Embed Size (px)
Citation preview

226
Published OnlineFirst December 22, 2009; DOI: 10.1158/1078-0432.CCR-09-1405
Imaging, Diagnosis, Prognosis Clinical
CancerResearch
Activation of WD Repeat and High-Mobility Group Box DNABinding Protein 1 in Pulmonary andEsophageal CarcinogenesisNagato Sato1,2, Junkichi Koinuma1, Masahiro Fujita3, Masao Hosokawa3, Tomoo Ito4, Eiju Tsuchiya5,Satoshi Kondo2, Yusuke Nakamura1, and Yataro Daigo1,6
Abstract
Authors' ACenter, Inst2Departmenof MedicinPathology,Center ReMedical On
Note: SuppResearch O
Corresponsity of Tokyo81-3-5449-5
doi: 10.115
© 2010 Am
Clin Canc
Dow
Purpose: We attempted to identify novel biomarkers and therapeutic targets for lung and esophagealcancers.Experimental Design:We screened for genes that were overexpressed in a large proportion of lung and
esophageal carcinomas using a cDNA microarray representing 27,648 genes or expressed sequence tags. Agene encoding WDHD1, a WD repeat and high-mobility group box DNA binding protein 1, was selectedas a candidate. Tumor tissue microarray containing 267 archival non–small cell lung cancers and 283esophageal squamous cell carcinomas (ESCC) was used to investigate the clinicopathologic significanceof WDHD1 expression. The role of WDHD1 in cancer cell growth and/or survival was examined by smallinterfering RNA experiments and cell growth assays. The mechanism of WDHD1 activation through itsphosphorylation in cancer cells was examined by immunoprecipitation and kinase assays.Results: Positive WDHD1 immunostaining was associated with a poor prognosis for patients with
non–small cell lung cancer (P = 0.0403) as well as ESCC (P = 0.0426). Multivariate analysis indicatedit to be an independent prognostic factor for ESCC (P = 0.0104). Suppression ofWDHD1 expression withsmall interfering RNAs effectively suppressed lung and esophageal cancer cell growth. In addition, induc-tion of the exogenous expression of WDHD1 promoted the growth of mammalian cells. AKT1 kinaseseemed to phosphorylate and stabilize the WDHD1 protein in cancer cells.Conclusions: WDHD1 expression is likely to play an important role in lung and esophageal carcino-
genesis as a cell cycle regulator and a downstream molecule in the phosphoinositide 3-kinase/AKTpathway, and that WDHD1 is a candidate biomarker and a promising therapeutic target for cancer. ClinCancer Res; 16(1); 226–39. ©2010 AACR.
Aerodigestive tract cancer (including carcinomas of lung,esophagus, oral cavity, pharynx, and larynx) accounts forone third of all cancer deaths in the United States and isthe most common cancer in some parts of the world (1).Lung and esophageal cancers are the two major thoraciccancers that share common clinicopathologic characteris-tics: (a) embryologically, both of them are derived fromendoblast; (b) epidemiologically, there is a risk factor suchas smoking; and (c) pathologically, a certain proportion of
ffiliations: 1Laboratory of MolecularMedicine, HumanGenomeitute ofMedical Science, TheUniversity of Tokyo, Tokyo, Japan;t of Surgical Oncology, Hokkaido University Graduate Schoole; 3Keiyukai Sapporo Hospital; and 4Department of SurgicalHokkaido University, Sapporo, Japan; 5Kanagawa Cancersearch Institute, Yokohama, Japan; and 6Department ofcology, Shiga University of Medical Science, Otsu, Japan
lementary data for this article are available at Clinical Cancernline (http://clincancerres.aacrjournals.org/).
ding Author: YataroDaigo, InstituteofMedicalScience,TheUniver-, 4-6-1 Shirokanedai, Minato-ku, Tokyo, 108-8639 Japan. Phone:457; Fax: 81-3-5449-5406; E-mail: [email protected].
8/1078-0432.CCR-09-1405
erican Association for Cancer Research.
er Res; 16(1) January 1, 2010
Researcon Januaclincancerres.aacrjournals.org nloaded from
them consists of the squamous cell carcinoma. In spite ofthe use of modern surgical techniques combined with var-ious treatment modalities, such as radiotherapy and che-motherapy, lung cancer and esophageal squamous cellcarcinoma (ESCC) are known to have the worst prognosisof all malignant tumors; 5-year survival rates for lung can-cer patients including all disease stages still remain as lowas 15% and those for ESCC patients are much the same at16% (2, 3). A better understanding of the molecular basisof cancer has led to novel targeted strategies that inhibitspecific key molecules in tumor growth, however currentlyavailable new targeted therapies are expected to improvethe prognosis of a small number of patients (4, 5). There-fore, novel strategies such as the development of molecu-lar-targeted agents and cancer vaccines, which targetmolecules essential for the growth/survival of cancer cells,are eagerly awaited.We have been attempting to isolate potential molecu-
lar targets for diagnosis and/or treatment of lung cancerand ESCC by analyzing genome-wide expression profilesof 101 lung cancer and 19 ESCC tissue samples on acDNA microarray containing 27,648 genes or expressedsequence tags (6–12). To verify the biological and clinical
h. ry 8, 2021. © 2010 American Association for Cancer

Translational Relevance
Because there is a correlation between WDHD1 ex-pression and poor prognosis for patients with lung andesophageal carcinomas, and multivariate analysis indi-cated it to be an independent prognostic factor foresophageal carcinomas, WDHD1 positivity in resectedspecimens could be an index that provides informa-tion useful to physicians in applying adjuvant therapyand intensive follow-up to the cancer patients who arelikely to suffer a relapse. Because WDHD1 shouldproperly be classified as a typical cancer testis antigenand is likely to play an important role as a key compo-nent of the phosphoinositide 3-kinase/AKT pathway incancer proliferation, the selective inhibition ofWDHD1 expression and/or the targeting of enzymaticinteraction between AKT1 and WDHD1 by small mol-ecule compounds could be a promising therapeuticstrategy that is expected to have a powerful biologicaleffect on cancer with a minimal risk of adverse events.
WDHD1 in Pulmonary and Esophageal Carcinogenesis
Published OnlineFirst December 22, 2009; DOI: 10.1158/1078-0432.CCR-09-1405
significance of the gene products, we have established ascreening system by combining the tumor tissue microar-ray analysis of clinical lung and ESCC with RNA interfer-ence technique and cell growth assays (13–37). In thecourse of these systematic studies, we found that WD re-peat and high-mobility group box DNA binding protein1 (WDHD1; alias acidic nucleoplasmic DNA-binding pro-tein, AND-1) was overexpressed in the great majority oflung cancers and ESCCs.WDHD1 is a human homologue of Ctf4 in Saccharomyces
cerevesiae, which was originally identified by screening formutant genes affecting chromosome transmission fidelity(38). Later studies indicate that Ctf4 is required for sisterchromatid cohesion and interacts with DNA polymeraseα in yeasts (39). Mcl1, a homologue of CTF4 in Schizosac-charomyces pombe, is essential for the viability, maintenanceof genome integrity, and regulation of telomere replicationin fission yeast (40). Mcl1/Ctf4 is functionally related withmolecules involved in lagging strandDNA synthesis such asRad2, Dna2, and Fen1 that plays a role in processing Oka-zaki fragments and physically interacts with DNA polymer-ase α to promote the chromatin association of DNApolymerase α (40), but its exact role in DNA replicationhas not yet been defined. Recently, it has been shown thatWDHD1 could interact with Mcm10 and is required for theproper loading of DNA polymerase α and replication initi-ation in osteosarcoma U2OS cells (41). However, no reporthas yet clarified the significance of WDHD1 transactivationin clinical cancer progression.We report here the identification of WDHD1 as a pre-
dictive cancer biomarker in the clinic and as a potentialtherapeutic target, and also provide evidence for its in-volvement as a downstream target of phosphoinositide3-kinase (PI3K)/AKT pathway in human pulmonary andesophageal carcinogenesis.
www.aacrjournals.org
Researcon Januaclincancerres.aacrjournals.org Downloaded from
Materials and Methods
Cell lines and tissue samples. The human lung cancer celllines used in this study were as follows: lung adenocarcino-mas (ADC) NCI-H1781, NCI-H1373, LC319, A549, andPC14; lung squamous cell carcinomas (SCC) SK-MES-1,NCI-H2170, NCI-H520, NCI-H1703, and LU61; a lunglarge-cell carcinoma LX1; and small-cell lung cancers(SCLC) SBC-3, SBC-5, DMS273, and DMS114 (Supple-mentary Table S1). The human esophageal carcinoma celllines used in this study were as follows: 10 SCC cell lines(TE1, TE2, TE3, TE4, TE5, TE6, TE8, TE9, TE10, and TE11)and one ADC cell line (TE7; ref. 42). All cells were grown inmonolayer in appropriate medium supplemented with10% FCS and maintained at 37°C in humidified air with5% CO2. Human small airway epithelial cells (SAEC) usedas a normal control were grown in optimized medium(small airway growth medium) from Cambrex Bioscience,Inc. Primary non-SCLC (NSCLC) and ESCC tissue samplesas well as their corresponding normal tissues adjacent to re-section margins from patients having no anticancer treat-ment before tumor resection had been obtained earlierwith informed consent (7, 11, 12, 15). All tumors werestaged on the basis of the pathologic tumor-node-metasta-sis classification of the International Union Against Cancer(43). Formalin-fixed primary lung tumors and adjacentnormal lung tissue samples used for immunostaining ontissuemicroarrays had been obtained from267 patients un-dergoing curative surgery at Hokkaido University and its af-f i l i a t ed hosp i t a l s (Sapporo , J apan ; p l ea se seeSupplementary Table S2A). A total of 283 formalin-fixedprimary ESCCs and adjacent normal esophageal tissue sam-ples near to resection margins had also been obtained frompatients undergoing curative surgery at Hokkaido Universi-ty Hospital and Keiyukai Sapporo Hospital (Sapporo, Ja-pan; Supplementary Table S2B). To be eligible for thisstudy, tumor samples were selected from patients who ful-filled all of the following criteria: (a) patients suffered pri-mary NSCLC or ESCC with histologically confirmed stage(only pT1 to pT3, pN0 to pN2, and pM0); (b) patients under-went curative surgery, but did not receive any preoperativetreatment; (c) among them, NSCLC patients with positivelymph node metastasis (pN1, pN2) were treated with plati-num-based adjuvant chemotherapies after surgery, andESCC patients with pN positive were treated with adjuvantchemotherapy using both platinum and 5-fluorouracil aftersurgery, whereas patients with pN0 did not receive adjuvantchemotherapies; and (d) patients whose clinical follow-updatawere available. This study and the use of all clinicalma-terials mentioned were approved by individual institution-al ethics committees.Semiquantitative reverse transcription-PCR. A total of 3
μg aliquot of mRNA from each sample was reversely tran-scribed to single-stranded cDNAs using random primer(Roche Diagnostics) and SuperScript II (Invitrogen). Semi-quantitative reverse transcription-PCR (RT-PCR) experi-ments were carried out with the following sets ofsynthesized primers specific to WDHD1 or with β-actin
Clin Cancer Res; 16(1) January 1, 2010 227
h. ry 8, 2021. © 2010 American Association for Cancer

6 http://rsb.info.nih.gov/ij/index.html
Sato et al.
228
Published OnlineFirst December 22, 2009; DOI: 10.1158/1078-0432.CCR-09-1405
(ACTB)–specific primers as an internal control: WDHD1,5′-AGTGAAGGAACTGAAGCAAAGAAG-3′ and 5′-ATC-CATTACTTCCCTAGGGTCAC-3′; ACTB, 5′-GAGGTGATA‐GCATTGCTTTCG-3′ and 5′-CAAGTCAGTGTACAGG-TAAGC-3′. PCRs were optimized for the number of cyclesto ensure product intensity to be within the linear phase ofamplification.Northern blot analysis. Human multiple tissue blots cov-
ering 23 tissues (BD Bioscience) were hybridized with an[α-32P]-dCTP–labeled, 535-bp PCR product of WDHD1that was prepared as a probe using primers 5′-CTCTGATTC-CAAAGCCGAAG-3′ and 5′-ATCCATTACTTCCCTAGGGT-CAC-3′. Prehybridization, hybridization, and washingwere done following the manufacturer's specifications.The blots were autoradiographed with intensifying screensat −80°C for 7 d.Western blotting. Cells were lysed in lysis buffer [50
mmol/L Tris-HCl (pH 8.0), 150 mmol/L NaCl, 0.5%NP40, 0.5% sodium deoxycholate, and Protease InhibitorCocktail Set III (EMD Biosciences, Inc.)]. We used an en-hanced chemiluminescence (Amersham) Western blottinganalysis system (GE Healthcare Bio-sciences), as previous-ly described (15). A commercially available rabbit poly-clonal antibody to human WDHD1 was purchased fromATLAS Antibodies AB and was proved to be specific to hu-man WDHD1 by Western blot analysis using lysates oflung and esophageal cancer cell lines.Immunocytochemical analysis. Immunocytochemical
analyses were done as previously described (30), using0.5 μg/mL of a rabbit polyclonal anti-WDHD1 antibody(ATLAS Antibodies AB) for detecting endogenous WDHD1as a primary antibody and an Alexa 488–conjugated don-key anti-rabbit secondary antibody (Molecular Probe).Each stained specimen was mounted with Vectashield(Vector Laboratories, Inc.) containing 4′,6-diamidino-2-phenylindole and visualized with Spectral Confocal Scan-ning Systems (TSC SP2 AOBS; Leica Microsystems).Immunohistochemistry and tissue microarray. To investi-
gate the WDHD1 protein in clinical samples that had beenembedded in paraffin blocks, we stained the sections usingENVISION+ kit/horseradish peroxidase (DakoCytoma-tion) in the following manner. Briefly, slides were im-mersed in Target Retrieval Solution and boiled at 108°Cfor 15 min in an autoclave for antigen retrieval. Rabbitpolyclonal anti-WDHD1 antibodies (1.6 μg/mL; ATLASAntibodies AB) were added to each slide after blockingof endogenous peroxidase and proteins, and the sectionswere incubated with horseradish peroxidase–labeled anti-rabbit IgG as the secondary antibody. Substrate-chromo-gen was added, and the specimens were counterstainedwith hematoxylin.Tumor tissue microarrays were constructed with forma-
lin-fixed 267 primary lung cancers and 283 primaryesophageal cancers as described elsewhere (44–46). Thetissue area for sampling was selected based on visual align-ment with the corresponding H&E-stained section on aslide. Three, four, or five tissue cores (diameter, 0.6 mm;depth, 3-4 mm) taken from a donor tumor block were
Clin Cancer Res; 16(1) January 1, 2010
Researcon Januaclincancerres.aacrjournals.org Downloaded from
placed into a recipient paraffin block with a tissue micro-arrayer (Beecher Instruments). A core of normal tissue waspunched from each case, and 5-μm sections of the result-ing microarray block were used for immunohistochemicalanalysis. Three independent investigators semiquantita-tively assessed WDHD1 positivity without prior knowl-edge of clinicopathologic data. Because the intensity ofstaining within each tumor tissue core was mostly homog-enous, the positivity of WDHD1 staining was recorded byfollowing criteria: negative (no appreciable staining in tu-mor cells) and positive (brown staining appreciable in thenucleus and cytoplasm of tumor cells). Cases were accept-ed as positive only if all reviewers independently definedthem as such.Statistical analysis. Statistical analyses were done using
the StatView statistical program (SaS). Survival curves werecalculated from the date of surgery to the time of deathrelated to NSCLC or ESCC, or to the last follow-up obser-vation. Kaplan-Meier curves were calculated for each rele-vant variable and for WDHD1 expression; differences insurvival times among patient subgroups were analyzed us-ing the log-rank test. Univariate and multivariate analyseswere done with the Cox proportional hazard regressionmodel to determine associations between clinicopatholog-ic variables and cancer-related mortality. First, we analyzedassociations between death and possible prognostic fac-tors including age, gender, pT classification, and pN clas-sification, taking into consideration one factor at a time.Second, multivariate Cox analysis was applied on back-ward (stepwise) procedures that always forced strongWDHD1 expression into the model, along with any andall variables that satisfied an entry level of a P value of<0.05. As the model continued to add factors, indepen-dent factors did not exceed an exit level of P < 0.05.Two-tailed P value of <0.05 were considered statisticallysignificant.Cell growth assay. COS-7 cells were plated at densities of
1 × 106 cells/100-mm dish, transfected with plasmids de-signed to express WDHD1 or mock plasmids. Cells wereselected in medium containing 0.4 mg/mL of geneticin(Invitrogen) for 7 d, and cell viability was assessed byMTT assay (cell counting kit-8 solution; Dojindo Labora-tories). The number of colonies stained with Giemsa wasalso counted by colony formation assay using colonycounting software (ImageJ software 1.42, NIH).6
RNA interference assay. Small interfering RNA (siRNA)duplexes (Dharmacon, Inc.; 100 nmol/L) were transfectedinto a NSCLC cell line A549 and an esophageal cancer cellline TE9, using 30 μL of Lipofectamine 2000 (Invitrogen)as described (33). The transfected cells were cultured for7 d and cell growth was evaluated by MTT and colonyformation assays. siRNA duplexes against human WDHD1and AKT1 used were as follows: si-WDHD1-#1, siGenomeduplexes 1 [D-019780-01], 5′-GAUCAGACAUGUG-CUAUUA-3′; si-WDHD1-#2: siGenome duplexes 2
Clinical Cancer Research
h. ry 8, 2021. © 2010 American Association for Cancer

WDHD1 in Pulmonary and Esophageal Carcinogenesis
Published OnlineFirst December 22, 2009; DOI: 10.1158/1078-0432.CCR-09-1405
[D-019780-02], 5′-GGUAAUACGUGGACUCCUA-3′; andsi-AKT1: siGenome duplexes 8 [D-003000-08], 5′-GACCGCCUCUGCUUUGUCA-3′. We also designedsiRNA oligonucleotides against control-1 [EGFP, enhancedgreen fluorescent protein (GFP) gene, a mutant of Aequoreavictoria GFP], 5′-GAAGCAGCACGACUUCUUC-3′, andcontrol-2 (LUC, luciferase gene from Photinus pyralis), 5′-CGUACGCGGAAUACUUCGA-3′.Flow cytometry. Cells were collected in PBS and fixed
in 70% cold ethanol for 30 min. After treatment with100 μg/mL RNase (Sigma/Aldrich), the cells were stained
www.aacrjournals.org
Researcon Januaclincancerres.aacrjournals.org Downloaded from
with 50 μg/mL propidium iodide (Sigma/Aldrich) in PBS.Flow cytometry was done on a Becton Dickinson FACScanand analyzed by ModFit software (Verity Software House,Inc.). The cells selected from at least 20,000 ungated cellswere analyzed for DNA content.Live cell imaging. Cells were grown on a 35-mm glass-
bottom dish in phenol red–free DMEM containing 10%FCS. Cells were transfected with siRNA and subjected to timelapse imaging using a computer-assisted fluorescence micro-scope (Olympus, LCV100) equipped with an objective lens(Olympus, UAPO 40×/340 numerical aperature = 0.90),
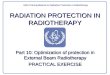
Fig. 1. Expression of WDHD1 in lung and esophageal cancers and normal tissues. A, expression of WDHD1 in a normal lung tissue, 15 clinical lungcancer samples (lung ADC, lung SCC, and SCLC; top), and 15 lung cancer cell lines (bottom) detected by semiquantitative RT-PCR analysis. B, expressionof WDHD1 in a normal esophagus and 10 clinical ESCC tissue samples and 11 ESCC cell lines detected by semiquantitative RT-PCR analysis.C, expression of WDHD1 protein in eight lung cancer and six esophageal cancer cell lines examined by Western blot analysis. D, subcellular localization ofendogenous WDHD1 protein in lung cancer LC319 cells. WDHD1 was localized abundantly in the nucleus and weakly in cytoplasm during G0-G1 toS phase, distributed mainly in cytoplasm during mitotic phase, and partly located in chromatin during anaphase to telophase.
Clin Cancer Res; 16(1) January 1, 2010 229
h. ry 8, 2021. © 2010 American Association for Cancer

Sato et al.
230
Published OnlineFirst December 22, 2009; DOI: 10.1158/1078-0432.CCR-09-1405
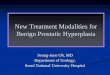
Fig. 2. Expression of WDHD1 in normal tissues and association of WDHD1 overexpression with poor prognosis for NSCLC and ESCC patients. A, Northernblot analysis of the WDHD1 transcript in 23 normal adult human tissues. A strong signal was observed in testis. B, immunohistochemical analysis ofWDHD1 protein expressions in five normal tissues (liver, heart, kidney, lung, and testis) with those in lung SCC. WDHD1 was expressed abundantly intestis (mainly in nucleus and/or cytoplasm) and lung cancers, but its expression was hardly detectable in the remaining four normal tissues. C and D,association of WDHD1 expression with poor prognosis. Kaplan-Meier analysis of survival of patients with NSCLC (C, P = 0.0403 by the log-rank test) andESCC (D, P = 0.0426 by the Log-rank test) according to expression of WDHD1.
Clin Cancer Res; 16(1) January 1, 2010 Clinical Cancer Research
Research. on January 8, 2021. © 2010 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

WDHD1 in Pulmonary and Esophageal Carcinogenesis
Published OnlineFirst December 22, 2009; DOI: 10.1158/1078-0432.CCR-09-1405
a halogen lamp, a red LED (620 nm), a CCD camera(Olympus, DP30), differential interference contrast opticalcomponents, and interference filters. For differential inter-ference contrast imaging, the red LED was used with a filtercube containing an analyzer. Image acquisition and analy-sis were done by using MetaMorph 6.13 software (Univer-sal Imaging).In vitro kinase assay. Flag-tagged WDHD1 protein that
was exogenously expressed in COS-7 cells was immuno-
www.aacrjournals.org
Researcon Januaclincancerres.aacrjournals.org Downloaded from
precipitated using Flag-M2 agarose. The immunoprecipi-tant was confirmed to be WDHD1 by Western blottingusing a mouse monoclonal anti–Flag-M2 antibody. TheFlag-tagged WDHD1 protein was incubated with recombi-nant human AKT1 protein (rhAKT1; Invitrogen) in kinasebuffer [20 mmol/L Tris (pH 7.5), 10 mmol/L MgCl2, 2mmol/L MnCl2, 1 mmol/L phenylmethylsulfonyl fluo-ride, 1 mmol/L DTT] supplemented with a mixture of pro-tease inhibitors, 10 mmol/L NaF, 5 nmol/L microcystin
Table 1. WDHD1 positivity and NSCLC patients' characteristics
A. Association between WDHD1 positivity in NSCLC tissues and patients' characteristics (N = 267)
Total
WDHD1 positive/ne/65maon-C
/ne/65femonC
h. ry 8, 2021. © 2010 Am
WDHD1 negative
Clin Cancer Res; 16(1
erican Association
P: positive vsnegative
N = 267
n = 136 (50.9%) n = 131 (49.1%)Gender
Female 89 (33.3%) 27 (10.1%) 62 (23.2%) <0.0001* Male 178 (66.7%) 109 (40.8%) 69 (25.8%)Age (y)
<65 132 (49.4%) 58 (21.7%) 74 (27.7%) 0.0277* ≥65 135 (50.6%) 78 (29.2%) 57 (21.3%)Smoking
Nonsmoker 88 (33.0%) 31 (11.6%) 57 (21.3%) 0.0004* Smoker 179 (67.0%) 105 (39.3%) 74 (27.7%)Histologic type
ADC 157 (58.8%) 59 (22.1%) 98 (36.7%) <0.0001* Non-ADC 110 (41.2%) 77 (28.8%) 33 (12.4%)pT factor
T1 114 (42.7%) 43 (16.1%) 71 (26.6%) 0.0002* T2+T3 153 (57.3%) 93 (34.8%) 60 (22.5%)pN factor
N0 208 (77.9%) 98 (36.7%) 110 (41.2%) 0.0264* N1+N2 59 (22.1%) 38 (14.2%) 21 (7.9%)B. Cox's proportional hazards model analysis of prognostic factors in patients with NSCLCsB. Cox's proportional hazards model analysis of prognostic factors in patients with NSCLCs
P
VariablesVariables Hazards ratio (95% CI)Hazard ratio (95% CI) Unfavorable/favorableUnfavorab Pavorable Univariate analysisle/f
WDHD1Univariate analysis
1.668 (1.017-2.734) Positive/negative 0.0425†0.0425†
Age (y)WDHD1 2.171 (1.313-3.590)1.668 (1.017-2.734) ≥65/65> Positive 0.0025†gative 0.0025† GenderAge (y) 2.135 (1.198-3.803)2.171 (1.313-3.590) Male/Female0.0 ≥65 100†> 100† SmokingGender 1.870 (1.075-3.253)2.135 (1.198-3.803) Smoker/non-SmokerMale/Fe 0.0267†le0.00.0267†
Histologic typeSmoking 2.493 (1.516-4.101)1.870 (1.075-3.253) Non-ADC/ADCSmoker/n 0.0003†Smoker 0.0003† pT factorHistologic type 3.722 (2.026-6.838)2.493 (1.516-4.101) T2+T3/T1 Non-AD <0.0001†/ADC <0.0001† pN factorpT factor 4.430 (2.718-7.220)3.722 (2.026-6.838) N1+N2/N0 T2+ <0.0001†T1 <0.0001† Multivariate analysisT3/pN factor 4.430 (2.718-7.220) N1+N2/N0
WDHD1Multivariate analysis
0.816 (0.467-1.424) Positive/negative 0.4741 0.4741 Age (y)WDHD1 1.806 (1.084-3.011)0.816 (0.467-1.424) ≥65/65> Positive 0.0233†gative 0.0233† GenderAge (y) 1.263 (0.568-2.811)1.806 (1.084-3.011) Male/female ≥65 0.5669> 0.5669 SmokingGender 1.290 (0.619-2.685)1.263 (0.568-2.811) Smoker/nonsmokerMale/ 0.4966ale 0.4966 Histologic typeSmoking 1.628 (0.891-2.973no)1.290 (0.619-2.685) Non-ADC/ADCSmoker/n 0.1127smoker 0.1127 pT factorHistologic type 2.291 (1.199-4.380)1.628 (0.891-2.973no) T2+T3/T1 Non-AD 0.0121†/ADC†
pN factorpT factor 3.723 (2.254-6.148)2.291 (1.199-4.380) N1+N2/N0 T2+ <0.0001†T1(Continued on the following page)
T3/ 0.0121pN factor 3.723 (2.254-6.148) N1+N2/N0 <0.0001†
) January 1, 2010 231
for Cancer

Table 1. WDHD1 positivity and NSCLC patients' characteristics (Cont'd)
C. Multivariate logistic regression analysis for the correlation between WDHD1 expression and clinicopathologiccharacteristics
Characteristics‡ Odds ratio P
Gender (male/female) 2.130 0.0339§
Age (≥65 y/<65 y) 1.335 0.2914Smoking (smoker/nonsmoker) 1.285 0.4739Histologic type (non-ADC/ADC) 2.437 0.0033§
pT factor (T2-3/T1) 1.397 0.2690pN factor (N1-2/N0) 1.971 0.0487§
Abbreviations: Non-ADC, squamous cell carcinoma plus large-cell carcinoma and adenosquamous cell carcinoma; 95% CI, 95%confidence interval.*P < 0.05 (Fisher's exact test).†P < 0.05.‡Selected factors from Table 1A that were significantly associated with WDHD1 positivity.§P < 0.05.
Sato et al.
232
Published OnlineFirst December 22, 2009; DOI: 10.1158/1078-0432.CCR-09-1405
LR, and 50 μmol/L ATP. The reaction was terminated bythe addition of a 0.2 volume of 5× protein sample bufferand the proteins were analyzed by Western blotting usingphospho-AKT substrate (PAS) antibody (Cell Signaling). Areblotting of the same membrane with anti–Flag-M2 anti-body was done to confirm that the phosphorylated bandwas WDHD1.
Results
WDHD1 expression in lung and esophageal cancers andnormal tissues. To identify novel molecules such as cancertestis antigens that were highly transactivated in a largeproportion of lung and esophageal cancers, but scarcelyexpressed in normal tissues, we had applied cDNA micro-array analysis, and identified elevated expression (3-foldor higher) of the WDHD1 transcript in the majority oflung cancer and ESCC tissue samples examined. Moreover,WDHD1 showed testis-specific expression in normal tis-sues. We confirmed its overexpression by means of semi-quantitative RT-PCR experiments in 14 of 15 lung cancertissues, in all of 15 lung cancer cell lines, in 6 of 10 ESCCtissues, and in 8 of 11 ESCC cell lines (Fig. 1A and B). Wealso confirmed its elevated expression in another set ofprimary tumor tissues (six of six NSCLCs and five of sixESCCs); however, its expression was hardly detectable intheir adjacent normal lung or esophagus tissues (Supple-mentary Fig. S1A). We subsequently confirmed by Westernblotting analysis overexpression of WDHD1 protein (126kDa) in lung and esophageal cancer cell lines using anti-WDHD1 polyclonal antibody (Fig. 1C). To examine thesubcellular localization of endogenous WDHD1 in cancercells, we performed immunocytochemical analysis of lungcancer LC319 cells that overexpressed WDHD1 proteinusing anti-WDHD1 polyclonal antibody. WDHD1 wasdetected abundantly in the nucleus and weakly in cyto-
Clin Cancer Res; 16(1) January 1, 2010
Researcon Januaclincancerres.aacrjournals.org Downloaded from
plasm in the cells during G0-G1 to S phase and in chroma-tin during anaphase to telophase (Fig. 1D).Northern blot analysis using a WDHD1 cDNA fragment
as a probe identified about 5-kb transcript exclusively intestis (Fig. 2A). Immunohistochemical analysis with anti-WDHD1 polyclonal antibodies using five normal tissues(liver heart, kidney, lung, and testis) as well as lung cancertissues revealed strong staining of WDHD1 in testis andlung cancer cells (mainly in nucleus and weakly in cyto-plasm), but its expression was hardly detectable in the re-maining four normal tissues (Fig. 2B).Association of WDHD1 expression with poor prognosis for
patients with NSCLC or ESCC. To investigate the biologicaland clinicopathologic significance of WDHD1 in pulmo-nary and esophageal carcinogenesis, we carried out immu-nohistochemical staining on tissue microarray containingtissue sections from 267 NSCLC and 283 ESCC cases thatunderwent surgical resection. WDHD1 staining with poly-clonal antibody specific to WDHD1 was mainly observedin the nucleus as well as the cytoplasm of tumor cells, butnot detected in their adjacent normal lung tissue cells(Supplementary Fig. S1B and C). Of the 267 NSCLCs ex-amined, WDHD1 was stained positively in 136 cases(50.9%) and negatively in 131 cases (49.1%; Table 1A).We then examined the association of WDHD1 expressionwith clinical outcomes, and found that expression ofWDHD1 in NSCLCs was significantly associated with malegender (P < 0.0001, Fisher's exact test; Table 1A), olderage (≥65 years; P = 0.0277), smoker (current or exsmokers;P = 0.0004), non-ADC histology (P < 0.0001), larger tu-mor size (pT2-3; P = 0.0002), presence of lymph node me-tastasis (pN1-2; P = 0.0264), and with tumor-specific5-year survival after the resection of primary tumors(P = 0.0403 by log-rank test; Supplementary Table S3A;Fig. 2C). We also applied univariate analysis to evaluateassociations between patient prognosis and several factorsincluding age, gender, smoking history, pT stage (tumor
Clinical Cancer Research
h. ry 8, 2021. © 2010 American Association for Cancer

P
alysis009-1 0.0435*10-1 0.774693-6 0.0009*33-3 <0.0001*
<0.0001*nalys
99-2 0.0104*46-5 0.0012*73-3 0.0004*
WDHD1 in Pulmonary and Esophageal Carcinogenesis
Published OnlineFirst December 22, 2009; DOI: 10.1158/1078-0432.CCR-09-1405
size, T1 versus T2+T3), pN stage (node status, N0 versus N1
+N2), histologic type (non-ADC versus ADC), andWDHD1expression (positive versus negative). All those parameterswere significantly associated with poor prognosis (Table1B). In multivariate analysis, WDHD1 status did not reachthe statistically significant level as an independent prognos-tic factor for surgically treated lung cancer patients enrolledin this study (P = 0.4741), whereas pT and pN stages as wellas age did so (Table 1B). The result might be due to the rel-evance ofWDHD1 expression mainly to the other prognos-tic factors—male gender, non-ADC histology, and/orpresence of lymph node metastasis in lung cancer—proba-bly because multivariate logistic regression analysis for thesix clinicopathologic parameters that were significantly as-sociated with WDHD1 positivity in lung cancer (Table 1A)also determined that these three factors were independentfeatures associated with WDHD1 expression (P = 0.0339,0.0033, and 0.0487, respectively; Table 1C).Of the 283 ESCC cases examined, WDHD1 was stained
positively in the nucleus as well as the cytoplasm of tumor
www.aacrjournals.org
Researcon Januaclincancerres.aacrjournals.org Downloaded from
cells in 175 cases (61.8%) and negatively in 108 cases(38.2%), whereas their adjacent normal esophagus tissueswere not stained (Supplementary Fig. S1D and E; Table 2A).ESCCpatientswhose tumors showedWDHD1expression re-vealed shorter tumor-specific survival periods comparedwith those with absent WDHD1 expression (P = 0.0426 bylog-rank test; Supplementary Table S3B; Fig. 2D).We also ap-plied univariate analysis to evaluate associations betweenESCC patient prognosis and several factors including age,gender, pT stage (tumor depth, T1 versus T2+T3), pN stage(node status, N0 versus N1+N2), andWDHD1 status (positiveversus negative). All those parameters except for age were sig-nificantly associated with poor prognosis (Table 2B). Multi-variate analysis using a Cox proportional hazard factorsdetermined that WDHD1 (P = 0.0104) as well as other threefactors (male gender, larger tumor size, and lymph nodemetastasis) were independent prognostic factors for surgi-cally treated ESCC patients (Table 2B).Effects of WDHD1 on cell growth and cell cycle progres-
sion. To assess whether WDHD1 plays an essential role
Table 2. WDHD1 positivity and ESCC patients’ characteristics
A. Association between WDHD1-positivity in ESCC tissues and patients' characteristics (N = 283)
Total
WDHD1 positiveh. ry 8, 2021.
WDHD1 negative
Clin Cancer
© 2010 American Ass
P: positive vs negative
N = 283
n = 175 (61.8%) n = 108 (38.2%)Gender
Female 27 (9.5%) 15 (5.3%) 12 (4.2%) 0.5343 Male 256 (90.5%) 160 (56.5%) 96 (33.9%)Age (y)
<65 176 (62.2%) 116 (41.0%) 60 (21.2%) 0.0781 ≥65 107 (37.8%) 59 (20.8%) 48 (17.0%)pT factor
T1 73 (25.8%) 43 (15.2%) 30 (10.6%) 0.5775 T2+T3 210 (74.2%) 132 (46.6%) 78 (27.6%)pN factor
N0 91 (32.2%) 58 (20.5%) 33 (11.7%) 0.6954 N1+N2 192 (67.8%) 117 (41.3%) 75 (26.5%)B. Cox's proportional hazards model analysis of prognostic factors in patients with ESCCsB. Cox's proportional hazards model analysis of prognostic factors in patients with ESCCs
VariablesVariables
Hazards ratio (95% CI)Hazards ra Unfavorable/Favorable5% CI) Pavorable/FavorableUnivariate analysis
tio (9 Unf
WDHD1Univariate an
1.1317 (1.009-1.863) Positive/negative 0.0435* Age (y)WDHD1 0.957 (0.710-1.290)1.1317 (1. ≥65/65>.863) 0.7746Positive/negativeGenderAge (y)
3.117 (1.593-6.101)0.957 (0.7 Male/Female.290) 0.0009*≥65/65>pT factorGender
2.702 (1.833-3.983)3.117 (1.5 T2+T3/T1.101) <0.0001*Male/FemalepN factorpT factor
3.428 (2.347-5.009)2.702 (1.8 N1+N2/N0.983) <0.0001*T2+T3/T1Multivariate analysispN factor 3.428 (2.347-5.009) N1+N2/N0
WDHD1Multivariate a
1.496 (1.099-2.036)is Positive/negative 0.0104* GenderWDHD1 3.031 (1.546-5.940)1.496 (1.0 Male/female.036) 0.0012*Positive/negativepT factorGender
2.048 (1.373-3.053)3.031 (1.5 T2+T3/T1.940) 0.0004*Male/femalepN factorpT factor
2.865 (1.936-4.239)2.048 (1.3 N1+N2/N0.053) <0.0001*T2+T3/T1*P < 0.05.
pN factor 2.865 (1.936-4.239) N1+N2/N0 <0.0001*
*P < 0.05.
Res; 16(1) January 1, 2010 233
ociation for Cancer

Sato et al.
234
Published OnlineFirst December 22, 2009; DOI: 10.1158/1078-0432.CCR-09-1405
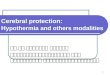
in cell growth or survival, we carried out a colony forma-tion assay of COS-7 transfected with WDHD1 expressionplasmids and confirmed the growth-promoting activityof cells overexpressing WDHD1, compared with thosetransfected with mock vectors (Supplementary Fig. S2).We further constructed several siRNA expression oligonu-cleotides specific to WDHD1 sequences and transfectedthem into lung cancer A549 cells as well as esophagealcancer TE9 cells that endogenously expressed WDHD1 athigh levels. Knockdown effects were confirmed by semi-quantitative RT-PCR when we used si-WDHD1-#1 andsi-WDHD1-#2 (Fig. 3A). MTT assays and colony forma-tion assays revealed a drastic reduction in the number ofcells transfected with si-WDHD1-#1 and #2 (Supplemen-tary Fig. S3; Fig. 3B). Flowcytometric analysis at 24 to 72hours after the transfection of si-WDHD1 to the A549 andTE9 cells revealed the decrease of the number of cells at Sphase and the increase of that in G0-G1 phase (Supple-mentary Fig. S4A; Fig. 3C). To further investigate the effectof WDHD1 on the cell cycle progression, we synchronizedA549 and TE9 cells (5 × 105 cells/100-mm dish) trans-fected with siRNA for si-WDHD1. The flow cytometricand Western blot analyses at 0, 4.5, and 9 hours after re-moval of aphidicolins showed that the number of theA549 and TE9 cells in G0-G1 phase was increased andthe progression to S phase was delayed (SupplementaryFig. S4B and C). To further clarify the effect of WDHD1knockdown on cellular morphology and cell cycle, we ex-amined A549 cells transfected with siRNA for WDHD1 us-ing time lapse microscopy. Although the cell division wasobserved at about every 10 hours in control cells, theWDHD1 knocked down cells started cell division slowlyand died shortly after cell division (Fig. 3D).Phosphorylation of WDHD1. WDHD1 protein was de-
tected as double bands by Western blotting, indicating apossible modification of the WDHD1 protein. Therefore,we first incubated extracts from A549 cells that overex-pressed endogenous WDHD1 and also COS-7 cells trans-fected with WDHD1-expressing plasmids in the presenceor absence of protein phosphatase (New England Bio-labs), and analyzed the molecular size of WDHD1 proteinby Western blot analysis. The measured weight of the ma-jority of both endogenous and exogenous WDHD1 pro-tein in the extracts treated with phosphatase was smallerthan that in the untreated cells. The data indicated thatWDHD1 was possibly phosphorylated in cells (Supple-mentary Fig. S5A). Immunoprecipitation of WDHD1 withanti-WDHD1 antibody followed by immunoblotting withpan-phospho–specific antibodies indicated phosphoryla-tion of endogenous WDHD1 at its serine and tyrosine re-sidues (Supplementary Fig. S5B).Involvement of WDHD1 in PI3K/AKT pathway. To eluci-
date the importance of WDHD1 phsphorylation in cancercells, we next screened the candidate kinases for WDHD1by referring possible phosphorylation sites on WDHD1protein, and found a consensus phosphorylation site forAKT kinase (R-X-R-X-X-S374; ref. 47). PI3K/AKT pathwayis well known to be activated in a wide range of tumor
Clin Cancer Res; 16(1) January 1, 2010
Researcon Januaclincancerres.aacrjournals.org Downloaded from
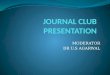
types, and this triggers a cascade of responses, from cellgrowth and proliferation to survival, motility, epithelial-mesenchymal transition, and angiogenesis (48). We there-fore examined whether WDHD1 could be involved in thePI3K and/or AKT pathway. We first immunoblotted, usingPAS antibody, the Flag-tagged WDHD1 protein that wasexogenously expressed in COS-7 cells and immunopreci-pitated using Flag-M2 agarose, and detected the positiveband that represented possibly phosphorylation by endog-enous AKT (Fig. 4A). In vitro kinase assay using the Flag-tagged WDHD1 immunoprecipitant as a substrate andrecombinant human AKT1 protein (rhAKT1) as a kinasewith subsequent immunoblotting with PAS antibody alsoproved the direct phosphorylation of WDHD1 by AKT1(Fig. 4B). To examine the effect of AKT1 on WDHD1 pro-tein function in cancer cells, we measured the level of en-dogenous WDHD1 protein after transfection of siRNA forAKT1 to LC319 cells or after treatment of the cells with var-ious concentrations of LY294002 (0-20 μmol/L for 24hours), a specific inhibitor of the catalytic subunit ofPI3K. Total amount of WDHD1 as well as phosphorylatedWDHD1 was significantly decreased by LY294002 treat-ment or introduction of siRNA for AKT1, indicating a pos-sibility that WDHD1 protein stability is regulated by thePI3K/AKT signaling (Fig. 4C and D).
Discussion
We performed a genome-wide expression profile analy-sis of 101 lung cancers and 19 ESCC cells after enrichmentof cancer cells by laser microdissection, using a cDNA mi-croarray containing 27,648 genes or expressed sequencetags (7–12). Through the analyses, we identified a numberof genes that could be potentially good candidates for thedevelopment of novel diagnostic markers, therapeuticdrugs, and/or immunotherapy (13–37). In this study, weselected WDHD1 as a good candidate for cancer biomark-er(s) for lung cancer and/or ESCC, and provided evidencesfor its possible role in human carcinogenesis.WDHD1, a homologue of Ctf4/Mcl1 in Saccharomyces
cerevesiae and Schizosaccharomyces pombe, encodes a puta-tive 1129 amino acid protein with high-mobility groupbox domains and a WD-repeat domain. Ctf4/Mcl1 hasbeen described as a part of a replisome progression com-plex that associates with the GINS complex as well as withDNA polymerase/primase (49). To maintain the genomeintegrity, chromosomal DNA is precisely replicated onlyonce per cell cycle. Initiation of chromosomal replicationstarts by the binding of several factors to replication ori-gins, and the interactions among these factors are crucialfor subsequent processes (50). Ctf4/Mcl1 physically inter-acts with DNA pol α and induces the association of Pol αto chromatin, and plays a critical role in lagging strandsynthesis and Okazaki fragment processing (40). Recentstudies showed that WDHD1 interacts with MCM10 andis essential for DNA synthesis, suggesting its role as a rep-lication initiation factor (41). The function of Ctf4/Mcl1in chromosome replication, cohesion, and segregation
Clinical Cancer Research
h. ry 8, 2021. © 2010 American Association for Cancer

WDHD1 in Pulmonary and Esophageal Carcinogenesis
Published OnlineFirst December 22, 2009; DOI: 10.1158/1078-0432.CCR-09-1405
Fig. 3. Growth-promoting effect of WDHD1. A and B, inhibition of growth of a lung cancer cell line A549 (left) and an esophageal cancer cell line TE9 (right)by siRNAs against WDHD1. A, WDHD1 gene knockdown effect in A549 and TE9 cells by two si-WDHD1 (si-WDHD1-#1 and si-WDHD1-#2) and twocontrol siRNAs (si-EGFP and si-LUC), analyzed by semiquantitative RT-PCR. B, MTT assays of A549 and TE9 cells transfected with si-WDHD1s or controlsiRNAs. Columns, relative absorbance of triplicate assays; bars, SD. C, flow cytometric analysis of lung cancer cells transfected with si-WDHD1. A549cells were transfected with si-WDHD1-#1 or si-LUC, and collected at 24, 48, and 72 h after transfection for flow cytometry. The numbers besides the panelsindicate the percentage of cells at each phase.
Clin Cancer Res; 16(1) January 1, 2010www.aacrjournals.org 235
Research. on January 8, 2021. © 2010 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Fig. 3. Continued. D, time lapse imaging analysis of A549 cells transfected with si-WDHD1. A549 cells were transfected with si-WDHD1-#1 or si-LUCand their microscopic images were captured every 30 min. Representative microscopic images of cells at every 12 h (from 24-108 h; left) and at every 30 min(from 90-92.5 h; right) are shown.
Sato et al.
236
Published OnlineFirst December 22, 2009; DOI: 10.1158/1078-0432.CCR-09-1405
was reported to date, but the overexpression of WDHD1 inhuman cancer cells and its possible role in human carcino-genesis have not been described.In this study, we obtained important clinicopathologic
and biological evidences supporting the significance ofWDHD1 transactivation in human carcinogenesis. Weshowed through our tissue microarray experiments thatNSCLC and ESCC patients with WDHD1-positive tumorshad shorter cancer-specific survival periods than thosewith WDHD1-negative tumors. In addition, the enhancedexpression of WDHD1 significantly promoted growth ofmammalian cells. Moreover, WDHD1 knockdown bysiRNA in cancer cells delayed S-phase entry and progres-sion, and resulted in cell death right after cell division.The data imply the importance of WDHD1 in cancer cellcycle progression, although further detailed analyses ofWDHD1 function in coordinated maintenance of thecancer genome integrity are required.Our study also described the involvement of WDHD1
activation in cancer cell signaling. WDHD1 seemed tobe phosphorylated and stabilized by AKT1. PI3K/AKT sig-naling is important for cell proliferation and survival (48).In addition, AKT1 phosphorylation frequently occurs in
Clin Cancer Res; 16(1) January 1, 2010
Researcon Januaclincancerres.aacrjournals.org Downloaded from
various human cancers, and has been recognized as a riskfactor for early disease recurrence and poor prognosis(48). Our data indicated that inhibition of PI3K/AKTpathway using LY294002 or siRNA for AKT1 decreasedthe level of total and phosphorylated WDHD1 in lungcancer cells. Because these results indicate that WDHD1plays a significant role in cancer cell growth/survival asone of the components of the PI3K/AKT pathway, selec-tive targeting of functional interaction between AKT1and WDHD1 could be a promising therapeutic strategy.Further analyses of the mechanism of growth suppressionby specific inhibition of WDHD1 phosphorylation byAKT1 may be of the great benefit toward the developmentof new types of anticancer agents.From the result of Northern blot and immunohisto-
chemical analyses, WDHD1 was expressed only in testisand cancer cells. Cancer testis antigens have been recog-nized as a group of highly attractive targets for cancer vac-cine treatment (34–37). Although other factors, such asthe in vivo spontaneous immunogenicity of the protein,are also important and further examination will be neces-sary, WDHD1 oncoantigen may be useful for screeningof HLA-restricted epitope peptides for cancer vaccine that
Clinical Cancer Research
h. ry 8, 2021. © 2010 American Association for Cancer

WDHD1 in Pulmonary and Esophageal Carcinogenesis
Published OnlineFirst December 22, 2009; DOI: 10.1158/1078-0432.CCR-09-1405
Fig. 4. Possible regulation of WDHD1 stability by its phosphorylation through PI3K/AKT signaling. A, immunoprecipitant of Flag-tagged WDHD1 inCOS-7 cells transfected with Flag-tagged WDHD1-expressing plasmid was detected with anti-PAS antibody or anti–Flag-M2 antibody. B, in vitrophosphorylation of Flag-tagged WDHD1 protein by recombinant human AKT1 (rhAKT1). C, reduction of WDHD1 protein by PI3K inhibition with LY294002.LC319 were treated with PI3K inhibitor LY294002 in concentrations of 0 or 20 μmol/L for 24 h and served for Western blot analysis. D, reduction ofWDHD1 protein by AKT1 inhibition with siRNA against AKT1. LC319 were transfected with siRNA for AKT1 or EGFP and served for Western blot analysis.
Clin Cancer Res; 16(1) January 1, 2010www.aacrjournals.org 237
Research. on January 8, 2021. © 2010 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Sato et al.
238
Published OnlineFirst December 22, 2009; DOI: 10.1158/1078-0432.CCR-09-1405
can induce specific immune responses by cytotoxic T cellsagainst WDHD1-positive cancer cells. Because WDHD1expression could have pivotal functions in cancer cellsurvival, vaccination with the peptides from this proteinshould reduce the risk of the emergence of immune escapevariant tumors that have lost their antigen expression.In conclusion, WDHD1 was overexpressed in the great
majority of lung and esophageal cancer tissues, and itis likely to play significant roles in cancer cell growthand/or survival. The data indicate WDHD1 to be a poten-tial therapeutic target and a candidate biomarker forpatients with lung and esophageal cancers.
Clin Cancer Res; 16(1) January 1, 2010
Researcon Januaclincancerres.aacrjournals.org Downloaded from
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
Acknowledgments
The costs of publication of this article were defrayed inpart by the payment of page charges. This article musttherefore be hereby marked advertisement in accordancewith 18 U.S.C. Section 1734 solely to indicate this fact.Received 6/2/09; revised 8/27/09; accepted 8/29/09;
published OnlineFirst 12/22/09.
References
1. Berwick M, Schantz S. Chemoprevention of aerodigestive cancer.Cancer Metastasis Rev 1997;16:329–47.2. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer
J Clin 2008;58:71–96.3. Shimada H, Nabeya Y, Okazumi S, et al. Prediction of survival with
squamous cell carcinoma antigen in patients with resectable esoph-ageal squamous cell carcinoma. Surgery 2003;133:486–94.
4. Hida T, Ogawa S, Park JC, et al. Gefitinib for the treatment of non-small-cell lung cancer. Expert Rev Anticancer Ther 2009;9:17–35.
5. Shepherd FA, Rodrigues Pereira J, Ciuleanu T, et al. Erlotinib in pre-viously treated non-small-cell lung cancer. N Engl J Med 2005;353:123–32.
6. Daigo Y, Nakamura Y. From cancer genomics to thoracic oncology:discovery of new biomarkers and therapeutic targets for lung andesophageal carcinoma. Gen Thorac Cardiovasc Surg 2008;56:43–53.
7. Kikuchi T, Daigo Y, Katagiri T, et al. Expression profiles of non-smallcell lung cancers on cDNA microarrays: identification of genes forprediction of lymph-node metastasis and sensitivity to anti-cancerdrugs. Oncogene 2003;22:2192–205.
8. Kakiuchi S, Daigo Y, Tsunoda T, Yano S, Sone S, Nakamura Y. Ge-nome-wide analysis of organ-preferential metastasis of human smallcell lung cancer in mice. Mol Cancer Res 2003;1:485–99.
9. Kakiuchi S, Daigo Y, Ishikawa N, et al. Prediction of sensitivity of ad-vanced non-small cell lung cancers to gefitinib (Iressa, ZD1839).Hum Mol Genet 2004;13:3029–43.
10. Kikuchi T, Daigo Y, Ishikawa N, et al. Expression profiles of meta-static brain tumor from lung adenocarcinomas on cDNA microarray.Int J Oncol 2006;28:799–805.
11. Taniwaki M, Daigo Y, Ishikawa N, et al. Gene expression profiles ofsmall-cell lung cancers: molecular signatures of lung cancer. Int JOncol 2006;29:567–75.
12. Yamabuki T, Daigo Y, Kato T, et al. Genome-wide gene expressionprofile analysis of esophageal squamous cell carcinomas. Int J Oncol2006;28:1375–84.
13. Suzuki C, Daigo Y, Kikuchi T, Katagiri T, Nakamura Y. Identificationof COX17 as a therapeutic target for non-small cell lung cancer. Can-cer Res 2003;63:7038–41.
14. Ishikawa N, Daigo Y, Yasui W, et al. ADAM8 as a novel serologicaland histochemical marker for lung cancer. Clin Cancer Res 2004;10:8363–70.
15. Kato T, Daigo Y, Hayama S, et al. A novel human tRNA-dihydrouri-dine synthase involved in pulmonary carcinogenesis. Cancer Res2005;65:5638–46.
16. Furukawa C, Daigo Y, Ishikawa N, et al. Plakophilin 3 oncogene asprognostic marker and therapeutic target for lung cancer. CancerRes 2005;65:7102–10.
17. Ishikawa N, Daigo Y, Takano A, et al. Increases of amphiregulin andtransforming growth factor-α in serum as predictors of poor re-sponse to gefitinib among patients with advanced non-small celllung cancers. Cancer Res 2005;65:9176–84.
18. Suzuki C, Daigo Y, Ishikawa N, et al. ANLN plays a critical role inhuman lung carcinogenesis through the activation of RHOA and by
involvement in the phosphoinositide 3-kinase/AKT pathway. CancerRes 2005;65:11314–25.
19. Ishikawa N, Daigo Y, Takano A, et al. Characterization of SEZ6L2cell-surface protein as a novel prognostic marker for lung cancer.Cancer Sci 2006;97:737–45.
20. Takahashi K, Furukawa C, Takano A, et al. The neuromedin u-growthhormone secretagogue receptor 1b/neurotensin receptor 1 onco-genic signaling pathway as a therapeutic target for lung cancer. Can-cer Res 2006;66:9408–19.
21. Hayama S, Daigo Y, Kato T, et al. Activation of CDCA1-2, membersof centromere protein complex, involved in pulmonary carcinogene-sis. Cancer Res 2006;66:10339–48.
22. Kato T, Hayama S, Yamabuki Y, et al. Increased expression of insu-lin-like growth factor-II messenger RNA-binding protein 1 is associ-ated with tumor progression in patients with lung cancer. Clin CancerRes 2007;13:434–42.
23. Suzuki C, Takahashi K, Hayama S, et al. Identification of Myc-asso-ciated protein with JmjC domain as a novel therapeutic target onco-gene for lung cancer. Mol Cancer Ther 2007;6:542–51.
24. Yamabuki T, Takano A, Hayama S, et al. Dickkopf-1 as a novel se-rologic and prognostic biomarker for lung and esophageal carcino-mas. Cancer Res 2007;67:2517–25.
25. HayamaS, Daigo Y, Yamabuki T, et al. Phosphorylation and activationof cell division cycle associated 8 by aurora kinaseBplays a significantrole in human lung carcinogenesis. Cancer Res 2007;67:4113–22.
26. Taniwaki M, Takano A, Ishikawa N, et al. Activation of KIF4A as aprognostic biomarker and therapeutic target for lung cancer. ClinCancer Res 2007;13:6624–31.
27. Ishikawa N, Takano A, Yasui W, et al. Cancer-testis antigen lympho-cyte antigen 6 complex locus K is a serologic biomarker and a ther-apeutic target for lung and esophageal carcinomas. Cancer Res2007;67:11601–11.
28. Mano Y, Takahashi K, Ishikawa N, et al. Fibroblast growth factor re-ceptor 1 oncogene partner as a novel prognostic biomarker and ther-apeutic target for lung cancer. Cancer Sci 2007;98:1902–13.
29. Kato T, Sato N, Hayama S, et al. Activation of HJURP (Hollidayjunction-recognizing protein) involved in the chromosomal stabilityand immortality of cancer cells. Cancer Res 2007;67:8544–53.
30. Kato T, Sato N, Takano A, et al. Activation of placenta specific tran-scription factor distal-less homeobox 5 predicts clinical outcome inprimary lung cancer patients. Clin Cancer Res 2008;14:2363–70.
31. Dunleavy EM, Roche D, Tagami H, et al. HJURP is a cell-cycle-dependent maintenance and deposition factor of CENP-A at cen-tromeres. Cell 2009;137:485–97.
32. Hirata D, Yamabuki T, Ito T, et al. Involvement of epithelial cell trans-forming sequence 2 (ECT2) oncoantigen in lung and esophageal can-cer progression. Clin Cancer Res 2009;15:256–66.
33. Takano A, Ishikawa N, Nishino R, et al. Identification of Nectin-4 on-coprotein as a diagnostic and therapeutic target for lung cancer.Cancer Res. 2009;69:6694–703.
34. Suda T, Tsunoda T, Daigo Y, Nakamura Y, Tahara H. Identification ofhuman leukocyte antigen-A24-restricted epitope peptides derived
Clinical Cancer Research
h. ry 8, 2021. © 2010 American Association for Cancer

WDHD1 in Pulmonary and Esophageal Carcinogenesis
Published OnlineFirst December 22, 2009; DOI: 10.1158/1078-0432.CCR-09-1405
from gene products upregulated in lung and esophageal cancers asnovel targets for immunotherapy. Cancer Sci 2007;98:1803–8.
35. Mizukami Y, Kono K, Daigo Y, et al. Detection of novel cancer-testisantigen-specific T-cell responses in TIL, regional lymph nodes, andPBL in patients with esophageal squamous cell carcinoma. CancerSci 2008;99:1448–54.
36. Harao M, Hirata S, Irie A, et al. HLA-A2-restricted CTL epitopes of anovel lung cancer-associated cancer testis antigen, cell division cy-cle associated 1, can induce tumor-reactive CTL. Int J Cancer 2008;123:2616–25.
37. Kono K, Mizukami Y, Daigo Y, et al. Vaccination with multiple pep-tides derived from novel cancer-testis antigens can induce specificT-cell responses and clinical responses in advanced esophagealcancer. Cancer Sci. 2009;100:1502–9.
38. Kouprina N, Kroll E, Bannikov V, et al. CTF4 (CHL15) mutants exhibitdefective DNA metabolism in the yeast Saccharomyces cerevisiae.Mol Cell Biol 1992;20:5736–47.
39. Petronczki M, Chwalla B, Siomos MF, et al. Sister-chromatid cohe-sion mediated by the alternative RF-CCtf18/Dcc1/Ctf8, the helicaseChl1 and the polymerase-α-associated protein Ctf4 is essential forchromatid disjunction during meiosis II. J Cell Sci 2004;83:3547–59.
40. Tsutsui Y, Morishita T, Natsume T, et al. Genetic and physical inter-actions between Schizosaccharomyces pombe Mcl1 and Rad2,Dna2 and DNA polymerase α: evidence for a multifunctional role ofMcl1 in DNA replication and repair. Curr Genet 2005;48:34–43.
41. Zhu W, Ukomadu C, Jha S, et al. Mcm10 and And-1/CTF4 recruitDNA polymerase α to chromatin for initiation of DNA replication.Genes Dev 2007;21:2288–99.
www.aacrjournals.org
Researcon Januaclincancerres.aacrjournals.org Downloaded from
42. Nishihira T, Hashimoto Y, Katayama M, et al. Molecular and cellularfeatures of esophageal cancer cells. J Cancer Res Clin Oncol 1993;119:441–9.
43. In: Sobin LH, Witterkind C, editors. TNM Classification of MalignantTumours. 6th ed New York: Whiley-Liss; 2002.
44. Callagy G, Cattaneo E, Daigo Y, et al. Molecular classification ofbreast carcinomas using tissue microarrays. Diagn Mol Pathol2003;12:27–34.
45. Callagy G, Pharoah P, Chin SF, et al. Identification and validationof prognostic markers in breast cancer with the complementaryuse of array-CGH and tissue microarrays. J Pathol 2005;205:388–96.
46. Chin SF, Daigo Y, Huang HE, et al. A simple and reliable pretreat-ment protocol facilitates fluorescent in situ hybridisation on tissuemicroarrays of paraffin wax embedded tumour samples. Mol Pathol2003;56:275–9.
47. Olsen JV, Blagoev B, Gnad F, et al. Global, in vivo, and site-specificphosphorylation dynamics in signaling networks. Cell 2006;127:635–48.
48. Kandel ES, Hay N. The regulation and activities of the multifunc-tional serine/threonine kinase Akt/PKB. Exp Cell Res 1999;253:210–29.
49. Gambus A, Jones RC, Sanchez-Diaz A, et al. GINS maintains asso-ciation of Cdc45 with MCM in replisome progression complexes ateukaryotic DNA replication forks. Nat Cell Biol 2006;8:358–66.
50. Gonzalez MA, Tachibana KE, Laskey RA, et al. Control of DNAreplication and its potential clinical exploitation. Nat Rev Cancer2005;5:135–41.
Clin Cancer Res; 16(1) January 1, 2010 239
h. ry 8, 2021. © 2010 American Association for Cancer

2010;16:226-239. Published OnlineFirst December 22, 2009.Clin Cancer Res Nagato Sato, Junkichi Koinuma, Masahiro Fujita, et al. CarcinogenesisBinding Protein 1 in Pulmonary and Esophageal Activation of WD Repeat and High-Mobility Group Box DNA
Updated version
10.1158/1078-0432.CCR-09-1405doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2010/01/07/1078-0432.CCR-09-1405.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/16/1/226.full#ref-list-1
This article cites 42 articles, 20 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/16/1/226.full#related-urls
This article has been cited by 9 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/16/1/226To request permission to re-use all or part of this article, use this link
Research. on January 8, 2021. © 2010 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 22, 2009; DOI: 10.1158/1078-0432.CCR-09-1405