Embed Size (px)
Citation preview

ORIG INAL ART ICLE
Acute aortocaval fistula: role of low perfusion pressure andsubendocardial remodeling on left ventricular functionFl�avia R. R. Mazzo*, Clovis de Carvalho Frimm*, Ana Iochabel S. Moretti†, Maria C. Guido† andMarcia K. Koike**Laboratory of Medical Investigation, LIM-51, Department of Clinical Medicine, University of S~ao Paulo Medical School, S~aoPaulo, Brazil and †Heart Institute (InCor), University of Sao Paulo Medical School, S~ao Paulo, Brazil
INTERNATIONAL
JOURNAL OF
EXPERIMENTAL
PATHOLOGY
doi: 10.1111/iep.12025
Received for publication: 14 August2012Accepted for publication: 5 March2013
Correspondence:Marcia Kiyomi KoikeLaboratory of Medical InvestigationLIM-51Department of Clinical MedicineUniversity of S~ao Paulo MedicalSchoolS~ao PauloBrazilTel.: +55 11 3061-8485Fax: +55 11 3061-7170E-mail: [email protected]
SUMMARY
The experimental model of aortocaval fistula is a useful model of cardiac hypertro-
phy in response to volume overload. In the present study it has been used to investi-
gate the pathologic subendocardial remodeling associated with the development of
heart failure during the early phases (day 1, 3, and 7) following volume overload.
Compared with sham treated rats, aortocaval fistula rats showed lower systemic
blood pressure and higher left ventricular end-diastolic pressure This resulted in
lower coronary driving pressure and left ventricular systolic and diastolic dysfunc-
tion. Signs of myocyte necrosis, leukocyte cell infiltration, fibroplasia and collagen
deposition appeared sequentially in the subendocardium where remodeling was more
prominent than in the non-subendocardium. Accordingly, increased levels of TNF-
alpha, IL-1 beta, and IL-6, and enhanced MMP-2 activity were all found in the sub-
endocardium of rats with coronary driving pressure �60 mmHg. The coronary
driving pressure was inversely correlated with MMP-2 activity in subendocardium in
all time-points studied, and blood flow in this region showed positive correlation
with systolic and diastolic function at day 7. Thus the predominant subendocardial
remodeling that occurs in response to low myocardial perfusion pressure during the
acute phases of aortocaval fistula contributes to early left ventricular dysfunction.
Keywords
aortocaval fistula, coronary perfusion, cytokines, fibrosis, metalloproteinases,
subendocardium
The remodelling of the heart is associated with increased
cardiovascular morbidity and mortality (Fedak et al. 2005).
It has been characterized by enhanced gene and protein
expression resulting in changes of cardiac geometry, shape
and function (Cohn et al. 2000).
Surgical aortocaval fistula represents an experimental
model of cardiac hypertrophy in response to volume over-
load (Garcia & Diebold 1990). In this study it has been
employed in rats to investigate the pathophysiologic mecha-
nisms associated with the development of heart failure dur-
ing the early phases following volume overload. Although
distinct in fundamental structural cardiovascular aspects, we
believe aortocaval fistula mimics the acute volume overload
to the left ventricle that occurs in emergency clinical entities
such as acute aortic valve insufficiency and myocardial
infarction.
The increase in preload gives rise to the development of
the eccentric type of cardiac hypertrophy with sarcomere
lengthening and cardiac chamber enlargement (Olivetti et al.
2000). According to Laplace′s law, the increase in chamber
dimensions corresponds to a proportional elevation in sys-
tolic wall stress. The physiologic adaptation consists of wall
thickening to counteract the elevated systolic wall stress,
thus preserving systolic function. Since myocardial hypertro-
phy is not developed sufficiently to compensate uniformly,
chamber enlargement proves to be out of proportion to wall
thickening. This results in unbalanced systolic wall stress
with elevated oxygen consumption and cardiac dysfunction
(Grossman et al. 1975).
Previously, it has been recognized that myocardial remod-
elling is accompanied by extracellular matrix changes char-
acterized mainly by interstitial fibrosis (Weber 2004).
© 2013 The Authors.
178 International Journal of Experimental Pathology © 2013 International Journal of Experimental Pathology
Int. J. Exp. Path. (2013), 94, 178–187

Furthermore, myocardial fibrosis was shown to be associated
with cardiac dysfunction and heart failure (Weber & Brilla
1991). The contributing role of myocardial fibrosis in the
development of pathologic hypertrophy has been demon-
strated by clinical findings showing a poor cardiovascular
outcome (Brilla et al. 2003). The presence of myocardial
fibrosis has been disputed in aortocaval fistula (Dolgilevich
et al. 2001; Cox et al. 2004), but seems obvious when left
ventricular systolic dysfunction is present (Dolgilevich et al.
2001; Guido et al. 2007). Previously we have demonstrated
that the accumulation of excess collagen fibres occurs in
chronic aortocaval fistula within the subendocardium predo-
minantly (Guido et al. 2007). Also it has been recognized
that extracellular matrix must be remodelled by the activa-
tion of metalloproteinase (MMP) to allow cardiac chamber
to enlarge (Brower & Janicki 2001). Oxidative stress (Cox
et al. 2002), leucocyte migration (Kolpakov et al. 2009),
degranulation of mast cells (Brower et al. 2002), release of
cytokines (Cox et al. 2002; Guido et al. 2007) may all
potentially activate myocardial MMPs. The inflammatory
response and MMP activation have been suggested to result
from increased preload (Brower et al. 2002). However, in
previous aortocaval fistula experiments, we showed that left
ventricular end-diastolic pressure, an index of preload, had
no significant correlation with MMPs activation in contrast
to low myocardial perfusion pressure which substantially
contributed to left ventricular subendocardial fibrosis (Guido
et al. 2007). These findings suggested that, in addition to
volume overload, the heart has to respond to a chronic is-
chaemic process resulting in fiber loss, inflammation and
fibrosis, all occurring predominantly in the subendocardial
region of the left ventricle. Accordingly, in rats with myo-
cardial infarction, also an experimental model of volume
overload, we found myocyte necrosis, inflammatory cell
infiltration, fibroplasia and reparative fibrosis within the
subendocardial layer of the non-infarcted left ventricle (de
Carvalho Frimm et al. 2003; Koike et al. 2005). Subendo-
cardial fibrosis was significantly and independently related
to left ventricular dilatation and contributed to the develop-
ment of left ventricular dysfunction (Koike et al. 2007).
We hypothesize that the ability of cardiac adaptation to vol-
ume overload may be restricted by ischaemic myocyte losses.
This seems more likely to occur in the acute phases post-aor-
tocaval fistula when left ventricular end-diastolic pressure
increases concomitantly to systemic blood pressure decrease.
The early pathologic changes following aortocaval fistula la
have not been investigated yet. As long as our hypothesis is
correct, we anticipate the development of ischaemia, myocyte
necrosis, inflammation, MMPs activation, all predominantly
occurring in the subendocardial region of the left ventricle and
potentially contributing to cardiac dysfunction.
Objective
To investigate myocardial perfusion and cardiac structural
and functional changes during the early phases post-aorto-
caval fistula.
Methods
Male Wistar rats, weighing 300–350 g, were used. Animals
were divided into two groups undergoing either aortocaval
fistula creation or sham surgical treatment and submitted to
hemodynamic studies Morphometry was performed on 10%
formalin fixed tissue. For geometric determination of left ven-
tricular enlargement the heart was fixed under a perfusion
pressure corresponding to the in vivo systemic diastolic blood
pressure determined at sacrifice. Small samples of liver and
lung tissue were weighed before and after 48 h storage at
50 °C. The water content (%) of these tissue samples was cal-
culated as the percentage difference between wet and dry
weights of each organ and used as an estimate of heart failure.
The following experimental groups were constituted:
� Eighteen sham and 25 aortocaval fistula animals were
submitted to hemodynamic measurements at day 1;
among them, eight sham and 11 aortocaval fistula had
morphometric studies and nine sham and 14 aortocaval
fistula geometric studies.
� Ten sham and 11 aortocaval fistula animals were submit-
ted to hemodynamic measurements at day 3; among
them, five sham and 11 aortocaval fistula had morpho-
metric studies and seven sham and 11 aortocaval fistula
geometric studies
� Eighteen sham and 27 aortocaval fistula animals were
submitted to hemodynamic measurements at day 7;
among them, eight sham and 14 aortocaval fistula had
morphometric studies and eight sham and 13 aortocaval
fistula geometric studies.
� Seven sham and 11 aortocaval fistula animals were submit-
ted to measurements of myocardial blood flow at day 7.
� Four aortocaval fistula animals with coronary driving
pressure � 60 mmHg were used to measure tissue inter-
leukin levels and myeloperoxidase activity (MPO) and
compared with six non-operated control rats at days 1, 3
and 7 to avoid the inflammatory response caused by sur-
gery itself.
� Four aortocaval fistula animals with coronary driving
pressure � 60 mmHg and four aortocaval fistula animals
with coronary driving pressure >60 mmHg were submit-
ted to the measurement of MMP-2 activity at days 1, 3
and 7 and compared with a non-operated control rat
devoid of inflammation.
Ethical approval
All procedures were performed in accordance with the
norms of the Brazilian College of Animal Research. The
study protocol was approved by the ethics committee of the
Medical School, Sao Paulo University (Cappesq-HCFMUSP,
protocol number 1071/08).
Experimental model
Surgical procedures were performed using a previously
described and modified technique (Garcia & Diebold 1990).
International Journal of Experimental Pathology, 2013, 94, 178–187
Subendocardial remodeling in aortocaval fistula 179

Briefly, under anaesthesia with 10% chloral hydrate
(330 mg/kg, i.p.) (Zausinger et al. 2002) and positive
pressure ventilation (Rodent Ventilator, model 683; Har-
vard, South Natick, MA, USA), a median laparotomy was
performed, and the abdominal aorta and inferior vena cava
were identified and isolated from neighbouring structures
below the emergence of the renal arteries. Arterial and
venous blood flows were briefly interrupted with vascular
clamps to allow the insertion of an 18-G needle into the
aorta. The needle was advanced carefully, and the posterior
aortic wall was punctured three to four times aiming at the
vena cava wall. After removing the needle, homoeostasis
was conducted with local application of superglue. The
abdominal wall was closed, and the animals were returned
to their cages after full recovery. Fistula patency was
assessed daily using a paediatric stethoscope. Mortality rate
was 22% at day 1, 20% at day 3 and 24% at day 7.
Haemodynamics
Under general anaesthesia, rats underwent systemic and left
ventricular haemodynamic measurements. Briefly, a 0.5 mm
polyvinyl polychloride catheter was inserted through the
right carotid artery into the ascending aorta and advanced
into the left ventricle. Another similar catheter was inserted
into the right jugular vein and advanced to the right
atrium. Both catheters were connected to pressure transduc-
ers coupled to a calibrated preamplifier (General Purpose
Amplifier 4 model 2; Stemtech Inc., Wiscosin, USA). Pres-
sure tracings were recorded and analysed using a computer-
ized system processor (Windaq AT/Codas; Dataq
Instruments, Akron, OH, USA). Once complete stabiliza-
tion of the pressure curves was achieved, haemodynamic
measurements were taken. Computed values correspond to
the average of beat-to-beat measurements of each haemody-
namic parameter were recorded continuously over a 10-
minute period.
The following parameters were measured: systemic sys-
tolic and diastolic blood pressure (mmHg), right atrial mean
pressure (mmHg), left ventricular systolic and end-diastolic
pressure (mmHg) and maximum rates of increase and
decrease of left ventricular pressure (+dP/dt and �dP/dt,
respectively, mmHg/s). Coronary driving pressure was calcu-
lated as the difference between aortic pressure and left ven-
tricular pressure at end-diastole and used as an estimation
of myocardial perfusion pressure (Cross et al. 1961).
Morphometry
Immediately after the haemodynamic study, rats were killed
using an anaesthetic overdose, and the heart was arrested in
irreversible diastole using 100 mM/l cadmium chloride solu-
tion (Capasso et al. 1992). The heart was removed, cleansed
and relative heart weight index (g/Kg) determined. Subse-
quently, the right atrium and the left atrium were separately
dissected from the ventricles, and relative weight index (g/
Kg) of each was calculated.
Following fixation, a 1–2 mm transverse slice of the heart,
including both ventricles, was obtained at the equatorial
plane, embedded in paraffin and cut into 5-lm sections. Tis-
sue sections stained with haematoxylin and eosin, and Sirius
red underwent morphometric and geometric studies using an
image analysis system (Nikon Image System Elements AR
3.1, Japan).
The areas corresponding to the interventricular septum,
the left ventricular free wall, and the left ventricular total
cavity were determined separately using a telemacro lens
(Carl Zeiss, Vario Tessar, 2.8–5.8/5.35–21.4, Oberkochen,
Germany). The appropriateness of eccentric left ventricular
hypertrophy was calculated by the ratio between the areas
of interventricular septum plus left ventricular free wall and
the entire area of the left ventricle including walls and
chamber cavity.
Left ventricular hypertrophy was examined using haemat-
oxylin and eosin stained sections under 9 1000 magnifica-
tion. Myocyte diameter (lm) was measured around oval and
central nuclei of longitudinally displayed myocytes.
Myocyte necrosis, inflammatory cell infiltration, fibropla-
sia and left ventricular fibrosis were examined separately
taking into account two regions: the subendocardium, corre-
sponding to the inner one-third of the left ventricular wall,
and the non-subendocardium, corresponding to the remain-
ing outer two-thirds. The inner third of the left ventricle has
been previously shown to be the most susceptible myocar-
dial region to ischaemia during low perfusion events (Buck-
berg et al. 1972).
Myocyte necrosis (cells/mm2) was examined in haemat-
oxylin and eosin stained tissue sections under 9 1000 mag-
nification. Nuclear pyknosis and karyolysis as well as
cytoplasmatic changes including vacuolization, contraction
bands and hypereosinophilia were taken into account alto-
gether (Kumar et al. 2012).
Leucocyte infiltration (cells/mm2) was examined in hae-
matoxylin and eosin stained sections under 9 1000 magnifi-
cation. Inflammatory cells were identified by nuclear and
cytoplasmic typical aspects. Cells with morphological char-
acteristics of fibroblasts, cardiomyocytes, endothelial vascu-
lar cells and smooth muscle cells were excluded (Gartner &
Hiatt 2009).
Fibroplasia was examined by measuring positive alpha-
smooth muscle actin myofibroblasts (cells/mm2) detected by
immunohistochemistry under 9 1000 magnification. The tis-
sue sections were incubated with a 1:800 dilution of the
mouse antihuman alpha-smooth muscle actin antibody
(Sigma Aldrich, St. Louis, USA). Sections were then incubated
with labelled streptavidin-biotin-peroxidase kit (Dako Cyto-
mation LSAB+ System-HRP, California, USA) and diam-
inobenzidine for colour development. Finally, the sections
were faintly counterstained with haematoxylin. Vascular
smooth muscle cells with intense staining were used as posi-
tive controls. Negative controls were obtained by omitting the
primary antibody and using a non-immune bovine serum.
Collagen volume fraction (%) was determined in Sirius
red-stained tissue sections under 9 580 magnification
International Journal of Experimental Pathology, 2013, 94, 178–187
180 F. R. R. Mazzo et al.

(Junqueira et al. 1979). The collagen volume fraction was
calculated as the per cent of red-stained connective tissue
areas per total myocardium, excluding perivascular areas
(de Carvalho Frimm et al. 1997).
For myocyte necrosis and leucocyte cell infiltration, a
total amount of 15 microscopic fields were examined in
each subendocardium and non-subendocardium regions. For
collagen volume fraction, a total amount of 20 microscopic
fields were examined in each subendocardium and non-sub-
endocardium regions. For myocyte hypertrophy, a total
amount of 20 fields of the interventricular septum were
examined.
Myocardial blood flow
To estimate myocardial blood flow, the colour microsphere
method was used (Hakkinen et al. 1995; De Angelis et al.
2005). Briefly, rats were anesthetized, and the femoral and
carotid arteries were catheterized as already described. The
femoral artery catheter was advanced into the aorta and the
carotid artery catheter into the left ventricle to withdraw
blood and to administer 180 ll of 300,000 yellow micro-
spheres in suspension respectively (Dye-Trak CM; Triton
Technology, USA).
After removing the heart, the left ventricle was weighed
separately. Left ventricular subendocardial and non-suben-
docardial regions were dissected apart and, in addition to a
blood sample, were processed to calculate regional myocar-
dial blood flow.
MPO activity, Interleukin expression, and MMPs activ-
ity. After the sacrifice, the hearts were rapidly removed,
and a slice corresponding to the medium one-third of the
left ventricular myocardium was cut off at the equatorial
plane. For each analysis, tissue samples were obtained from
two distinct myocardial regions carefully trimmed away: the
inner subendocardial one-third and the outer non-subendo-
cardial left ventricular wall. All samples were snap-frozen in
liquid nitrogen.
For MPO activity, each of the two distinct left ventricular
tissue samples was homogenized on 0.5% hexadecyltrime-
thylammonium bromide in 10 mM/l 3-N-morpholinopro-
panesulphonic acid and centrifuged at 15,000 g for 40 min
(Soriano et al. 2002). An aliquot of the supernatant was
mixed with 1.6 mM/l tetramethylbenzidine and 1 mM/l
hydrogen peroxide. Activity was measured spectrophotomet-
rically as the change in absorbance at 650 nm at 37 °C,using a Spectramax microplate reader (Molecular Devices,
Sunny-vale, CA, USA). Results are expressed as mU MPO
activity/mg protein determined by the Bradford protein
assay (Bio-Rad).
For interleukin and MMPs analysis, the two distinct left
ventricular tissue samples were grounded in ice-cold RIPA
buffer (20 mM/l Tris-HCl pH 7.5, 0.5% deoxycholic acid,
0.1% SDS, 150 mM/l NaCl, 2 mM/l sodium pyrophosphate
and 20 mM/l NaF) containing 1% Triton X-100 and agi-
tated for 1 h at 4 °C. Upon completion of the extraction
incubation, samples were centrifuged (4 °C, 15 min,
10,000 g). Supernatant samples were divided in aliquots and
stored at �80 °C. Protein concentrations were determined
by the Bradford protein assay (Bio-Rad).
Tumour necrosis factor-alpha, interleukin-1beta, interleu-
kin-6 and interleukin-10 were measured in each of the two
distinct left ventricular samples by ELISA, according to the
manufacturer’s instructions (R&D Systems, Minneapolis,
MN, USA) (Deten et al. 2002).
Gelatin zymography was performed for evaluation of
MMPs activity using non-reducing, non-denaturating SDS-
PAGE. For this analysis, equal amounts of protein from
each sample were mixed with non-reducing Laemmli SDS
sample buffer and electrophorized at 20 °C in a 10% poly-
acrylamide gel containing 1 mg/ml gelatin. Later, gels were
washed for 1 h in 2% Triton X-100 to remove the SDS and
allow enzyme renaturation. Gels were then placed in enzyme
activation buffer (50 mM/l Tris-HCl, pH 7.4, 200 mM/L
NaCl, 5 mM/L CaCl2 and 0.02% NaN3; all from Sigma (St
Louis, MO, USA) for 18 h at 37 °C. Gels were then stained
with 0.1% Coomassie brilliant blue, and the activity of the
MMPs bands was quantified by densitometry (ImageQuant
LAS4000, GE Healthcare Bio-Sciences, Uppsala, Sweden).
Zymograms showed two lytic bands corresponding to gelati-
nase A (MMP-2) pro-enzyme (68 kDa) and activated
(62 kDa) forms. To normalize our results, subendocardial
and non-subendocardial left ventricular extracts from a single
non-operated rat were used. Percentage activities from left
ventricular tissue samples belonging to the same group were
averaged (Brower et al. 2002).
Statistical Analysis. Data are expressed as the mean � SD.
Normal distribution and equality of variances were tested.
Student′s t-test or Mann–Whitney rank test were used for
morphometric and hemodynamic comparisons, and one-
way repeated-measures ANOVA, complemented by Bonfer-
roni′s test, was used for myocardial blood flow, MPO, in-
terleukins and MMP-2 comparisons between groups, taking
into account subendocardial and non-subendocardial
regions.
Linear regression was used to test the potential relation-
ships between MMP-2 activity and coronary driving pres-
sure, between coronary driving pressure and myocardial
blood flow, and between myocardial blood flow and left
ventricular function. Statistical significance was established
as P < 0.05. Analyses were performed using Sigma Stat Sta-
tistical Software (version 3.1; Jandel Scientific Software, San
Rafael, CA, USA) and SAS software (Statistical Analysis
System, version 9.1; SAS Institute Inc., Cary, NC, USA).
Results
Haemodynamics
Haemodynamic results corresponding to the three follow-up
periods are depicted in Table 1. Compared with sham, aor-
tocaval fistula groups had significantly lower systemic blood
International Journal of Experimental Pathology, 2013, 94, 178–187
Subendocardial remodeling in aortocaval fistula 181

pressure and higher left ventricular end-diastolic pressure
resulting in coronary driving pressure 48% lower at day 1,
52% lower at day 3 and 56% lower at day 7. Also,
right atrial mean pressure was comparatively elevated in
aortocaval fistula groups. Left ventricular systolic dysfunc-
tion occurred at the three follow-up periods and left ventric-
ular diastolic dysfunction at days 1 and 7.
Morphometry
The results regarding the morphometric study are shown in
Table 2. Heart failure was evidenced by significantly higher
lung percentage of water content found in aortocaval fistula
rats at the three time points assessed. Heart failure was also
demonstrated to occur according to Davidoff′s criteria
(Davidoff et al. 2004). The ratio between lung and body
weight was higher (> mean + 2 SD) in aortocaval fistula
than in sham (day 1: 6.2 vs. 5.6, day 3: 6.8 vs. 5.5, and day
7: 7.3 vs. 7.1 respectively).
Left ventricular hypertrophy was evidenced by increased
myocyte diameter at days 3 and 7. The calculated ratio
between interventricular septum plus left ventricular free
wall area and total left ventricular area including the cham-
ber cavity showed that hypertrophy was inappropriate.
Myocytes with signs of necrosis were found at days 1 and
3 in the subendocardium where they outnumbered those in
the non-subendocardium by fivefold.
Leucocyte infiltration was evident throughout all acute
phases, but was more pronounced during the two earlier
periods in the subendocardial region where inflammatory
cells outnumbered those in the non-subendocardium by two-
fold (Figure 1).
Table 1 Haemodynamic measurements at days 1, 3 and 7 following aortocaval fistula
Group sham1 ACF1 sham3 ACF3 sham7 ACF7
SBP (mmHg) 116 � 6 88 � 17† 121 � 4 83 � 28† 122 � 6 96 � 21†
DBP (mmHg) 84 � 13 51 � 19* 92 � 5 46 � 21† 93 � 6 66 � 21†
CDP (mmHg) 77 � 14 37 � 18† 86 � 5 29 � 20† 86 � 6 48 � 19†
RAP (mmHg) 4.6 � 1.8 7.1 � 2.9* 5.6 � 2.3 8.8 � 2.1* 4.7 � 2.5 9.1 � 2.8*LVSP (mmHg) 122 � 15 106 � 14* 115 � 12 104 � 11 129 � 13 109 � 15*LVEDP (mmHg) 7 � 3 15 � 6† 7 � 3 18 � 3* 7 � 3 18 � 5†
+dP/dt (mmHg/s) 7898 � 4045 5828 � 2262† 5594 � 571 4553 � 983* 7924 � 2317 4564 � 2044*�dP/dt (mmHg/s) 6626 � 1717 4728 � 863† 5309 � 1325 4528 � 803 6435 � 1302 4750 � 1442*
ACF, aortocaval fistula; 1, day 1; 3, day 3; 7, day 7; SBP, systolic blood pressure; DBP, diastolic blood pressure; CDP, coronary driving pres-
sure; RAP, mean right atrial pressure; LVSP, left ventricular systolic pressure; LVEDP, left ventricular end-diastolic pressure; +dP/dt, maxi-
mum rate of increase of left ventricular pressure; �dP/dt, maximum rate of decrease of left ventricular pressure.
*P < 0.05 vs. sham (Student’s t-test).†P < 0.05 vs sham (MannWhitney test).
Table 2 Morphometric measurements at days 1, 3 and 7 following aortocaval fistula
Groups sham1 ACF1 sham3 ACF3 sham7 ACF7
Heart weight (g/Kg) 3.2 � 0.3 3.5 � 0.6 3.6 � 0.1 3.3 � 0.3 3.4 � 0.2 3.2 � 0.8Right atrium (g/Kg) 0.11 � 0.02 0.18 � 0.08* 0.11 � 0.03 0.19 � 0.09* 0.10 � 0.03 0.2 � 0.18*Left atrium (g/Kg) 0.12 � 0.02 0.12 � 0.02 0.10 � 0.02 0.12 � 0.05 0.11 � 0.03 0.13 � 0.03
Lung percentage of water content (%) 76.5 � 4.4 83.7 � 4.0* 79.0 � 2.0 82.8 � 2.0* 78.1 � 2.0 80.7 � 1.0*Liver percentage of water content (%) 75.2 � 0.1 74.7 � 2.0 73.2 � 0.5 74.0 � 3.0 73.8 � 0.4 78.3 � 1.0*IVS + LV free wall area / total LV area 0.77 � 0.04 0.71 � 0.10 0.88 � 0.02 0.71 � 0.15* 0.77 � 0.07 0.60 � 0.12*Myocyte diameter (lm) 10.0 � 0.6 11.0 � 1.4 10.0 � 0.2 14.0 � 0.1* 11.3 � 1.1 14.3 � 1.0*Myocyte necrosis (cells/mm2)SE 114 � 5† 208 � 8*† 82 � 12† 148 � 31*† 34 � 12† 42 � 9†
non-SE 27 � 3 42 � 10* 21 � 3 31 � 6* 17 � 2 21 � 4
Leucocytes (cells/mm2)
SE 48 � 5 84 � 13*† 48 � 10 117 � 13*† 33 � 5 50 � 6*†
non-SE 33 � 4 40 � 6* 41 � 6 65 � 8* 27 � 6 38 � 7*Fibroplasia (cells/mm2)
SE 10.9 � 4.0 14.6 � 5.7 10.8 � 2.6 26.1 � 10.0*† 10.9 � 2.3 47.5 � 12.0*†
non-SE 10.9 � 1.6 10.9 � 2.6 9.8 � 1.6 11.7 � 2.6 10.8 � 2.2 15.3 � 2.5CVF (%)
SE 1.2 � 0.4 1.2 � 0.2† 1.7 � 0.3 5.4 � 0.1*† 1.8 � 0.4 10.3 � 2.3*†
non-SE 1.2 � 0.2 1.7 � 0.5* 1.4 � 0.3 1.8 � 0.1* 1.7 � 0.1 2.8 � 0.7*
ACF, aortocaval fistula; 1, day 1; 3, day 3; 7, day 7; IVS, interventricular septum; LV, left ventricle; CVF, collagen volume fraction.*P < 0.05 vs. sham†P < 0.05 vs. non-SE, Repeated-Measures ANOVA complemented by Bonferroni′s test.
International Journal of Experimental Pathology, 2013, 94, 178–187
182 F. R. R. Mazzo et al.

Fibroplasia was evident during the late two periods in the
subendocardium where the number of alpha-actin-positive
myofibroblasts outnumbered those in the non-subendocardi-
um by two- to threefold.
Fibrosis deposition became evident by days 3 and 7
particularly in the subendocardium where collagen volume frac-
tion was threefold greater than in the non-subendocardium.
Myocardial blood flow
The haemodynamic changes of rats submitted to the study
of myocardial blood flow at day 7 did not differ from those
described before. Compared with sham, aortocaval fistula
showed lower myocardial blood flow, particularly within
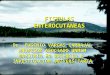
the subendocardial region (Figure 2). The relationships
examined between coronary driving pressure, blood flow
and left ventricular function are depicted in Figure 3. As
coronary driving pressure was below the lower limit of cor-
onary blood flow auto regulation in all rats examined, a
positive correlation was found between coronary driving
pressure and myocardial blood flow. Furthermore, subendo-
cardial blood flow but not non-subendocardial blood flow
was positively related to both +dP/dt and �dP/dt.
MPO and Interleukins
The coronary driving pressure of aortocaval fistula groups
submitted to the measurement of MPO and interleukins was
below the lowest limit of coronary flow auto regulation.
MPO activity was increased in all aortocaval fistula groups
regardless the left ventricular region examined; interleukin-
1beta levels were increased at day 1 in subendocardium and
non-subendocardium; Tumour necrosis factor-alpha levels
were increased at day 3 in subendocardium; and interleukin-
6 levels were increased at day 7 in subendocardium (Fig-
ure 4). Interleukin-10 did not change in either region and
was comparable between the two groups at the three differ-
ent follow-ups.
MMP-2
MMP-2 activity was measured comparing between aorto-
caval fistula groups with coronary driving pressure either
� 60 mmHg or >60 mmHg (Figure 5). MMP-2 activity of
rats with coronary driving pressure � 60 mmHg was
increased in both subendocardium and non-subendocardium
at days 1 and 7 and only in subendocardium at day 3. There
was an inverse relationship between coronary driving pres-
sure and MMPs activity measured in subendocardium at the
three time points examined.
Discussion
The present study demonstrated that during the first week
of aortocaval fistula systemic blood pressure decreases and
left ventricular end-diastolic pressure increases resulting in
markedly low coronary driving pressure and in ischaemic
remodelling of the subendocardium. The direct relationship
found between left ventricular subendocardial blood flow
and function suggests that low coronary perfusion pressure
impairs the development of appropriate left ventricular
hypertrophy. The present results are in agreement with
our previous findings showing that subendocardial fibrosis
was associated with left ventricular dysfunction in chronic
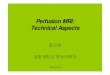
Figure 1 Photomicrographs of the subendocardial layer of the left ventricle of rats with aortocaval fistula in HE, Sirius red andsmooth muscle alpha-actin immunohistochemistry-stained tissue sections. Panels a depicts intense cytoplasmatic vacuolization ofmyocytes, as necrosis signs at day 1; in panel b, inflammatory cell infiltration stained with HE at day 3; in panel c, fibroplasiaevidenced by myofibroblasts positively marked for smooth muscle alpha-actin in brown at day 7; and in panel d, Sirius red-stainedpatch of collagen fibres indicative of fibrosis repair at day 7.
Figure 2 Myocardial blood flow of subendocardial (SE, in blackbar) and non-subendocardial (non-SE, in white bar) layers ofthe left ventricle at day 7. ACF, aortocaval fistula. Statisticalanalysis: one-way repeated-measure ANOVA complemented byBonferroni′s test; *P < 0.05 vs. SHAM SE; #P < 0.05 vs.SHAM non-SE; $P < 0.05 vs. ACF non-SE.
International Journal of Experimental Pathology, 2013, 94, 178–187
Subendocardial remodeling in aortocaval fistula 183

aortocaval fistula (Guido et al. 2007). The importance of
decreased perfusion pressure and subendocardial damage to
pathologic remodelling following experimental acute aorto-
caval fistula had not being examined before. We have
observed the development of myocyte necrosis, followed by
inflammation, fibroplasia and fibrosis, all changes found
prominently within the subendocardial region.
Markedly low coronary driving pressure resulted in a cor-
responding deprivation of myocardial perfusion. In fact, val-
ues of coronary driving pressure currently below 60 mmHg
are under the inferior limits of auto regulation of myocar-
dial blood flow (Le et al. 2004). At these levels, driving
pressure directly determines perfusion and explains the posi-
tive relationship found between coronary driving pressure
and myocardial blood flow in the present study. Interest-
ingly, subendocardial hypoperfusion was associated with left
ventricular dysfunction, implying subendocardial ischaemic
damage for the cardiac inability to adapt to acute volume
overload. Indeed, myocyte diameter was enlarged as early as
3 days following aortocaval fistula, but left ventricular wall
to total left ventricular area ratio was reduced, indicating
that the hypertrophy was inappropriate. We suggest this has
occurred as a result of subendocardial ischaemic damage.
The determinant role of local MMPs and leucocyte infil-
tration in the pathophysiological mechanism resulting in
eccentric cardiac remodelling following aortocaval fistula
has been recognized (Kolpakov et al. 2009). This exagger-
ated MMPs activation may result in pathological remodel-
ling by restricting wall thickening of enough magnitude to
counteract chamber enlargement and elevated systolic wall
stress. Accordingly, left ventricular enlargement and dys-
function may be prevented by the inhibition of MMP activ-
ity (Cox et al. 2004; Brower et al. 2007). Previously we
have demonstrated that, in contrast to left ventricular end-
diastolic pressure, low coronary driving pressure and suben-
docardial fibrosis were the only independent determinants of
left ventricular dysfunction. In the present study, we found
an inverse relationship between coronary driving pressure
and MMP-2 activation within the subendocardial region.
MMP-2 activation accompanies myocyte necrosis at day 1,
increases further in association with the inflammatory pro-
cess at day 3 and still remains elevated at day 7. These
results confirm similar findings found during the chronic
phase (Guido et al. 2007) and support the hypothesis that at
least in part, MMPs are activated in response to myocardial
ischaemia that follows the decrease in perfusion pressure.
The determinant role of ischaemia in pathological remodel-
ling may be recognised better by the observation that relat-
ing it to outstanding numbers of myocytes undergoing
necrosis in the subendocardium at day 1. As many as 10%
of myocyte fibres showed necrotic changes, corresponding to
3–4% of the total number of left ventricular myocytes.
Myocyte necrosis also occurred beyond the SE region and
was still present 3 days after aortocaval fistula surgery.
Besides myocyte necrosis, local inflammation is likely to
have contributed to left ventricular dysfunction. The associa-
tion between cytokine levels and pathologic remodelling is
well recognized (Hwang et al. 2001). Elevated tumour
necrosis factor-alpha and interleukin-1beta levels have been
related to the development of myocardial fibrosis, myocyte
hypertrophy, left ventricular enlargement, apoptosis and
cardiac dysfunction (Yndestad et al. 2006). In the present
study, increased tissue levels of tumour necrosis factor-
alpha, interleukin-6, and interleukin-1beta, leucocyte
infiltration and MPO activation occurred predominantly in
the subendocardium.
The first region of the left ventricle to undergo ischaemia
in response to low perfusion pressure is the subendocardium
where, in comparison with the mid wall, there is a paucity
of collateral vessels, the metabolic activity is enhanced, and
oxygen extraction increased (Moss 1968; Weiss & Sinha
1978). Accordingly, the subendocardium is the left ventricu-
lar region showing the greatest myocyte losses following
non-transmural infarcts and the first region affected by
ongoing ischaemia following transmural infarcts (Kuwada
& Takenaka 2000). We have demonstrated using the rat
model of experimental infarction a predominant damage to
the subendocardial non-infarcted region (Koike et al. 2007).
Furthermore, the decrease in coronary driving pressure that
followed acute infarction was the hemodynamic parameter
that best explained subsequent left ventricular enlargement
and dysfunction (de Carvalho Frimm et al. 2003; Koike
et al. 2007). As a matter of fact, in both these two experi-
mental models of acute volume overload, infarction and
(a) (b)
(c) (d)
Figure 3 The relationships found between coronary perfusionpressure and blood flow and between coronary blood flow andleft ventricular function of rats with aortocaval fistula at day 7.Graphs represent the relationships of coronary driving pressure(CDP) with subendocardial (SE) and non-subendocardial (non-SE) blood flow (panels a and b); and of SE blood flow with+dP/dt and –dP/dt (panels c and d). Statistical analysis: linearregression.
International Journal of Experimental Pathology, 2013, 94, 178–187
184 F. R. R. Mazzo et al.

aortocaval fistula, our findings indicate that cardiac dysfunc-
tion seems to result more likely from low perfusion pressure
than from increased preload. The limited ability of the myo-
cardium to adapt to acute increases in preload appears lar-
gely a consequence of ischaemic myocyte losses occurring
predominantly in the subendocardium. Remnant myocytes
increase in width but wall thickening turns out to be inap-
propriate to maintain a proportional wall to volume ratio
and to preserve left ventricular function.
The present results indicate that heart failure develops
early after experimental aortocaval fistula as a consequence
of low coronary perfusion pressure that jeopardizes suben-
docardial integrity and limits the ability of the heart to
adapt to volume overload.
Study limitations
We assessed myocyte necrosis in paraffin-embedded tissue
sections stained with haematoxylin and eosin, which may
give rise to artefacts represented mostly by contraction
bands. In fact, both aortocaval fistula and sham animals
showed histological evidence of myocardial contraction
bands. However, other parameters of myocyte necrosis such
as pyknosis, karyolysis, karyorrhexis and eosinophilic cyto-
plasm staining were also taken into account, and for that
reason, we believe that the assessment of myocyte damage
was not biased.
We found signs consistent of some degree of subendocar-
dial damage other than contraction bands in sham rats.
These changes were of little magnitude and did not result in
fibrosis deposition, meaning they have most likely occurred
during sacrifice. Potential causes include factors related to
the experimental procedure and to the anaesthesia. The
impairment of venous return and the decrease in systemic
blood pressure associated with positive pressure ventilation
might have jeopardized subendocardial perfusion to some
extent. The effects of anaesthetic drugs with different hae-
modynamic properties on myocardial perfusion have been
poorly investigated to date and deserve more attention
(Rodrigues et al. 2006).
This study lacks an appropriate estimation of the degree of
volume overload to which the animals were submitted
because the magnitude of fistula shunt was not assessed.
Fistula dimension may be estimated indirectly by pulse
pressure. In contrast to the present findings, pulse pressure
has been shown to be elevated in chronic aortocaval fistula
(Guido et al. 2007). The absence of pulse pressure elevation
in the acute phase post-aortocaval fistula is likely to be due
to the recent surgical trauma. Blood losses and fluid seques-
tration into the third space in response to surgical trauma
Figure 4 Myeloperoxidase activity (MPO) (panel a), interleukin levels (IL-1b and IL-6; panels b and d respectively) and tumournecrosis factor-alpha level (TNF-a; panel c) measured in the subendocardial (SE) and non-subendocardial (non-SE) layers of the leftventricle of rats with aortocaval fistula (ACF) and coronary driving pressure � 60 mmHg at days 1, 3 and 7. Statistical analysis:one-way repeated-measure ANOVA complemented by Bonferroni′s test; *P < 0.05 vs. control SE; †P < 0.05 vs. control non-SE.
International Journal of Experimental Pathology, 2013, 94, 178–187
Subendocardial remodeling in aortocaval fistula 185

may have impaired venous return and reduced systemic
blood pressure.
Systemic volume overload has been well recognized to
represent a hemodynamic burden to both cardiac chambers.
Unfortunately, right ventricular pressure or function were
not determined. In the absence of tricuspid valve dysfunc-
tion, however, right atrial changes indeed indicated the pres-
ence of right ventricular dysfunction. The importance of
right as opposed to left ventricular remodelling in contribut-
ing to heart failure was beyond the scope of this study.
Whether or not similar subendocardial remodelling changes
observed in the left ventricle also occurs in the right ventri-
cle has yet to be investigated.
Clinical implications
The present findings suggest that the adequacy of myocardial
perfusion, particularly to the left ventricular subendocardium,
is expected to be negatively affected by low coronary driving
pressure, which may occur especially in the setting of acute
volume overload and low systemic blood pressure.
Conclusion
Subendocardial ischaemic remodelling in response to low
coronary driving pressure may result in left ventricular dys-
function during the acute phases of aortocaval fistula.
Conflict of interest
There are no conflicts of interest.
Funding source
This work was supported by Fundacao Faculdade de Medi-
cina, University of Sao Paulo, and Conselho Nacional de
Desenvolvimento Cientıfico e Tecnologico (CNPq), Brazil.
References
Brilla C.G., Rupp H., Maisch B. (2003) Effects of ACE inhibition
versus non-ACE inhibitor antihypertensive treatment on myocar-
dial fibrosis in patients with arterial hypertension. Hertz 28, 744–753.
Brower G.L. & Janicki J.S. (2001) Contribution of ventricular
remodeling to pathogenesis of heart failure in rats. Am. J. physiol.
Heart Circ. Physiol. 280, H674–H683.
Brower G.L., Chancey A.L., Thanigaraj S., Matsubara B.B., Janicki
J.S. (2002) Cause and effect relationship between myocardial
mast cell number and matrix metalloproteinase activity. Am. J.
Physiol. Heart Circ. Physiol. 283, H518–H525.
Brower G.L., Levick S.P., Janicki J.S. (2007) Inhibition of matrix
metalloproteinase activity by ACE inhibitors prevents left ventric-
ular remodeling in a rat model of heart failure. Am. J. Physiol.
Heart. Circ. Physiol. 292, H3057–H3064.
(a) (b) (c)
(d) (e) (f)
Figure 5 In the upper panels are represented MMP-2 activity measured in the subendocardial (SE) layer and in the non-subendocardial (non-SE) layer of the left ventricle of rats with aortocaval fistula accordingly to coronary driving pressure (CDP) atdays 1, 3 and 7 (panels a, b, and c). In the bottom panels are represented the graphs of the relationships found between CDP andMMP-2 activity in the SE layer at days 1, 3 and 7 (panels d, e and f). Statistical analysis: from a to c, one-way repeated-measureANOVA complemented by Bonferroni′s test. From d to j, Linear regression analysis; †P < 0.05 vs. >60 mmHg SE; #P < 0.05 vs.>60 mmHg non-SE; *P < 0.05 vs. � 60 mmHg non-SE.
International Journal of Experimental Pathology, 2013, 94, 178–187
186 F. R. R. Mazzo et al.

Buckberg G.D., Fixler D.E., Archie J.P., Hoffman J.I.E. (1972)
Experimental subendocardial ischemia in dogs with normal coro-
nary arteries. Circ. Res. 30, 67–81.Capasso J.M., Li P., Zhang X., Anversa R. (1992) Heterogeneity of
ventricular remodeling after acute myocardial infarction in rats.
Am. J. Physiol. 262, H486–H495.
de Carvalho Frimm C., Sun Y., Weber K.T. (1997) Angiotensin II
receptor blockade and myocardial fibrosis of the infarcted rat
heart. J. Lab. Clin. Med. 129, 439–446.de Carvalho Frimm C., Koike M.K., C�uri M. (2003) Subendocardial
fibrosis in remote myocardium results from reduction of coronary
driving pressure during acute infarction in rats. Arq. Bras. Car-
diol. 8, 509–514.Cohn J.N., Ferrari R., Sharpe N. (2000) Cardiac remodeling - con-
cepts and clinical implications: a consensus paper from an interna-
tional forum on cardiac remodeling Behalf of an International
Forum on Cardiac Remodeling. J. Am. Coll. Cardiol. 35, 569–582.Cox M.J., Sood H.S., Hunt M.J. et al. (2002) Apoptosis in the left
ventricle of chronic volume overload causes endocardial endothe-
lial dysfunction in rats. Am. J. Physiol. Heart. Circ. Physiol. 282,
H1197–H1205.
Cox M.J., Hawkins U.A., Hoit B.D., Tyagi S.C. (2004) Attenuation
of oxidative stress and remodeling by cardiac inhibitor of metallo-
proteinase protein transfer. Circulation 109, 2123–2128.
Cross C.E., Rieben P.A., Salisbury P.F. (1961) Coronary driving
pressure and vasomotor tonus as determinants of coronary blood
flow. Circ. Res. 9, 589–600.
Davidoff A.W., Boyden P.A., Schwartz K. et al. (2004) Congestive
heart failure after myocardial infarction in the rat: cardiac force
and spontaneous sarcomere activity. Ann. NY. Acad. Sci. 1015,
84–95.
De Angelis K., Gama V.M., Farah V.A., Irigoyen M.C. (2005)
Blood flow measurements in rats using four color microspheres
during blockade of different vasopressor systems. Braz. J. Med.
Biol. Res. 38, 119–125.
Deten A., Volz H.C., Briest W., Zimmer H.G. (2002) Cardiac cytokine
expression is upregulated in the acute phase after myocardial infarc-
tion Experimental studies in rats. Cardiovasc. Res. 55, 329–340.Dolgilevich S.M., Siri F.M., Atlas S.A., Eng C. (2001) Changes in
collagenase and collagen gene expression after induction of aorto-
caval fistula in rats. Am. J. Physiol. Heart. Circ. Physiol. 281,
H207–H214.
Fedak P.W.M., Verma S., Weisel R.D., Li R. (2005) Cardiac remod-
eling and failure: from molecules to man (part I). Cardiovasc.
Pathol. 14, 1–11.
Garcia R. & Diebold S. (1990) Simple rapid and effective method
of producing aortocaval shunts in the rat. Cardiovasc. Res. 24,
430–432.Gartner L.P. & Hiatt J.L. (2009) Color atlas of histology. 5th edn.
Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins.
pp. 105–108.
Grossman W., Jones D., McLaurin L.P. (1975) Wall stress and pat-
terns of hypertrophy. J. Clin. Invest. 56, 56–64.
Guido M.C., de Carvalho Frimm C., Koike M.K., Cordeiro F.F.,
Moretti A.I.S., Godoy L.C. (2007) Low coronary driving pressure
is associated with subendocardial remodeling and left ventricular
dysfunction in aortocaval fistula. Clin. Exp. Pharmacol. Physiol.
34, 1165–1172.
Hakkinen J.P., Miller M.W., Smith A.H., Knight D.R. (1995) Mea-
surement of organ blood flow with colored microspheres in the
rat. Cardiovasc. Res. 29, 74–79.Hwang M.W., Matsumori A., Furukawa Y. et al. (2001) Neutral-
ization of interleukin-1beta in the acute phase of myocardial
infarction promotes the progression of left ventricular remodeling.
J. Am. Coll. Cardiol. 38, 1546–1553.Junqueira L.C., Bignolas G., Brentani R.R. (1979) Picrosirius stain-
ing plus polarization microscopy, a specific method for collagen
detection in tissue sections. Histochem. J. 11, 447–455.
Koike M.K., de Carvalho Fimm C., Higuchi M.L. (2005) Bradyki-
nin B2 receptor antagonism attenuates inflammation, mast cell
infiltration and fibrosis in remote myocardium after infarctions in
rats. Clin. Exp. Pharmacol. Physiol. 32, 1131–1136.
Koike M.K., de Carvalho Frimm C., C�uri M. (2007) Low cororary
pressure early in the course of myocardial infarction is associated
with subendocardial remodeling and left ventricular dysfunction.
Int. J. Exp. Pathol. 88, 279–290.
Kolpakov M.A., Seqqat R., Rafiq K. et al. (2009) Pleiotropic effects
of neutrophils on myocyte apoptosis and left ventricular remodeling
during early volume overload. J. Mol. Cell. Cardiol. 47, 634–645.Kumar V., Abbas A.K., Aster J.C. (2012) Robbins Basic Pathology.
9th edn. Philadelphia, PA: Elsevier Saunders. pp. 8–11.Kuwada Y. & Takenaka K. (2000) Transmural heterogeneity of the
left ventricular wall: subendocardial layer and subepicardial layer.
J. Cardiol. 35, 205–218.
Le D.E., Jayaweera A.R., Wei K., Coggins M.P., Lindner J.R., Kaul
S. (2004) Changes in myocardial blood volume over a wide range
of coronary driving pressures: role of capillaries beyond the aut-
oregulatory range. Heart 90, 1199–1205.Moss A.J. (1968) Intramyocardial oxygen tension. Cardiovasc. Res.
2, 314–318.Olivetti G., Cigola E., Maestri R., Lagrasta C., Corradi D., Quani
F. (2000) Recent advances in cardiac hypertrophy. Cardiovasc.
Res. 45, 68–75.
Rodrigues S.F.P., Martins J.O., Sannomiya P., Nigro D., Carvalho
M.H., Fortes Z.B. (2006) Differential effects of chloral hydrate-
and ketamine-induced anesthesia by the s.c. route. Life Sci. 79,
1630–1637.
Soriano F.G., Liaudet L., Szab�o E. et al. (2002) Resistance to acute
septic peritonitis in poly (ADP-ribose) polymerase-1-deficient
mice. Shock 17, 286–292.Weber K.T. (2004) From Inflammation to Fibrosis: A Stiff Stretch
of Highway. Hypertension 43, 716–719.Weber K.T. & Brilla C.G. (1991) Pathological hypertrophy and car-
diac interstitium fibrosis and renin-angiotensin-aldosterone sys-
tem. Circulation 83, 1849–1865.
Weiss H.R. & Sinha A.K. (1978) Regional oxygen saturation of
small arteries and veins in the canine myocardium. Circ. Res. 42,
119–126.Yndestad A., Damas J.K., Oie E., Ueland T., Gullestad L., Aukrust
P. (2006) Systemic inflammation in heart failure – the whys and
wherefores. Heart Fail. Rev. 11, 83–92.
Zausinger S., Baethmann A., Schmid-Elsaesser R. (2002) Anesthetic
methods in rats determine outcome after experimental focal cere-
bral ischemia: mechanical ventilation is required to obtain con-
trolled experimental conditions. Brain Res. 9, 112–121.
International Journal of Experimental Pathology, 2013, 94, 178–187
Subendocardial remodeling in aortocaval fistula 187