Embed Size (px)
Citation preview


2
Banff デ᩿䛻ᇶ䛵䛔䛯⌮ุᐃ
䠍 B ff l f h &䠍. Banff classification history & topics2. Banff classification WG issues
BK virus nephropathy3. non-rejection findings
medullary ray injury (MRI)
短期のTCMRは免疫抑制剤の進歩により10-20%台に短期・長期のAMRが問題として残されている
移植腎長期生着率と免疫抑制薬の進歩䝗䝘䞊ᢠయ᳨ฟἲLCT, Flow –PRA, LABscreen PRA
DSA detecting
ction / graft survival (%)
45%
96%80%
アザチオプリンATG
シクロスポリン
MMFダクリズマブ
タクロリムス
エベロリムス
急性拒絶反応1年 graft survival
80
100
60
40
移植年1960
0
Acute reje
Radiation prednisone 6-メルカプトプリン 11%
バシリキシマブ20
2005 1965 1970 1975 1980 1985 1990 1995 2000 2010Björn Nashan, CAST(アジア移植学会)2011より引用
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」

3
Major Banff classification change
1. clinical definition 䊻 immunological definition;91’䊻97’
2. C4d on PTC; 01’DSA is necessary on diagnosis.
3. CAN 䊻 CSAN 䊻 IF/TA91’䊻 97’ 䊻 05’
4. chronic antibody mediated rejection; 05’4. chronic antibody mediated rejection; 05chronic T cell mediated rejection
5. isolated v lesion certainly exists.; 07’-13’
C4d negative AMR certainly exists.
Banff code
2013
ti code
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」
4
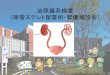
䠄⮫ᗋⓗ䠅ᣄ⤯ᛂ䛾ศ㢮
≉㞟䠖⭈⛣᳜ Banff ศ㢮䛾ኚ㑄䛸᭱᪂䛾ヰ㢟Ṋ ⏣ ᮅ ⨾ ୧ ゅ ᅧ ⏨᪥⭈ㄅ 2013䠗55䠄2䠅䠖98䠉101.᪥⭈ㄅ 2013䠗55䠄2䠅䠖98 101.
DSA or non-DSADSA or non-DSA
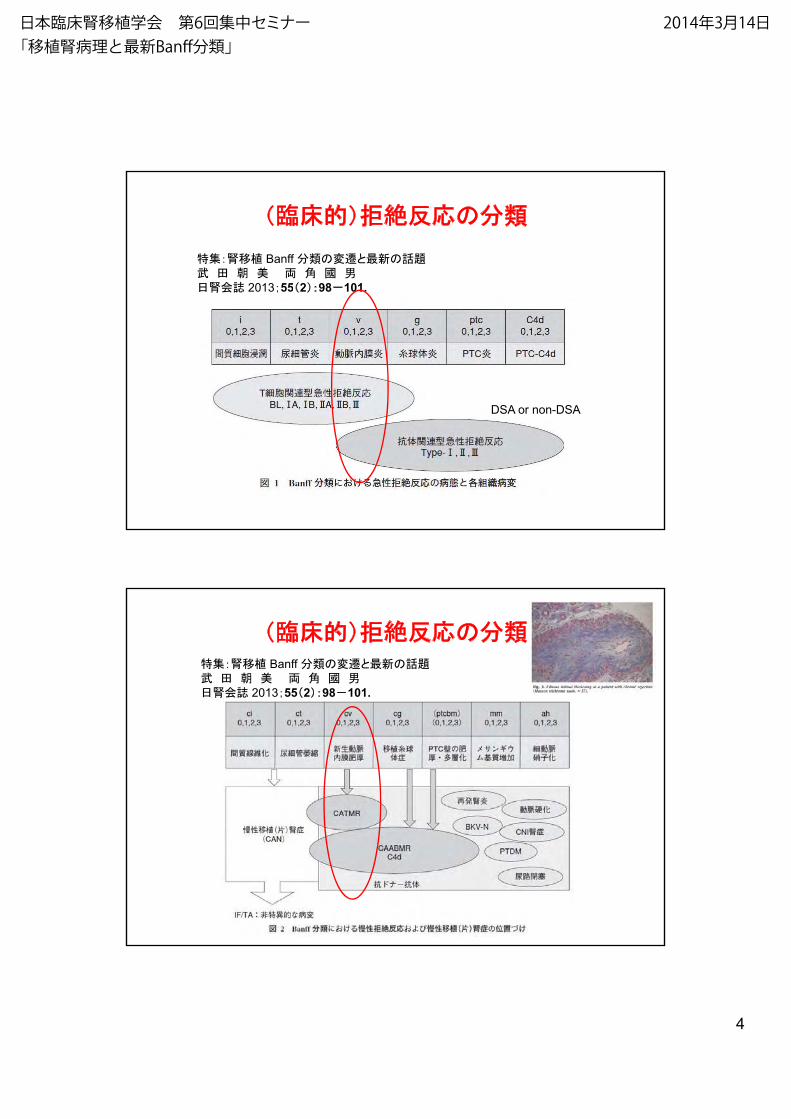
䠄⮫ᗋⓗ䠅ᣄ⤯ᛂ䛾ศ㢮≉㞟䠖⭈⛣᳜ Banff ศ㢮䛾ኚ㑄䛸᭱᪂䛾ヰ㢟Ṋ ⏣ ᮅ ⨾ ୧ ゅ ᅧ ⏨᪥⭈ㄅ 2013䠗55䠄2䠅䠖98䠉101.
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」
5
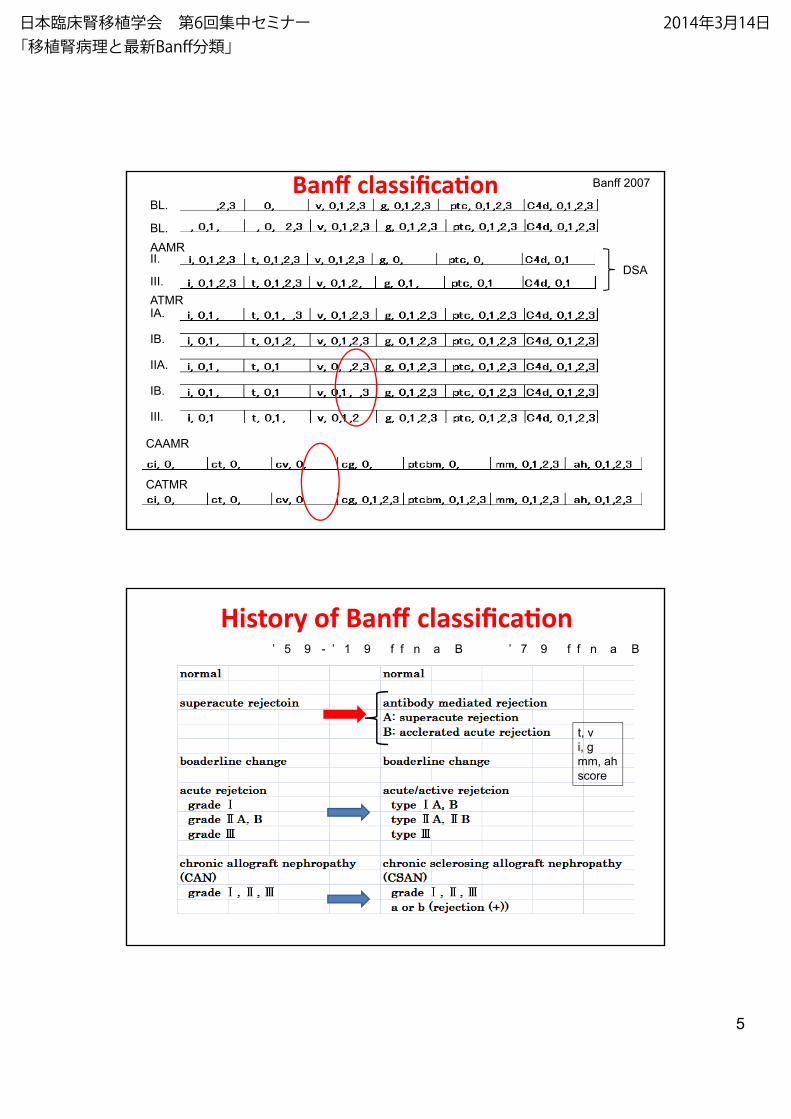
Banī ĐůĂƐƐŝĮcaBL.
BL.
AAMR
II.
III.
Banff 2007
DSA
IA.
IB.
IIA.
IB.
ATMR
III.
CAAMR
CATMR
History of Banī classiĮca
’ 7 9 f f n a B’ 5 9 - ’ 1 9 f f n a B
t, v
i, g
mm, ah
score
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」
6
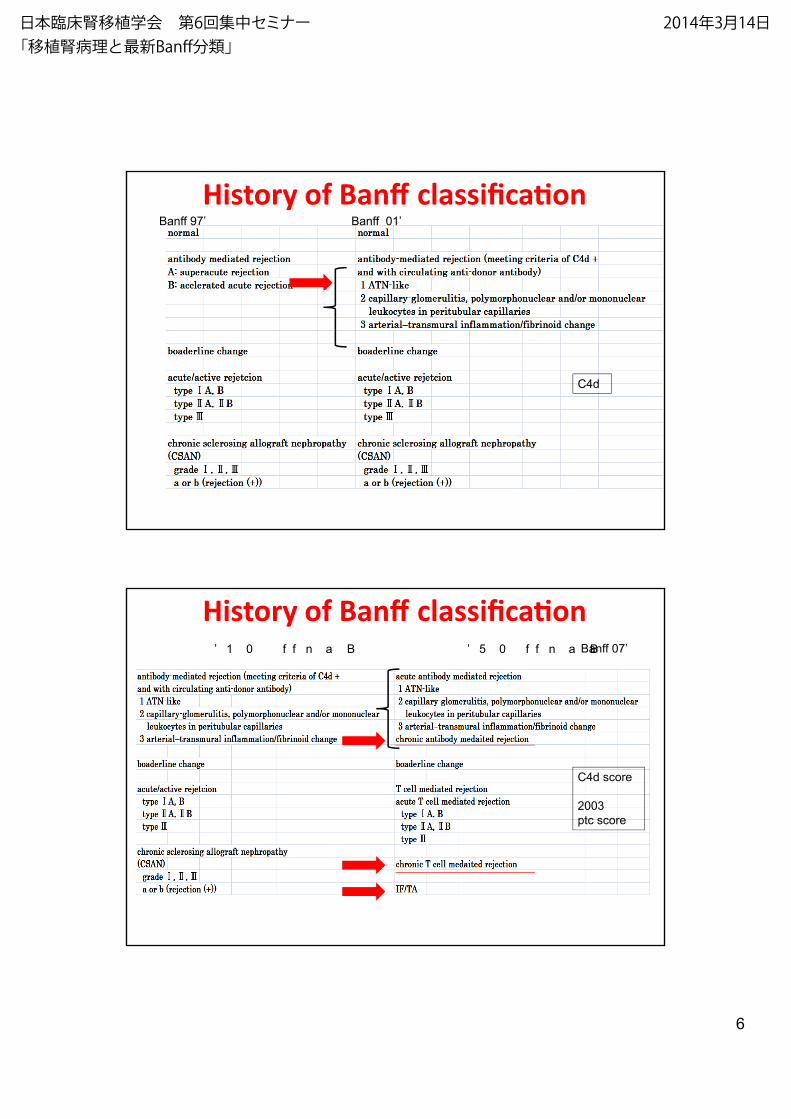
History of Banī ĐůĂƐƐŝĮcaBanff 01’Banff 97’
C4d
History of Banī ĐůĂƐƐŝĮca
’ 5 0 f f n a B’ 1 0 f f n a B Banff 07’
C4d score
2003
ptc score
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」
7
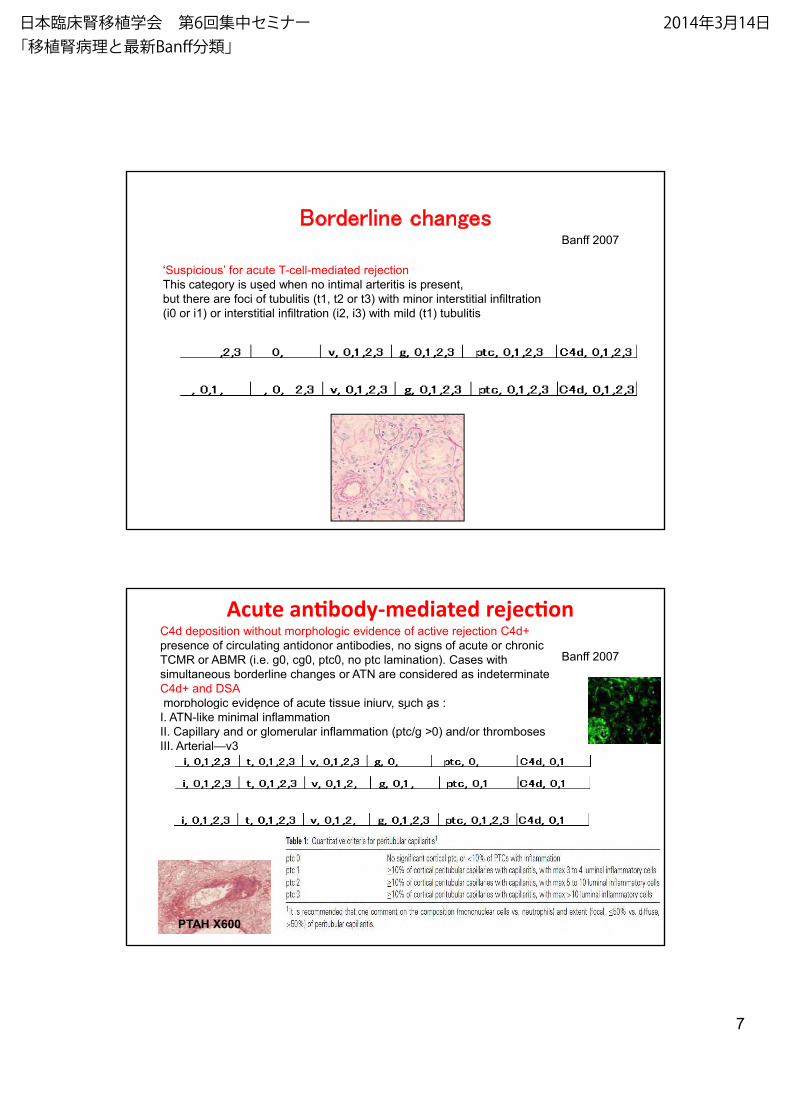
Borderline changes
‘Suspicious’ for acute T-cell-mediated rejection
This category is used when no intimal arteritis is present,
Banff 2007
py g
but there are foci of tubulitis (t1, t2 or t3) with minor interstitial infiltration
(i0 or i1) or interstitial infiltration (i2, i3) with mild (t1) tubulitis
Acute an -mediated rejec
Banff 2007
C4d deposition without morphologic evidence of active rejection C4d+
presence of circulating antidonor antibodies, no signs of acute or chronic
TCMR or ABMR (i.e. g0, cg0, ptc0, no ptc lamination). Cases with
simultaneous borderline changes or ATN are considered as indeterminate
C4d+ and DSA
morphologic evidence of acute tissue injury, such as :, y jg p
I. ATN-like minimal inflammation
II. Capillary and or glomerular inflammation (ptc/g >0) and/or thromboses
III. Arterial—v3
PTAH X600
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」
8
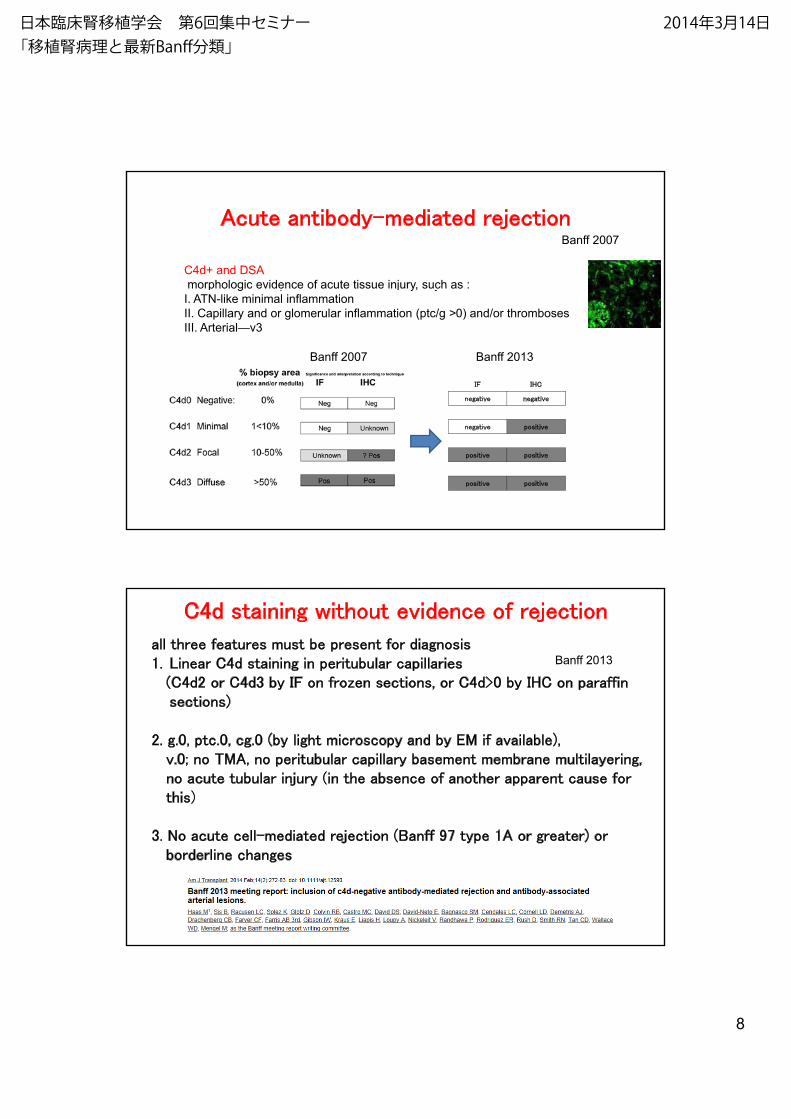
Acute antibody-mediated rejectionBanff 2007
C4d+ and DSA
morphologic evidence of acute tissue injury, such as :y jg p
I. ATN-like minimal inflammation
II. Capillary and or glomerular inflammation (ptc/g >0) and/or thromboses
III. Arterial—v3
IF IHC
negative negative
Banff 2007 Banff 2013
negative positive
positive positive
positive positive
C4d staining without evidence of rejection
all three features must be present for diagnosis1. Linear C4d staining in peritubular capillaries
(C4d2 or C4d3 by IF on frozen sections, or C4d>0 by IHC on paraffin sections)
Banff 2013
)
2. g.0, ptc.0, cg.0 (by light microscopy and by EM if available), v.0; no TMA, no peritubular capillary basement membrane multilayering, no acute tubular injury (in the absence of another apparent cause for this)
3. No acute cell-mediated rejection (Banff 97 type 1A or greater) or borderline changes
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」

9
Acute antibody-mediated rejection
Banff 2007C4d+ and DSA
morphologic evidence of acute tissue injury, such as :
I. ATN-like minimal inflammation
II Capillary and or glomerular inflammation (ptc/g >0) and/or thrombosesII. Capillary and or glomerular inflammation (ptc/g >0) and/or thromboses
III. Arterial—v3
Banff 2013
g1 = 1 loop ௨ୖEM 䛷䜒OK
cg0 –
no GBM double contours by LM or EM
cg1a – no GBM double contours by LM bu
t t l t th CL b EM ith i t d
cg
tat least three CL by EM with associated
endothelial swelling and/or subendothelial
electron- lucent widening
cg1b – one or more GBM double contours
in 1 nonsclerotic glomerulus by LM
EM con¿rmation is recommended if EM is
available.
all three features must be present for diagnosis1. Histologic evidence of acute tissue injury, including one or more of the following:
Microvascular inflammation (g>03 and/or ptc>0)Intimal or transmural arteritis (v>0)
Acute/active ABMR Banff 2013
Intimal or transmural arteritis (v>0)Acute thrombotic microangiopathy, in the absence of any other cause acute tubular injury, in the absence of any other apparent cause
2. Evidence of current/recent antibody interaction with vascular endothelium, including at least one of the following:Linear C4d staining in peritubular capillaries (C4d2 or C4d3 by IF on frozen
sections, or C4d>0 by IHC on paraffin sections), y p )At least moderate microvascular inflammation (g+ptc>2)Increased expression of gene transcripts in the biopsy tissue indicative of endothelial injury, if thoroughly validated
3. Serologic evidence of donor-specific antibodies (DSAs) (HLA or other antigens)
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」

10
Chronic active antibody-mediated rejectionBanff 2007
C4d+ and DSAC4d+ and DSA
morphologic evidence of chronic tissue injury, such as glomerular double contours and/or
peritubular capillary basement membrane multilayering and/or
interstitial fibrosis/tubular atrophy and/or
fibrous intimal thickening in arteries cg1a: LM (-), EM (+) loop>0
cg1b: LM (+) loop>0
all three features must be present for diagnosis1. Morphologic evidence of chronic tissue injury, including one or more of the
following:T l t l l th (TG) ( 0) if id f h i
Chronic, active ABMR Banff 2013
Transplant glomerulopathy (TG) (cg>0), if no evidence of chronicthrombotic microangiopathySevere peritubular capillary basement membrane multilayering (requires EM)Arterial intimal fibrosis of new onset, excluding other causes
2. Evidence of current/recent antibody interaction with vascular endothelium, including at least one of the following:Linear C4d staining in peritubular capillaries (C4d2 or C4d3 by IF on frozenLinear C4d staining in peritubular capillaries (C4d2 or C4d3 by IF on frozensections, or C4d>0 by IHC on paraffin sections)At least moderate microvascular inflammation (g+ptc>2)Increased expression of gene transcripts in the biopsy tissue indicative of endothelial injury, if thoroughly validated
3. Serologic evidence of DSAs (HLA or other antigens)
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」

11
Acute T-cell-mediated rejectionBanff 2007
IA. Cases with significant interstitial infiltration (>25% of parenchyma affected, i2 or i3)
and foci of moderate tubulitis (t2)
IB. Cases with significant interstitial infiltration (>25% of parenchyma affected, i2 or i3)
and foci of severe tubulitis (t3)
IIA. Cases with mild-to-moderate intimal arteritis (v1)
IIB. Cases with severe intimal arteritis comprising >25% of the luminal area (v2)
III. Cases with ‘transmural’ arteritis and/or arterial fibrinoid change and necrosis of medial
smooth muscle cells with accompanying lymphocytic inflammation (v3)
IA.
IBIB.
IIA.
IB.
III.
Chronic active T-cell-mediated rejectionBanff 2007
‘chronic allograft arteriopathy’
arterial intimal fibrosis with mononuclear cell infiltration in fibrosis formation ofarterial intimal fibrosis with mononuclear cell infiltration in fibrosis, formation of
neo-intima
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」
12
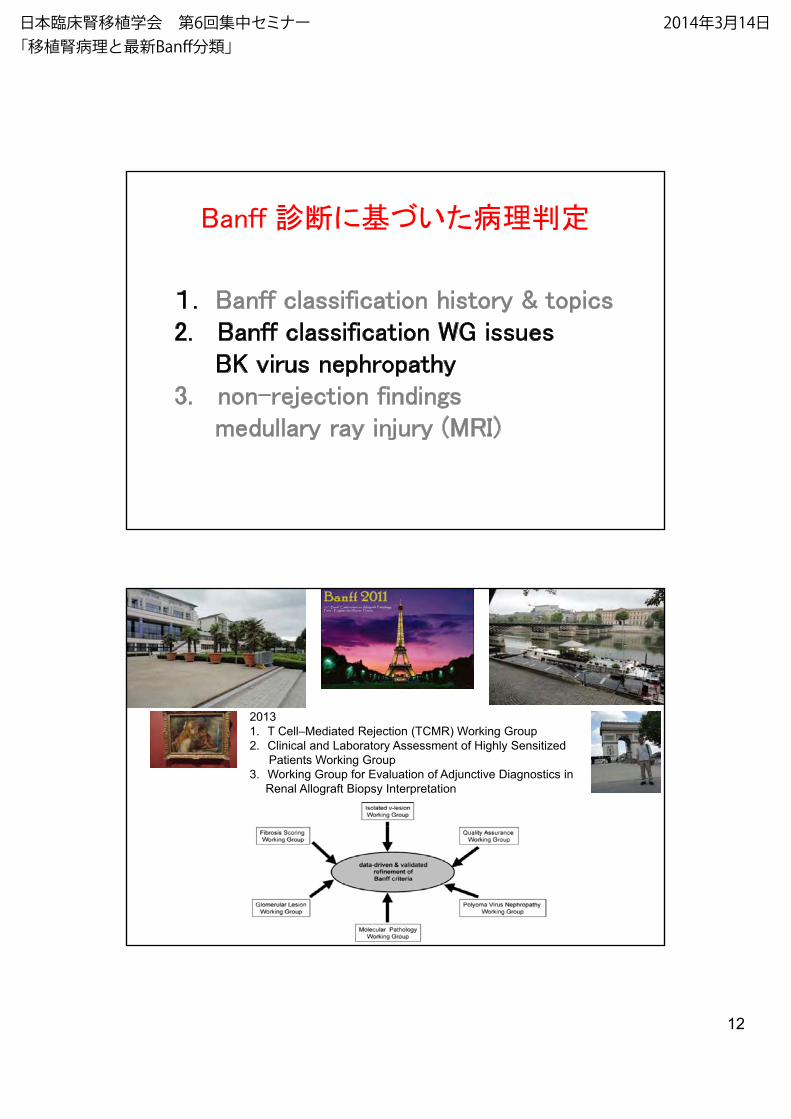
Banff デ᩿䛻ᇶ䛵䛔䛯⌮ุᐃ
䠍 B ff l f h &䠍. Banff classification history & topics2. Banff classification WG issues
BK virus nephropathy3. non-rejection findings
medullary ray injury (MRI)
2013
1. T Cell–Mediated Rejection (TCMR) Working Group
2. Clinical and Laboratory Assessment of Highly Sensitized
Patients Working Group
3. Working Group for Evaluation of Adjunctive Diagnostics in
Renal Allograft Biopsy Interpretation
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」

13
BK virus nephropathy
Progressing report of the working group on the classification of polyomavirus nephropathy (PVN)
2011 report
Pathological stages of PVNPathological stages of PVN
Stage A medulla/cortex
Stage B medulla/cortex
Stage C medulla/cortexStage C medulla/cortex
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」

14
Stage A
varying degree of viral replication with intranuclear inclusion bodies and/or positive immunohistochemistry (SV-40 T antigen) and/or in-situ hybridization signals.No or minimal tubular epithelial cell lysis / cell necrosisNo or minimal denudation of tubular basement membrane caused by viral epithelial lysislysis.
Interstitial fibrosis < 50% of renal cortex (Banff chronicity score ci2)
Medulla changes limited to medullaCortex changes seen in cortex +/- medulla
Drachenberg CB, Hum Pathol. 2005 Dec;36(12):1245-55
Stage B
Marked virally induced tubular epithelial cell injury/necrosis/cell lysis with frank denudation of associated tubular basement membrane.
Stage C
Viral replication in cortex and/or medulla (minimal to marked)Interstitial fibrosis > 50% of cortex (Banff chronicity score=ci3)
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」

15
6S-Cr
S Cr change
Progressing report of the working group on the classification of polyomavirus nephropathy (PVN)
2011 report
2
3
4
5
stage A
stage B
stage C
S-Cr change
0
1stage C
weeks
100
%
*
Gra failure /all causes
Progressing report of the working group on the classification of polyomavirus nephropathy (PVN)
2011 report
20
40
60
80
100
all cases
cases without
rej on
0
20
PVN stage A PVN srage B PVN stage C
gra failure
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」

16
Progressing report of the working group on the classification of polyomavirus nephropathy (PVN)
2011 report
Polyomavirus nephropathy all repeated biopsy
repeat biopsy n=22 regression 27%stable 43%
i 30%progression 30%
Ěŝīeren diagnosis between
PVN and acute r
PVN ARlocation : medulla cortexC4d: on TBM on PTCInfilt. cell plasma lymphocytenucleus change (+) (-)nucleus change (+) (-)SV-40 (+) (-)
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」


18
medullary ray injury (MRI)ᩥ⊩㈨ᩱ
The etiology of MRI n=36CNI toxicity (44.4%)chronic obstruction (36 1%)chronic obstruction (36.1%)acute or chronic pyelonephritis (5.6%)and others (13.9%)
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」
19
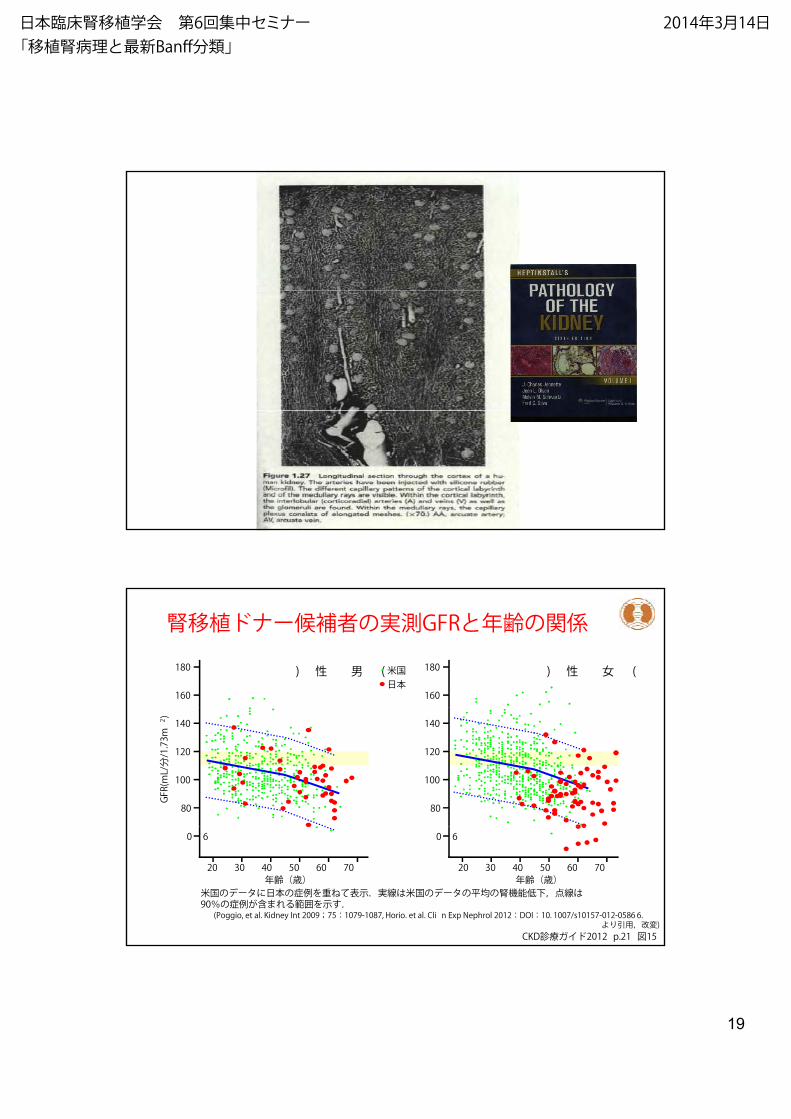
腎移植ドナー候補者の実測GFRと年齢の関係180
160
180
160
) 性 女 () 性 男 (米国日本
140
120
100
80
140
120
100
80
GFR(mL/分/1.73m
2 )
(Poggio, et al. Kidney Int 2009;75:1079-1087, Horio. et al. Cli n Exp Nephrol 2012:DOI:10. 1007/s10157-012-0586 6. より引用,改変)
米国のデータに日本の症例を重ねて表示.実線は米国のデータの平均の腎機能低下,点線は90%の症例が含まれる範囲を示す.
0 60 6
20 30 40 50 60 70年齢(歳)
20 30 40 50 60 70年齢(歳)
CKD診療ガイド2012 p.21 図15
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」
20
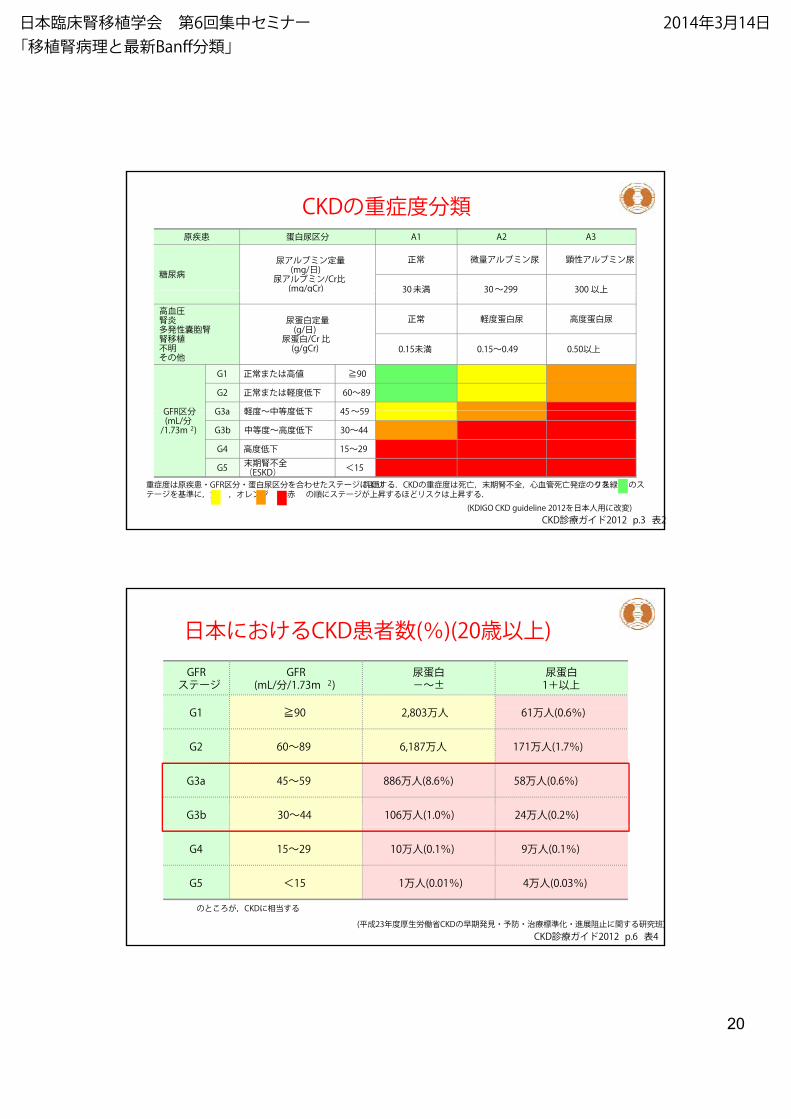
CKDの重症度分類原疾患 蛋白尿区分 A1 A2 A3
糖尿病尿アルブミン定量(mg/日)
尿アルブミン/Cr比(mg/gCr)
正常 微量アルブミン尿 顕性アルブミン尿
30未満 30~299 300 以上(mg/gCr) 30未満 30~299 300 以上
高血圧腎炎多発性囊胞腎腎移植不明その他
尿蛋白定量(g/日)
尿蛋白/Cr 比(g/gCr)
正常 軽度蛋白尿 高度蛋白尿
0.15未満 0.15~0.49 0.50以上
GFR区分
G1 正常または高値 ≧90G2 正常または軽度低下 60~89G3a 軽度~中等度低下 45~59GFR区分
(mL/分/1.73m 2)
G3a 軽度~中等度低下 45~59G3b 中等度~高度低下 30~44G4 高度低下 15~29G5 末期腎不全
(ESKD) <15スリの症発亡死管血心,全不腎期末,亡死は度症重のDKC.るす価評 りよにジーテスたせわ合を分区尿白蛋・分区RFG・患疾原は度症重 クを緑 のス
テージを基準に,黄 ,オレンジ ,赤 の順にステージが上昇するほどリスクは上昇する.(KDIGO CKD guideline 2012を日本人用に改変)
CKD診療ガイド2012 p.3 表2
日本におけるCKD患者数(%)(20歳以上)GFRステージ
GFR(mL/分/1.73m 2)
尿蛋白-~±
尿蛋白1+以上
G1 ≧90 2,803万人 61万人(0.6%)
G2 60~89 6,187万人 171万人(1.7%)
G3a 45~59 886万人(8.6%) 58万人(0.6%)
G3b 30~44 106万人(1.0%) 24万人(0.2%)
G4 15~29 10万人(0.1%) 9万人(0.1%)
G5 <15 1万人(0.01%) 4万人(0.03%)
(平成23年度厚生労働省CKDの早期発見・予防・治療標準化・進展阻止に関する研究班)のところが,CKDに相当する
CKD診療ガイド2012 p.6 表4
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」

21
¾ฟ⭈ᶆᮏ◊✲
Labyrinth
Labyrinth
37ṓ37ṓ
MRMR MR
MR
MIMR
37ṓ 37ṓ
MR
MR
MR
MR
MR MR
¾ฟ⭈ᶆᮏ◊✲
60ṓ46ṓ
72ṓ 75ṓ
MR
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」

22
¾ฟ⭈ᶆᮏ◊✲
Labyrinth72ṓ
MR
Labyrinth
MR
Labyrinth
¾ฟ⭈ᶆᮏ◊✲
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」
23
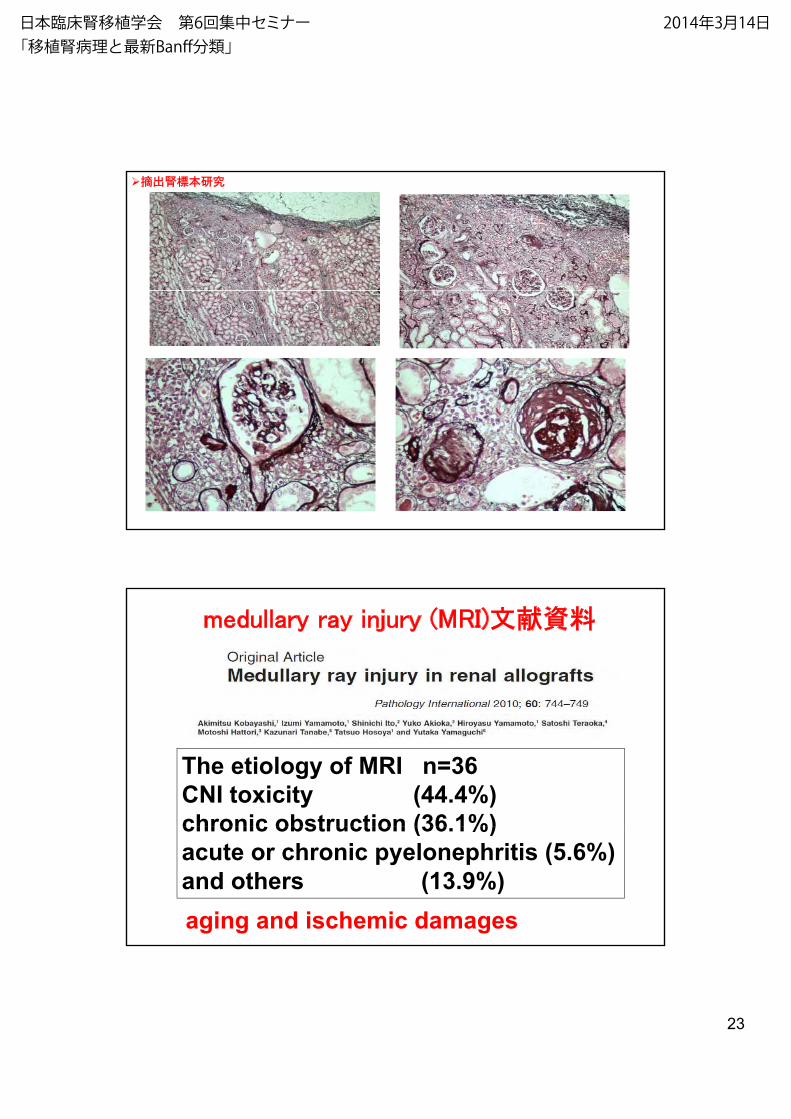
¾ฟ⭈ᶆᮏ◊✲
medullary ray injury (MRI)ᩥ⊩㈨ᩱ
The etiology of MRI n=36CNI toxicity (44.4%)chronic obstruction (36 1%)chronic obstruction (36.1%)acute or chronic pyelonephritis (5.6%)and others (13.9%)aging and ischemic damages
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」


25
᪥ᮏ⮫ᗋ⭈⛣᳜Ꮫ 2014
COI 㛤♧COI 㛤♧➹㢌Ⓨ⾲⪅ྡ䠖す ៅ୍
₇㢟Ⓨ⾲䛻㛵䛧䚸㛤♧䛩䜉䛝COI㛵ಀ䛻䛒䜛ᴗ䛿䛒䜚䜎䛫䜣䚹
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「移植腎病理と最新Banff分類」