Embed Size (px)
Citation preview

EUROPEAN HOSPITAL���������������� �������������������������������������������� !
������� ���
������������������������� ����� ��
�������������������������� ������������������
����������������� ����
���������������������� ���� �����������
�������������������������� !�"#�$%��"
News & Management . . . . 1-4
Radiology & IT . . . . . . . . . . 5-9
Hygiene . . . . . . . . . . . . . . 10-11
Cardiology . . . . . . . . . . . . . . 12cont
ents
T H E E U R O P E A N F O R U M F O R T H O S E I N T H E B U S I N E S S O F M A K I N G H E A L T H C A R E W O R K
War casualtiesUK - In preparation for war, sixNational Health Service (NHS)military hospitals and over 30NHS hospitals are said to be onalert to receive injured personnelflown back from field hospitals.6,000 casualties are predicted inthe first four days of battle.
Civilian deaths About 35 people are killed everyhour as a direct result of war(source: WHO) In the 20thcentury, about 191 million peopledied directly or indirectly due toarmed conflict. Most werecivilians.
TV soap hits labsUK - 14,000 additional cervicalsmear tests were performed inManchester and the nation’sCancerBACUP helpline alsoreceived 300 extra weekly calls,after a TV soap actress played acancer victim who died. In lettersto the British Medical Journal,researchers suggested greaterresponsibility in the media.
Intensive care . . . . . . . . . 13-15Urology . . . . . . . . . . . . . . 16-17Company news, awards . . . 19& innovationsGlobal events & nutrition . . 20
16-17Urology
Remote controlsurgery,
imaging anda new
kidney test
IN BRIEF
13-15Intensive care
Medical air,e-monitoring andthe international
symposium
GENEVA - Fivegroups represent-ing healthcareprofessionalsare urginggovernments tofind non-violentand democraticmeans to resolveconflicts and bringabout peace. Theyinclude the WorldMedical Association(WMA), a globalfederation ofnational medicalassociations,representing
millions of physicians worldwide; the InternationalCouncil of Nurses, a federation of 124 national nurses’associations representing millions of nurses; theInternational Confederation of Midwives, comprisedof 83 national midwifery associations from 70countries; The World Confederation for PhysicalTherapy, comprised of national physio associationsfrom 83 countries, representing 250,000+physiotherapists, and the FDI World DentalFederation, with over 150 national dental associ-ations and 700,000 dentists.
In a press release, the groups point out that thehealth consequences of even ‘conventional’ war areborne overwhelmingly by civilians, with particularlycatastrophic effects on women and children’sphysical and mental health. Death and debilitatinginjury are coupled with threatened access to safewater, sanitation and food, undermining the healthof a population and creating circumstancesfavourable to epidemic diseases. Details: www.icn.ch
5-9Radiology
The 3-Dembryonicheart, plus
imaging -the future
continued on page 2
10-11Hygiene
Surveillance,prophylaxis,
Legionnaire’stest kit etc
V O L 1 2 I S S U E 1 / 0 3 F E B R U A R Y / M A R C H 2 0 0 3
CHINA - Fear of another ‘killer’ fluepidemic arose this month whenHong Kong’s Department of Healthconfirmed that a man, who died inhospital there, had a new viral strainof influenza A(H5N1)- which is avianin origin. The victim’s 9-year-old sonalso tested positive for the same viralstrain, but has since recovered, as hashis mother. The family had visited theFujian Province (China) in January,where another family member, aged8, died this month.
The spectre of the pandemics of1957 and 1968 again rose. In thoseperiods two million people died of aparticularly virulent influenza.
Laboratory tests have shown thatthe genes of the A(H5N1) virus arepurely avian (i.e. without any humangene content). Dr Yeoh Eng-kiong,Secretary for Health, Welfare andFood, urged the public to keep calm,and stressed that the Government hasstepped up its surveillance system and
Will you become aglobal radiologist?
COVE
R PH
OTO
S:M
ARY
PARG
ETER
comprising heightened farm bio-secu-rity, stringent hygienic practices andan effective surveillance system,should minimise risk, he said.
Some poultry have been destroyedand various rules have been set tocover hygiene and poultry sales. DrYeoh added that officials are studyingthe feasibility of vaccinating importedlive poultry to reduce the bird-flu risk.But he also predicted that, in theabsence of human genes in the virus,the risk of human-to-human transmis-sion will be low, but Dr Yeoh expectsmore sporadic cases of avian flu, asthe virus is endemic to the area.However, the Department of Healthin Hong Kong has reported no unusu-al increase in influenza activity duringthe past few weeks.
Further laboratory tests, includinggene sequencing, are being conducted,and epidemiological investigations arecontinuing to find the source of thisinfection. The World HealthOrganisation is in close contact withthe health authorities in Beijing andHong Kong. The WHO GlobalInfluenza Surveillance Network hasbeen alerted and additional reagentsfor laboratory diagnosis are beingmade available to National InfluenzaCentres and other Members of theGlobal Influenza SurveillanceNetwork.
will enhance liaison with Mainlandauthorities on ways to reduce therisk of the outbreak of infectiousdiseases. Dr Yeoh added thatalthough the trade has been co-operative, a multi-pronged strategy,
For some years, while Europeans have slept, elec-tronic banking and other systems have been ser-viced online and overnight by technicians work-ing in different time zones, such as India. Theconcept is good, for it keeps the wheels of indus-try turning and shares revenues with other,perhaps poorer countries. Obviously, astelemedicine develops, this is having,and will have, an ever-increasingeffect on how we deliver healthcare.
For now, everyone is fascinated bythe implications and complications ofcross-border healthcare, in whichpatients move to other EU countries fortreatments, with payments reimbursed bytheir own. But how about patients staying put,and their medical files doing the travelling, notonly in the EU, but to far-off places such asAustralia, Israel and the Far East for diagnoses?
This has already occurred with tele-radiology.In the US, where there is a shortage of radiolo-gists, hospitals have been transmitting com-pressed images to Australia and India, for initialdiagnoses. Again the concept is good, in that staffshortages and night emergencies can be bettercovered, and workflow speeded up. Readingsaccomplished overnight can be presented atmorning ward rounds. Ultimately the system
Medics against war!
could shorten the length of stay for in-patients. Although online radiology firms mushroomed,
not all have been successful, but now, a new con-cept, from the Massachusetts General Hospital,Boston, may set the standard for this type of out-
sourcing. The plan is aimed at advancingpatient care as well as the hospital’s role
in teaching and research - i.e. to alsoadvance aspects of radiology andpatient care in India. Initially the tel-eradiology centre - based in Bangaloreand set up with the help of Wipro GE
Medical Systems, with PACS from AgfaHealthCare, and with the close involve-
ment of an Indian university - is to have US-trained staff who will relocate to Bangalore.Following this, Indian radiologists will beemployed and receive advanced US training.
The PACS system will enable access to a fullpatient case history.
When the centre is fully operational, theBoston hospital may then offer services to otherhealthcare services. For European this could be ofconsiderable value in terms of overnight readings- and with quality set by the ‘mother’ hospital.
All well and good, except for criticism fromsome radiologists that the plan will affect employ-
New HFN1 virus puts WHO on alert
Email youropinions!
[email protected] want to hear fromEuropean radiologistsabout the implications
of cross-nationsteleradiology
Anti
War
dem
onst
raio
n,th
e Ce
nota
ph,L
ondo
n

2 EUROPEAN HOSPITAL Vol 12 Issue 1/03
N E W S
Funding healthcareNew options and choices for patientsUSA - In the era of soaring healthcosts and the inability of healthmaintenance organisations to effec-tively control those costs withouttightening restrictions on the con-sumer end, Americans are now fac-ing new options in which they gainmore flexibility to determine thetype of care they receive. So-calledConsumer Directed Health Plansare now an option with whichemployees are increasinglypresented.
How they work: Employers setaside a fixed amount of moneyannually, which employees can putinto a healthcare account.Although the employer owns theaccounts this money can be used
by the employee to cover health-care costs that may arise. Whileconventional health plans placetight restrictions by limiting theproviders that can be seen, thesenew health plans allow for agreater choice. Alternative medi-cine, not usually covered by tradi-tional insurance policies, can bereimbursed using the accounts.
Another benefit of ConsumerDirected Health Plans is that themoney set aside by the employeecan roll over into the next year.Additionally, the money not taxed,since it is taken out before SocialSecurity Tax.
A disadvantage of the ConsumerDirected Health Plan is that a
change in job will not permit theemployee to transfer the funds.This is not the case with anothersystem, the Medical SavingsAccounts. These are similaraccounts, set up by the FederalGovernment. They also ask theemployee to take responsibility forhis own healthcare by setting asideamounts into an account ownedby the employee. However, in con-trast to the Consumer DirectedHealth Plan, these can move withthe person, and will not be wastedshould a change in company occur.Although they look attractive,there is a hook: the employeeneeds to provide proof of coveragethrough a catastrophic healthinsurance, be self-employed, orbelong to a small company. Thesetight restrictions by the FederalGovernment make it very difficultfor most consumers to actuallyqualify.
FSA’s, Flexible SpendingAccounts, are yet another optionin which employee can set asidepart of their pay, but again, theaccounts do not move.
While it is too early to say thereis a trend in the US, ‘... there is agreat deal of interest in greaterchoice,’ says Larry Akey,spokesman of the HIAA, a health-care organisation that managesthese accounts. ‘There is a sense inthe industry that this will be thefuture, and a recognition that themanaged care efforts of the 1990’s- where employers ask HMOs totightly control costs, who thenanswer by restriction of choice -are becoming increasinglyunfavourable,’ he adds.
US consumers no longer want toparticipate in tightly regulatedplans. They want to becomeincreasingly involved in the finan-cial decision-making process con-cerning their healthcare. Perhapsthe future in the US will see areturn to the partial indemnityplans prevalent during the 1970’s.
Karen Dente: EH US correspondent
Meanwhile ...who can heal sick healthcare?Writer offers $10,000 prize to find a cureOver 40 million US citizens lack health insurance; in Washington State this is true for
about 11% of residents, for whom treatment may be denied, because some doctorsconsider Medicaid reimbursements too low. Those are only two of the many dire
problems afflicting US healthcare provision.‘We don’t have a health care system. We have a business-to-business enterprise,’
says Kathleen O’Connor MA, Seattle-based healthcare consultant, analyst and well-known local columnist. ‘Our “system” is a mess and in an irreparable crisis. Something
must be done, so we are putting our money where our mouth is. Healthcare is toooften held hostage to armed camps and special interests. So we are sponsoring anindependent contest to see if we can get different results by engaging the public.’
On offer is a $10,000 prize for the best proposal toimprove her country’s healthcare services. This she
hopes will provide a transfusion of ideas and promptdiscussion that may lead to reform. The top three
entries will be announced at The O’ConnorReport ‘Build an American Health
System’ Summit (October2003) and will be presented
to the Washington StateCongressional Delegation.
Details: www.oconnorhealthanalyst.com/contest.html
ment, pay levels and have issues toresolve regarding remuneration,insurance cover, the acceptability ofqualifications, confidentiality, andlegal positions in cross-nation med-ical services.
In Europe teleradiology has alsoadvanced. For example, in Swedenand Norway there is also a shortageof radiologists. In 2001, Sectra, theinternational IT and medical tech-nology firm, formed PaxLink AB.Images and patient data are trans-mitted for diagnosis by qualifiedradiologists at the Orebro MedicalCentre Hospital, a service that nowcovers both countries when there arestaff shortages or by contract.
Recently, Sectra (which has alsodeveloped the digital MicroDoseMammography system) also agreedto provide RIS and PACS for CapioDiagnostik, a private Swedishhealthcare provider. Capio, withclinics carrying out up to 130,000radiological examinations annually,will pay Sectra for each examina-tion. Capio Diagnostik is part of theCapio Group, offering medical ser-vices in Sweden, Norway, Denmark,Finland, UK, France, Switzerlandand Poland.
In time, Sectra’s services will prob-ably be offered to countries outsideScandinavia.
continued from page 1
ENTRY COUPONFAX TO: EUROPEAN HOSPITAL, +49-211-7357-530PLEASE ACCEPT MY REQUEST FOR A FREE SUBSCRIPTION TO EUROPEAN HOSPITAL
Name
Job title
Hospital/Clinic
Address
Town/City Country
Phone number Fax
Now, tell us more about your work, so that we can plan future publications with your needs in mind.Please put a cross ✘ in the relevant boxes.
1. SPECIFY THE TYPE OF INSTITUTION IN WHICH YOU WORK
� General hospital � Outpatient clinic � University hospital
Specialised hospital/type
Other institution (eg medical school)
2.YOUR JOB
� Director of administration � Chief medical director � Technical director
Chief of medical department/type
Medical practitioner/type
Other/department
3. HOW MANY BEDS DOES YOUR HOSPITAL PROVIDE
� Up to 150 � 151-500 � 501-1000 � more than 1000
� None, (not a hospital/clinic)
4 . WHAT SUBJECTS INTEREST YOU IN YOUR WORK?� Surgical innovations/surgical equipment � Radiology, imaging/high tech advances� Clinical research/treatments/equipment � Intensive Care Units/
management/equipment� Ambulance and rescue equipment � Pharmaceutical news � Physiotherapy updates/equipment � Speech therapy/aids� Nursing: new aids/techniques � Laboratory equipment, refrigeration, etc.� Hospital furnishings: beds, lights, etc. � Hospital clothing and protective wear� Hygiene & sterilisation � Nutrition and kitchen supplies� Linens & laundry � Waste management� Information technology & digital communications � Hospital planning/logistics� Personnel/hospital administration/management � Hospital Purchasing� Material Management � Medical conferences/seminars� EU political updatesOther information requirements - please list
ESPECIALLY FOR DOCTORS:Please complete the above questions and we would like you to answer the following addi-tional questions by ticking yes or no or filling in the lines as appropriate.
What is your speciality?
In which department do you work?Are you head of the department? � Yes � NoAre you in charge of your department’s budget? � Yes � No
How much influence do you have on purchasing decisions?I can only present an opinion � Yes � NoI tell the purchasing department what we need � Yes � NoI can purchase from manufacturers directly � Yes � No
Do you consider that your equipment isout-dated � Yes � Norelatively modern � Yes � Nostate-of-the-art � Yes � No
Do you use/buy second-hand equipment? � Yes � NoIf so, what do you use of this kind?
Is your department linked to an internal computer network? � Yes � NoIs your department linked to an external computer network? � Yes � NoIs your department involved with telemedicine in the community? � Yes � NoDo you consider your department is under-staffed? � Yes � NoAre you given ample opportunities to up-date knowledge? � Yes � NoDo you attend congresses or similar meetings for your speciality? � Yes � No
This information will be used only in an analysis for European Hospital, Höherweg 287, 40231 Düsseldorf, Germany, andfor the mailing out of future issues of the Beta publication European Hospital. Candidates will also be automaticallyentered for a draw to win the prize featured on this page.
EUROPEAN HOSPITALReader Survey
EH 1/03
✂
YOU may qualify for a FREE subscription toEUROPEAN HOSPITAL, the bi-monthly journalserving hospitals throughout the EU.* If selected, you will be sent a copy ofEUROPEAN HOSPITAL every three monthsAND you will have a chance to win our
splendid prize (see below) because yourname will be entered for the draw.
To participate, simply fill in this coupon and fax to:+49 211 73 57 530No fax? No problem. Please post your coupon to: EuropeanHospital Verlags GmbH, Höherweg 287, D-40231 Düsseldorf
EUROPEAN HOSPITAL���������������� �������������������
������������������������� !
������� ���
���������
�������
��������
�
����� �
�
��������
�����������
������
� �������
�������
����
�������
�������
��� ���
�
��������
����������
��
�� ����
��������
���
���������
���������
��������
!�"#�$%��
"
News & Management . . . . 1-4
Radiology & IT . . . . . . . . . . 5-9
Hygiene . . . . . . . . . . . .
. . 10-11
Cardiology . . . . . . . . . . . .
. . 12
cont
ents
T H E E U R O P E A N F O R U M F O R T H O S E I N T H E B U S I N E S S O F M A K I N G H E A L T H C A R E W O R K
War casualties
UK - In preparation for war, six
National Health Service (NHS)
military hospitals and over 30
NHS hospitals are said to be on
alert to receive injured personnel
flown back from field hospitals.
6,000 casualties are predicted in
the first four days of battle.
Civilian deaths
About 35 people are killed every
hour as a direct result of war
(source: WHO) In the 20th
century, about 191 million people
died directly or indirectly due to
armed conflict. Most were
civilians.
TV soap hits labs
UK - 14,000 additional cervical
smear tests were performed in
Manchester and the nation’s
CancerBACUP helpline also
received 300 extra weekly calls,
after a TV soap actress played a
cancer victim who died. In letters
to the British Medical Journal,
researchers suggested greater
responsibility in the media.
Intensive care . . . . . . . . . 13-15
Urology . . . . . . . . . . . .
. . 16-17
Company news, awards . . . 19
& innovations
Global events & nutrition . . 20
16-17Urology
Remote control
surgery,
imaging anda new
kidney test
IN BRIEF
13-15
Intensive careMedical air,
e-monitoring and
the international
symposium
GENEVA - Five
groups represent-
ing healthcare
professionals
are urging
governments to
find non-violent
and democratic
means to resolve
conflicts and bring
about peace. They
include the World
Medical Association
(WMA), a global
federation of
national medical
associations,
representing
millions of physicians worldwide; the International
Council of Nurses, a federation of 124 national nurses’
associations representing millions of nurses; the
International Confederation of Midwives, comprised
of 83 national midwifery associations from 70
countries; The World Confederation for Physical
Therapy, comprised of national physio associations
from 83 countries, representing 250,000+
physiotherapists, and the FDI World Dental
Federation, with over 150 national dental associ-
ations and 700,000 dentists.
In a press release, the groups point out that the
health consequences of even ‘conventional’ war are
borne overwhelmingly by civilians, with particularly
catastrophic effects on women and children’s
physical and mental health. Death and debilitating
injury are coupled with threatened access to safe
water, sanitation and food, undermining the health
of a population and creating circumstances
favourable to epidemic diseases. Details: www.icn.ch
5-9Radiology
The 3-D
embryonic
heart, plus
imaging -
the future
continued on page 2
10-11Hygiene
Surveillance,
prophylaxis,
Legionnaire’s
test kit etc
V O L 1 2 I S S U E 1 / 0 3
F E B R U A R Y / M A R C H 2 0 0 3
CHINA - Fear of another ‘killer’ flu
epidemic arose this month when
Hong Kong’s Department of Health
confirmed that a man, who died in
hospital there, had a new viral strain
of influenza A(H5N1)- which is avian
in origin. The victim’s 9-year-old son
also tested positive for the same viral
strain, but has since recovered, as has
his mother. The family had visited the
Fujian Province (China) in January,
where another family member, aged
8, died this month.
The spectre of the pandemics of
1957 and 1968 again rose. In those
periods two million people died of a
particularly virulent influenza.
Laboratory tests have shown that
the genes of the A(H5N1) virus are
purely avian (i.e. without any human
gene content). Dr Yeoh Eng-kiong,
Secretary for Health, Welfare and
Food, urged the public to keep calm,
and stressed that the Government has
stepped up its surveillance system and
Will you become a
global radiologist?CO
VER
PHOT
OS:M
ARY
PARG
ETER
comprising heightened farm bio-secu-
rity, stringent hygienic practices and
an effective surveillance system,
should minimise risk, he said.
Some poultry have been destroyed
and various rules have been set to
cover hygiene and poultry sales. Dr
Yeoh added that officials are studying
the feasibility of vaccinating imported
live poultry to reduce the bird-flu risk.
But he also predicted that, in the
absence of human genes in the virus,
the risk of human-to-human transmis-
sion will be low, but Dr Yeoh expects
more sporadic cases of avian flu, as
the virus is endemic to the area.
However, the Department of Health
in Hong Kong has reported no unusu-
al increase in influenza activity during
the past few weeks.
Further laboratory tests, including
gene sequencing, are being conducted,
and epidemiological investigations are
continuing to find the source of this
infection. The World Health
Organisation is in close contact with
the health authorities in Beijing and
Hong Kong. The WHO Global
Influenza Surveillance Network has
been alerted and additional reagents
for laboratory diagnosis are being
made available to National Influenza
Centres and other Members of the
Global Influenza Surveillance
Network.
will enhance liaison with Mainland
authorities on ways to reduce the
risk of the outbreak of infectious
diseases. Dr Yeoh added that
although the trade has been co-
operative, a multi-pronged strategy,
For some years, while Europeans have slept, elec-
tronic banking and other systems have been ser-
viced online and overnight by technicians work-
ing in different time zones, such as India. The
concept is good, for it keeps the wheels of indus-
try turning and shares revenues with other,
perhaps poorer countries. Obviously, as
telemedicine develops, this is having,
and will have, an ever-increasing
effect on how we deliver healthcare.
For now, everyone is fascinated by
the implications and complications of
cross-border healthcare, in which
patients move to other EU countries for
treatments, with payments reimbursed by
their own. But how about patients staying put,
and their medical files doing the travelling, not
only in the EU, but to far-off places such as
Australia, Israel and the Far East for diagnoses?
This has already occurred with tele-radiology.
In the US, where there is a shortage of radiolo-
gists, hospitals have been transmitting com-
pressed images to Australia and India, for initial
diagnoses. Again the concept is good, in that staff
shortages and night emergencies can be better
covered, and workflow speeded up. Readings
accomplished overnight can be presented at
morning ward rounds. Ultimately the system
Medics against war!could shorten the length of stay for in-patients.
Although online radiology firms mushroomed,
not all have been successful, but now, a new con-
cept, from the Massachusetts General Hospital,
Boston, may set the standard for this type of out-
sourcing. The plan is aimed at advancing
patient care as well as the hospital’s role
in teaching and research - i.e. to also
advance aspects of radiology and
patient care in India. Initially the tel-
eradiology centre - based in Bangalore
and set up with the help of Wipro GE
Medical Systems, with PACS from Agfa
HealthCare, and with the close involve-
ment of an Indian university - is to have US-
trained staff who will relocate to Bangalore.
Following this, Indian radiologists will be
employed and receive advanced US training.
The PACS system will enable access to a full
patient case history.
When the centre is fully operational, the
Boston hospital may then offer services to other
healthcare services. For European this could be of
considerable value in terms of overnight readings
- and with quality set by the ‘mother’ hospital.
All well and good, except for criticism from
some radiologists that the plan will affect employ-
New HFN1 virus puts WHO on alert
Email your
opinions!
We want to hear from
European radiologists
about the implications
of cross-nations
teleradiology
Anti
War
dem
onst
raio
n,th
e Ce
nota
ph,L
ondo
n
5370_EH_
01/2003
03.03.2
003 16:
01 Uhr S
eite 1
Signature Date
The ZOLL AED Plus lays out
the whole rescue in pictures
and voice and text prompts. From the first thing to do
when you get on the scene, to administering
defibrillation and doing CPR while the AED Plus
gives feedback on compression and rate. All with
a new, simplified one-piece electrode, consumer
batteries, small size, light weight, and a
price you’d never pictured possible.
Resuscitation at a Glance
©2002 ZOLL Medical Corporation
Call +31 (0) 488 411183 or visit www.zoll.com for more information.
Introducing the First AED with Interactive Cues for Defibrillation and CPR.

www.SiemensMedical.com
© 2
002.
Sie
men
s M
edic
al S
olut
ions
USA
, Inc
. Ele
ctro
med
ical
Sys
tem
s D
ivis
ionThis used to be one of
the most dangerous places in the hospital.
INFINITY ensures continuous, high-acuity
monitoring even here.
In a busy hospital, patients are constantly moved
from one place to another. The INFINITY SystemTM
was designed for uninterrupted monitoring of all
required parameters, across all acuity levels, in any
location— even the hallway.
INFINITY provides two-way, wireless* connectivity, so
you and remote team members can view the same
critical patient data simultaneously. And our unique
PICK AND GO® concept ensures that the INFINITY
monitor best suited for your patient stays with him
no matter where his care plan takes him.
In addition, INFINITY’s modularity allows you to
upgrade your system as your needs change, ensuring
that your monitoring capabilities are always current.
With INFINITY, even when you’re in transit, you’re still
in touch.
Siemens Medical Solutions that help
A9
10
04
-M3
00
0-Z
11
9-0
1-7
60
0
EUROPEAN HOSPITAL Vol 12 Issue 1/03 3
N E W S / M A N A G E M E N T
Swiss law does not prohibit assisting suicide as longas the motive is altruistic. Also, it does not give physi-cians a special status in assisting suicide, whichmeans that whether assisted voluntary death shouldever be allowed has been discussed without exclusivereference to physicians. Physicians have separatelydebated their role at the end of life.
The few existing data do suggest public supportfor assisted suicide. In a 1999 survey of the Swiss pub-lic, four fifths agreed that ‘...a person suffering froman incurable disease and who is in intolerable physi-cal and psychological suffering has the right to askfor death and to obtain help for this purpose.’
WHAT DO CROSS BORDER
patients think?
Language (and teaquality) affect
patients’ choices.Report by Christian
Pruszinsky
In the distant future Europeanhospitals, focusing on corecompetencies, may serve patientsfrom all over the Union. For now,however, this is very much a pipedream. There can be no quick rideto cross border healthcare. Tobecome a reality, health standardsmust first be streamlined Europe-wide, the service ‘shopping basket’must be defined and nationalproviders of health services needto co-ordinate efforts.
For now, as Michael Huebel,European Commission, DGHealth and Consumer Protection,says, ‘The individual MemberStates can neither quantify patientmigration nor can they project
Director of the Estonian HealthInsurance Fund. Estonia, withonly 1.5 million inhabitants,cannot create a state-of-the-arthealthcare system. ThereforeEstonians go to Finland fortreatment not provided in theirown country. Conversely, the Finslike to use Estonian spas anddental care.
Swiss controversy over assisted suicideLegislation to allow euthanasia was favoured by 71%.
However, resources for palliative care in Switzerland arenot yet available to all terminally ill patients. This remains astrong argument against decriminalising euthanasia.
Despite acceptance of assisted suicide, support for pallia-tive care is growing, as end of life issues are kept in thepublic eye, say the authors of a study in the BritishMedical Journal (Assisted suicide and euthanasia inSwitzerland: allowing a role for non-physicians. BMJVolume 326, pp 271-3). They conclude that further researchon public attitudes and practices at the end of life is impor-tant, in this unique situation.Details: www.bma.org.uk
costs.’ However, experts believe wewill not see major patientmigration.
The patient mobility projectIZOM in the Maas-Rhine region(1,800 participants) has shownthat the ability to communicate inone’s mother tongue is a majorfactor in the choice of a doctor.Flemish-speaking Belgians tend toopt for Dutch doctors, German-speaking Belgians go to Germany,Dutch patients also prefer Germanmedical care when the waiting listsin their own country are too long.
Tim Baxter of the BritishDepartment of Health reports thatits pilot project to cut inordinatelylong waiting lists by providingmedical care in France or Germanywas used by only 190 patients insix months - compared with a totalof six million treatments in its ownhealthcare system. Those 190patients did provide an insight thatcould be more than statisticallyrelevant: British patients pointedout that continental hospitalsfailed to supply a ‘good cupof tea’.
During last year’s EuropeanHealth Forum Gastein, itspresident, Guenther Leiner, pointedout that during the last 20 yearsover 3,000 Bavarian patients weretreated for heart conditions inSalzburg’s Landeskrankenhaus.Indeed, with its huge level oftourism, Austria has lengthyexperience with cross-borderpatients - and related problems.‘When an Italian tourist breaks hisleg and receives treatment inAustria, the health insurancecompany here has to wait up tofour years for reimbursement ofcosts,’ said Gabi Burgstaller,Deputy Governor responsible forHealth Affairs in the Salzburg area.
Two countries on the north-eastern edge of Europe might wellbe on the cutting edge of Europeancross border care. The EstonianCentral Sickness Fund has first-hand experience with patientmigration, said Maris Jesse, MD,

ist doctors were recruited, the AMStogether with representatives from thecounty councils are planning furtherrecruitment fairs in Italy and Spain.
About 90 German specialist doctorshave joined the Swedish health servicesas a result of the recruitment activities.
The Health Services in VastraGotaland have recruited 25 general prac-titioners from Spain. Three recruitmentfairs took place in Rome in October 2002.
The county councils have alsoapproached Poland and the CzechRepublic to recruit doctors, but theprocess is much more complicated dueto restrictions on non-EU citizens work-ing in Sweden.
The government is currently workingon a special provision for applicants withspecialist qualifications to make it easierfor hospitals to recruit from non-EUcountries.
Between 2000 and 2002, 362 doctorsand 90 nurses from Poland, Hungary,Estonia and the Czech Republic wereawarded temporary work permits inSweden.
FINLANDFinland has one of the highest numbersof doctors in Europe - on average onedoctor per 269 population. Currently thecountry has 19,300 doctors, of which17,200 are of working age. Only about100 doctors were unemployed in 2001.
Finland has a long tradition of recruit-ing doctors and healthcare professionalsfrom abroad - mostly from Sweden andNorway. To receive a licence to practicemedicine there, a doctor from outsidethe EU (or European Economic Space(EES)) has to undergo practical trainingand pass a three-part examination,including questions on administration,legislation and clinical medicine, and apractical section testing ability to copewith normal clinical situations. There arealso separate language tests.
Licences are granted in stages. The ini-tial licence is valid only for hospital work.It can subsequently be extended to coverhealth centre work, and then work inother institutions and in private practice.
Licences are always granted for specif-ic periods of time. If a holder of anextended licence is granted Finnish citi-zenship, the National Authority forMedico-Legal Affairs can authorise himor her to practise medicine independent-ly as a licenced physician.
Doctors from within the EU and theEES can obtain a licence to practice med-icine in Finland on the basis of directivesconcerning mobility of doctors andmutual recognition of diplomas.
The National Authority for Medico-Legal Affairs assesses and approves theeducation of healthcare professionalsand recognises their degrees. Physiciansand dentists need sickness insurancenumbers. These can be obtained fromthe Social Insurance Institution aftergranting of a licence.
Licensing of doctors from within theEU/EES area does not involve any lan-guage proficiency requirements, butemployers, e.g. the municipalities, mayrequire a certificate relating to languageskills.
Treating patients is difficult withoutknowledge of Finnish. All workers com-ing to Finland from abroad must obtainresidence permits if their employmentlasts longer than three months.
The permit is granted by the policedepartment at the place of residence.Citizens of EU member states do notneed work permits. Foreign doctors canapply for membership in the FinnishMedical Association if they have alicence to practice medicine in Finlandand a senior colleague recommendsmembership.* Sara Assarsson is a freelance writer. Thisfeature appears by courtesy ofHospitalHealthcare.com.All rights reserved.
InternationalSTAFF RECRUITMENT
An overview of Sweden, Denmark, Norway, Finland and Germany, by Sara Assarsson*
4 EUROPEAN HOSPITAL Vol 12 Issue 1/03
M A N A G E M E N T
GERMANYUnlike most European countries,Germany has a surplus of doctors, nurs-es and other qualified healthcare pro-fessionals. According to recent statisticsfrom the German Doctors Association,an estimated 6,500 doctors are current-ly unemployed, with the problem esca-lating in the northern parts of thecountry.
However, the trend is beginning toturn and unemployment figures havedropped in the last couple of years.
The situation is most difficult fornewly qualified doctors and unemploy-ment figures are particularly high foryoung doctors. The average age for hos-pital doctors in Germany is 40.17.
The average age of hospital doctorshas increased since 1993. Salaries alsovary greatly between newly qualifieddoctors and specialists, and as a resultmany young doctors look abroad foremployment where working conditionsare different.
In the Scandinavian countries, forexample, a newly qualified doctor earnsmore than colleagues in Germany, butexperienced physicians and specialistsearn considerably more in Germany.
There are currently 375,000 medicaldoctors registered in Germany, of which298,000 are of working age. Despitethe high unemployment figures,Germany has a large proportion of for-eign doctors working in the health ser-vices.
A total of 15,000 doctors have over-seas qualifications, of which 4,000 arefrom other EU countries and othersfrom the remaining European countriesand the rest of the world. A large pro-portion is from Asia.
There are currently 3,600 Asian doc-tors working in Germany. A number ofsuccessful recruitment fairs, hosted byDanish, Norwegian and Swedish healthauthorities and employment services,have attracted a large number ofGerman doctors and other healthcareprofessionals. Generous salary pack-ages draw young doctors who couldface longer working hours or unem-ployment if they stay in Germany aftercompleting medical school.Work condi-tions in Scandinavia are more regulat-ed.
NORWAYNorway has a long tradition ofrecruiting labour from abroad. SinceWorld War II the private as well asthe public sector has been depen-dent on immigrant labour.
The growth of the industrial sec-tor has seen an increase in immi-grant professionals in a range of sec-tors, from building and industry tothe healthcare sector.
Norway has one of the most effi-cient healthcare services in Europe.But as in most other EU countries,there is a shortage of qualifiedhealthcare professionals.
In the mid-90s there was an acuteshortage of doctors. As a result, anextensive recruitment project wasinitiated in 1996. The recruitment
10 million per year for recruitmentof healthcare professionals.
In 1998, around 100 doctors wererecruited from abroad, of which themajority came from Germany. Since1999, around 200 doctors per yearhave been recruited from abroad.Because of the common labourmarket in the Nordic countriesthere are a significant number ofSwedish and Danish healthcare pro-fessionals.
Large proportions of the Nordicpopulation move between thecountries, primarily betweenDenmark, Norway and Sweden asthey share similar languages andculture. The majority of doctorsfrom outside the Nordic countriesare from Germany.
SWEDENAccording to estimates from theSwedish Employment Service, AMS, anextra 500,000 qualified healthcareworkers will be needed in the healthservices within the next ten years.
On average, 23,000 new recruitswill be required per year for the next15 years, which means that every thirdundergraduate will have to choose ahealth profession to meet thedemand.
The shortage of hospital staff, cou-pled with a lack of medical schoolplaces at Swedish universities, meansthat an increasing number of doctorsand nurses are expected to be recruit-ed abroad. The Federation of CountyCouncils (LF) estimates that there is aneed to recruit between 300 and 350
project involved co-operationbetween employment services andcentral and regional health authori-ties.
In 1997, the Norwegian employ-ment services approached their coun-terparts in Germany, France andAustria. Negotiations led to severalrecruitment agreements betweenthe countries. These include informa-tion about the labour market, recruit-ment facilities and intensive lan-guage courses, including a three-month course in Norwegian, provid-ed for French, German and Austriandoctors and nurses in their homecountries.
The average cost of a languagecourse for 10 participants amounts toNkr 450,000, excluding administra-tive costs. In total, the Norwegianhealth authorities have invested Nkr
Immigrant professionals fromoutside the EU are only grantedtemporary work permits - similar tothe work permits awarded musi-cians, artists, au pairs and seasonalworkers in the agricultural sector.
However, because of the shortageof healthcare staff, health profes-sionals are exempt from these regu-lations.
Norway’s employment servicesestimate a continuous need forinternational recruitment of health-care professionals. The healthcareservices are increasingly dependenton foreign doctors and nurses andthe need is estimated to increaseeven further.
The demographic developmentimplies there will be a shortage oflabour in all sectors, both privateand public.
overseas doctors per year.In a move to meet the acute short-
age, county councils have turnedabroad to recruit nurses and special-ist doctors from Denmark, Austria,Germany, Spain and Italy.
Sweden has a long-standing rela-tionship with the Nordic countries forfree movement of labour. The majori-ty of doctors, nurses and otherhealthcare staff with foreign qualifi-cations are from Denmark, Norway,Finland and Iceland.
Doctors with foreign qualifications- primarily from Germany and theScandinavian countries - constituteabout a third of all qualified doctorsin Sweden.
Following a number of successfulrecruitment activities in Germany,from November 2000 to June 2002,during which more than 500 special-

%exists in nine countries.Nuclear medicine is aspeciality in 13 coun-tries while clinical phys-iology seems to be alocal speciality.
The end result of the developmenttoward a more integrated functionaland morphological curriculum inradiology training has to be evaluat-ed. This cannot only be done by theupcoming European Diploma ofRadiology, but also assessed throughthe European Training AssessmentProgramme. Representing a smallcountry in the periphery of Europe, Ifind it encouraging that the UEMSRadiology section is active in devel-oping such tools in defence of thequality of our speciality.
See you at a digital ECR!
EUROPEAN HOSPITAL Vol 12 Issue 1/03 5
R A D I O L O G Y
ECRsees21%increasein abstracts
With 527 submittedabstracts, Italy ranks firstand surpassed last year’sleading country Germany(485 abstracts). Greece isagain third, but with asignificantly highernumber of abstracts(+89%). Spain (+93.4%),Turkey (+92.8%) andYugoslavia (+142.1%), all amongthe top 10 countries, also showed anenormous rise in abstracts.
Most submissions relate to Abdominaland Gastrointestinal Radiology (567),followed by Interventional Radiology(364) and Musculoskeletal Radiology(345).
If viewed by type of abstract, mostscientific exhibits were submitted onAbdominal and Gastrointestinal Radiology(333, +34 %), Musculoskeletal Radiology(201, +54%) and Genitourinary Radiology(173, +74.7%). The topic Physics inRadiology recorded the most pronouncedincrease in scientific exhibits (+120%).
In the scientific papers, Abdominal andGastrointestinal Radiology was again themost popular topic, with 234 paperssubmitted. Interventional Radiology saw aremarkable 61% increase in submissionfigures.
Morphologic and functional imagingBy Professor Hans Ringertz, Director of the Karolinska Institute’s radiology faculty, and Deputy Chairman of the Nobel Assembly
As a spin-off from theEuropean list of specialitiesin medicine, the SwedishGovernmental Office of
Health and Welfare has started anevaluation aimed at reducing thenumber of specialities. The real rea-son for this evaluation has been thehigh costs caused by too many doc-tors being on duty in hospitals. Areduced number of specialitieswould allow doctors to cover morethan one speciality. The evaluationhas suggested that radiology shouldbe part of what literally translatedcan be called ‘Imaging and func-tional medicine’ or more freelytranslated ‘Morphologic and func-tional imaging’. The term ‘medi-cine’ covers both diagnostic andinterventional imaging.
A common period of 2.5 years oftraining is suggested for all radiolo-gists, nuclear medicine doctors anddoctors in clinical physiology. Afterthis common period of training,each of these groups of doctorsshould continue separate studiesfor another 2.5 years. Today theproportion of doctors working inthese three specialities is 20:2:3;thus the resulting double specialistswill hopefully mostly cover thework that radiologists do today. Itis specifically pointed out that thisscheme is needed to comply withthe rules on the free movement ofdoctors within the EU. These rulesapply only to doctors of a recog-nised speciality.
The suggested changes in nameand content have two very differentgeneral implications for radiology.On the one hand there is a short-term professional and clinicalimplication, which might be dealtwith by the Union of EuropeanMedical Specialists (UEMS)Radiology sections at the Europeanlevel. The changes in this respectmight be both politically bad andgood. On the other hand there isthe long-term academic evolutionof our science and the future ofmedical imaging.
This implication can be illustrat-ed by the schematic representationof possible new pathways to thedevelopment of new clinical imag-ing methods, modified after Li:Acad Radiol 2002;999. I am con-vinced that more physiology,nuclear medicine and functionalthinking, as part of a new curricu-lum for clinical medical imagers (orwhat they should be called), wouldsimplify a development where co-operation with all the illustratedscientific groups is essential, not
only for participation in researchbut also for feedback from clinicalwork close to patients.
Without the research and adapta-tion needed, there is a considerablerisk that other specialities will fillthe vacuum in the course of exist-ing or new turf battles with ourprofession. The question is ratherhow quickly we, as imagers, canadapt our work to the upcomingaspects of molecular medicine. Inthis respect, I am afraid thatEurope might be less prepared than
our American colleagues, for exam-ple, with their new MolecularImaging Laboratory at NIH andtheir National Institute ofBiomedical Imaging andBioengineering.
As far as professional aspects areconcerned, there are already twodifferent curricula for radiologytraining in Europe. Diagnostic radi-ology belongs to the 17 specialitiesthat exist in all 15 EU countries,while radiology including diagnos-tic radiology and radiotherapy still
3,413 abstracts have been submitted via the Online AbstractSubmission System for ECR 2003 (Vienna. 7-12 March). The increase of
597 represents 21.2% more than those received for ECR 2002. Theorganisers say the 50.5% increase in the number of posters submitted
demonstrates acceptability of a newly introduced Electronic PosterOnline System (EPOS), and that radiologists are keen to join the first
all-electronic poster exhibition ever staged at a radiological event.
Acceptance
Of 3,413 abstracts reviewed by theteam of reviewers consisting of allECR 2003 SubcommitteeChairpersons and Members, theProgramme Planning Committeeaccepted 2,073 for presentationduring ECR 2003, creating arejection rate of 39.3%.
For the first time in ECR’s history,the number of accepted scientificexhibits (1,064 or 51.3%) surpassedthe number of abstracts accepted fororal presentation (1,009 or 48.3%),which again confirms the greatsuccess and wide acceptanceof the ECR Electronic Poster OnlineSystem.

6 EUROPEAN HOSPITAL Vol 12 Issue 1/03
R A D I O L O G Y
3-D embryo
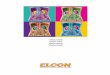
When a 58-years-old woman was admitted toour Institute with a former diagnosis of liverechinococcal cyst, she had already received as acausal treatment albendazole (Zentel, Glaxo) 1cdaily. The original diagnosis was based mainlyon an ultrasound (US) examination whichsharply described an iso-hypoechoic mass withan hyperechoic outer rim whose thickness wasabout 2-3 mm, while the overall size of themass was 7.0 x 6.0 cm. The segmental locationwas in the VIII liver segment.
A spiral CT scan showed an hypodense masswith outer enhancing rim in the early arterialphase and a non-enhancing mass in the portaland late phases. The MR showed anhyperintense mass in the T1-weighted imagesand an hypointense mass with outer thinenhancing rim in the T2-weighted gadolinium-enhanced images. Despite the imaging results,the liver, kidney and the most of routinebiochemistry was remarkably normal.Additional studies, such as full endoscopy ofupper and lower gastrointestinal tract, did notadd any useful information to the patient’smedical record. Finally, a serology test forechinococcal infection was negative.
Due to the lack of evidence about the natureof the mass, we decided to perform a new USand contrast-enhanced (CE) US, using Aloka
DETECTIVE WORK S Rossi, L Rosa and V Ravetta (UO of Hepatology) and F Calliada, P.Quarettiand A Azzaretti (Department of Radiology), Policlinico S.Matteo IRCCS,Pavia, Italy, discover a liver carcinoid mimicking an echinococcal cyst
Kodak will launch a range ofproducts at the European Congressof Radiology this March,including:● The DirectView PACS System 5architecture, currently underdevelopment. This will expediteefficient storage, diagnostic readingand review of radiology reportsand imaging studies, the firmreports, adding that the system canbe scaled for use in a small hospital,one or more imaging centres, or alarge healthcare facility. ● DirectView Web DistributionSystem, distributing images andradiology reports to referringphysicians via the internet, includesthe new database to use with PACSSystem 5 architecture. The Websystem enables clinical review byphysicians on dual-monitor, high-resolution workstations; providesboth lossless and lossy (wavelet)compression, and supports bothMacintosh and PC platforms usingan Internet Explorer or Netscapebrowser.● DirectView DR 5100 System, anenhanced version of the Kodak DR5000 system, designed for chestand other upright examinations forambulatory and non-ambulatory
patients, has a new integratedtouch-screen operator console, newgenerator, bucky and tube standand Kodak DirectView PTSsoftware. ● DirectView CR 850 System, asingle-cassette system, offers 100cassettes throughput per hour, plus‘exceptional image quality’ the firmsays, adding that with a footprint ofjust 63 x 73 cm, it also needs littlespace. ● DirectView CR Long-LengthImaging System. This digitalimaging system, with wall-mountedvertical cassette holder, produces
full leg and spine digital images ofup to 43x129 cm, viewable insoftcopy or as radiographic film.The form points out that thissystem significantly reduces themost frequent causes of examretakes - poor stitching, incorrectalignment or images that are not inthe right order. ● DryView 8900 Laser Imager,producing 180 films per hour at650 dpi laser resolution, in five filmsizes, using three film drawers. ● X-Sight Screen, for use withradiographic film to improve imagequality, produces images about20% sharper than those from the
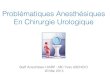
Not much bigger than a thumbnail, the heart under observationcontracts three times per second,pumping a few drops of bloodthrough an 18-week-old embryo.Although 15 cm of skin, fat andmuscle tissue shield the organ, onthe computer screen the tiny heartcan be seen pulsating as a 3-Dimage. Tapping on the mouse, DrUlrike Herberg, child cardiologistat the University of Bonn, turnsthe image in various directions andpoints to the clearly definedcardiac valves, opening andclosing. ‘Conventional equipmentgives us 2-D images, which arecross-sections - cutting through theventricles, for example,’ sheexplains. What the ventricles looklike spatially, whether they aresmaller than normal or perhapsare defective in the way theycontract, must be decided by
doctors by mentally assemblingthose cross-sections into a 3-Dmodel.
‘For that, even with animmobile organ, an excellent senseof space and plenty of experienceare required, which is even morenecessary with the heart -regularly contracting then fillingup with blood again.’ Althoughleading ultrasound specialists maydiagnose, whether an unborn childis suffering from a heart defect,with a rate of about 80%accuracy, less experienced medicalpersonnel may achieve only a25% rate.
In conjunction with theUniversity of Bonn’s Clinic forObstetrics and Pre-natalDiagnostics and experts from thesoftware firm MedCom Ltd, DrHerberg is currently developing asystem to carry out that mental
Prosound SSD 5500 ePHD (Aloka, Tokyo) with adedicated technology for microbubblesdetection, a low mechanical index (MI<0.04),second harmony filtering and phase detection(ePHD, extended pure Harmonic Detection). TheCEUS was performed by microbubbles of atotally innocuous sulphur hexafluoride gas(SonoVue, Bracco, Milan). The US confirmed aniso-hypoechoic mass with an hyperechoicperipheral rim (Fig.1), while the US color Dopplerdid not detect any signal of flow inside or aroundthe mass because of some artifacts from theheart beat. CEUS showed an enhancing rim atthe arterial phase (Fig.2), which becameisoechoic at the portal and late phases (Fig.3),while the inner core of the mass did not enhanceat all. During CEUS we performed spectralanalysis which showed an arterial pattern on thesignal detected in the peripheral rim of the mass(Fig.4).
As a final step, the inner core of the mass wasaspired, under US guidance, using Ecojet 21Gwhile the outer rim was also biopsied withBiomol 21G (both Hospital Service, Milan). Thefirst sample collected a bloody fluid, while thesecond gave a sample of solid tissue, which lateron demonstrated, in pathology studies, a patternof carcinoid (immunohistochemistry positive forchromogranine A, Ab Ki67= 2 to 5%).
Fig.1 Iso-hypoechoic mass with a peripheralhyperechoic rim, 7.0 x 6.0 cm in diameter, in the VIIIsegment of the liver
Fig.2 CEUS showed an enhancing rim at the arterialphase
Fig.3 Enhancing rim detected at the arterial phase ofCEUS become isoechoic at the portal phase
Fig.4 During CEUS, spectral analysis detected anarterial pattern at the site of the signal flow, visible inthe peripheral rim
New at the ECR Left: Kodak diagnostic workstationBelow left: Kodak web distributionBelow: Kodak CR 850
previous X-Sight film and screensystem, the firm reports: ‘Thescreen’s smaller phosphor particlesfacilitate modulation transferfunction (MTF) improvements athigh x-ray absorption and reduceimage noise, while its zerocrossover film technologyminimises light scatter.’
Tricuspid (TV) and mitral valves (MV) from the same set of data. Unlike 2-D-images, it is possibleto show a frontal view of the valves with a 3-D data set, or even to show the interventricular
septum (here, top of ventricle and top of atrium were cut from the set of data above, inechocardiographic four-chamber view and the set of data was then rotated 90 degrees)

EUROPEAN HOSPITAL Vol 12 Issue 1/03 7
R A D I O L O G Y
The Point of Knowledge
ShareShare the right information, the right way,At the right time, with the right people.
Share the advantages of a digitally connected world:From Home to Hospital;From Clinic to Multi-site Network.
Share beyond Radiology and PACS.Share end-to-end.
Our IMPAX™ and Quadrat solutions pave the way from entry level digitization to a comprehensive Electronic Patient Record:In an integrated & open environment, yet fully secure.
Use our experience of more than 10 years in over 700 PACS projects.
Grow into the future.Share, with Agfa.
www.agfa.com/healthcare
H E A L T H C A R E
Visit us at ECR, expo B, booth 211
Italian presidentfor EuroPACS
Professor Davide Caramella, associate professor of radiology at theUniversity of Pisa, Italy, has been elected president of the EuropeanAssociation for the Promotion of Information on Picture Archiving andCommunication Systems (EuroPACS). The Society, with about 50members, mainly from institutions involved in the design, installationand assessment of PACS, aims to promote research and encouragediscussion about technological evolution and experiences in clinicalimplementation and evaluation of PACS in Europe and internationally.
cardiac function‘assembling’ of data.
In this, a conventional ultra-sound probe placed on themother’s abdomen is swivelled in acertain way to image the completeheart of the unborn baby within20 seconds, and provide a 1,000-image record. At the same time abaton (sensor) records the foetalheartbeat, feeding data to thecomputer to match an image topart of a beat. If, for example, ababy’s heart contracts and expands60 times during the examination,the machine will record 60 cross-sections, all taken from differentareas of the heart, during theswivelling movement at the time ofmaximum contraction.
The imaging software thenassembles a composite 3-D imagefrom the 2-D ultra-sound images.When the probe is swivelled for amaximum of 20 seconds thesoftware receives 3-D picturesfrom different phases of theheartbeat - from completecontraction to completerelaxation. Thus the entiremovement of the myocardium can
Eight out of 1,000 babies are born with a heartdefect. Prenatal detection and specialist careheighten chances of survival and can lowerundesirable after-effects. Cardiologists at BonnUniversity are currently developing a method toimprove and simplify diagnosis of embryonicheart defects by watching cardiac activity in 3-D
be followed on the screen. ‘Wecan even see exactly how thecardiac valves open - informationnot available from conventionalcross sections,’ says Dr Herberg.
The ability to see 3-D imagesfrom various directions alsoenables treatment planning - andwhat Dr Herberg finds‘particularly attractive, is thepossibility that some cardiacdiseases may be treatable orprevented before birth if detectedearly enough.
The software enables thevolume of the heart to becalculated far more precisely thanbefore - often an early indicatorthat there is a problem withdevelopment of cardiac muscle.Twins, for example, may developa joint cardiovascular system viathe placenta. ‘One twin keepspumping blood into its sibling’sbloodstream, whereby that twin’sheart becomes overloaded. Itbecomes excessively large andserious heart defects are possibleconsequences.’ Detected early, thismalformation can be prevented bylasering and sealing the joinedblood vessels.
There are still minor problemsto resolve, such as reduction ofimage quality during heartbeatmeasurements by the baton, andimproving the technique to evenlyswivel the probe; then the systemwill face clinical trials.Contact e-mail:[email protected]

8 EUROPEAN HOSPITAL Vol 12 Issue 1/03
R A D I O L O G Y & T E L E M E D I C I N E
DZ: Your business card readsMedical Solutions, GlobalSolutions, what does this meanand how does it relate to the first,fully digitised cardiology project inthe US?LM: I was previously head of theGlobal Solutions project. Whenthe Siemens Medical Boarddecided to turn the project into anew business section - GlobalSolutions - I became head of thisdivision. To ensure that we candeliver outstanding quality and toenable greater expansion, ourinitial focus has been oncardiology and the ‘digitalhospital’. We are not trying toattempt everything at the sametime, worldwide. For now we areconcentrating on Germany and theUS.DZ: ...to advance Cardiology andEPR?LM: Not EPR, but the digitalhospital. This entails far morethan EPR - which is only a smallcomponent. Another, veryimportant component is workflowadvice. How does a cardiologistwork, how can we improveprocesses in the health service,such as in a heart centre orhospital. This brings us to DrBulitta’s role. Among our team ofadvisers, he is responsible for thehealth service.
One of our pilot projects incardiology is the Heart Centre ofIndiana, which opened inDecember 2002. This is theworld’s first, fully digitised heartcentre - and, from the outset, wedeveloped all processes, workflowand equipment that are used at thecentre.CB: In principle, the hospitalworks without paper. However,for legal reasons, there still has tobe paper documentation.However, all of the imagingprocedures, the EPR, RIS,administrative, medical and
DELFT DIAGNOSTIC IMAGING will present anew, digital thorax scanner at this year’s ECRexhibition (booth 321 Expo). EuropeanHospital interviewed the firm’s ManagingDirector, Guido Geerts, about this new productplus the structure and scope of his company intoday’s highly competitive healthcare market
DELFT DIAGNOSTIC IMAGING (DDI), is a subsidiary ofDelft Instruments NV, which has medical and industrialdivisions. Within the medical division, DDI concentrateson radiology, whilst Nucletron, its sister company, focus-es on radiotherapy. DDI is comprised of three groups:Rogan Delft (software - PACS systems); Delft ImagingSystems - formerly Oldelft (hardware - producer of thenew ThoraScan) and Oldelft Benelux (system integration,which covers servicing). ‘They have a lot of experience,’he points out, ‘We understand the kind of problems thatoccur when you install soft- or hardware. So we can offera better service.
Guido Geerts refers to ThoraScan as a ‘Rolls Royce’ in itsfield - offering a very low dose and very, very high imagequality. ‘Oldelft has 50-years of experience in the produc-tion of thorax equipment, and ThoraScan is the latesttechnology, having a direct radiology (DR) system. Thiscan be bought with our Mini-PACS-System, dedicated toone modality, but connectable to others - you canincrease and expand the Mini-PACS into a larger PACSsystem.’
The use of IT in healthcare is increasing rapidly, hepoints out. ‘We are in the middle of this growing andinteresting market. We foresee a massive market forPACS, which includes tele-radiology to link with generalpractitioners (GPs). There is also a huge need for very
The world’s first, fully-digitised
Heart Centre
Louise F. Morgan, Senior VicePresident of Global Solutionsand Dr Clemens Bulitta, SeniorManagement Consultant,Siemens AG, describe thecompany’s impressive role inprogressing digitisation ofhealthcare delivery, in a brandnew and luxurious US heartcentre. Interview by DanielaZimmermann, of European Hospital
logistic information thataccumulate in the process areelectronically produced and madeaccessible in this way. Of course,there are certain documents, suchas patient consent forms, whichmust be signed and kept as hardcopies. However, everything,administrative and demographicdata starting from a patient’sadmission, to the final dischargereport is fully digitised.DZ: Who can access this system?LM: Only those authorised totreat patients, for example thegeneral practitioner, cardiologists,etc.CB: The IT hardwareinfrastructure is available
LM: No! And it is veryarchitecturally pleasing. Thedesign supports the workflow.Patients never have to wait ontrolleys in corridors, nor are theytransported long distances throughthe centre. We co-operate withcardiologists, nurses and thearchitect for the design. A patientis allocated a room for theduration of his stay - irrespectiveof his state of health. This meansthat every single room caninstantly be turned into a cardiaccritical care unit, if necessary.Monitors, data, information andexaminations can be madeavailable at very short notice inthe same way that they would be
examination via computer. This wasa diagnosis examination, usuallycarried out by a radiologist. Withthe mobile unit, the examinationwas carried out on site - digitally -and the images were relayed to theradiology department via theinternal network. The radiologist, inanother part of the building,immediately carried out an on-screen diagnosis, without leaving hisdepartment, and sent it back inseconds.DZ: That procedure works if alldoctors involved feel they are partof a team, and are agreed thatoutput is the most important aspectand they serve a common purpose.That’s not always the case for alldoctors...CB: Yes, it is difficult. This is whywe think that, apart from ourclassic, product-based business, weneed to offer additional services thatimprove processes, and processmanagement advice for hospitalsetc. We have to offer the customer acomplete solution, not just a perfecttechnical solution - customers beingthose delivering a medical service,such as a cardiologist with his ownpractice, a heart centre, or hospital.We enable them to have the righttechnology as well as support, bydefining and improving processes.DZ: So, to progress, you need toparticipate actively in hospitalmanagement...CB: Yes, we must explain theimportance of such measures to allthose involved in the process. Wetake on the roles of presenters. Thisis a big challenge, but I believe it iseasier to find solutions for internalproblems with external support. DZ: Discussion about networks,planning and equipment is not anentirely new concept...LM: The focus on the entiretreatment phase is new. And notevery doctor or every hospitalappreciates this approach. However,there are doctors who do want andunderstand it. They are examples toothers and proof that it can work.They are our references for thosewho doubt the concept. We canshow them the clinic - thecardiologists, the radiologists andshow how successfully they worktogether, how much they enjoy theirjobs, how proud they are of whatthey have achieved together - thequality of the treatment and howmany cases they have treated withsuccess.
information available to make theright decision about the righttherapy. This enhances bothpatient satisfaction and quality oftreatment. Taking this intoconsideration, the investment isnot really that expensive, and a lotof it is recouped through improvedworkflow processes. If quality ishigh and patients are happy, thisattracts more patients andincreases the turnover of the clinic.It’s an investment in a growingbusiness area.DZ: Intensive care beds are amongthe most costly items in a hospital,which is why patients are oftentransferred from ICUs veryquickly...CB: The entire heart centre onlyhas 60 beds. In many cases, oncepatients have received basicmedical care, they can betransferred to an associated hotel,but they continue to receiveoutpatient treatment from thecardiologist. This is also commonpractice in other areas of theAmerican health service. Patientswho continue inpatient treatmentfor a length of time in Europe,would have been moved to a hoteland treated as an outpatient in theUS much sooner. The Heart Centretries to keep inpatient numbersdown, so as to treat as manypatients as possible and thusincrease revenues. LM: I would like to return to thesubject of process optimisation.When the centre opened and thefirst patients were admitted, I metone of the Heart Centre Boardmembers, standing at a patient’sbed. He had requested a mobile
high quality digital thorax equipment - ThoraScan is dig-ital - so in both the hard- and software markets we haveproducts that are very interesting now and for thefuture.
Considerable consolidation has occurred in the radiol-ogy market, with Philips and GE buying many suppliers,which, he says, has presented Delft with many possibili-ties: ‘There aren’t many suppliers anymore, so it’s noteasy for distributors to survive. For those people it is verygood to know that there is this new division. I think a lotof distributors need a high-tech new supplier, and we arean interesting source. So the market will grow for us. Weare active in Europe (and still seeking more distributionpartners there), as well as in the USA and Far East.
IT is the general hype; everybody is talking about digi-tising hospitals, so they need the hard- and software. Inthe short term we are focusing on PACS and dedicatedthorax equipment, but we are also looking at goodmodalities to add to our range of products.
COMPANY PROFILE
everywhere, whether on a ward orthe heart catheter laboratory. Theway individual users access thesystem depends on their roleswithin a patient’s treatmentprocess.DZ: So is the main challenge tocreate communication between thelaboratory, administration, RISand so on.?LM: That’s the technicalcomponent, but the mostimportant thing is that once youare in the Heart Centre, you don’tfeel like a patient, but more like aresident in a luxury hotel. This isunique. Patient satisfaction is veryimportant here. The centre evenhas a hotel-like reception. Itdoesn’t seem like a hospital at all.DZ: It doesn’t ‘smell’ like ahospital either?
available on an intensive careward.DZ: This sounds expensive!LM: Everything is to hand veryquickly, so treatment cancommence without delay. Thedoctor has all the necessary
Above: Louise F MorganRight: Dr Clemens Bulitta

EUROPEAN HOSPITAL Vol 12 Issue 1/03 9
R A D I O L O G Y & T E L E M E D I C I N E
THE INNOVATOR IN ULTRASOUND
www.aloka-europe.com
EH: Will PC capabilities andstorage capacities increasinglydominate a radiologist’s work inthe future?
TH: I think that’s a wrongconclusion. Of course the trend istowards telemedicine, molecularimaging, digital radiography, CADand PET - all developmentssupported by continuallyimproving computer capabilities.However, the radiologist of thefuture won’t necessarily have to bea computer freak and softwarespecialist. A decade’s worth ofexperience with PACS has shownquite impressively that copingwith huge amounts of data can beachieved in a very user-friendlyway, and that radiologists canquickly develop a new andimproved grasp of imaging anddiagnostics.
That’s not only limited todevelopments in hospitals but alsoapplies to radiologists with theirown practices who areincreasingly using digital imagingfor conventional bone and lung X-rays. Most radiology surgeries arenow changing and upgrading theirequipment.
EH: Will film X-rays becomerelics quite soon?
TH: In the long run - andphotographic companies haveadapted to this trend - Agfa, forinstance, have equipped largehospitals with PACS.
EH: What about documentationrequirements?
TH: With teleradiography, used incertain hospital areas, a hard copyof the digital image is filed fordocumentation. But even so, thegeneral trend is towards web-based documentation, for whichthe radiologist only needs CD-ROM compatible software on aPC.
There is a concept that one daya radiologist will be at home, buton call, and he may instruct hisradiographer to carry out anexamination, to then make hisdiagnosis after receiving itelectronically. This may seem farfetched, but I believe it willbecome common practice muchsooner than we think.
In California they already havemobile mammography screeningunits, that are driven from town totown and which relay images toan examination centre in SanFrancisco via satellite. In Europe,there are similar screening projectsin Norway, Sweden, Finland,Holland, France, England, Spainand Italy.
focusIn a pre-ECR interview, Thomas H Helbich MD, Associate Professor of Radiology, Department ofRadiology, University of Vienna (AKH), discussed trends in imaging and IT and their future effects
EH: Isn’t there a danger thatradiology, with ever-increasinginvestment in IT, will come underfire eventually?
TH: I cannot comment on the highlypolitical issue of healthcare costcutting. However, But from amedical point of view I must look atthe cost-benefit analysis. Thisclearly shows that modern imagingprocedures present enormous costcutting potential. Look at vascular
diagnostics: modern, non-invasivemulti-slice technology (MR-angiography) enables me todiagnose the vascular structure of apatient suffering from peripheralarterial occlusive disease (PAVK)within 10 minutes. Withconventional methods, the samepatient would spend a day inhospital and be examined with thehelp of a catheter inserted throughthe groin.
With knee injuries, I can avoid
arthroscopies, and there areenormous savings potentialswith modern imaging intumour diagnosis. On top ofeverything, modern imagingprocedures obviously achievebetter, more precise diagnosis,which in turn facilitates morefocused treatment - and thatmeans shorter hospital stays. Itis very obvious to me thatevidence-based medicine is costeffective.
THE FUTURE IN
“

H Y G I E N E
Bacterial nosocomial infec-tions (NI) are mainly causedby bacteria belonging to‘normal’ microbial flora
colonising the human macro-organism. The main micro-ecologi-cal systems are the intestinal tract,mucosas of the oropharynx, uro-genital tract and the skin. Otherbacteria associated with NI havetheir natural habit in moist areas(e.g. Pseudomonas spp.) and plants(e.g. Stenotrophomonas maltophil-ia, Burkholderia cepacia).
Bacterial species relevant tonosocomial infections are condi-tional pathogens that exert theirfatal activities when in the wrongplace at the wrong time. Althoughnot intentional, treatments andnursing can place bacteria in thewrong places (e.g. injections, inci-sions, catheters, ventilation).
‘The ten pillars of hygiene are: wash your hands, wash your hands, wash your hands, wash your hands, washyour hands, wash your hands, wash your hands, wash your hands, wash your hands, wash your hands.’
Helmut Raake, Moderator, Hygiene Professional, Bergisch Gladbach
A DECADE OFhygiene forums
Angelika Lermen Becker (Ev.Jung-Stilling-Krankenhaus
Siegen gGmbH), Gisela Gallus-Teffahi (Kreiskrankenhaus
Huettental) and Rita Kempf (St.Marien-Krankenhaus Siegen
gGmbH) organisers of thehygiene forum in Siegen
GERMANY - This year’s ‘10th Hygiene Forum’, attended by c. 700people, focused on nosocomial infections - particularly MRSA. Herewe highlight several presentations, which can be accessed in full atwww.hygieneforum-siegen.de.
The Forum series is organised by hygiene professionals: GiselaGallus-Teffahi, Rita Kempf and Angelika Lermen-Becker, who alsoform the management board of Hygiene und Umwelt imKrankenhaus e.V, a non-profit organisation promoting further andcontinuing education in hospital hygiene. Three hospitals in Siegenorganise the event and programmes are certified as continuingmedical education. Many subjects have been covered, such as thekitchen, endoscope hygiene, allergies, infections such as HIV, andnow various aspects of prophylaxis (which included a discussionby Dr Klaus Jung on prophylaxis and naturopathy. Legal issueswere also covered (Werner Roehlig), as were quality and costs.
Dr Margret Seewald pointed out that the number of agedpatients is rising, as are ‘uncomplicated’ cases ‘... which areincreasingly being moved to out-patient care or to specialisedclinics. For everyday life in the hospital this means frequentcolonisation with multiresistant bacteria, previous broad-spectrumantibiosis, poor post-op risk scores. Consequently, hospitals andwards, depending on their speciality, witness significant shifts inthe severity of the illnesses. To reconcile quality demands andeconomic constraints in the age of case-mix, departments willhave to develop their own, very specific answers to these issues.’
New guidelines call for actionAbout 640,000 nosocomial infections are caused annually inGermany by incorrect or erroneous recycling procedures of medicalproducts. Corresponding figures for homes or out-patient treatmentcentres are not available.
Last November, the DGSV (German society for the supply of sterilegoods) and the Robert Koch Institute (RKI) presented new guidelinesfor recycling medical products in Potsdam. These will be binding. Infuture medical trials, hospital compliance with the guidelines willfacilitate the burden of proof.
The guidelines, which consist of urgent recommendations for allhospitals, are based on professional commentaries (category lb).
A complex quality management system for a centralisedsterilisation process is required. Simply looking at an instrumentcannot determine whether it has been sterilisedThe user must be able to rely on internalquality assurance procedures.
Reasons, prophylaxis and therapyBy Professor Wolfgang Witte of the Robert Koch Institute, Wernigerode
age of patients have led to higherrisks for infections, thus increasingconsumption of antibiotics andselective pressure in favour ofantibiotic resistance. This is clearlyreflected by prevalence of multire-sistance to different antibioticclasses in S. aureus from healthycarriers, from sporadic nosocomialinfections and from outbreaks ofnosocomial infections. As is partic-ularly known for methicillin resis-tant S. aureus (MRSA), multipleresistant epidemic strains haveevolved that possess a pronouncedcapacity to spread in nosocomialsettings.
Epidemic MRSA can be identi-fied by genomic fingerprints. Thesestrains are widely disseminated in
Central European hospitalsand even intercontinentally,due to neglect in hospital
transfers of patients colonised orinfected with multiresistant bacte-ria -such transfers should be pre-ceded by a warning to the receivinginstitution. Among many risk fac-tors for dissemination inside a hos-pital, the most important areunfavourable patient-staff ratiosand antibiotic selective pressure.Antibiotics do not just act against atargeted pathogen, but also affectcolonising microflora, which areeradicated by long lasting antibiot-ic treatment and replaced by mul-tiresistant nosocomial strains.
Historically, antibiotics can beused only for a quite short period.Bacterial resistance has always fol-lowed the introduction of new sub-stances.
During the past 10 years analarming development of antibioticresistance has been observed.
ConclusionsResults from bacteriological diag-nostics of nosocomial infectionsshould be continually analysed, asan early warning for transmissionsand emerging of multiresistantstrains and of new resistance types.
A number of recommendations,from management of MRSA out-breaks, are known to be effectivefor infection control. Countrieswith low prevalence of MRSA havestrong infection control systems.The recommendations are a compi-lation of various measures.Although not always evidence-based for some situations, theyshould be fully utilised. The ineffec-tiveness should be demonstrated,not the opposite!
Records of nosocomialpathogens and their resistance pro-files should be analysed togetherwith data on antibiotic resistance tosteer antibiotic regimens. ■
Materials with specificrecycling regulations ● Non-critical - Material
with only skin contact(e.g. electrodes)
● Semi-critical - Materialthat has contact withmucous membrane ordiseased skin.
● Critical - Material thatenters the body or hasblood contact. Thisrequires specialprocessing.
Nosocomial infections originat-ing from the patient’s natural floraare ‘autogenous’ and ‘endogenous’.30% of healthy humans arecolonised in the vestibulum nasi byStaphylococcus aureus. Moleculartyping has demonstrated that mostwound infections after primarilyaseptic surgery are caused by thesame strain that colonise thatpatient’s nasal cavity. In exogenousinfections, bacteria come from out-side to predisposed epitopes, andthe main transmission route is viathe doctors’ and other personnel’shands; other routes (directly fromthe colonising flora of medicalteams or from the patient’s environ-ment) are obviously of minorimportance. The progress in medi-cine (e.g. intensive care, surgery,haematology, nephrology)and the increasing
UK - Two new kits designed to help engineers and contrac-tors comply with the demands of the HSC’s Legionnaires’ dis-ease ACoP, L8, have been launched by JS Humidifiers. Thesecompact, portable kits include equipment to monitor chemicallevels and microbes in most water systems, such as cooling tow-ers that are regularly dosed with biocides.
The JS L8C test kit includes a digital thermometer, digital pHmeter with buffer solutions, and digital conductivity meter with ref-erence solution, all offering fast accurate results, the firm reports.Other equipment includes reagents and indicators for water hardnessas well as chlorine, alkalinity, oxidising biocide and iron levels, plus dip slides for microbial test-ing.
The JS L8B is designed for lower risk water systems, where chemical treatment is not typicallyrequired. This basic kit incorporates free chlorine and pH level tests, a thermometer, a conductiv-ity meter and dip slides.
Each kit has a lightweight carry case, which includes instructions, dip slides, sample bottles andtubes, filter papers, syringes and stirrers.
Consumable items from the kits can be purchased separately and incubators, to provide theconditions recommended in L8 for dip slide development, are also available. Additionally, JS offersan UKAS approved water testing service for Legionella and a specialist risk assessment service forhumidifiers.
JS Humidifiers is offering 2000 FREE dip slides to those who would like to test the microbialcontent of their water systems as part of their monitoring programme. To claim free dip slides,maintenance engineers and facilities managers should call JS on +44 (0) 1903 850200.Details: [email protected]
10 EUROPEAN HOSPITAL Vol 12 Issue 1/03
Tests forLegionnaire’s disease

EUROPEAN HOSPITAL Vol 12 Issue 1/03 11
H Y G I E N E
Q:A:
How can I handle a growing case load with a shrinking staff ?
A s demand increases and resources tighten, it’s becoming harder – and more crucial – for radiologists to maximize productivity. Kodak solves this dilemma, with products and systems that give you better access to diagnostic information, integrate with your current equipment, and provide a platform for future growth. We listen to where you are going today, and where you want to be tomorrow. And then offer intelligent imaging choices across the entire film-to-digital spectrumto make it all happen. Customers around the globe depend on Kodak’s 100-year legacy in medical imaging. That same expertise can help you achieve success.
For more information visit www.kodak.com/go/health.
HEALTH IMAGINGA B E T T E R V I E W O F L I F E .
The RKI Guidelines specify thatpersonnel working in CentralSterilisation Services (CSS) musthave completed a training coursethat includes the guidelinesdrawn up by Hamburg’s Senate,and the Intensive Workshops 1-3,developed by the DGSV.
DGSV objectivesThe DGSV has about 500members, who are recyclingspecialists in hospitals. In comingyears, the society will update thecurricula for Intensive Workshops1 & 2. The society is alsodeveloping public relationsguidelines with hospitals, to gainsupport from management toput CSS quality into effect.Details: www.dgsv-ev.de or:www.rki.de
SURVEILLANCE IMPROVES MANAGEMENTSurveillance of nosocomial
infections has proved a valu-able tool for internal quality
management, said Dirk Zolldannand Sebastian W Lemmen, of theDepartment of Infection Control,University Hospital Aachen (UHA),describing a hospital infections sur-veillance system called KISS, devel-oped at their hospital since 1998.
KISS - provides references fordevice-associated nosocomialinfections and surgical site infec-tions. The KISS criteria are similarto the USA’s National NosocomialInfection Surveillance System(NNIS) for benchmarking. (FromJanuary 2001, according the coun-try’s new prevention Act, hospitalsmust perform targeted surveillancefor nosocomial infections).
At the 1,500-bed tertiary referralcentre - covering all clinical disci-plines and with nine specialisedintensive care units - a physiciantrained in infection control super-vises a nurse trained to carry outsurveillance according to the KISScriteria. Nosocomial infections arecategorised according to the defini-tions of the Centres for DiseaseControl and Prevention (CDC).
According to the team’s report,in intensive care units, surveillanceis performed for the three mostimportant nosocomial infections(bloodstream and urinary tractinfections and pneumonia), whichare associated with invasivedevices as the main exogenous riskfactors (central venous catheter,mechanical ventilation, urinarytract catheter). Patient days anddevice days are recorded daily byward staff. Nosocomial infectionsare identified by prospective chartreview twice a week, combinedwith participation in the infectiousdisease consulting service wardrounds once weekly. Device utilisa-tion ratios are calculated per 100patients, device-associated inci-dence densities per 1,000 days atrisk (use of central venouscatheter, mechanical ventilationand urinary tract catheter, respec-tively). For time requirements, aquarterly rotating intensive careunit surveillance system has beenestablished.
Surgery - Surveillance is per-formed in selected surgical proce-dures, established as indicators forsurgical quality management, such
as hip replacement or a coronarybypass. A record, for every patientundergoing the selected procedure,includes baseline information andoccurrence of specific risk factorssuch as wound class, duration ofsurgery and the American Societyof Anaesthesiology (ASA) score.Up to discharge patients are moni-tored - by chart review and wardrounds twice weekly - for theoccurrence of surgical site infec-tions. Using a composite index forpredicting risk of surgical site
infections after surgery, surgicalsite infection rates can be stratifiedaccording to the risk factors, theteam points out.
‘Interpretive feedback of the sur-veillance data is given in writtenand oral presentations to wardstaff and the department head.Thus, the unit-specific nosocomialinfection situation can be madeclear for ward staff. As a result, inour hospital, quality managementactivities, such as establishment ofevidence-based infection control
guidelines and quality circles, havebeen initiated. Surveillance dataare used for further risk factoranalysis and optimisation ofempirical antibiotic therapy. Inaddition, several specific infectioncontrol problems could be detectedduring the surveillance process,which led to specific interventionstrategies.’
Surveillance activities need care-ful planning, in terms of personneland time resources, they pointedout. ‘Essential surveillance compo-
nents are distribution of responsibil-ity, knowledge of classification,analysis and interpretation of sur-veillance data as well as the imple-mentation of interventional man-agement techniques due to theresults of the surveillance process.’
Dr SebastianLemmen

12 EUROPEAN HOSPITAL Vol 12 Issue 1/03
C A R D I O L O G Y
In the US about 450,000 people ayear die from sudden cardiacarrest, making this one of the mostcommon causes of death in theWestern world. In Germany thefigure is about 100,000. Generally,it is thought that in 80-90% ofcases, patients had tachycardiacdysrhythmias (ventricular tachy-cardia or ventricular fibrillation)prior to sudden death, whereasbradycardiac arrhythmias are notas significant.
One of the central objectives ofmodern cardiology is the preven-tion of cardiovascular diseases, theidentification of patients who arein danger because of life-threaten-ing cardiac dysrhythmias, but alsothe development of therapeuticprocedures that can treat acute,life-threatening dysrhythmias safe-ly and successfully and savepatients’ lives. Whilst the treat-ment of malignant dysrhythmiasby emergency medics and electroshock therapy (defibrillation) hasbeen a treatment used for danger-ous arrhythmias for many years,‘early defibrillation’ with semi-automated defibrillators by trainedfirst aid teams is often viewed asan experiment and not a wellthought-out therapy concept.However, first results from studiescarried out in Europe and the USshow that early defibrillation notonly makes sense but can also beused safely and reliably.
Survival chancesPatients who develop ventriculartachycardia or ventricular fibrilla-tion have a life-threatening illnessand may die. Worldwide examina-tions have clearly shown that theprognosis for those with cardiacarrest due to ventricular tachycar-dia or ventricular fibrillation isbad, and that only 5-8% of thesepatients will survive the event.Only quick, targeted action will
Award-winning Austrian innovation checks out NASA astronautsA pioneering innovation, awarded the AustrianInnovation Prize in January, promises previouslyinconceivable opportunities for diagnosis andmonitoring, particularly in internal medicine, cardi-ology and neurology, says the maker, CNSystems,based in Graz. The firm reports that its Task Forcemonitor is the world’s first diagnosis and monitor-ing system to determine all relevant heart circula-tion values for each individual heartbeat, using anon-invasive procedure that plots them in realtime.
The first two monitors were supplied to NASA,where they were used to investigate astronauts’cardiac circulation during parabolic flights (weight-less simulation). The monitor was also selected forfuture use on the International Space Station (ISS)crew.
The system measures, inter alia, the heart’sstroke volume (amount of blood pumped from theheart at each heartbeat), the peripheral vascularresistance as an indication of dilations or stricturesof blood vessels, the duration of a heartbeat, or
THE CASE FORearly defibrillationProfessor Hans-Joachim Trappe MD, of Medical Clinic II (specialising in cardiology and angiology), Ruhr University Bochum presents
heart rate, to the millisecond, as well as blood pres-sure and its course during a cardiac period.
The non-operative measurement procedure notonly provides details of the heart circulation sys-tem but also evaluates important informationabout how the brain controls the system - other-wise possible only at great expense and with con-siderable patient stress (using a pulmonary arterycatheter).The combination of four measuring/measurementmethods● continuous blood pressure measurement (beat-
to-beat)● impedance cardiography● high-resolution 2-channel ECG● oscillometric blood pressure measurement
also provides the opportunity to record the func-tions of the autonomic nervous system indirectlyvia the heart circulation measurement. Usingmethods applied in the chaos theory, it is possibleto sift out rhythms from apparently chaoticchanges in heart rate, blood pressure and stroke
ensure their survival.Indecisiveness, hesitation, helpless-ness or ‘therapeutic passivity’ willinvariably lead to the patient’sdeath. The ‘survival chain’, madeup of four part components (emer-gency call, basic first aid, defibril-lation, further treatment) is of vitalimportance.
Emergency callCalling for professional help is animportant part of the survivalchain. It is a prerequisite for theearly arrival of an ambulance thatfacilitates further treatment. It alsogives medical professionals at theend of the phone line a chance to
According to recommendationsfrom the Liaison Committee onResuscitation [ILCOR] and theAmerican Heart Association[AHA], cardiac massage should becarried out with a frequency of100/min, with the ratio from heartmassage to respiration of 15:2.
DefibrillationVentricular fibrillation is the mostcommon dysrhythmia, which cancause sudden cardiac arrest, lead-ing to the patient’s certain deathwithout defibrillation.Defibrillation, an ‘electric’ shockprocedure, is carried out with adefibrillator via two electrodes,
public semi-automatic defibrilla-tors without any training.Although there are some promis-ing results from studies of this useof the equipment, it is better tocomprehensively train as manyfirst responders as possible.
Worldwide experiencesThe concept of early defibrillationhas been known in the US formany years, and first respondersare integral to the survival chain inmany regions. In October 2002,the New England Journal ofMedicine published two importantstudies indicating the success ofearly defibrillation by security staff
tive but also safe, when making adecision as to whether a patient issuffering from ventricular fibrilla-tion or another, non-treatablearrhythmia, and to ensure thatshocks are not given when there isno life-threatening arrhythmia.
A recent study in Chicago carriedout over a 2-year period reportedthat of 21 people who suffered car-diac arrest, 18 had prior ventricularfibrillation (New England Journalof Medicine 2002; 347:1242-1247).Out of four patients who where notin the vicinity of an AED when car-diac arrest occurred and whoreceived no shock treatment, nonesurvived. Three other patients suf-
BRUSSELS - The first European human implant of the Vitality AVT - acardiovertor defibrillator (ICD) - was carried out at the UniversityHospital Dusseldorf, soon after the Guidant Corporation obtained theEuropean CE Mark for the device this January. The firm reports that, at30cc, the Vitality AVT is the smallest dual-chamber full-featured ICD inthe world. ‘It combines leading, automatic ventricular and atrialtherapies with three-channel energy-efficient FullView EGM capabilitythat is important in customising treatment for ICD patients.’Footnote: In February, Nicky Spaulding became president of Guidant Europe, Middle East,Africa and Canada - a post based in the US firm’s Belgian offices
The multi-purpose monitorvolume from one heartbeat to another, which pro-vides valuable information about brain functions,the firm pointed out.
Other areas of application include internal med-icine, neurology and cardiology - to replacecatheters, non-surgically adjust pacemakers,explain sudden and unaccountable unconscious-ness, offer real time monitoring in the ICU or dialy-sis units. The monitor is also used to investigatedrugs that affect circulation, the firm says, addingthat in addition to medical benefits, surgical coststreatment time, data handling and purchasing canbe reduced.
The European reference list includes numerousuniversity and specialist clinics in Germany (e.g.The Charity, Berlin; Heart and Diabetes Centre, BadOeynhausen), and others in Belgium, France, Italy,Portugal, Spain, Britain and Austria. Following FDAlicensing, the firm believes US opportunities will begood, as reimbursements are granted for patient-friendly non-invasive heart circulation measure-ments.
CE mark for defibrillator implant
fered further ventricular fibrillationand did not recover although AEDswere used within 5 minutes. 11patients with ventricular fibrillationwere successfully defibrillated; 56%of these patients with ventricularfibrillation followed by successfulAED defibrillation were still alive ayear after the event and had noneurological damage.
The Early Defibrillation inGermany project
The introduction of early defibrilla-tion in Germany, compared withthe US, has been late and relativelyslow. Apart from a few institutionswith semi-automatic defibrillators,such as the Stadium Gelsenkirchenor Munich’s underground stations,a model project, one of the largestin Europe, was introduced to theGerman public on 13 December2002. In a co-operation betweenthe German Cardiac Society, theGerman Heart Foundation and theFraport AG Frankfurt, Terminal 1of the Rhein-Main Airport inFrankfurt/Main is to be equippedwith 20 AEDs. Around 2000 firstresponders (500 airport workersand 1500 members of the federalborder guard) are to be trained andavailable. This scientifically moni-tored project will eventually beextended to all parts of FrankfurtAirport.
Conclusions and outlookThe concept of early defibrillationto prevent sudden cardiac death iswithout doubt one of the mostimportant projects in modern cardi-ology. The fascination of this thera-py is that a rather complicatedmeasure is being simplified so thatinitially first responders can use it -then, later, so can an untrainedpublic. First results and experienceshave not only confirmed the valueof this concept but also actually farexceeded expectations. We canhope that experiences initiallygained in the US will meet with thesame enthusiasm in Germany, ashas been seen in other Europeancountries. However, the introduc-tion of early defibrillation and itsspread in this country requires theco-operation of everyone involved,as the concept can only be compre-hensively introduced if everyoneagrees this is an important strategyto prevent many unnecessary, sud-den cardiac deaths.
advise the caller on any first aidmeasures he/she may be able togive.
Basic aidFor a patient to survive, the timeperiod between cardiac arrest andthe onset of cardio-pulmonal rean-imation must be as short as possi-ble. We know that the humancerebral function can only berestored within 8-10 minutes ofthe arrest. So the time period fromthe occurrence of cardiac arrest tothe initial reanimation attemptsare a critical component. Artificialrespiration and cardiac massageare essential basic measures, whichshould be initiated on the uncon-scious patient as soon as possible.
attached to the patient’s chest andgiving a DC impulse of 8-12 ms.This impulse leads to the fibrillat-ing cardiac muscle cells (nowmechanically arrested and notpumping blood) restarting andresuming electric and haemody-namic activity.
Who should defibrillate?There are two kinds of early defib-rillation - one carried out bytrained first aid teams (firstresponders), the other carried outby members of the public withaccess to a defibrillator (publicaccess defibrillation). First respon-ders are trained helpers such assecurity staff, policemen, firemenetc. trained in measures of cardio-pulmonal reanimation and in han-dling a semi-automatic defibrilla-tor (ref.: German Medical Council,2001; 98:1211] 4th May 2001). Inplaces where large crowds gather,such as theatres, stations, sportscentres, airports, departmentstores etc, staff should be trainedas first responders.
Public access defibrillation isbased on another concept - peoplein the vicinity of automated exter-nal defibrillators (AEDs) use these
in casinos and airports.In various casinos in Nevada,
AEDs were used on 105 patientswho initially suffered ventricularfibrillation. 56 of these (53%) sur-vived and discharged from hospi-tal. The survival rate was 74% forthose patients who had been giventheir first defibrillation withinthree minutes of the onset ofsymptoms and 49% for patientswhere AED shocks were com-menced more than three minuteslater.
In a further US study, AEDswere used on 200 patients whohad documented loss of conscious-ness on a plane (191 patients) orwithin an airport terminal (9patients). With 14 patients, theAED revealed ventricular fibrilla-tion, which was successfully treat-ed in 13 patients; in the other oneno treatment was given as thepatient was in the very final stageof a terminal cancer. In all patientswho did not appear to suffer fromventricular fibrillation, the equip-ment was not recommended andnot used.
This study impressively provedthat the use of AEDs by trainedfirst responders is not only effec-

EUROPEAN HOSPITAL Vol 12 Issue 1/03 13
I N T E N S I V E C A R E
Proven outcomes. It’s what we are helping
to deliver right now. Across the entire
healthcare continuum. Outcomes that result from
truly efficient workflow. Outcomes that dramatically
improve your bottom line. Outcomes that lead to
a level of care that feels exceptional to the patient.
And the care provider. Proof positive of the value
of integrating medical technology, IT, management
consulting and services. In a way that only Siemens
can. Visit SiemensMedical.com/proof. See what we
see. Tangible solutions. Proven outcomes.
A9
11
00
-M-Z
75
4-1
-76
00
we see a way to do 50% more exams with only 25% more staff
Siemens Medical Solutions that help
What do you see?
we see a way to increase patient satisfaction by improving scheduling accuracy
we see a way to speed radiology order time by 3 hours
we see a way to get reports to physicians 12 hours faster
Helmut Beuster, Head of Sales Support, Draeger ANSY Ltd, and Michael Clarkson, of DomnickHunter Ltd, discuss uncertainties, misunderstandings - and the intricacies of the on-going debate
Medical air came under thePharmaceutical ProductsAct since April 2000,with a transition period
until August 2002. For hospitals, thismeant that the quality requirementsupon air for artificial respiration rosesharply and that they should alreadyhave invested in the production andprocessing of compressed air.However, because some professionalrepresentations advised waiting andseeing for the present, a feeling ofuncertainty prevails. Additionally,the sense of the new quality require-ments, partly characterised by tech-nical misunderstandings, is beingdebated.
The state of affairs is clear - untilJanuary 2000, the first version of thestandard DIN EN 737-3 (enforcedfrom November 1998) regulatedrequirements on medical air, usedboth in artificial respiration and todrive medical equipment. Includedamong this standard’s most impor-tant requirements was an atmospher-ic dew point of approximately -25ºC.This is about equivalent to a dewpoint under pressure of + 5ºC, whichwas achieved using commerciallyavailable refrigeration dryers - andwhich hospitals almost always used,until then. However, a draft of a sup-plement to the EuropeanPharmacopoeia, published in 1998,classified ‘air for medical applica-tions’ as a pharmaceutical, whichplaced far higher requirements uponit. The amount of water vapour hadto be 60 ppm maximum, equivalentto an atmospheric dew point ofapproximately - 47ºC. In addition,the draft demanded that the residualoil content be 0.1 mg/m3, maximum.The bill also cited maximum levelspermitted for carbon dioxide, carbonmonoxide, nitrogen oxides and sul-phur dioxide in air used for artificialrespiration but did not make anyspecifications on the separation ofparticulate matter.
The transition period ended at thebeginning of August 2001.
As a result, the legal situation wasunclear from the beginning. Therewere two different standards for oneand the same medium. So, in the sec-ond edition (January 2000) of theharmonised European standard DINEN 737-3, passages concerning med-ical air quality were deleted. Thisunclear legal situation did not enduntil a notification, in April 2000,for the 2000 Addendum to theEuropean Pharmacopoeia. The 2000Addendum became valid in August2000. A transition period was grant-ed up to August, the following year.
The consequence for hospitals wasthus clear: They must invest, becausein the majority of cases these require-ments cannot be achieved by usingpresent systems for production andprocessing. Experts estimate thatupgrading compressed air systems
for all (German) hospitals withadsorption dryers, filters and cat-alytic converters for converting car-bon monoxide, will cost into thedouble-digit millions. Operatingcosts are also increasing for com-pressed air plants because part ofthe medical air produced is used toregenerate the necessary adsorptiondryers, and additional hopkalite fil-ters must be replaced regularly.
Medical air from the pharmacyOn publication of this law, the
industry felt challenged to developspecial processing equipment thatwould reliably meet medical airrequirements. However, althoughthe time limit for the transitionapproached and expired last year,hospitals hesitated about invest-ment - and many still do. This maybe due to the fact that responsibili-ty was rearranged - since medicalair is now considered a pharmaceu-tical - production of medical air isnow the responsibility of pharma-cies supplying hospitals. Thus phar-
macies have been confronted withan entirely new and differentresponsibility.
Since mid-2002 discussions onthis subject have focused on objec-tive technical arguments but alsobordered on the philosophical, thusseveral articles in medical engineer-ing journals, included one advocat-ing ‘just don’t rush matters!’, andsome authors advising hospitals notto put the new requirements intoactual practice. This interpretationof the law may surprise some - thePharmaceutical Products Act is inforce, so ignoring valid law isexplicitly recommended!
continued on page 14
medicalAIR

14 EUROPEAN HOSPITAL Vol 12 Issue 1/03
I N T E N S I V E C A R E
Debate: What is air?This approach might represent awish and the hope that thePharmaceutical Products Act willlater be amended. Key question: Isthe air used to provide patientswith artificial respiration actually apharmaceutical? Representatives ofthe ADKA (Federal Association ofGerman Hospital Pharmacists)believe that compressed air formedical purposes should not be
ly harms patients. Literature on thiscites as a requirement for long-termartificial respiration an air temper-ature of 22º to 37ºC and watervapour content of 15,800 to43,900 ppm - a far higher figure!Consequence: air for artificial res-piration must always be humidi-fied!
All users know these generalparameters. The respirators neces-sary are therefore all equipped withhumidifying systems to meet thoserequirements. The amount of watervapour in compressed air, accord-ing to the outdated specifications ofthe standard, was 630 ppm, thePharmacopoeia requires 67 ppm.Medical air therefore must behumidified by 563 ppm more,which is entirely negligible forapplications on patients, for whomthe amount of water vapourrequired between15,800 and43,900 ppm.
alytic converters, thus saving onoperating costs. It is also due to afundamental belief that theamount of harmful substances inair should be limited, when usedfor artificial respiration. Without adoubt, harmful substances in airstress an organism. From the tech-nical viewpoint, however, conden-sation should definitely be avoidedin the tubing systems for medicalgases. When operating surgicaltools driven by compressed air(e.g. air motors) no condensationmust form inside the drive turbineeither - water condensation coulddestroy the turbines and/or watercould drip out of the surgical tooland into a patient’s body.
Bottom line: Clean respiratory airbenefits patientsThe law demands that hospitalscomply with pharmacopoeia spec-
USA - Life monitoring equipment and software calledeICU, produced by Visicu Inc, has reduced intensive caremortality rates at Sentara Norfolk General Hospital,Virginia, by 25% and shortened the average length of stayfor patients by 17% - according to an independent study,by Cap Gemini, Ernst & Young (CGEY). ‘Mortality ratesplunged when our around the clock reaction time becamea matter of seconds,’ Rod Hochman MD, Senior VicePresident and Chief Medical Officer for Sentara Healthcaresaid.
Intensive care patients at the hospital are now continu-ously monitored and managed by intensivists who workonline from a remote eICU location when primary carephysicians are not at the patient’s bedside. Through a net-work of cameras, monitors and two-way communicationlinks, doctors and critical care nurses at the eICU com-mand centre make virtual rounds of patients. Intensivistscan monitor the condition of patients, check vital signsand communicate with hospital staff, patients or familymembers.
The eICU enables command centre computers to quick-ly establish a ‘base line readout’ of each patient, so evenslight changes in vital signs are detected and treated.Dramatic changes in vital signs trigger automatic alerts tointensivists or the nurses who prompt an immediate
Electronic monitoring drops deaths 25%
Sepsis therapy ups survival rates
response from on-site hospital staff. This is said to havesaved the life of more than one patient per week in twoseparate ICUs.
The report said per patient costs dropped $2,150, basedon reduced patient expenses and increased ICU capacity,and the system has generated c. $3 million in savingsabove annual programme costs.
‘What is most exciting is that we are only scratching thesurface of possibilities for remote, technology-enabledcare,’ said Brian Rosenfeld MD, Chief Medical Officer ofVisicu Inc, who, with another intensivist from JohnsHopkins, co-founded the Baltimore- based firm in 1998.Details: www.visicu.com.
considered a pharmaceutical, but afoodstuff. And the DKG (GermanHospital Association) believes theEN 737-3 requirements haveproved their value or, at least, nonegative consequences are knownabout air quality specified by this.The DKG has turned to the BMG(Federal Ministry of Health) toobtain an exemption, so that med-ical air would not be covered by theEuropean Pharmacopoeia.However, a decision has yet to bemade on this. Those studyingHospital Equipment Managementat the Giessen-Friedberg HigherTechnical College have written tothe BMG requesting that MinisterUlla Schmidt amend and/or supple-ment the Medical Air 2000 mono-graph regarding water vapour con-tent.
Due to the many debates, fourpetitions on revising the mono-graph (three German, one Swiss)were submitted to the 9G - the rel-evant commission of experts. At itsStrasbourg conference (September2002) in-depth discussions did notresult in any amendment.
Requirements that over do it andmight even be harmful?
The ‘wait-and-see’ advocates alsoraise material objections to theimproved quality requirements. Aparticularly important argument isthat an atmospheric dew point of -46ºC (equivalent to 67 ppm ofwater vapour in one cubic meter ofair) not only overdoes it but actual-
The technical debate - frequentfalse arguments The dryer compressed air the fewerharmful substances it can bind.That is one of the purposes of pro-cessing for compressed air, and it isnot a contradiction to re-humidifycompressed air purified in this way,to provide artificial respiration -providing no new, harmful sub-stances (e.g. bacteria) are added.However, there is another reasonfor the requirement for residualhumidity in compressed air: to reli-ably withhold poisonous amountsof carbon monoxide the air mustflow through a chemical catalyticconverter, turning carbon monox-ide into carbon dioxide. Filters ordryers cannot do this. However,this converter is only effective long-term if air flows through it with adew point of - 40ºC or less.Loading it with humidity substan-tially reduces its service life. Instandard systems for producingcompressed air, only adsorptiondryers can guarantee a dew point of- 40ºC.
Artificial respiration requiresclean airWhat does this technical data meanin the debate? To the expertsinvolved it is certainly not a matterof providing patients with the driestair possible. The required dewpoint under pressure is due to atechnical necessity to preserve theservice life of carbon monoxide cat-
Long term data on the use of Xigris [drotrecogin alfa(activated)], the only adjuvant therapy licensed for thetreatment of adult patients with severe sepsis and mul-tiple organ failure in addition to standard therapy, haveconfirmed increased chances of patient survival. Resultsfrom the placebo-controlled Prowess Study, presentedby Professor Rolf Rossaint, at the GermanInterdisciplinary Congress for Intensive Care andEmergency Medicine 2002, showed that the patients,monitored over a period of up to 2.5 years, also hadincreased long-term survival rates. Using the therapy,the death risk for patients with severe sepsis was low-ered by about 20%. However, it remained to be seen howchances of survival developed after the initial 28-daymonitoring period.
In the multi-centre observation study, survivingpatients who had taken part in the Prowess Study werebeing continuously monitored. Between September2001 and April 2002, in the double-blind study, 1,221patients were monitored. This corresponded with anobservation period of 15-45 months following thepatients’ initial inclusion in the study. Patients who hadbeen treated with drotrecogin alfa (activated) not onlysurvived the acute phase of severe sepsis more often(p=0.005) but also the first 90 days in the hospital fol-lowing the onset of the illness (p=0.048). ÇAfter the 90-day period, mortality is determined by other factors,such as age and general health, which are not directlyconnected with severe sepsis as such,’ the professorpointed out. Even if the entire observation period of 2.5years is taken into consideration, chances of survival
remain increased for those patients receivingdrotrecogin alfa (activated) during the acute phase ofthe illness.
Because of the increased rate of survival, more ofthese patients could be sent directly home followingtheir hospital stay, with no additional treatment nec-essary.
Professor Rossaint concluded that treatment forsepsis revolves around five factors: sourcecontrol/administration of antibiotics, early, target-orientated circulation management, artificial respi-ration, endocrinal and metabolic management aswell as administration of recombinant human acti-vated protein C, drotrecogin alfa (activated)GUIDELINES - Private lecturer Ernst Kuse, of Hanover,introduced guidelines developed by the ICU atHanover’s Medical University.Source: Symposium ‘rhAPC: Experiences in clinical use’.Details: [email protected]
continued from page 13
medicalAIR
ifications. Many hospitals farexceed the time limit granted fortransition (August 2001). Reliablecompliance with air quality charac-teristics is only achieved, particu-larly for the carbon monoxidelimit, by a combination of anadsorption dryer combined with acatalytic converter (hopkalite fil-ter).
Recommendation Due to legal requirements, com-pressed-air control units should beupgraded immediately with adsorp-tion dryers. Hospital technicaldirectors should contact their phar-macy suppliers and reach a writtenagreement on the process‘Pharmaceutical Production - Airfor Medical Purposes’.
An organisation chart should bedrawn up to show instances ofaccountability concerning gases for
medical purposes. This also appliesto supply systems for oxygen,nitrous oxide and carbon dioxide.In addition, work instructionsshould be prepared for inspectionand production of these pharma-ceuticals. Maintenance contractsshould be concluded for the main-tenance of compressed air systems.Maintenance should be document-ed, for submission in case of anyinspection by the responsible phar-maceutical monitoring and inspec-tion offices.
Hospitals should not only imple-ment these measures for legal rea-sons, but because air polluted byharmful substances is a stress onpatients’ whole organisms. Cleanrespiratory air, free of harmful sub-stances, is thus an important aspectthat contributes to the quality ofmedical care provided and thus alsoeffect quicker patient recovery.

EUROPEAN HOSPITAL Vol 12 Issue 1/03 15
I N T E N S I V E C A R E
Because you careEmergency Care · OR/Anesthesia · Critical Care · Home Care
M E D I C A L
You can hardly miss the EvitaXL’s new screen. It’s bigger and better than ever with curves, loops,short trends and trends that are easier to read and an intuitive human interface that lets youconcentrate on caring for your patient. But size isn’t everything. When it comes to first-class venti-lation therapy, it’s content that counts – as you’d expect from this extension to the Evita familywith its ideal balance of innovation and continuity. After listening to your needs, we’ve intro-duced a number of improvements that set new standards in screen content. Our online manualsupplies you with cause-and-remedy guidance in every possible situation. Directly accessible settings are easier and quicker to operate. And enhanced configurability lets you choose preciselythe features you need.
EvitaXL – a bigger and better screen to make life easier for you.
Sorry, but this ad is too small for our
www.draeger-medical.com
Sorry, but this ad istoo small for our
XL
BELGIUM -J e a n - L o u i sVincent, Head,Department ofIntensive Care,Erasme Hospital,
Free University of Brussels, points outthat over 4,500 participants comefrom all global points to attend thisannual symposium. These includeintensive care physicians, anaes-thetists, cardiologists and pneumoniaand emergency care specialists.‘Indeed,’ he adds, ‘since its birth some23 years ago, this has grown tobecome the leading meeting in itsfield, providing a forum for allinvolved in these disciplines to pre-sent, discuss and debate the mostrecent results and discoveries.’
‘Our faculty for 2003 includesalmost 200 physicians, many interna-tionally recognized, but we also liketo encourage input from likely futureleaders.’ Sepsis - This year’s reports onadvances will include: new interven-tions and management strategiesshown to improve outcome in cases ofsevere sepsis or septic shock, includ-ing drotrecogin alfa (activated), mod-erate doses of corticosteroids, earlyresuscitation, and tight control ofblood glucose levels. Other agents stillin early phases of clinical testing willalso be discussed, as will new defini-tions and grading systems for sepsisproposed last year, which include thePIRO system.Microcirculation - ‘Recently, bettermonitoring of the microcirculationhas become possible, via minimallyinvasive optical methods (orthogonalpolarisation spectral imaging), using asimple probe under the tongue.Although the mouth may not typical-ly be an at risk body region duringacute illness, it is easily accessible - themicrovasculature is available immedi-ately below the mucosa.Microcirculatory alterations seenthere may be present throughout thebody. Recent studies suggest thatexploring microcirculation with thistechnique could help to guide therapyin the critically ill.’Extracorporeal techniques - Results ofnew studies will be presented onextracorporeal techniques, used tosupport the failing kidney as well asthe liver. In severe infections, thesetechniques may also remove media-tors. Blood transfusions - A large Europeanstudy (the ABC), which involved3,534 patients from 15 WesternEuropean countries, recently reportedthat 37% of patients received a bloodtransfusion during their ICU stays.However, blood transfusions remaincontroversial. Possible alternatives,such as erythropoietin, will be dis-cussed. Ethics - are also on the agenda. Themajority of deaths in the ICU are pre-ceded by a medical decision to with-hold and/or withdraw life supportsystems. These decisions, althoughremaining a medical responsibility,should be shared by several individu-als within the ICU team and optimal-ly involve discussions with the nursingteam, and with the patient whereverpossible, Professor Vincent points out.
In a study published in the official journal ofthe Society of Critical Care Medicine (Nov.2002), members of the Barnes-JewishHospital Infection Control Team report thatthey followed all patients admitted to theICUs from October 1999 to September 2001,surveying for the occurrence of ventilator-associated pneumonia (V-AP). 191 casesoccurred in 15,094 ventilator days (12.6 per1000 ventilator days) in the 12 monthsbefore the education programme. After theprogramme, the rate of V-AP decreased to 81episodes in 14,171 ventilator days, a decline of
LEARN TO BEAT PNEUMONIAdepartment of respiratory care services.
Many studies suggest strategies for theprevention of V-AP but many of these inter-ventions are not widely implemented inICUs. The most common reason for not fol-lowing recommendations was disagree-ment with the interpretation of clinical tri-als, lack of resources, and costs associatedwith implementation of specific interven-tions.
*Critical Care Medicine is a peer-reviewed,scientific publication
Cases of ventilator-associatedpneumonia can decrease dramatically
23rdInternational Symposiumof Intensive Care andEmergency Medicine
18-21March
57.6%. In addition to reducing pneumonia,the program also resulted in cost savingsestimated as between $425,606 and $4.05million.
The programme, directed at respiratorycare practitioners who care for mechanicallyventilated patients and ICU nurses, anddeveloped by a multidisciplinary task force,consisted of a ten-page study module on riskfactors and practice modifications involvedin V-AP, training at staff meetings, and for-mal lectures. Fact sheets and posters werealso posted throughout the ICUs and the

U R O L O G Y
Professor D Frohneberg (below), Director of the Urology Clinicat the Karlsruhe Academic Teaching Hospital, Freiburg University,describes aspects of new urology guidelines to be presented in Madrid
The 18th EAU Congress
SPAIN. 12-15 MARCH - In the past seven years over 130 urologyexperts, supported by the European Association of Urology(EAU) Board, and governed by the Health Care Office, success-fully published guidelines covering almost all interests andsubjects in European urology - including urogenital trauma,neurogenic bladder disorders, renal transplantation and painmanagement.
Additionally, guidelines on specific subjects and problemsof the ageing male are progressing.
Traumatic injuries to the genitourinary tract are seen in 2.2- 10.3% of patients admitted to hospitals. Standardisation andclassification of these injuries help to select appropriate ther-apy and predict best treatment results. Thus establishingrules and a scaling system for diagnostic measures and initialemergency treatment is extremely important to guaranteeadequate therapy for a patient often suffering multi-discipli-nary traumatic injuries.
European experts in urogenital trauma will present adetailed summary based on a review of worldwide literature.
On the other hand congenital courses of neurogenic blad-der dysfunction, such as myelomeningocele, produces dam-age to urogenital organs, which, in the long run are compara-ble with trauma-induced paraplegia and lesions of the nervalplexus of the small pelvis after pelvic surgery, for example.Toxic neuropathia, in diabetic patients for example, may alsoresult in neurogenic bladder dysfunction.
Routinely, those cases involve a time-consuming diagnos-tic process to evaluate neurophysiological disorders of blad-der function. Additionally, the lesions may not be stable dur-ing their lifetime. Adequate management of lower urinarytract symptoms often mislead, or disguise probably severedamage to the upper urinary tract. Therapeutic options in theearly treatment phase avoid renal damage and renal failure
Memorial Sloan-Kettering CancerCentre praises itself as the world’soldest and largest institutiondevoted to prevention, patientcare, research and education inoncology. It is presently one ofonly two places in the world thatoffer MR spectroscopic imaging ofthe prostate gland - the Universityof California, San Francisco(UCSF) being the other. GeneralElectric is now devising the
CC: What is your department’s mainfocus?LK: There are several areas of exper-tise. This is the internationallyknown centre for prostate cancer.Treatments ranging from traditionalsurgery to non-surgical approaches,including laparoscopic and robotic,gene therapy research, radiationtherapy, and genetic studies to deter-mine who may develop prostate can-cer and who may be treated earlier,perhaps non-surgically.
In our prostate cancer procedure,the technique is to remove theprostate and spare the nerves thatcontrol erections. This was devel-oped here by Dr Patrick Walsh, andalso perfected here. So, we have per-haps the world’s best rate for pre-serving potency of the nerves. Weare now looking into other ways topreserve them with less invasivesurgery. Presently the outcome is not100%, but it varies depending uponthe case. Older patients have lesshope of having erections thanyounger men. Also, there are moreextensive cancers, and sometimesthe nerves must be removed to com-pletely remove the cancer - the pri-mary goal of this surgery:
We also have a very active pro-gramme in minimally invasivesurgery for kidney tumours and
blockages. This can be done with-out making a big incision -
during lifetime therapy. Both surgical and medicalapproaches must be used differently or combined.
The guidelines on urogenic bladder dysfunction offer acomplete overview of the actual scientific publications, eval-uated by experts in this field.
In addition, an exchange of knowledge and attitudes inthe treatment of patients with acute and chronic pain issummarised in the section on pain management.
An interdisciplinary team - urologists, anaesthetists andpain specialists - has guaranteed an actual review of the lit-erature that results in recommendations and therapyschemes.
Last but not least experts in renal transplantation volun-teered and co-operated in establishing the guidelines onrenal transplantation. Due to different European healthcaresystems these experts have been very ambitious to provideour urologists with guidelines on the basis of an expertreview of all literature in this field.
All medical professionals must be aware of governmenttendencies to regulate medical quality and patient informa-tion on an official basis, which often bypasses the advice ofthe scientific medical associations. Nevertheless, this almostcomplete list of urological guide-lines provides urologistswith the best therapyoptions, and also can pro-vide patients and offi-cials with appropriateand adequate guidelinesand recommendationsthat are renewed on a reg-ular basis within one to twoyears of follow up.
MR spectroscopicprostate gland imaging
‘We look at exactly where thetumour is located and how far ithas spread, so we can then make abetter decision as to the furthercourse of treatment,’ said DrHricak.
The alternatives are surgery orradiation therapy. MRSI not onlyhelps in deciding the proper choiceof treatment, but also in treatmentplanning. ‘In the case of radiationtherapy, we really look at thelocation of the tumour, and whenthey proceed with radiationtherapy, under guidance of MRSI,there is more certainty that theexact tumour area is covered.’Before surgery is performed, MRSIaids in deciding whether to excisethe neurovascular bundle,depending on the tumour’slocation. This type of imaging isalso used for local recurringcancers, as well as for patients
only half the picture -”well,probably more than half, but atleast we say so here,’ she added,laughing.
MRSI looks at membraneproliferation via a visible ratio ofthe metabolites choline and citrate.Depending on the elevation of thisratio, insights into the state of thecancer can be made.
Unlike FDG, a radionuclideglucose metabolite used in PETscanning, ‘... the choline to citrateratio is very good at distinguishingmalignant from healthy tissue’,said Dr Steven Larson, Chief ofthe Nuclear Medicine Service atthe Centre. ‘MRSI now helps indefining better degrees ofspecificity, since tumours are morelikely at certain metabolic ratios.’Dr Larson sees the most promisingbenefit of MRSI to be in helpingsurgeons to remove the right
in a clinical setting. By assuming amore a general leadership andmentoring role, Dr Hricak nowwants to help others chart a courseto excellence in imaging scienceand clinical care. ‘Understandingtechnology is important, buthelping to develop a generation ofyoung scientists and physicians isessential for our future,’ she said.Her work now involves helping toopen doors for junior scientists andphysicians, to inspire them, keepingher goal for the advancement ofclinical care in mind.
She very much hopes that MRSIwill become a standard addition toMRI in the care of patientsdiagnosed with prostate cancer.However, she could not be certainthat this will be the only exciting newimaging modality widely used in thefuture. ‘If you look down the line fiveyears from now, molecular imagingwill make a great breakthrough inour ability to detect cancer, predictoutcome and really design patientspecific therapy, really tailored to theindividual. We hope that will comewith molecular imaging.’
laparoscopically. For some smallertumours, we can now just put a needleinto the tumour using local anaesthe-sia, then destroy it with various ener-gies.
We also have a group working onincontinence - controlling urine - andwe are working with our gynaecolo-gists to find new ways to help peoplewith urinary leakage.
In addition we offer a variety ofpost-medical and surgical treatments,to help men with enlarged prostates tourinate better.CC: Would you describe the depart-ment’s latest research?LK: My main area is in minimally inva-sive surgery and robotics. Our labora-tory is working on developing roboticdevices that will allow us to do surgerythrough much smaller incisions and,hopefully, eventually no incisions.
There is technology now - in somecases we can destroy tissue inside thebody without making any incision.This is experimental, but we hope tomove that along.
We are also very interested intelemedicine, to care for patients overlong distances, so they don’t have toleave home and travel far. Our labora-tory also works with telerobotics, sowe can actually do procedures at longdistances. CC: How does laparoscopic surgeryhelp kidney cancer and live donortransplant patients?
Saving nerves and
NEW! Dr Hricak witnessed the evolutionof radiology from simple x-rays to
ultrasound and MRI
software as a clinical package forgeneral use.
Dr Hedvik Hricak, Chairman ofthe centre’s Department ofRadiology, is a Croatianimmigrant who became aradiologist in the 1970’s. Soonafter Dr Hricak came to theCentre in 1999 from the UCSF,where the first clinical magneticresonance unit was developed inthe US, magnetic resonancespectroscopic imaging of theprostate gland was offered atMSKCC. The clinical trial, whichstarted in January 2000, hasenrolled 980 patients to date, mostwith previously diagnosed cancerof the prostate gland.
The majority of prostate glandcancer patients who come toSloan-Kettering are offered MRSI.
with an elevated PSA and threeconsecutive negative biopsies. Inthose cases, MRSI and MRI areoffered, and a biopsy is guided byfindings on the MRI.
‘MRSI can never be used inisolation,’ Dr Hricak points out.MRI offers outstandinganatomical information, whileMRSI only delivers metabolicinformation. Combining the twointo one provides a more accuratepicture of the tumour’s location -far better than MRI alone, which,according to Dr. Hricak, ‘... gives
regions without damaging neuralstructures around the prostategland. MR spectroscopic imagingis also widely used in other areas,such as the brain and heart.
Dr Hricak emphasises that it isvery difficult for the untrained eyeto accurately read imagespresented by MSRI, and refers toseveral studies that have showngreat ‘inter observer variability’.She pointed out that it takes timeto learn, and that there is a greatneed to train future physicians towork with emerging technologies
EH correspondent Karen Dente interviewed Dr Hricak at the Cancer Centre
Hedvick Hricak
16 EUROPEAN HOSPITAL Vol 12 Issue 1/03

EUROPEAN HOSPITAL Vol 12 Issue 1/03 17
U R O L O G Y
BOWA-electronic GmbHNehrener Strasse 4-6, D-72810 Gomaringen, Tel. +49 (0) 7072-6002-0 Fax +49 (0) 7072-8719, e-mail [email protected], Internet www.bowa.de
• computerized clinical unit
• superior cutting performance by spark regulation "arc-control"
• allows bipolar cutting
• 4 individual outputs for monopolar and bipolar instruments
• high current coagulation "LigaSafe" optionally
• special programs for TUR, cardiac surgery, microsurgery, argon coagulation
The future is arc !
BOWAelectrosurgery for the 21st century
Focusurinary tract infections
BUDAPEST - Urologists, clinicalmicrobiologists and infectious dis-ease specialists from 32 countriesmet in January for the ‘Hot topicsin urinary tract infections’ sympo-sium. Part of a series, Hot Topicmeetings are organised by TheEuropean Society for ClinicalMicrobiology and InfectiousDiseases (ESCHMID) in collabora-tion with various organ-related spe-cialist societies. The meeting result-ed from collaboration with theEuropean Society for Infections inUrology (ESIU), is a division of theEuropean Association of Urology(EAU).
Urinary tract infections (UTI) areamong the commonest infectionsseen in the community and in hos-pitals. In the USA over eight mil-lion cases of cystitis occur annually,and over 100,000 patients (95%women) are hospitalised for acutepyelonephritis each year.
UTIs are by far the most commonnosocomial infection (NAUTI), dueto the frequent use of urinarycatheters. In urology departmentsNAUTIs are also caused by the rel-atively contaminated location ofurological surgery with instrumentsintroduced to the urinary tract, fre-quent use of urinary catheters anddrains and the use of intestine forreplacement surgery. Large propor-tions of urinary stones relate topathogens in the urinary tract. Forthese reasons effective antimicro-
bial prophylaxis is extremelyimportant in urological surgery.
Antimicrobial resistanceSome patients have special risk fac-tors for developing and maintain-ing UTI, which also make a casemore difficult to treat. Commonrisk factors are diabetes, immuno-suppression, urinary retention andcatheters. These complicated UTIgenerally cannot be cured unlessthe underlying condition isresolved. Repeated courses ofantibiotics are often administered,resulting in drug resistance amongpathogens.
Most cases of uncomplicated UTIare successfully treated, with feweasily measurable, seriously adverseevents in the course of the disease.However, the incidence of UTI andNAUTI, the pathogens involvedand resistance patterns can be easi-ly registered and have becomeimportant benchmarks for infec-tion control and hospital health-care. Furthermore, this is extreme-ly important information, becausemost courses of antibiotics are pre-
scribed for UTI on an empiricalbasis, before the results of bacterio-logical culture are known.
In Budapest, Kahlmeter (Sweden)presented results from an interna-tional community-based study onantimicrobial resistance amongpathogens causing cystitis. In somecountries in Southern and EasternEurope the resistance rates to fre-quently used antibiotics is a causeof concern. Consequently, morebroad-spectrum antibiotics must beprescribed, and within hospitalsresistant strains threaten the effectof peri-operative antimicrobial pro-phylaxis.
Seeking new antibiotics andadministration regimensIn the first decades after WWII,doctors saw new antibiotics devel-oped at only a few years’ interval.Today no new antibiotics can beseen in the horizon. Thus it is ofparamount importance to keep theuse of currently available antibi-otics under scientific control.
During the meeting Marchese etal (Italy) presented an assessment ofFosfomycin, a relatively new mem-
brane active peptide agent. Thedrug had 99% activity against E.coli, the most common urinarytract pathogen. Effect was seeneven in biofilms - particularlyimportant in complicated UTI.
Wagenlehner and colleagues(Germany) presented clinical stud-ies on linezolid, a substance in anew class of antibiotics that have aparticular effect against Gram-pos-itive pathogens. The drug hadfavourable effects on most mecilli-nam-resistant strains.
In pharmacodynamic studies thenew extended release formulationof ciprofloxacin was shown to haveexcellent bactericidal effect in bothonce daily and twice daily adminis-tration. Riffer et al (USA) achieved95% clinical success withciprofloxacin 500mg once daily forthree days in uncomplicated cysti-tis.
Graninger (Vienna) presentedstudy data supporting the use ofpivmecillinam as a first line empiri-cal treatment of acute cystitis.
Facing responsibilityEuropean urologists within ESIU
have invited microbiologists(ESCHMID) to join in a pan-European prevalence study, to reg-ister the incidence of NAUTI, thepathogens involved and their resis-tance pattern, as well as the use ofantibiotics in urology departmentsfor prophylaxis and treatment.
The study will provide an inter-national overview of NAUTI -important because pathogens donot respect geographical borders.Taking part will stimulate urologi-cal departments to monitorNAUTI, which has become animportant quality parameter forhospital care. The study will becombined with a quality improve-ment effort regarding protocols forthe use of urinary catheters andantimicrobial prophylaxis.
The study plan, publiclylaunched at the Budapest meeting,will be discussed in more detailduring the EAU-congress (Madrid,March 2003). Detailed informa-tion about the study will be foundat the ESIU/EAU website onUROWEB on the Internet.European Hospitals are stronglyrecommended to join this study.
LK: The advantages of this surgeryinclude shorter hospitalisation,less pain and quicker recupera-tion, as well as better cosmeticresults compared to open surgery.
However, the surgery is easy fora patient but hard for doctors. Asurgeon needs a lot of extra train-ing to become facile in laparo-scopic surgery, but results over-come disadvantages for the doc-tors, and we shouldn’t develop aprocedure just because it might be
easy. The main goal is to make iteasier and less painful for thepatient to recover.
At present, we also hope todevelop technology so that, usingan X-Ray image, we can place aneedle or probe into a tumour todestroy it completely by ‘cook-ing’ it. So far, so good. We arestill investigating that. CC: What are your hopes in termsof renal obstruction, kidneystones and testicular cancer? LK: We’re working with col-leagues to develop a vaccine totry to prevent kidney stones -using gene therapy. Certain peo-ple who have kidney stones dis-ease have family genes that wemay be able to change, to preventthem having stones.
Likewise, with testicular can-cer we’re developing laparoscopyfor patients who need moreextensive surgery, to avoid thebig incision, which usually runsfrom the chest all the way downto the pubic bone. Hopefully,with the laparoscopic approach,we can avoid that and people canget back to activity quicker.
Finally, with urinary obstruc-tion there are ways of suturingthings together. We have severaldifferent robotic devices that cansuture, to help us do less invasivesurgeries.
By Truls E Bjerklund Johansen MDPhD, co-chairman of the EuropeanSociety for Infections in Urology,and Professor of Urology at theTelemark Hospital, University ofTromso, Norway
much else
Professor Louis R. Kavoussi, expert in minimally invasiveapproaches to urological diseases, describes his pioneeringwork in laparascopic nephrectomy for cancer and live renaltransplant, and a prostate cancer procedure developed by Dr.Patrick C. Walsh, Chairman of the Brady Urological Institute.Prof. Kavoussi is Vice-Chairman of Urology, Professor of UrologySurgery and Chief of the Endourology Division at JohnsHopkins Medical Institutions Interview by Claudia Costabile
At the American College of Surgeon’s 86thClinical Congress in Chicago, Prof. Kavoussiused a remote controlled robot camera todirect surgeons operating on a patient 700miles away, at the John Hopkins BayviewMedical Centre, Baltimore

Professor Frans M J Debruyne, CourseDirector for the European School of Urology(ESU), says the European Urological WinterForum has built up a respected reputation ‘...due to excellent and distinguished international faculty teaching as well asthe enthusiasm and interaction of the delegates, who make educationalsessions lively, stimulating and relevant for every day urological practice’.
Short presentations will summarise the latest achievements in urology,followed by a programme covering most aspects of the field, with state ofthe art lectures alternating with interactive discussions,workshops, etc. (... and, this forum will take place inDavos, allowing many delegates to fit in some skiing -if time allows!) Contact: [email protected]
SWEDEN - The Unfors Mult-O-Meter 730-series - a new generation of non-invasive X-ray meters - havebeen designed to simplify themeasurement procedure.Unfors also reports thatoperation of these pocket-sized meters takes just tenseconds to learn. ‘Theinstrument has just two controlbuttons: on/off and parameter for scrolling themeasured values,’ the firm adds. ‘No set-uptime is needed. The specially designed LCDclearly indicates measured value and unit together.
‘The Unfors Mult-O-Meter 731L offers the most costeffective way for simultaneous measurements. Thismeter uses an external current clamp for non-invasivemeasurements of mA and mAs. The clamp can be usedwhen the mA is greater than 50 and the diameter of thehigh voltage cable is less than 23 mm. An externaldetector measures the kVp, dose, rate, time and pulses inthe range 50-150 kVp, with high accuracy. The meter iscalibrated to international traceable standards.
‘For reports, measurements can be transmitted via an
18 EUROPEAN HOSPITAL Vol 12 Issue 1/03
U R O L O G Y
Non-invasive X-ray meters
PT-141 gets resultsNEW YORK - Even though stillundergoing phase II a trials, a newsexual dysfunction drug termed PT-141 is showing positive results in agroup of patients who had previ-ously shown an inadequateresponse to Pfizer Inc’s Viagra.
After testing PT-141 as a treat-ment for erectile dysfunctionagainst a placebo, the drug wastested on 24 men, unable to sustainan erection more than 25% of thetime after taking at least a 100mgdose of Viagra. In the phase II a
PRAGUE, CZECH REPUBLIC -EUREP, the European UrologyResidents Education Programme,(29 August - 3 September) is ateaching programme developedexclusively for European urolog-ical residents. (Scientific Board:European School of UrologyBoard Members. Course direc-tors: C Chapple, R Nijman, WArtibani).
The aims are optimal prepara-tion of the final year resident forthe Fellow of the EuropeanBoard of Urology (FEBU) exami-nation.
The AquaFlate balloon catheter is hygienic and speeds upcatheterisation, says its manufacturer Ruesch GmbH. ‘Unlikeconventional catheters, this new product comes with asyringe that already contains the precise amount of sterilewater required. The syringe is packed in the same box as thecatheter, but protected by separate packaging. Consequentlyit remains sterile until ready for use, thus ensuring aseptictechnique for the care personnel. The reduction in preparato-ry work saves both time during catheterisation and money.’
Two self-adhesive pre-printed labels, on the back of thecatheter packaging, contain all relevant product information,and these can be fixed to the patient file as an update thatalso avoids errors, the firm adds.The product comes in two versions:● Brillant, latex-free, made of 100% silicone● SympaCath, made of natural latex and featuring hydrogel
coating.Both are available in standard or shorter lengths.Ruesch GmbH , PO Box 1180, 71385 Kernen, Germany.Phone: +49(0) 7151 406 0 Fax: +49(0) 7151 406 150E-mail: [email protected]. www.ruesch.de
Medullary cystic kidney disease type 2 starts in childhood and is a pro-gressive disease of both kidneys, eventually leading to renal failure anddeath. Familial juvenile hyperuricaemic nephropathy is caused by the kid-neys’ inability to process purines, found in many foods. This leads to abuild-up of uric acid, potentially causing gout, and eventually renal failure.
Definitive diagnosis of both conditions is often possible only afterextensive disease has occurred, but now new research findings may resultin a definitive diagnostic test. Dr Tom Hart et al, at the University ofPittsburgh, Pittsburgh, USA (pub: Journal of Medical Genetics (2002; 39:882-92), have found that the same gene mutation in a urinary proteincauses these two kidney diseases. DNA analysis and gene mapping stud-ies were carried out on four large families, spanning several generations.Three families had a history of familial juvenile hyperuricaemic nephropa-thy and one medullary cystic kidney disease. Four different gene muta-tions for the protein uromodulin were found across these families for bothdiseases.
High levels of this protein are normally excreted in urine, although theexact role of the protein remains a mystery, the researchers say it mightact as an antioxidant, and may help to preserve the impermeability of theLoop of Henle.
Although long suspected to have a role in these diseases, this is the firsttime that research has shown conclusive evidence that uromodulin is aprime suspect. Because these diseases are autosomal dominant (i.e. everyfamily member has a one in two chance of being affected), a definitivetest could be devised. Conclusive results before the development of symp-toms would mean early treatment and the prevention of the long termand potentially serious complications of both diseases, the researcherspoint out. It could also be particularly important for siblings wanting toact as kidney donors for brothers or sisters who already have symptoms.Details: www.bma.org.uk - Journal of Medical Genetics.
Topicalanaesthetic
clearedUSA - The FDA has clearedAkorn to market a lido-caine jelly bioequivalent toAstraZeneca’s XylocaineJelly. The product is a topi-cal anaesthetic used byurologists and hospitals.
E D U C A T I O N
infrared interface to Excel. Other models withdifferent parameters, including kVp, dose, dose rateand exposure time, are available within the UnforsMult-O-Meter family.
‘The meters are CE approved and UnforsInstruments is certified in accordance with ISO 9001and EN 46001.’Details: www.Unifors.com
Ruesch AquaFlateFor faster balloon catheterisation
trial, over 80% of the men, aged37-54, could achieve erections suf-ficient for sexual intercourse aftertaking the new drug.
PT-141 had a highly significanteffect on both the primary and sec-ondary efficacy endpoints relatingto the time of penile rigidity. Theaverage duration of erectile dys-function in the study group wasmore than eight years. The individ-ual scores in the InternationalIndex of Erectile Function (IIEF)domain score averaged about 11. A
Learning(and skiing)
The EUREPcourse Modules
● Renal Cancer- Bladder Cancer -Penile Cancer/Testis Cancer.
● Prostate Cancer- BPH/Prostatitis. ● Stones- Endourological techniques -
Infection in Urology ● Prolapse - Incontinence -
Pharmacotherapy/Painful BladderDisorders - Neurourology -Urodynamics
● Paediatric Urology- Trauma-Transplantation- Reconstruction -Andrology
Supported by an unrestricted educa-tional grant from Sanofi-Synthelabo,travel and accommodation costs will becovered for participants. Contact for ESU - Phone +31 263890680
A promising new erectile dysfunction drug may oust ViagraSpana. They are hoping to developthe agent to treat sexual dysfunc-tion in both men and women.
The first trial will begin midwaythrough this year in the US, while asecond will begin before the end of2003, possibly to include Europeanpatients.
Trial results surpassed all expec-tations, and were encouraging,since no clinically adverse eventswere noted and side effects weregenerally mild.
Raymond Rosen, principal inves-tigator and Professor of Psychiatryand Medicine at Robert Wood
Johnson Medical School, said PT-141 was ‘... an exciting new investi-gational drug with great potentialfor treatment of male erectile dys-function’.
Palatin’s research suggests thatPT-141 works through activation ofmelanocortin receptors in the CNS,rather than acting directly on thevascular system. Studies such asthese are increasing the understand-ing of the basic mechanisms thatcontrol sexual responses in bothmen and women.
In addition to oral treatment, anasal application is being developed.
New kidney teston the horizon
score below 11 is considered severe,with 11-16 being moderate andmore than 26 considered normal.
Palatin Technologies Inc, thecompany testing PT-141, plans toadvance the drug to two phase II btrials that will enrol about 300 menwith erectile dysfunction, accordingto the President and CEO, Dr Carl
The cause of two types of kidney diseaselies in a gene mutation in urinary protein

Disney-movie characters MickeyMouse, Pluto et al, decoratingNexcare bandages, have alreadydelighted children - and nowNexcare Disney Gel Warmbottleshave been launched. Made inwashable velvety material that has been allergy tested and is tearand bite proof. There’s no risk of burns due to leaks or easy-to-openplugs, the manufacturer reports. The non-toxic gel filling warms in90 seconds, at 650 watts, and keeps warm longer than conventionalhot-water bottles. Made by 3M, these are available at pharmacies (rrp: 9.95 euros).
EUROPEAN HOSPITAL Vol 12 Issue 1/03 19
C O M P A N Y , N E W S , A W A R D S & I N N O V A T I O N S
DELFT, THE NETHERLANDS - CardioControl NV and Welch Allyn Inc, ofSkaneateles Falls, NY, have announcedthat the US firm has made a cash offerfor all outstanding shares (at six euroseach) of Cardio Control’s stock. Basedon the number of outstanding sharesand options on shares, the expectedoffer could be over 18 million euros.Cardio Control predicts 2002 revenuesto be just over 10 million euros.
Welch Allyn (founded 1915) employs2,300 people and manufactures med-ical diagnostic equipment, patientmonitoring systems and miniatureprecision lamps. It has also successful-ly expanded into new product areas,e.g. diagnostic cardiology.The transac-tion, the firm says, will further its
SWITZERLAND - The pharmaceuti-cal firm Roche has made a publictender offer for the medical devicesupplier Disetronic, an acquisitionamounting to 1.09 billion euros.
With sales of 121.4 million euros inthe first nine months of the2002/2003 accounting period,Disetronic is Europe’s leading andthe USA’s second manufacturer ofinsulin pumps. Its infusion systemswill become part of RocheDiagnostic’s Diabetes Care unit.Roche will not acquire the firm’sinjection systems division. This willbe bought by Willy Michel,Disetronic’s founder, chairman andmajor shareholder, who will form anindependent company.
This deal could make RocheDiagnostics one of the mainproviders of integrated diabetesmanagement and, Roche points out,the worldwide diabetes market isworth 477.5 million euros, holdingan 11% annual growth rate.
100 millioninfusion devicesGERMANY - A decade after opening afacility at Pfieffewiesen, B. BraunMelsungen AG has reported an annu-al manufacturing output of infusiondevices (Intrafix and Eurofix) topping100 million. In 1992 the output was55.2 million infusion/transfusiondevices per annum.‘We are manufac-turing almost twice the quantity onthe same floor space,’ said Hans-Dieter Froehlich, production managerat Pfieffewiesen, possible due to ‘continuous technological develop-ment and ... well-trained employeesworking in teams’.
The firm adds that it will soon topthe billion mark in its Melsungenfactory.
Over 70% of German patientshave considerable confidence indoctor’s equipment used for pro-phylactic medical examinations,according to a poll presented atMEDICA 2002 by CortexBiophysik GmbH of Leipzig,Germany.
The majority of those polledsaid top priorities for medicalequipment/instruments are qualityand precision. Nonetheless, themajority of medical professionalspolled said they would replaceequipment (particularly for car-
Gaining the Japanese G-markJAPAN - The Electromedical Systems Division of SiemensMedical Solutions has been awarded a G-Mark for Servo-I,an advanced ventilator platform suitable for use forpatients from neonates, through infants to adults, featuresadvanced treatment options.
The G-Mark award, based on the ‘Good DesignSelection System’ established by the Ministry ofInternational Trade and Industry in 1957, is conferred bythe country’s Good Design Award organisation. In Japan,the logo signals high quality, practicality, pleasingergonomics - and good value for money, Siemens says.
AUSTRIA - David Byrne, EUCommissioner for Health andConsumer Protection, has receivedthe Goethe Challenge Trophy for aSmoke Free Environment for hisinitiation of the pan-Europeaninformation campaign entitled ‘Feelfree to say no!’ Aimed at preventingadolescents from taking upsmoking, this was the first campaignaimed at convincing youngsters thatit’s ‘cooler’ to resist temptation,despite advertisements to thecontrary.
Accepting the award from
3-year warrantyextension forvaporiserUK - Penlon Limited, the 50-year-old anaesthesia systems firm, hasextended the 12-month warrantyon its Delta Vaporiser to three years- at no cost to its customers.
Delta has proved ultra-reliableand successful since its 2000 intro-duction. (In 2002, Penlon receiveda Queen’s Award for Enterprise -
Innovation Category- for this prod-uct). Delta sales, in over 100 coun-tries, have reached almost £14 mil-lion (including over £4 million inthe USA).
Craig Thompson, Penlon’s Mar-keting Manager, said, ‘The warran-ty extension adds to Delta’s impres-sive list of features - outstandingperformance over the widest rangeof vapour concentration and tem-peratures, particularly at low flows,low body-weight, ease of use and amaintenance-free system’.
I N N O V A T I O N S
Prof. Fritz Kempner and EU CommissionerDavid Byrne with Prof. Portheine, founder ofthe Goethe Endowment for Non-smoking
Byrne wins Goethe’s smoke-free bust
for Non-smoking has annuallypresented the 20kg, silver bust ofGoethe (value 50,000 euros), since1992 - to institutions, universities orindividuals who have contributed tothis aim.
Cash offer for PC-based ECG firminterest in advancing worldwidecardio pulmonary and informationmanagement sales. If the dealmaterialises, the company will ownat least 95% of the issued share cap-ital of Cardio Control.
Dick G van Luijk, MD of CardioControl, pointed out that, as part ofWelch Allyn, the firm also expects toaccelerate growth in sales of itsdiagnostic systems for heart andlung functions. In recent years thecompany also launched softwarethat records and analyses combinedmedical and patient data for bothcentralised and remote use (withbuilt-in features for telemedicineand connectivity with electronicmedical record software).
Disetronic tosplit in Roche
deal
Progress must match patients’ confidence
Professor Fritz Kempner, at the 5thEuropean Health Forum Gastein,David Byrne pointed out that overhalf a million Europeans dieannually due to direct and indirectsmoking. Dedicating the trophy tohis anti-smoking colleagues, headded that he sees the award asencouragement for a Europeanhealth policy aimed at stoppingsmoking.
The author Johann Wolfgangvon Goethe campaigned for asmoke-free environment 200 yearsago, and the Goethe Endowment
GERMANY - In recognition of his work in devel-opmental biology, Professor Christof Niehrs,
head of the Department of Molecular Embryology at the GermanCancer Research Centre, has been presented with the 2003 GottfriedWilhelm Leibniz Prize by the German Research Council (DFG).
Worth about 1.55 euros, the award is the highest for research inGermany, and is used to support research over a five-year period, withspending according to the scientist’s requirements. So far there havebeen eleven recipients.
diac and circulatory treatments)only after five to ten years - gener-ally because of the nation’s weakeconomy plus healthcare changes.
In view of these findings, DrMatthias Gehrke, CEO of CortexBiophysik pointed out thatpatients’ confidence in sophisticat-ed technology must be maintainedand that research, developmentand use of the best equipment,especially for ergospirometry -focusing on the heart, circulation,breathing or metabolism - is ofprime importance.
Embryology
Everyone wants one!

25-27 Istanbul, TurkeyExpomed -International Fair of Medical Technology andHospital Equipment
25-27 Nuremberg, GermanyAltenpflege + HealthCare 2003www.altenpflege-healthcare.de
28-2 April Istanbul, TurkeyEuropean Association for the Studyof the Liver. www.easl.ch
30-2 April Chicago, Illinois, USAACC 52nd Annual Scientific Session ofthe American College of Cardiology.www.acc.org
30-2 April Miami, USA 15th National HIV/AIDS UpdateConferencewww.amfar.org
APRIL
1-4 Munich, Germany1st International Trade Fair andBioAnalytica Conferencewww.bioanalytica.de
2-5 The Hague, NetherlandsEAPC - 8th Congress of EuropeanAssociation for Palliative Carewww.eapcnet.org
2-5 Verona, Italy37th Annual Meeting of the EuropeanSociety for Clinical InvestigationThe Pathophysiology Of Diseases: FromBench To Bedside. A vast array of subjects,from molecular pathophysiology toemergency med. & critical care. Contact:Giovanni Ricevuti, MD, Dept. InternalMedicine & Therapeutics, University ofPavia. [email protected] Details:www.genomica.net/ESCI/ESCI.htm
2-5 Hague, The Netherlands8th Congress of the EuropeanAssociation for Palliative Care www.eapcnet.org/theHague2003
L I N K U P
Highlight your congress,conference or trade fair hereSimply contact us for detailsOur readers are leading hospitaladministrators, medicalprofessionals and medicalmanufacturers throughoutEurope. GLOBAL EVENTS is aspecial courtesy section, publishedto help our readers keep abreastof future conferences and muchelse. We present many event detailsfree of charge. However, we canalso offer greater space, for asmall fee, so that your event willbe highlighted - and even morecertain to be seen and read.Contact: Daniela Zimmermann,EUROPEAN HOSPITALPhone +49 211 7357 531Fax +49 211 7357 530 E-mail: [email protected], contact your localAdvertising Representative - seeour masthead (above)
Reach youraudience!
2003
MARCH
6-10 Birmingham, UK17th Annual Congress of theEuropean Association of UrologyBirmingham, UK,
7-11 Vienna, AustriaECR 2003www.ecr.org
11-13 Tel Aviv, Israel National Biotechnology Week
12-15 Monte Carlo, France Heart & Brain - 6th InternationalConference on Stroke & 3rdConference of the MediterraneanStroke Society
12-15 St. Gallen, SwitzerlandPrimary Therapy of Early BreastCancer 2003www.oncoconferences.ch
12-15 Madrid, SpainEAU-Congress of the EuropeanAssociation of Urology
18-21, Brussels, Belgium ICEM 23rd International Symposiumon Intensive Care and EmergencyMedicinewww.intensive.org
19-21 Cairo, Egypt1st PanArab ‘IT in medicine’ congress& fairOrganised by the Egyptian Society of HealthAwareness IT & telemedicine section.www.arabitmed.com
19 - 22, Posen, Poland SALMED 2003www.mtp.com.pl
19-22 Barcelona, Spain 4th International GlaucomaSymposium
20-23 Istanbul, TurkeyExpomed 2003, Lab-tech 2003 andIstanbul Hospital SuppliesEquipment Fair Venue: Tuyap Fair,Convention & Congress Centre, Beylikduzu.Details: www.tuyap.com
24 - 26 Zurich, Swizerland2nd Global Medical Forum
5 - 9 Toronto, Canada94th AACR Annual Meeting 2003www.aacr.org
6-10 Brussels, Belgium 13th International Meeting of theEuropean Society of GynaecologicalOncology - ESGOwww.esgo.org/esgo13
9-11 LuxembourgTelemedicine & Telecare InternationalTrade Fairwww.telemedicine.lu
9-13 Munich, GermanyGerman Congress of Anaesthesiawww.mcn-nuernberg.de
9-13 Sicily21st Annual Meeting of the EuropeanSociety for Paediatric InfectiousDiseases (ESPID)
24-25 Brussels, BelgiumIntensive Care - internationalconsensus conferencewww.escim.org
24-26 Mannheim, Germany69th Annual Meeting of GermanCardiac Societywww.dgkardio.de
24-27 Berlin 4th World Congress on Controversiesin Obstetrics, Gynaecology &Infertility
26-30 Florence, ItalyICNC - 6th International Conferenceof Nuclear Cardiology
26-30 Lyon, France6th European Congress ofEndocrinologywww.endocrinology2003.com
29-5 May Munich, GermanyGerman Congress of Surgerywww.dgch.de
Published by: EUROPEAN HOSPITAL GmbHHöherweg 287, 40231 DüsseldorfPhone: +49 (0)211-7357-532Fax: +49 (0)211-7357-530e-mail: [email protected]
Editor-in-Chief Brenda Marsh
Art Director Mary Pargeter
Executive Directors Daniela Zimmermann,Reiner Hoffmann
Editorial Assistant Denise Hennig
Sales Assistant Jennifer Plum
Founded by Heinz-Jürgen Witzke
CorrespondentsAustria: Christian Pruszinsky. Belgium: HannesFrank. Czech Republic: Rostislav Kuklik. Finland:Marti Kekomaki. France: Jaques Lalbat. Germany:Anja Behringer, Heidi Heinold, Max Heymann,Stephen Schnaittacher, Prof Tinneberg. GreatBritain: Brenda Marsh. Italy: G. Sinaccio. Poland:Pjotr Szoblik. Spain: Eduardo de la Sota. Sweden:Ake Spross. Switzerland: Jaqueline Merlotti. USA:Ivan Oransky, Craig Webb.
UK editorial address55 Wey Meadows,WeybridgeSurrey KT13 8XY
SubscriptionsDenise Hennig, European Hospital,Höherweg 287, 40231 Düsseldorf, Germany
Subscription rate12 issues: 60 EuroSingle copy: 4,60 EuroSend order and cheque to:European Hospital Subscription Dept
Finishing AMK, Bonn, Germany
Printed by Frotscher Druck,Darmstadt, Germany
Publication frequency bi-monthly
European Hospital ISSN 0942-9085
Advertising:Simon Kramer, Germany, +49-211-9 94 58 81Denise Hennig, Germany, +49-211-7 35 75 32Juri Laskin, Russia, +70-95-2 71 10 06Hanna G. Ibrahim, France, +33-1-43 37 07 00C.K. Kwok, Hong Kong, +85-2 28 90 55 10Ted Asoshina, Japan, +81-3-32 63 50 65C.H. Park, South Korea, +82-2-3 64 41 82Hanna Politis, USA, +1-3 01-8 69 66 10
GermanyHead Office DüsseldorfEuropean Hospital, Höherweg 287,40231 Düsseldorf, Federal Republic of GermanyTel: +49 211 7357 531. Fax: +49 221 7357 530e-mail: [email protected]
GB, Scandinavia and BeNeLuxSimon Kramer, Willem Alexander Plantsoen 25,2991 NA BarendrechtTel: +31-180-617226. Fax: [email protected]
FranceSisco, Communication et DéveloppementInternational, Hanna G. Ibrahim,33 rue Croulebarbe, F-75013 ParisTel: +33-1-43370700. Fax +33-1-43315363
Hong Kong, ChinaEastern Source Int. Media Centre, C K Kwok,25/F Great Smart Tower, 230 Wanchai Road,Wanchai, Hong KongTel: +8522 8 90 55 10. Fax: + 8522 8 95 14 43
JapanEcho Japan Corporation, Tetsuzo Asoshina,Grande Maison Room 3032-2 Kudan Kita, 1 Chome Chiyoda-KuTokyo 102, JapanTel: + 81 3 32 63 50 65. Fax: +81 3 32 24 20 64
South KoreaFar East Marketing Inc, C H Park,Room 1806/7, Golden Tower Building, 191, 2-kaChoongjung-ro, Sedoaemun-ku, Seoul, KoreaTel: +82 2 364 41 82/3. Fax: +82 2 364 41 84
USA & CanadaMedia International, Hanna Politis, 8508 PlumCreek Drive, Gaitherburg, MD 20882, USATel: +1 301 869 66 10. Fax: +1 301 869 66 11
One more time:‘Is alcohol medicinal?’
Although studies of the benefits of moderate alcohol consumptionabound, most are epidemiological and findings often conflict.Stefan Pruszinsky reports from Austria on a current, comparativestudy, described at the 5th European Health Forum in Gastein‘Dr Reinhard Resch, of the Institutefor Physical Medicine andRehabilitation, Landeskrankenhaus,Krems, Austria, described his cur-rent prospective, randomised, open,comparative study, aimed at discov-ering if wine really does have health-promoting properties.
He takes ‘drink’ to mean a mod-erate, measured consumption ofwine (about 20mg daily) withoutdependency. The study concentrateson white wine, because the positivebenefits of moderate consumptionof the red - said to include a goodeffect on cardio-vascular function -have been sufficiently shown inlarge-scale studies of recent years, hepoints out. These benefits mayprove no greater than those of whitewine.
Dr Resch is testing two equallysized, mixed-sex groups of volun-teers of various ages, all of whomreceived advice on diet and exercise.Members of the control group con-sume no alcohol. The others con-sume white wine over a period oftwelve weeks, based on the above
Med. diet checks arthritis SWEDEN - AMediterraneandiet signifi-cantly lessensr h e u m a t o i d
arthritis symptoms, according to asmall study by Dr Lars Skoldstamet al, of the Department ofMedicine, Visby Hospital, (pub:Annals of Rheumatic Diseases2003; 62: 208-14).
26 people with stable rheumatoidarthritis were assigned to an exper-imental Mediterranean/Cretan, dietfor three months. The remainderstayed on their usual diet. Bothgroups were similar in weight andsmoking habits.
Olive and canola oils were usedas a primary source of fat in theMed. diet, which was high in fish,poultry, fruit, vegetables, and
Fruit combats cancerUK - High fruit consumption during childhood mayreduce the risk of developing cancer as an adult, andincreasing fruit intake may be associated with lowerdeath rates from all causes, according to results from along term study of almost 4,000 people, published inthe Journal of Epidemiology and Community Health(Fruit, vegetables, and antioxidants in childhood andrisk of adult cancer: the Boyd Orr cohort 2003; 57: 218-25)
The study found little evidence that vitamins C, E, andbeta carotene were responsible for the apparently pro-tective effects of fruit.
MAY7-10 Karlsruhe, GermanyREHAB 2003
1-4 Buenos Aires, ArgentinaCongress of the InternationalSociety for Non-invasiveElectrocardiologyThe XII Congress of Cardiology for theConsultant and Inter-American Forum onCV Prevention
8-9 New York, USAValves in the Heart of the Big AppleIII: Evaluation & Management ofValvular Heart Diseases 2003
10-16 Toronto, CanadaISMRM11th Scientific Meeting and Exhibition ofthe International Society for MagneticResonance in Medicine
18-22 Prague, Czech Republic2nd World Congress of theInternational Society of PhysicalRehabilitation Medicine- ISPRM
25-28 Prague, Czech RepublicEACTA 2003, European Association.of Cardiothoracic Anaesthesiologists www.eacta.org
JUNE
1-4 Montreal, Canada10th congress of the WorldFederation for Ultrasound inMedicine and Biologywww.aium.org
2-5 Verona, Italy37th Annual Meeting of theEuropean Society for ClinicalInvestigation
3 - 6 Genoa, ItalyESPR- Annual Meeting of theEuropean Society of PaediatricRadiology
11-14 Helsinki, FinlandXXX International Congress onElectrocardiology
15-17 Lapland, FinlandMidnight Sun Symposium onElectrocardiology
N U T R I T I O N
guidelines. The exact amountdepends on the alcohol content ofthe wine. Wines chosen for the studyinclude Gruener Veltliner, WhiteBurgundy, Riesling andWelschriesling. Clinical data such asliver function, blood sugar andblood fat content are being mea-sured in both groups, along with‘soft’ factors such as subjective well-being and general quality of life.
We will report on Dr Resch’s find-ings - due for publication early thisyear.’
legumes, and low in red meat andhigh fat dairy produce.
During the three-month trial, forthe first three weeks the patientsreceived lunch and dinner at thehospital, where they were taughtabout Mediterranean food andcooking.
Disease activity, reflected in jointtenderness and swelling, physicalfunction, quality of life, and use ofanti-inflammatory drugs were clini-cally assessed at the beginning ofthe study, and at three, six andweek intervals. Secondary measuresincluded biochemical indicators,pain severity, and a standard griptest.
The patients on the Med-iterranean diet lost 3 kg in weight,and cholesterol levels fell after threeweeks. Otherwise there was littledifference until six weeks later,when the index of inflammatoryactivity began to fall in the Med.diet candidates.
After 12 weeks, both physicalfunction and vitality had alsoimproved, and in total, nine out ofthe 14 variables had also improved.There was no evidence of anychanges in the group followingtheir normal diet.
The authors caution that a larger,longer study would be neededbefore definitive conclusions can bedrawn.