Embed Size (px)
Citation preview
The Heart of the Matter: Anesthesia for Patients with
Cardiac Disease
Molly Shepard DVM Dipl. ACVA
Continuing Education Seminar
Cobb Emergency Veterinary Clinic
October 3rd, 2012
Overview
• Cardiac function review
• Cardiovascular effects of anesthetic drugs
• Cardiac diseases
– General anesthetic considerations
– Case examples
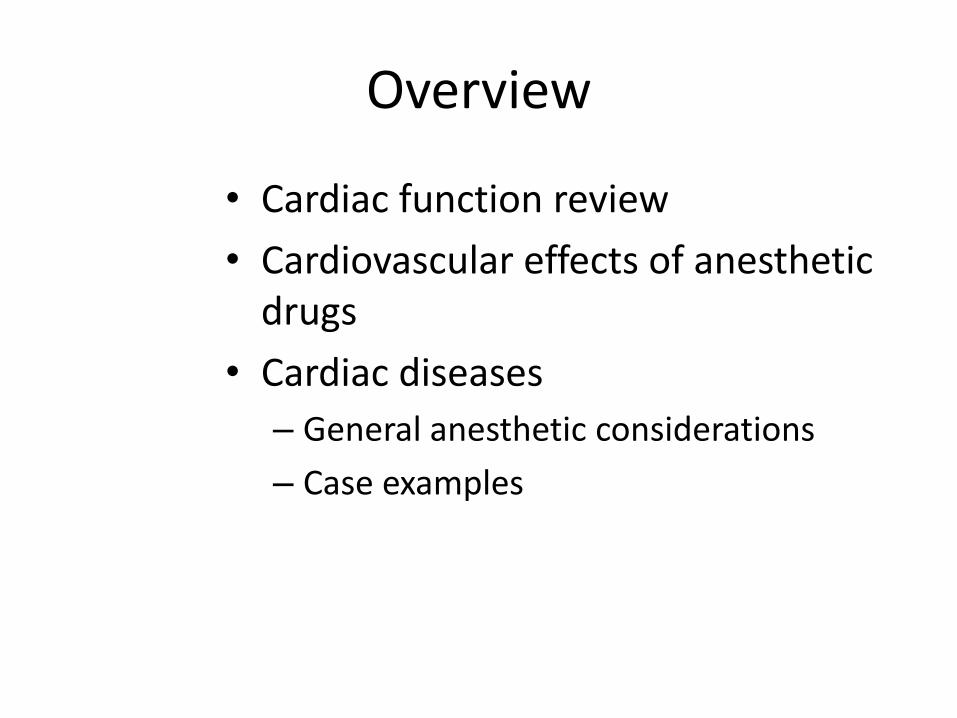
Normal cardiac function
• It all starts with an action potential • Pacemaker cells
http://php.med.unsw.edu.au/embryolo
gy/index.php?title=Advanced_-
_Cardiac_Conduction
SA node 70-160 bpm
AV node/ His Bundle region
40-60 bpm
Bundle branches/
Purkinje network
20-40 bpm

Action potential – pacemaker cell
Craven 2006

Variable cardiac action potentials
http://healthyheart-sundar.blogspot.com/2011/03/cardiac-action-potential.html

Action potentials and ECG
http://www.pharmacolog
y2000.com/Cardio/antiar
r/antiarrtable.htm
Ventricular
muscle
Purkinje fibers
AV node
SA node

Atrial depolarization
http://www.sciencephoto.co
m/media/304266/view

AV node conduction
http://www.sciencephoto.co
m/media/304266/view

Bundle of His, bundle branches
http://www.sciencephoto.co
m/media/304266/view

Purkinje fibers
http://www.sciencephoto.co
m/media/304266/view

Ventricular depolarization
http://www.sciencephoto.co
m/media/304266/view

Ventricular repolarization
http://www.sciencephoto.co
m/media/304266/view

Two full cardiac cycles
http://web.squ.edu.om/med-Lib/MED_CD/E_CDs/anesthesia/site/content/v02/020536r00.HTM

Evaluation of cardiac function
• Physical exam/monitoring – Thoracic auscultation
• Heart rate and rhythm
• Presence of murmurs
– Mucous membrane color • Intestinal color
– CRT
– Pulse palpation • Pulse quality
• Pulse deficits

Evaluation of cardiac function
• Heart rate
• Heart rhythm
• Blood pressure – Indirect
– Direct
• Pulse oximetry
• Capnography
• Central venous pressure
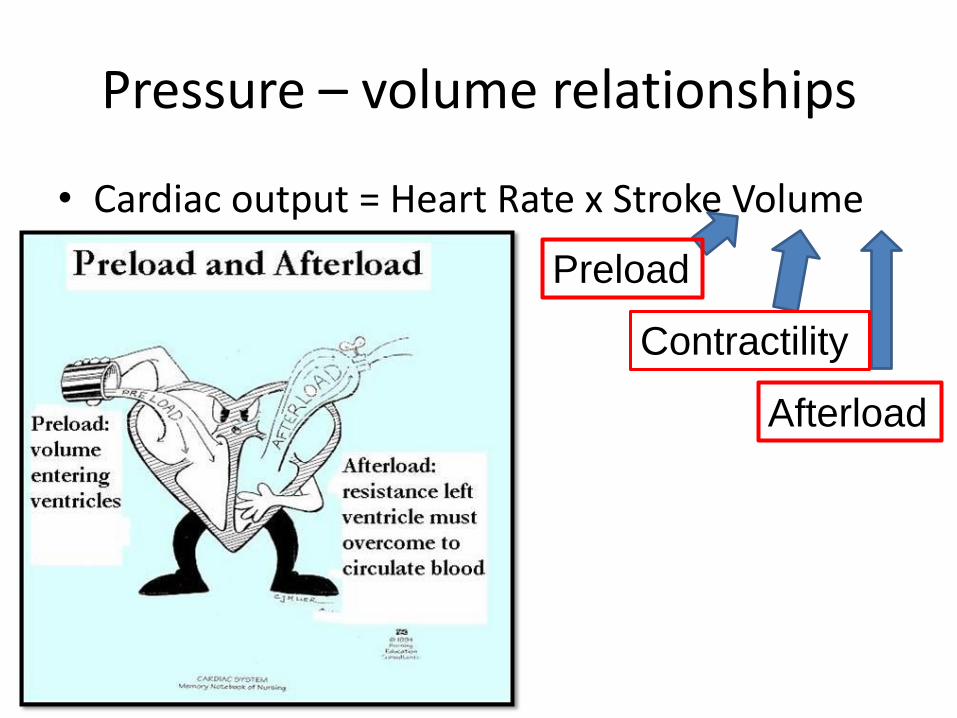
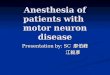
Pressure – volume relationships
• Cardiac output = Heart Rate x Stroke Volume
Preload
Afterload
Contractility

Determinants of stroke volume
http://www.cvphysiology.co
m/Cardiac%20Function/CF
002.htm

Overview
• Cardiac function review
• Cardiovascular effects of anesthetic drugs
• Cardiac diseases
– General anesthetic considerations
– Case examples

Opioids
• Minimal CV effects (clinical analgesic dosing)
• Bradycardia
– Medullary vagal stimulation
– Responds to anticholinergics
• Histamine release hypotension
– Especially morphine (avoid rapid IV)
http://www.dailymedplus.com/monograph/view/setid/b325028e-0722-4c8c-9fdb-ab6fb0dc460c

Benzodiazepines
• Limited CV effects
• No appreciable change in HR, myocardial contractility, CO, ABP
– 0.5-2.5mg/kg IV (dogs)
• Generally cardio-protective
http://vurtpunk.deviantart.com/art/Mr-
Diazepam-13629111

Phenothiazines (acepromazine)
• Conscious dogs – Decreases SV, CO, MAP (20-25%, 0.1mg/kg IV)
– Increase or no change in HR
• Dogs on inhalant
• Ace premed then
isoflurane: 24% decrease
in MAP (0.1mg/kg IM)
• Conscious cats
• 30% decrease in MAP
(0.1mg/kg IM)
http://www.gopetplan.com/blogpost/petplan-pet-insurance-presents-a-
sedentary-life--pets-and-anesthesia
Alpha-2-agonists (dexmedetomidine)
• Dose-dependent CV effects
– Endogenous catecholamines antagonize the clinical effect
• Vasoconstriction hypertension
– Reflex bradycardia (e.g. HR<40-50 bpm)
– HR and CI decrease (60%, 5-20 micr domitor/kg, conscious dogs)
– Hypertension exacerbated by atropine when given simultaneously (Congdon 2011)

Dexmedetomidine
• ~35-45 minutes post injection
– Decreased vascular tone hypotension & decreased cardiac output
• CV effects lessened under inhalant

Imidazole hypnotics (etomidate)
• Metomidate in 35% propylene glycol – Can cause hemolysis (clin signif??)
• No change in HR, BP or myocardial performance (canine)
• Anti-convulsant properties – May be neuroprotective after global
ischemia (e.g. cardiac arrest)
• Should not be used as CRI – Cortisol suppression
http://www.safestchina.
com/wholesalers-
powder-injection/
Dissociatives (ketamine, tiletamine)
• Increased sympathetic efferent activity
– Positive inotropy
• Increased myocardial O2 demand
– 2 minutes post injection
• Increased HR, MAP, CO
– 15 min post-inj: normal HR, MAP, CO
– No change in vascular tone
http://www.adammaxwell.com/t
he-library/published-
online/special-k-and-the-
yorkshire-terrier-floatation/

Sedative hypnotic (propofol)
• Decreases arterial pressure
– Myocardial contractility
– Vasodilation (arterial and venous)
• Enhances catecholamine-associated arrhythmias
– Not inherently arrhythmogenic
http://www.za
zzle.com/got_
propofol_shirt
-
23546131003
3221603

Anticholinergics
• Block presynaptic muscarinic cholinergic receptors and parasympathetic nerve terminals
– facilitates NE and ACh release
– Sinus tachycardia
• Increased myocardial work
• Decreased myocardial perfusion

Volatile inhalants
• Dose-dependent CV effects – Direct myocardial depression
• Decreased CO, blood pressure
– Vasodilation HYPOTENSION
• Decrease sympathoadrenal activity – Renin/angiotensin system may not respond normally
to hemorrhage
• Partially obtunded baroreceptor reflexes – hypotension or hypovolemia may not cause
tachycardia

Cardiac diseases in dogs/cats
• Congenital – Patent ductus arteriosus – Aortic or pulmonic stenosis – AV valve dysplasia – Septal defects
• Acquired – Valvular endocardiosis – Hypertrophic cardiomyopathy (feline) – Dilated cardiomyopathy (canine) – Pulmonary hypertension
• Heartworm disease
– Dysrhythmias (noncardiac disease)

Overview
• Cardiac function review
• Cardiovascular effects of anesthetic drugs
• Cardiac diseases
– General anesthetic considerations
– Case examples

Cardiac murmurs
• Intensity: Grade (I-VI out of VI)
• Timing: systolic, diastolic
• Location (point of maximal intensity:
– Basilar/apical
– Left/right

http://en.wikipedia.org/
wiki/Heart_murmur

Innocent murmurs
• “Innocent” = functional – Mild turbulence within heart and great
vessels – Diminish by 4-5 months of age
• Characteristics – Systolic – < III or IV/VI intensity
• Intensity may change from day to day
– Short duration, low-pitched/vibrating
• Murmurs that are not innocent – >IV/VI intensity, precordial thrill, diastolic

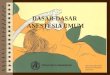
Aortic and pulmonic stenosis
• Narrowed aortic or pulmonic outflow tracts
• Systolic basilar murmur
• CO depends primarily on HR – Positive inotropy doesn’t increase
CO
– Bradycardia decreased CO
– Tachycardia may predispose to ventricular arrhythmias • Very cautious use of anticholinergics
http://www.heart-valve-
surgery.com/aortic-stenosis-
valve-heart-narrowing.php

Pulmonic stenosis – Anesthetic recommendations
• Avoid drugs that drastically change heart rate – Anticholinergics
– Alpha-2-agonists (xylazine, dexmedetomidine)
• Maintain preload to maintain stroke volume – If fluid overload, result is ascites (this is less
critical than pulmonary edema)
– 5ml/kg/hr fluid rate
– 5ml/kg crystalloid boluses as needed for hypotension

Aortic stenosis – Anesthetic considerations
• Maintain heart rate
– Avoid: ketamine, alpha-2-agonists
– Use: opioids (maybe not fentanyl?)
• Maintain adequate stroke volume
– Fluid restriction
• Good monitoring is key
– TPR, ECG, Invasive blood pressure
– Capnography

Myxomatous Valvular disease
• Insufficiency or stenosis – impaired CO failure (if severe)
– Great variability in severity and valves involved
• Preanesthetic work-up – Min database, chest films, +/- echo
• Anesthetic goals – Maintain HR, contractility
– Avoid vasocontriction (increases in afterload)
http://www.dog-
obedience-training-
review.com/cavalier-king-
charles-spaniel.html

Valvular insufficiency – anesthetic guidelines
• Skip morning dose of ACE inhibitor
• Protocol: – Use opioids +/- benzodiazepines
– Induce with ket/val or propofol (mild) or etomidate/val (severe)
– Conservative IV fluid therapy
– Use anticholinergics with caution
– BP monitoring +/- CVP
• Contraindicated: α-2-agonists – Bradycardia, increased afterload

Hypertrophic cardiomyopathy (feline)
• Stiff LV, poor diastolic function
– Mitral regurg and hypertension
• Early disease
– symptomatic (+/- murmur)
• Progressive disease
– Murmur, arrhythmias, dyspnea, thromboembolic disease
– Heart failure, sudden death with stress
http://www.statesymbolsu
sa.org/Maine/cat_maine_
coon.html
Anesthetic management (feline HCM)
• Contraindicated drugs – Acepromazine
• Decreases afterload reduced coronary perfusion
– Ketamine and anticholinergics • Increases myocardial O2 demand
• Monitoring – TPR, indirect blood pressure, ECG
– Ideal if symptomatic: direct blood pressure, capnography, pulse oximetry
• Ventilation for Fozzy: peak airway pressure <15 cm H2O
Dilated cardiomyopathy (canine DCM)
• Features – Systolic dysfunction
– Increased end-systolic and end-diastolic volumes eccentric hypertrophy
– Poor myocardial contractility
– +/- dysrhythmias • Atrial fibrillation
– No atrial contraction (“kick”)
– No atrial-ventricular synchrony low stroke volume

DCM - Anesthetic recommendations
• Delay elective procedures
• Maintain contractility – Avoid negative inotropic drugs, e.g.
propofol, alpha-2-agonists
• Maintain normal heart rate – Avoid drugs that cause tachycardia
(anticholinergics)
– Avoid drugs that cause bradycardia (alpha-2-agonists, high dose opioids)

DCM – Anesthetic recommendations
• Pre-operative: measure blood pressure
• Premeds: opioid/benzo combo
• Induction drugs – Etomidate or neurolept combo
– Ketamine = okay if paired with benzodiazepine.
• Maintenance with inhalant – Opioids decrease inhalant requirement
http://balilandandvilla.blogsp
ot.com/2012/08/doberman.ht
ml
Pulmonary hypertension (e.g. heartworm disease)
• Pulmonary hypertension
– Avoid ketamine and dexmedetomidine
– Good monitoring
• Symptomatic HW disease
– Dysrhythmias
– Pulmonic embolic disease
– Possible decreased CO
https://www.msu.edu/~silvar/h
eartworm.htm?pagewanted=al
l

Heartworm disease: anesthetic recommendations
• USE benzodiazepines and opioids
• Avoid drugs that significantly increase afterload – Don’t use dexmedetomidine
• Cautious with acepromazine
• +/- Avoid drugs with documented link to pulmonary hypertension – Ketamine
– Oxymorphone
General anesthetic guidelines for cardiac patients
• Preoxygenate ~3-5 minutes
• Good monitoring (case-appropriate)
– TPR
– Blood pressure!!
– +/- ECG
– +/- capnography
– +/- pulse oximetry
• Use multi-modal approach!
Drugs to use carefully in cardiac patients
• Drugs that cause tachy- or bradycardia
• Drugs that significantly change SVR
• Drugs that decrease contractility
• Drugs/techniques with a narrow margin of safety
– Mask induction (no premed)
– High-dose acepromazine (>0.05mg/kg)
General anesthetic guidelines for cardiac patients
• +/- fluid restriction (2-5ml/kg/hr)
– Depends on disease and procedure
• Drugs almost always appropriate for cardiac patients (with good monitoring!)
– Opioids
– Benzodiazepines
– Etomidate
– Regional/local anesthesia

General anesthetic guidelines for cardiac disease
• Keep procedure as short as possible
• Post-op monitoring
• Skip morning dose of ACE inhibitors
–Reduce intraanesthetic
hypotension
http://shop.farmvet.com/P
harmacy/Pet_Pharmacy/E
nalapril-Maleate-Tablets

Summary…
• Anesthetic drugs have variable effects on cardiovascular function
– Safe anesthetic management depends on…
• Knowledge of these anesthetic drug effects
• Knowledge of cardiac pathophysiology
• Monitoring!
• Good planning and organization!
“There are no safe anesthetic
agents, there are no safe anesthetic
procedures. There are only safe
anesthetists.” -Robert Smith, MD
And for those lingering questions or difficult cases…
• The UGA Anesthesia service does phone consultations! 800-861-7456 – Erik Hofmeister, DVM MA DACVA, DECVAA
– Jane Quandt, DVM MS DACVA DACVECC
– Molly Shepard, DVM DACVA
– Cynthia Trim, BVSc, MRCVS, DVA, DACVA, DECVAA
– Residents: • Jill Maney, VMD
• Stephanie Kleine, DVM
References
• Congdon JM, et al 2011. Evaluation of the sedative and cardiovascular effects of intramuscular administration of dexmedetomidine with and without concurrent atropine administration in dogs. 1;239(1):81-9.
• Guyton and Hall. 2006. Textbook of Medical Physiology.
• Tranquilli, Thurmon, Grimm. 2007. Lumb and Jones’ Veterinary Anesthesia and Analgesia.
• Tilley, Smith, Oyama, Sleeper. 2008. Manual of Canine and Feline Cardiology.
• Lamont LA, et al. 2002. Doppler echocardiographic effects of medetomidine on dynamic left ventricular outflow tract obstruction in cats. JAVMA 221 (9): 1276-1281.
• Cardiac cycle diagram: http://www.google.com/imgres?imgurl=http://2.bp.blogspot.com/_uiyskjNZYt8/TJW2uBf-P2I/AAAAAAAACHc/efGjdpXNqwQ/s1600/Mechanical%2Band%2BElectrical%2BEvents%2Bof%2Bthe%2BCardiac%2BCycle.jpg&imgrefurl=http://medipptx.blogspot.com/2010/09/mechanical-and-electrical-events-of_501.html&usg=__0wpCdLXkpAFTj2CZG4YKEB-8MrQ=&h=816&w=1200&sz=149&hl=en&start=0&sig2=yv9g0Q1TS4vTCsIbQ9N9lw&zoom=1&tbnid=nsmBikvf3tCLTM:&tbnh=129&tbnw=179&ei=nhPLTbSiLYS2twfklvDhBw&prev=/search%3Fq%3Dcardiac%2Bcycle%26hl%3Den%26sa%3DX%26rls%3Dcom.microsoft:en-us:IE-SearchBox%26rlz%3D1I7TSNA_enUS371US371%26biw%3D1345%26bih%3D585%26tbm%3Disch%26prmd%3Divns0%2C34&itbs=1&iact=hc&vpx=382&vpy=225&dur=6942&hovh=185&hovw=272&tx=142&ty=105&page=1&ndsp=21&ved=1t:429,r:9,s:0&biw=1345&bih=585
• Aortic stenosis diagram: http://www.google.com/imgres?imgurl=http://petheatlhinfo.com/wp-content/uploads/2011/01/Aortic-Stenosis.gif&imgrefurl=http://petheatlhinfo.com/aortic-stenosis-dogs.html&usg=__FmP2lWIklHLRucmlNSbSVBqI2GE=&h=350&w=350&sz=38&hl=en&start=0&sig2=fxyOUSz2-w3ELXMk_rhPUg&zoom=1&tbnid=BpWaWJnxyDDMDM:&tbnh=160&tbnw=156&ei=6lnLTYfRIcXL0QGSvsCoBQ&prev=/search%3Fq%3Daortic%2Bstenosis%2Bcanine%26hl%3Den%26sa%3DX%26rls%3Dcom.microsoft:en-us:IE-SearchBox%26rlz%3D1I7TSNA_enUS371US371%26biw%3D1345%26bih%3D585%26tbm%3Disch%26prmd%3Divns&itbs=1&iact=hc&vpx=133&vpy=185&dur=9454&hovh=225&hovw=225&tx=108&ty=134&page=1&ndsp=12&ved=1t:429,r:0,s:0
• PDA diagram: http://www.google.com/imgres?imgurl=http://health.stateuniversity.com/article_images/gem_04_img0496.jpg&imgrefurl=http://health.stateuniversity.com/pages/1146/Patent-Ductus-Arteriosus.html&usg=__RHxfb65ZXDu3dBE2B1FP3kSHPN4=&h=282&w=370&sz=22&hl=en&start=0&sig2=mMcAqGG1Q_Q4RAjfFTB9xQ&zoom=1&tbnid=5QFzhJv9hR-JZM:&tbnh=121&tbnw=159&ei=glrLTd-mPKTY0QGy7sHCBQ&prev=/search%3Fq%3Dpatent%2Bductus%2Barteriosus%26hl%3Den%26sa%3DX%26pwst%3D1%26rls%3Dcom.microsoft:en-us:IE-SearchBox%26rlz%3D1I7TSNA_enUS371US371%26biw%3D1345%26bih%3D585%26tbm%3Disch%26prmd%3Divns&itbs=1&iact=hc&vpx=975&vpy=112&dur=10186&hovh=196&hovw=257&tx=144&ty=137&page=1&ndsp=23&ved=1t:429,r:5,s:0
• http://php.med.unsw.edu.au/embryology/index.php?title=Advanced_-_Cardiac_Conduction
• http://php.med.unsw.edu.au/embryology/index.php?title=Advanced_-_Cardiac_Conduction