main
transport of oxygen andcarbon dioxide in the blood.Hematocrit
38.7 40.5-49.7 vols% Increase in erythrocythosis,
dehydration and hemo-concentration associatedwith shock
Platelet Count Adequate 150,000- Platelets (also known
asthrombocytes) are the
12
http://www.medicinenet.com/script/main/art.asp?articlekey=331http://www.medicinenet.com/script/main/art.asp?articlekey=1900http://www.medicinenet.com/script/main/art.asp?articlekey=331http://www.medicinenet.com/script/main/art.asp?articlekey=1900
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
13/31
450,000/mm smallest formed elements ofthe blood. They are vital
tocoagulation of the blood toprevent excessive bleeding.
Differential Count
Lymphocytes 15 17.4-46.2% Depressed level mayindicate an
exhaustedimmune system.
Monocyte 3 4.3-10.3% Low levels are indicative of agood state of
health. .
Basophil 2.5 2-3% Basophilic activity is not fullyunderstood but
it is known tocarry histamine, heparin,and serotonin.
Blood Chemistry Date: August 1, 2009
Test Result Normal Value SignificancePhosphorus 5.43
2.50-50.0mgs/dL Metastatic neoplasm to bonePotassium 6.0
3.5-5.5mEq/L Increase excess IV
administration, Potassium-sparing diuretics,
infection,dehydration, acidosis, bloodtransfusion, burns and
trauma
Glucose 422.7 60.00-110.0 Diabetes MellitusSodium 150.6
135-145mEq/L Increase dietary or IV intake
DI, Cushings syndrome,
increase swating.
Blood Chemistry Date: August 1, 2009
Result Normal Value SignificanceCalcium 4.03 8.10-
10.40mmol/L
Acute pancreatitis, nephrosis,
Creatinine 2.93 0.6-1.1 mg/dL Increase renal failure,muscular
dystrophy,hyperthyroid, acromegaly,rhabdomyolysis
Chest X-RAY Date: August 2, 2009
ImpressionCardiomegaly, LV form
HEArt enlarged
13
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
14/31
Pulmonary congestion
Minimal Pleural effusion, bilateral
Atherosclerosis aorta
Fracture left clavicle and left 8 th posterior rib
ULTRASOUND Date: August 2, 2009
Liver and GallbladderImpression:
Contracted liver
Gall stone with sludge
Ascites Minimal
V. ANATOMY AND PHYSIOLOGY
The Skeletal System serves many important functions; it provides
theshape and form for our bodies in addition to supporting,
protecting, allowingbodily movement, producing blood for the body,
and storing minerals.
Its 206 bones form a rigid framework to which the softer tissues
andorgans of the body are attached. Vital organs are protected by
the skeletal
14
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
15/31
system. The brain is protected by the surrounding skull as the
heart and lungsare encased by the sternum and rib cage.
Bodily movement is carried out by the interaction of the
muscular and skeletalsystems. For this reason, they are often
grouped together as the musculo-
skeletal system. Muscles are connected to bones by tendons.
Bones areconnected to each other by ligaments. Where bones meet one
another istypically called a joint. Muscles which cause movement of
a joint are connectedto two different bones and contract to pull
them together. An example would bethe contraction of the biceps and
a relaxation of the triceps. This produces abend at the elbow. The
contraction of the triceps and relaxation of the bicepsproduces the
effect of straightening the arm.
The Ribs
The ribs are thin, flat, curved bones that form a protective
cage around theorgans in the upper body. They are comprised 24
bones arranged in 12 pairs.
The first seven bones are called the true ribs. These bones are
connected to thespine (the backbone) in back. In the front, the
true ribs are connected directly tothe breastbone or sternum by a
strips of cartilage called the costal cartilage. Thenext three
pairs of bones are called false ribs. These bones are slightly
shorterthan the true ribs and are connected to the spine in back.
However, instead ofbeing attached directly to the sternum in front,
the false ribs are attached to the
lowest true rib. The last two sets of rib bones are called
floating ribs. Floating ribsare smaller than both the true ribs and
the false ribs. They are attached to thespine at the back, but are
not connected to anything in the front. The ribs form akind of cage
the encloses the upper body. They give the chest its familiar
shape.
15
http://www.mnsu.edu/emuseum/biology/humananatomy/skeletal/joints.htmlhttp://www.mnsu.edu/emuseum/biology/humananatomy/skeletal/ribs/trueribs.htmlhttp://www.mnsu.edu/emuseum/biology/humananatomy/skeletal/ribs/falseribs.htmlhttp://www.mnsu.edu/emuseum/biology/humananatomy/skeletal/ribs/floatingribs.htmlhttp://www.mnsu.edu/emuseum/biology/humananatomy/skeletal/joints.htmlhttp://www.mnsu.edu/emuseum/biology/humananatomy/skeletal/ribs/trueribs.htmlhttp://www.mnsu.edu/emuseum/biology/humananatomy/skeletal/ribs/falseribs.htmlhttp://www.mnsu.edu/emuseum/biology/humananatomy/skeletal/ribs/floatingribs.html
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
16/31
The Shoulder Girdle
The Shoulder Girdle, also called the Pectoral Girdle, is
composed of fourbones: two clavicles and two scapulae .
The clavicle, commonly called the collarbone, is a slender
S-shaped bonethat connects the upper arm to the trunk of the body
and holds the shoulder jointaway from the body to allow for greater
freedom of movement.
PATHOPHYSIOLOGY
16
http://www.mnsu.edu/emuseum/biology/humananatomy/skeletal/shoulder/clavicle.htmlhttp://www.mnsu.edu/emuseum/biology/humananatomy/skeletal/shoulder/clavicle.html
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
17/31
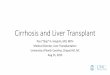
Predisposing Factor Precipitating
Age (79 y.o)Liver cirrhosisDiabetes Mellitus
Unsafe externalenvironment
Body malaise,dyspnea, pain
Fall (4 steps stairs)
Rib fracture,clavicle frature
Impaired tissueperfussion
Increase bloodglucose level
Renin-angitensin-Aldosterone-system
activation
Liver unable to synthesizeprotein/amino acid
Low fat absorption
Low protein absorption
Pleural infusion
PAIN
Impaired
oxygenation
17
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
18/31
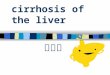
NURSING ASSSESSMENT (System Review Chart) Date: August
2,2009
Age (79 y.o)Liver cirrhosisDiabetes Mellitus
Unsafe externalenvironment
Body malaise,dyspnea, pain
Fall (4 steps stairs)
Rib fracture,clavicle frature
Impaired tissueperfussion
Increase bloodglucose level
Renin-angitensin-Aldosterone-system
activation
Increase sodium andwater retention
Liver unable to synthesizeprotein/amino acid
Low fat absorption
Low protein absorption
Fluid shifting to secretion
Pleural infusion
PAIN
Impairedoxygenation
Aldosterone secretion
Water and sodiumretention
EDEMA
18
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
19/31
EENT:[ ] Impaired vision [ ] blind[ ] pain redden [ ] drainage[
] gums [ ] hard of hearing [ ] deaf[ ] burning [ ] edema [ ] lesion
teeth[ ] assess eyes ears nose[ ] throat for abnormality [x] no
problem
RESP:[ ] Asymmetric [x] tachypnea [ ] barrel chest[ ] apnea [ ]
rales [ ] cough[ ] bradypnea [ ] shallow [ ] rhonchi[ ] sputum [ ]
diminished [x ] dyspnea[ ] orthopnea [ ] labored [ ] wheezing[ ]
pain [ ] cyanotic[ ] assess resp. rate, rhythm, depth, pattern,
breath sounds, comfort [ ] no problem
CARDIOVASCULAR:[ ] arrhythmia [ ] tachycardia [ ]numbness[ ]
diminished pulses [ ] edema [] fatigue[ ] irregular [ ] bradycardia
[ ] murmur[ ] tingling [ ] absent pulses [ ] pain[ ] Assess heart
sounds, rate rhythm, pulse, blood
pressure, circ., fluid retention, comfort[ x ] no problem
GASTROINTESTINAL TRACT:[ ] obese [ x ] distention [ ] mass[ ]
dysphagia [ ] rigidity [ ] pain[ ] assess abdomen, bowel habits,
swallowing[ ] bowel sounds, comfort [ ] no problem
GENITO URINARY AND GYNE[ ] pain [ ] oliguria [ ] color [ ]
vaginal bleeding[ ] hematuria [ ] discharge [] nocturia[x ] assess
urine frequency, control, color, odor, comfort[ ] gyne bleeding [ ]
discharge [ x ] no problem
NEURO:[ ] paralysis [ ] stuporus [ x ] unsteady [ ] seizure[ ]
lethargic [ ] comatose [ ] vertigo [ ] treamors[ ] confused [ ]
vision [ ] grip[ ] assess motor, function, sensation, LOC,
strength[ ] grip, gait, coordination, speech [x] no problem
MUSCULOSKELETAL and SKIN:[ ] appliance [ ] stiffness [ ] itching
[ ] petechie[ ] hot [ ] drainage [ ] prosthesis [x] swelling
[ ] lesion [ ] poor turgor [ ] cool [ ] flushed[ ] atrophy [x]
pain [ ] ecchymosis [ ] diaphoreticmoist[ ] assess mobility, motion
gait, alignment, joint function[ ] skin color, texture, turgor,
integrity[ ] no problem
Name: C.B.P.BP: 140/80 mmHg T: 36.6C PR: 85 bpm RR: 22 cpm
Height: 52inches Weight:
NURSING ASSESSMENT IISUBJECTIVE OBJECTIVE
19
Swelling/edema
Pitting Edema (grade 1)
Adbominal distention
Wound
Dry skin
Generalized Weakness
Edema
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
20/31
COMMUNICATION:
[ ] hearing difficulty
[] visual changes
[x ] denied
Comments:"dili na kyosiya ka-klaro pero sigetanaw og tv as
verbalized by watcher
[ ] glasses [ ] languages
[ ] contact lenses [ ] hearing difficulties due to age
[ ] speech difficultiesPupil size:R:3 mm L:3mm
Reaction: PERRLA (Pupil Equally Round andReactive to Light
Accommodation)
OXYGENATION:
[x ] dyspnea
[ ] smoking history
[] cough
[ ] sputum
[ ] denied
Comments: lisud auiginhawa, asverbalized by thepatient.
Resp. [x ]regular [] irregular
Describe: RR is regular and it is within range.
R: unsymmetrical to the left lung
L: unsymmetrical to the right lung
CIRCULATION:
[ ] chest pain
[ ] leg pain
[] numbness of
extremities
[x ] denied
Comments: wala manko ing ana ngaproblema ang akungtiyan lang ang
sakit ogayo , as verbalized bypatients watcher.
Heart Rhythm [x] regular [ ] irregular
Ankle Edema: ankle edema is present on bothextremities
Pulse Car Rad. DP Fem
R + 85bpm + +____
L + + + +____Comments: Pulse on all sites are palpabale yet
weakon the radial and dorsalis pedis areas due topresence of
edema.
NUTRITION:
Diet: Soft diabetic
Character
[x] recent change in
weight
[] swallowing
Difficulty
[ ] denied
Comment: Gamay ralagi iyang gaka-on amolang luguson kydaghan bya
syatambal,as verbalized
by watcher.Ganiwang na ganisiya as verbalized bythe watcher
[ ] dentures [ x ]none
Full Partial With patient
Upper [ ] [ ] [ ]
Lower [ ] [ ] [ ]
20
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
21/31
ELIMINATION:
Usual bowel pattern:
Once a day
[ ] constipation
remedy______None______
Date of last BM
August 1, 2009
[ ] diarrhea
-______None________
[x] urinary frequency
In foley catheter
[ ] urgency
[ ] dysuria[ ] hematuria
[ ] incontinence
[ ] polyuria
[ ] foley in place
[ ] denied
Comments:Patientsbowel soundsauscultated and shehas an
audiblenormoactive.
Bowel sounds Audiblenormoactive bowel soundsevery 10-15 sec.
Abdominal Distention
Present [x ] yes [] no
Urine* (color, consistency,odor)
____amber or strong______
Foley if they are in place:Foley bag catheter in place
MGT. OF HEALTH & ILLNESS:
[ ] alcohol [x] denied
(amount/frequency)
[ ] SBE: Not recalled Last Pap Smear: NOT
RECAlled
LMP: Not recalled
Briefly describe the patients ability to followtreatments (diet,
meds, etc.) for chronic healthproblems (if present).
Patient is able to follow treatments, such as hermedications and
soft diabetic diet as prescribe by thephysician during this
admission but her maintenancefor her liver cirrhosis she stop it
because ofinconvenience during her follow up check up atCebu.
SUBJECTIVE OBJECTIVE
SKIN INTEGRITY:
[x ] dry
[ ] other
[] denied
Comments: dry lagi iyangpanit na basin sapagkatigulang na,
asverbalized by the watcher
[x ] dry [ ] cold [x ] pale
[ ] flushed [ ] warm
[ ] moist [ ] cyanotic
*rashes, ulcers, decubitus (describe size,
location, drainage: Healing woung at leftleg.
ACTIVITY/SAFETY:
[ ] convulsion
[ ] dizziness
Comments: Dili kayo laginiya malihok iyang abagaog likod, as
verbalized bythe watcher.
[ ] LOC and orientation Patient is orientedto time, place,
events and person.
Gait: [ ] walker [ ] cane [ ] other
21
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
22/31
[x ] limited motion of
Joints
Limitation in
Ability to
[] ambulate
[ ] bathe self
[ ] other
[ ] steady [x ] unsteady
[ ] sensory and motor losses in face or
extremities No sensory and motor losseson face or
extremities
[x] ROM limitations: she can move but withlimitation and with
accompany.
COMFORT/SLEEP/
AWAKE:
[] pain
(location,frequencyremedies)
[ ] nocturia
[x] sleep difficulties
[ ] denied
Comments: Dili kayo siyakatulog kay galisod siyaog ginhawa,
asverbalized by the watcher
[] facial grimaces
[x] guarding
[ ] other signs of pain :
Patient was able to manage the painwithin tolerable limit.
COPING:
Occupation: Housewife
Members of household: 5 members ofhousehold
Most supportive person: her five children
Observed non-verbal behavior: weaknessor fatigue
Phone number that can be reachedanytime:
Confidential
SPECIAL PATIENT INFORMATION
_Not ordered Daily weight ____N/A___ PT/OT
_140/80 mmHg BP q shift ____N/A___Irradiation
___not ordered__ _Neuro vs August 1, 2009 Urine test
____N/A_ _CVP/SG Reading not ordered 24 hour UrineCollection
22
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
23/31
VII NURSING MANAGEMENT
A. Ideal Nursing Management
Diagnoses: Ineffective Breathing Pattern related to respiratory
muscleweakness.
Intervention Rationale Investigate etiology of
respiratory failure.
Observe over-all breathingpattern.
Auscultate chest noting thepresence or absence of
breathsounds.
Count clients respiration 1 fullminute and compare with
desireset rate.
Check tubing of oxygen forobstruction.
To understand the underlying cause.
To attempt to correct the deficiency byover breathing.
To note the frequent crackles thatdoesnt clear with
coughing.
Respirations vary depending onproblem requiring
ventilatoryassistance.
Kinks in tubing prevent adequatevolume of delivery.
Diagnoses: Acute Pain related to injury to the soft
tissueIntervention Rationale
Maintain immobilization ofaffected area.
Elevate and support injuredextremities.
Avoid use of plastic sheets.
Evaluate reports ofpain/discomfort.
Identify any diversionalactivities.
Apply cold/ice pack.
Relieves pain and prevent extensionof the injury.
Promotes venous return.
Promotes discomfort
Monitor effectiveness of intervention.
Prevents boredom, reduces muscletension.
Reduces edema.
23
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
24/31
Diagnoses: Activity intolerance related to generalized
weakness
Intervention Rationale Adjust activities and reduce
intensity level or discontinue
activities that cause undesired
physiologic changes.
Increase exercise and activity
level gradually.
Plan care with rest periodsbetween activities.
Assist with activities and provide
client used of assistive devices.
Promote comfort measures and
provide for relief of pain.
Provide positive atmosphere
while acknowledging difficulty of
the situation for the client.
To prevent over excretion.
To conserve energy
To reduce fatigue
To protect the client from injury
To promote comfort measures and
provide for relief of client.
Helps to minimize frustration, reduce
channel energy.
Diagnoses: Risk for ineffective peripheral Tissue Perfusion
Intervention Rationale
Provide air mattress, sheepskinpadding, bed/foot cradle.
Apply ice and elevate lowerextremities.
Administer physicians order ofmedication.
To protect the extremities.
To reduce edema.
To give comfort and reduce edema.
24
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
25/31
Apply ace bandage to lowerextremities before arising
frombed.
To prevent venous stasis
B. Actual Nursing Management
S Lisud au iginhawa as verbalized by the patient.
O Dyspnea Changes in rate and depth of respirations Increased
restlessness
A Ineffective Breathing Pattern related to respiratory muscle
weakness.
P At the end of 2-3 minutes, the patient will maintain
respiratory
pattern.
IIndependent Maintained in moderate to high back rest. Checked
tubing for obstruction. Observe over-all breathing pattern
Dependent
Set Oxygen at 3L/min
EAt the end of 2 minutes, the patient maintains her respiratory
pattern.
25
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
26/31
S sakit lagi iyang abaga og likod as verbalized by the
patient.
O
Restlessness Facial grimace Guarding the affected part.
A Acute pain related to injury to the soft tissue
P At the end of 15-30 minutes the patient will able to
verbalized pain
into tolerable level
IIndependent
Reinforced position (semi-fowlers) to the patient. Encouraged
adequate rest periods
Reviewed ways to lessen pain, including techniques.
Discuss with significant others ways in which they can assist
the
client in activities.
Dependent
Administer medication for pain.
Celecoxib 200mg BID
EAt the end of 30 minutes the patient was able to response
tointerventions and verbalized relief of pain.
26
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
27/31
SDili kayo lagi niya malihok iyang abaga og likod busa dili kayo
siya
kalihok as verbalized by the watcher
O Weakness. Inability to begin activity
A Activity Intolerance related to generalized weakness
P At the end of 8 hours, the patient will be able to have
gradual
return to physical movement and mobility
IIndependent Encouraged patient to do bed exercises such as arm
exercises
abduction and external rotation of shoulder, hand and
fingers
exercises and foot exercises. Assisted patient in activities
that begins by sitting at the side of
the bed and in chair.
Assisted early ambulation of patient.
Assisted patient to performed ADL with involvement of
significant
others.
Provided physical support and maintained patients safety.
EAt the end of 8 hours, the patient was able to demonstrate
gradual
return to physical movement and mobility within tolerance as
evidenced by increasing ambulation and participation in
personal
care activities.
27
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
28/31
VIII. REFERRALS AND FOLLOW-UP
28
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
29/31
IX. EVALUATION AND IMPLICATION
MEDICATIONS
The patient was instructed to continue medications
namely Kalimate 2 sachets TID, Sodium
Bicarbonate 650mg TID, Lactulose 30ml OD,
Celecoxib 200mg BID, ITOPRIDE 50mg TID,Pancreatin I tab TID
She and her significant others was advised to
comply all the medications needed as prescribed by
the physician.
Patient and significant others was instructed aboutthe proper
administration of medications accordingto right dose, right time
and right route, and becautious to possible side effects.
EXERCISEEncourage Range of Motion Exercises
TREATMENT
Follow medication as prescribed by the physician. Turn to sides
every two hours. Provide footboard.
Maintained moderate to high back rest.OUTPATIENT
(Check-up)
The patient is advised to have her follow-up check-up oneweek
after at Cagayan de Oro Medical Center, Building 1,
2nd
Floor at the clinic of Dr. Chang.
DIET
Encourage patient to eat foods rich in Vit. C like fruits
toenhance the immune system.Encourage patient to increase fluid
intake to maintain fluidand electrolyte balance in the body.
29
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
30/31
PROGNOSTIC INDICATORS POOR GOODA. Onset of illness B. Duration
of illness C. Precipitating factors D. Attitude and willingness to
take
medication
E. Family support
After having interacted with the client for 2 days and rendered
nursing
interventions, we therefore concluded that our objectives were
met. Also based
on thorough observation and data gathered, we had identified
that the client has
a poor prognosis since she is too old to recover from her
illness and she had
experienced many complications. Although the family support
system towards
the client is good, we still encourages the family to continue
on supporting the
medical and emotional support of the client in gearing towards
hospitalization
and consultation. They are encouraged to be sensitive to the
needs and care of
the patient since she is old. We implied for a continue support
system towards
the client and be cautious if theres any complains from the
client or any signs of
another health problems.
B. BIBLIOGRAPHY
Kozier, B. et al. Fundamentals of Nursing, 7 th ed. Singapore:
Pearson
Education South Asia PTE LTD, 2004
30
-
8/6/2019 204 GYNE Fracture Liver Cirrhosis DM
31/31
Lippincott. Nursing 2007 Drug Guide, PA: Lippincott Williams
& Wilkins,
2007 Phipps, et al. Medical-Surgical Nursing: Concepts and
clinical
Practice, vol. 1, 5th ed Missouri: Mosby-Year Book, Inc.,
1995
MIMS Philippines, 109th ed. CMPMEdica, 2006
Tortora, G.J.& Grabowski S.R.; Principles of Anatomy and
Physiology; 10th
Edition; John and Wiley and Sons, Inc.; 2003.
Karch, Amy M.; Focus on Nursing Pharmacology; 3 rd Edition;
Lippincot
Williams and Wilkins; 2006.
Doenges, E.M., Moorhouse, M.F. Geisslerr-Murr, A.C.; Nurses
Pocket
Guide Diagnoses, Interventions and Rationales; 9th Edition; F.A.
Davis
Company Philadelphia; 2004.
![Advantages and Disadvantages of Hyperbaric Oxygen ... · to liver cirrhosis or hepatocellular carcinoma [3–5]. Although the elucidation of the mechanism behind ... Hyperbaric oxygen](https://img.pdfslide.tips/doc/110x75/5f522f31aa2a293a3d75b4a5/advantages-and-disadvantages-of-hyperbaric-oxygen-to-liver-cirrhosis-or-hepatocellular.jpg)