Embed Size (px)
Citation preview

8/3/2019 casehg7-101122073056-phpapp01
http://slidepdf.com/reader/full/casehg7-101122073056-phpapp01 1/13
LINICAL PICTURE:
50 years old female patient presented clinically with right sided hemiplegia due to left putameno-capsular cerebralmorrhage. (To inspect the patient's full radiological study, click on the attachment icon (The paper clip icon in the leftne) of the acrobat reader then double click on the attached file) (Click here to download the attached file)
ADIOLOGICAL FINDINGS:
CASE OF THE WEEK
PROFESSOR YASSER METWALLY
LINICAL PICTURE
ADIOLOGICAL FINDINGS
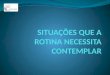
Figure 1. Precontrast CT scan showing aputameno-capsular hypertensivehematoma surrounded by a moderatedegree of edema with positive mass effect.
Figure 2. Precontrast CT of the samepatient one year later showing a slit-like
apoplectic cyst (slit-like scar) replacing thehematoma with negative mass effect.

8/3/2019 casehg7-101122073056-phpapp01
http://slidepdf.com/reader/full/casehg7-101122073056-phpapp01 2/13
AGNOSIS: HYPERTENSIVE PUTAMENO-CAPSULAR CEREBRAL HEMORRHAGE
SCUSSION:
aemorrhagic microvascular brain disease constitutes the other facet of the bad coin (the microvascular brain disease)e first facet of which is the ischemic microvascular brain disease. Both the haemorrhagic and the ischaemiccrovascular brain disease share common haemorheological, metabolic endocrinal abnormalities (The metabolicndrome) and cardiac changes(LVH). In microvascular brain disease, the small penetrating arterioles of thebependymal and the pial microvascular systems tend to become stenosed and undergo lipohyalinosis or they may dilateform microaneurysms. From the pathological point of view both Lipohyalinosis and microaneurysms, almost
variably, coexist in the same individual, thus making the patient Liable to develop either the ischaemic or theemorrhagic microvascular brain diseases.
icroaneurysmal formation occurs predominantly in the territory of the subependymal microvascular system,thusaking the incidence of the haemorrhagic microvascular events much more frequent in the periventricular gray matter
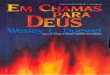
Figure 3. (A) The hematoma and (B) theapoplectic cyst (slit-like scar)
IAGNOSIS:
ISCUSSION
Figure 1. Microaneurysms of the smallpenetrating arterioles

8/3/2019 casehg7-101122073056-phpapp01
http://slidepdf.com/reader/full/casehg7-101122073056-phpapp01 3/13
halamus, basal ganglia and the internal capsule) or the immediate periventricular white matter. The coexistence of ohyalinosis and microaneurysms in the periventricular regions will explain the propensity of the diseasedcrovascular system either to thrombose (resulting in lacunar infarctions) or to rupture and leak resulting inriventricular haematoma formation. Lacunar infarctions and hypertensive cerebral haemorrhages are two facets of e and the same bad coin (the microvascular brain disease).
icroaneurysmal formation should weaken the arteriolar wall so that rupture and leakage can occur even inrmotensive states. When microaneurysmal rupture occurs, the bleeding will result in haematoma formation. Theeeding will then be arrested by occlusive thrombosis of the bleeding microaneurysms. Following microaneurysmalpture and bleeding, the size of the resulting haematoma will be determined by the bleeding time. The bleeding time is anction of the whole blood viscosity in general and the platelet aggregability in particular.
ould microaneurysmal bleeding occurs during periods of higher blood viscosity, the bleeding time will be shorter andbsequently the size of the resulting haematoma will be smaller. In fact during high blood viscosity the bleeding is notfrequently arrested before forming haemorrhages adequate to give rise to immediate clinical sequelae. Patients withgher blood viscosity and thrombotic tendency, although less likely to develop serious haemorrhagic microvascularents, they are particularly liable to develop serious ischaemic microvascular events.
uring periods of lower blood viscosity and thrombotic tendency of the blood, microaneurysmal bleeding might result inge haematoma formation that may split along the planes of the white matter forming a substantial space occupying
ot, or may rupture into the ventricular system resulting in massive ventricular haemorrhage. In general inverserrelation is present between the haematoma size and the current blood viscosity at the time of microaneurysmaleeding.
tients with microvascular brain disease might have recurrent events which could be purely haemorrhagic or purelyhaemic, however, it is not uncommon for some patients to fluctuate between the haemorrhagic and the ischaemicents, developing haemorrhagic events at certain times and ischaemic events at other times. In general ischaemiccrovascular events are much more common and much more frequent than the haemorrhagic events.
ATHOGENESIS OF HYPERTENSIVE CEREBRAL HEMORRHAGE
ypertension causes fibrinoid necrosis of these penetrating arterioles. The massive intracerebral hemorrhage which is amplication of hypertension, arises from rupture of a necrotic arteriole or from rupture of a minute "miliary"eurysm formed at the site of necrosis. These aneurysms were first described by CHARCOT and BOUCHARD. The
equency of fibrinoid necrosis and miliary aneurysm formation in vessels within basal ganglia and thalamus accountsr the frequency of intracerebral hemorrhage in those locations. Fibrinoid is identified by its structureless or sometimesanular red appearance on H&E stain and by the fact that , unlike hyalinized smooth muscle which is also eosinophilic,
Figure 2. Microaneurysms are predominatelydistributed in the immediate periventricularregion

8/3/2019 casehg7-101122073056-phpapp01
http://slidepdf.com/reader/full/casehg7-101122073056-phpapp01 4/13
e fibrinoid areas stain with stains for fibrin such as PTAH or Putz stain or with certain trichrome stains. The fibrinoidange in these vessels was called lipohyalinosis by Miller-Fisher in a very influential series of articles. However thatrm is confusing because hyalinized arteries are arteries whose media has undergone a pathologic change which is notrinoid necrosis and which by itself does not lead to rupture. Indeed hyalinized arterioles are common in hypertension.
he term lipohyalinosis stresses the presence of fat in the degenerate arteriolar wall but again this change is not thellmark of the arterioles that are in danger of rupturing or forming miliary aneurysms. The fibrinoid change is thetical change in these diseased arteriolar segments looks and stains just like the fibrinoid seen in renal and otherterioles in malignant hypertension. The important point to remember is that, for unknown reasons, the brain arteriolesn undergo fibrinoid necrosis even in so-called benign hypertension--that is in patents with only modest blood pressurevation. For that reason it is important to treat even benign hypertension. The series figures below illustrates thethologic processes that can lead to rupture.
gure 3. A, The figure shows the wall of an arteriole stained with H&E. The amorphous pink [eosinophilic] material ine wall could be either fibrinoid or amyloid. To prove that it is firbrinpoid the section or its close neighbor should beained with any one of several techniques that stain fibrin [e.g. Putz stain-blue; or the PTAH stain-blue; or a trichromeain such as the azo carmine stain; the azo carmine is particularly good because it distinguishes fibrinoid from gardenriety hyalinization by staining fibrin/fibrinoid red while staining collagen or hyalinized collagen blue.]. B, This section
as stained with azocarmine. An arteriole in the subarachnoid space has an amorphous red material occupying a goodrtion of its wall. This is fibrinoid. Fibrinoid is frequently segmental in distribution so that the entire circumferenceay not be involved and other areas along the length of the vessel may also be spared. C, This figure was also stainedth azocarmine. The arteriole wall is replaced by red fibrinoid and displays aneurysmal dilation.

8/3/2019 casehg7-101122073056-phpapp01
http://slidepdf.com/reader/full/casehg7-101122073056-phpapp01 5/13
gure 4. A,B Sometimes a miliary aneurysm thrombosis rather than ruptures. It then appears as a fibrous ball whichay be separated from the parent vessel due to the plane at which the section has been cut. If the section is close to therent arteriole there will be elastic tissue at the margin of the ball. This elastic tissue stains black with the VVG stain in)
ATHOLOGY
rebral Haematomas occur much more frequently at the putameno-capsular and the thalamic regions and may rupture
o the ventricular system. Less common sites include the cortical and the immediate subcortical white matter, especiallythe parietal region, the pons and the cerebellum.
he resulting haematoma is dark red in colour due to the existence of deoxyhaemoglobin inside the intact RBCS. Duringe subacute stage (3 days - one month) the dark red colour of the haematoma is replaced by a brownish discoloration,hich starts at the periphery of the haematoma and then extends to its center. This brownish discoloration occurs due toe replacement of deoxyhaemoglobin by the oxidized methemoglobin.
ute hematoma usually spreads between white matter tracts resulting in island of viable brain tissues within thematoma itself. Bleeding usually stops shortly after the initial ictus, however in a substantial minority of patients thematoma continues to expand usually within the first hour after the presentation. Expansion after one hour is unusual.nce hematoma forms, vasogenic edema forms around the clot as osmotically active serum proteins are released from thematoma. Edema peaks at about 48 hours and usually begins to resolve after 5 days. Whether the brain tissues
rrounding the acute hematoma is ischemic -due to vascular compression- or not is controversial. Functionalppression (diaschisis) of brain activity rather than ischemia is more probable.
Risk of Hematoma Enlargement
nearly one quarter of initially alert patients presenting with spontaneous intracerebral hemorrhage, secondaryterioration in level of consciousness occurs within the first 24 hours after onset. Hematoma expansion and edemarmation are believed to be the major factors involved In several large prospective and retrospective studies,vestigators have evaluated the rate of hematoma enlargement after initial presentation and report rates ranging fromto 38% within the first 24 hours of admission.[27,28]
their review of 627 patients with spontaneous intracerebral hemorrhage Fujii, et al..[27] reported that CT scanningthin 24 hours of admission demonstrated enlargement of the hematoma in 14% of patients. Five factors were found to
associated with enlargement: admission shortly after onset of symptoms, heavy alcohol consumption, irregularlyaped hematoma, reduced level of consciousness, and low level of fibrinogen.
Figure 5. The pathologist got lucky when this section wastaken. Here a miliary aneurysm that has neen converted to afibrous ball or globe, shown in this longitudinal section, stillconnected to the parent arteriole by a thin neck.

8/3/2019 casehg7-101122073056-phpapp01
http://slidepdf.com/reader/full/casehg7-101122073056-phpapp01 6/13
gure 6. Cerebral (A) and pontine (B) acute haemorrhage, C, acute cerebellar hemorrhage
radually the haematoma is surrounded by reactive gliosis and macrophages laden with haemosiderin granules (Ferricdroxide). The clot is gradually absorbed starting with its periphery and is replaced by a yellow fluid, this is called anoplectic cyst. Reactive gliosis progressively increases and ultimately transforms the haematoma into a slit-like scar.
gure 7. A, acute putameno-capsular & intraventricular hemorrhage, B, apoplectic cyst

8/3/2019 casehg7-101122073056-phpapp01
http://slidepdf.com/reader/full/casehg7-101122073056-phpapp01 7/13
gure 8. A, Subacute caudate hemorrhage, B, apoplectic cyst, C, Hypertensive hemorrhage into basal ganglia regionpecifically: internal capsule).
thologically the brains of patients with cerebral haemorrhages very frequently show evidence of past microvascularhaemic events such as lacunar infarctions, leukoaraiosis,etc.
CIDENCE OF COMMON ANATOMICAL SITES IN HYPERTENSIVE INTRACEREBRAL HAEMORRHAGE
gure 9. Incidence (in % ) of the common anatomical sites in hypertensive intracerebral haemorrhage
RUCTURAL NEUROIMAGING OF MICROVASCULAR CEREBRAL HAEMORRHAGE
CT imaging of haematoma.
cerebral haematoma, in the acute stage, has higher attenuation values on precontrast scan (hyperdense). The higherenuation values of fresh blood is due to the existence of packed haemoglobin in the haematoma. In particular the
obin component of the haemoglobin is responsible for the increased CT density on precontrast scan. With progressivesorption of haemoglobin, (this usually starts from the periphery of the haematoma) the attenuation value of theematoma gradually decreases until the high density haematoma is replaced by a low density space occupying cyst.
gure 10. A, Acute haematoma, B, an apoplectic cyst and C, an old haematoma (slit-like scar)
he evolution of the haematoma from a high density clot to a low density cyst usually takes a period that ranges betweene month to three months. The walls of this cyst might enhance and the haematoma at this stage might be mixed withscess or glioma. History is of paramount significance at this stage. Very old haematoma appears by CT scan as a slit-e hypodense area with negative mass effect.
general Haematomas are space-occupying with positive mass effect and are commonly surrounded by a hypodensedema area. The most common sites are the putameno-capsular and the thalamic sites and either of them might ruptureraventricularly. Less common sites includes the parietal lobe, pons and cerebellum.
he diagnosis of acute ICH is virtually 100% reliable with non-contrast CT due to the characteristic mass of blood of

8/3/2019 casehg7-101122073056-phpapp01
http://slidepdf.com/reader/full/casehg7-101122073056-phpapp01 8/13
gh attenuation value, due to the presence of the globin component of the haemoglobin molecule. Under exceptionalcumstances, patients with profound anaemia, with a haematocrit of 20% or less have presented with an acuteematoma which was isointense to brain on account of the low haemoglobin contents of the fresh haematoma. Freshood has an attenuation value of 55-85 Hounsfield units, the high attenuation (50-70 Hounsfield units) is from high
otein concentration within intact red blood cells and not iron content 1.
the fresh clot starts to retract after 24-48 hours from onset, there is serum extrusion around its periphery, resulting inring of hypointensity that surrounds the haematoma . In the subacute stage, the haematoma maintains its mass effectt becomes progressively less dense, from the periphery toward the center, until reaching isointensity with the adjacentain parenchyma. The infusion of intravenous contrast at this stage can demonstrate an area of ring enhancement at theriphery of the haematoma. In the chronic stage, the mass effect of the haematoma is no longer present, post-contrast
hancement has disappeared after about 6 weeks from onset , and the residual is a hypointense cavity, at times in therm of a slit that can be indistinguishable from an area of old cavitated infarction.
More detailed description of the CT scan appearance of brain hemorrhage
he CT appearance of hemorrhage is determined by the degree of attenuation of the x-ray beam, which is proportionalthe density of hemoglobin protein (relative to plasma concentration) within the hematoma.
mediately following vessel rupture, the hematoma consists of a collection of red blood cells, white blood cells, plateletumps, and protein-rich serum that has a heterogeneous appearance on CT with attenuation in the range of 30–60ounsfield units (HU), depending on the degree of plasma extrusion [20]. In this hyperacute phase, hemorrhage may befficult to distinguish from normal cortex because of similar attenuation. Over minutes to hours, a fibrin clot forms with
increase in attenuation to 60–80 HU (Fig. 11) [20]. Clot retraction and extrusion of serum can further increase
enuation to as high as 80–100 HU in the center of the hematoma. The degree of attenuation may be reduced in patientsth severe anemia [21], impaired clot formation due to coagulopathy, or volume averaging with adjacent tissue.
asogenic edema evolves around the hematoma within hours and may continue to increase for up to 2 weeks aftermorrhage onset [22].
ver the following days, cells and protein are broken down and scavenged by macrophages, leading to slowly decreasingenuation, with the greatest decrease at the periphery of the hematoma and more gradual evolution toward the centerig. 11) [23]. Within 4 to 9 days, the hematoma attenuation decreases to that of normal cortex, and within 2 to 3 weeks toat of normal white matter [20].
he CT recognition of subacute intracerebral hematoma can be challenging because the attenuation is similar to that of rmal brain tissue, although mass effect may still be present. MR imaging can confirm subacute hematoma. As timees on, attenuation continues to decrease to levels below that of the normal brain. Eventually, the hematoma resolveso a fluid-filled or slit-like cavity that may be difficult to visualize on CT (Fig. 11). Contrast enhancement is not presentthe initial days following ICH but may develop at the periphery in weeks to months [24], sometimes leading to
Figure 11. CT appearance of hemorrhage. Serial CT scans of right thalamichematoma. (A) Acute ICH in the right thalamus with mean attenuation 65HU. (B) CT performed 8 days later than (A); the periphery of thehematoma is now isodense to the brain while the center of the hematomahas mean attenuation 45 HU. (C) CT performed 13 days later than (A)shows continued evolution of the hematoma with decreasing attenuation.(D) CT performed 5 months later than (A) shows a small area of encephalomalacia in the location of the previous hemorrhage.

8/3/2019 casehg7-101122073056-phpapp01
http://slidepdf.com/reader/full/casehg7-101122073056-phpapp01 9/13
agnostic confusion with brain tumor or abscess.
blood-fluid level may be seen in medium to large ICH within the first hours after onset; the dependent portion displaysgher attenuation (Fig. 12) due to sedimentation of cellular elements [25]. This finding may be more common in ICHused by anticoagulation [26], but it is not specific and has also been described in ICH due to hypertension, trauma,mor, or arterial-venous malformation. The association with shorter time interval from ICH onset, and in some casesth anticoagulation, has led to speculation that incomplete clotting is required for blood-fluid level formation.
x 1. As the hemorrhage evolves, different characteristic appearances can be identified on CT, depending on the age of e bleed. CT findings over time are as follows:
EREBRAL EDEMA ASSOCIATED WITH NONTRAUMATIC CEREBRAL HEMORRHAGE
aditionally, ICH was believed to cause permanent brain injury directly by mass effect. However, the importance of matoma-induced inflammatory response and edema as contributors to secondary neuronal damage has since been
cognized. 28,29,30
least three stages of edema development occur after ICH (Table 1). In the first stage, the hemorrhage dissects alonge white matter tissue planes, infiltrating areas of intact brain. Within several hours, edema forms after clot retraction
consequent extrusion of osmotically active plasma proteins into the underlying white matter 28,29. The second stagecurs during the first 2 days and is characterized by a robust inflammatory response. In this stage, ongoing thrombinoduction activates by the coagulation cascade, complement system, and microglia. This attracts polymorphonuclear
ukocytes and monocyte/macrophage cells, leading to up-regulation of numerous immunomediators that disrupt the
ood-brain barrier and worsen the edema. 28,29,30 A delayed third stage occurs subsequently, when red blood cell lysis
ads to hemoglobin-induced neuronal toxicity. 28,29,30 Perihematomal edema volume increases by approximately 75%ring the first 24 hours after spontaneous ICH and has been implicated in the delayed mass effect that occurs in the
cond and third weeks after ICH. 28,29,30
hrombin is an essential component of the coagulation cascade, which is activated in ICH. In low concentrationsrombin is necessary to achieve hemostasis. However, in high concentrations, thrombin induces apoptosis and earlytotoxic edema by a direct effect. Furthermore, it can activate the complement cascade and matrix metalloproteinases
MMP) which increase the permeability of the blood brain barrier. 28,29,30
layed brain edema has been attributed, at least in part, to iron and hemoglobin degradation. Hemoglobin isetabolized into iron, carbon monoxide, and biliverdin by heme oxygenase. Studies in animal models show that heme
ygenase inhibition attenuates perihematomal edema and reduces neuronal loss. 28,29,30 Furthermore, intracerebralfusion of iron causes brain edema and aggravates thrombin-induced brain edema. In addition, iron induces lipid
Figure 12. CT with blood-fluid level. A 77-year-old woman was admitted with coma of 4hours' duration. CT scan shows massive left hemispheric hematoma with blood-fluid level.No history of anticoagulation or coagulopathy.
After 7-10 days, the high density of blood begins to decrease, starting from the periphery of the lesion.
From 1-6 weeks, peripheral enhancement can be seen, mimicking the appearance of an abscess, possibly related tohypervascularity at the periphery of a resolving hematoma or disruption of the blood-brain barrier.
By 2-4 months, decreased density indicates cavity formation. A residual cavity is the final stage, which is reachedafter complete absorption of necrotic and hemorrhagic tissue.

8/3/2019 casehg7-101122073056-phpapp01
http://slidepdf.com/reader/full/casehg7-101122073056-phpapp01 10/13
roxidation generating reactive oxygen species (ROS), and deferoxamine, an iron chelator, has been shown to reduce
ema after experimental ICH. 28,29,30
ble 1. Stages of edema after ICH
UMMARY
ng-standing hypertension is the leading cause of spontaneous intraparenchymal hemorrhage in adults.thophysiologically, long-standing hypertension leads to reactive hyperplasia of smooth muscle cells in cerebralterioles. Eventually, smooth muscle death occurs, and vascular walls are replaced by collagen. Vascular occlusion ortasia may then result, with either ischemic or hemorrhagic consequences. Hypertensive hemorrhages may also arise ates of previous ischemic damage to the walls of small arteries and arterioles. [35]
ypertensive hemorrhages tend to occur in the basal ganglia, thalami, cerebellum, and pons; the lobar white matter mayo be affected (Fig. 3). A homogeneous, round or ovoid hematoma in one of these locations in an older adult patient has
high likelihood of being a result of the microangiopathy associated with long-standing uncontrolled hypertension. Thee of the patient (whether older than 45 years or not), the presence of a history of hypertension, and the presence of
rtain associated imaging findings may help determine the yield of further imaging to assess for causes other thanpertension. On a CT scan, one may see evidence of microvascular ischemic change in the white matter as well asidence of lacunar infarcts; these changes are common in the setting of chronic hypertension and increase the likelihoodat hypertension is the underlying cause of the acute hemorrhage. On MR, one may also see evidence of white mattercrovascular changes on fluid attenuated inversion recovery (FLAIR) and T2-weighted images, as well as evidence of ior lacunar infarcts or remote parenchymal hemorrhages. It is important to include a T2*-weighted sequence in theR imaging protocol, because the presence of microbleeds in the brainstem and deep gray nuclei supports the likelihoodchronic hypertension and a hypertension-related hemorrhage. [36] Brain hemorrhages related to drug abuse (typicallycaine and methamphetamine) may mimic the appearance of brain hemorrhages associated with long-standingpertension on imaging studies, and likely share a common pathophysiology, but they tend to occur in a younger ageoup.
traparenchymal hematomas may expand by more than one-third of their original volume in up to 38% of patients who
e imaged early.[37] Hematoma expansion most commonly occurs in the first few hours after symptom onset and hasen associated with poor outcome. Risk factors for hematoma growth include time to initial CT scan (in that the earlierpatient is scanned after ICH onset, the more likely it is that the next CT will show ICH expansion), larger ICH volume
the initial CT, and oral anticoagulant use. [38] Other potentially important factors include hyperglycemia, renallure, low serum cholesterol, platelet dysfunction, and persistently increased blood pressure. [39] On CTA and on thentrast-enhanced CT obtained after the CTA, the presence of focal contrast extravasation is associated with hematomapansion, [40,41,42] providing potential justification for consideration of performing these studies on presentation to thespital. Performing CTA can also help avoid the pitfall of misinterpreting hemorrhages caused by underlyingthologic conditions such as aneurysms or vascular malformations as hypertensive in patients who are older and who dove a diagnosis of hypertension.
First stage (hours) Second stage (within first 2 days) Third stage (after first 2 days)
Clot retraction and extrusion of osmotically active proteins
Activation of the coagulation cascadeand thrombin synthesis
Complement activation
Perihematomal inflammation andleukocyte infiltration
Hemoglobin inducedneuronal toxicity
UMMARY

8/3/2019 casehg7-101122073056-phpapp01
http://slidepdf.com/reader/full/casehg7-101122073056-phpapp01 11/13
pportive care (including blood pressure control and correction of coagulopathy) is the mainstay of management of ute intraparenchymal hemorrhage, with surgical evacuation having a more limited role in its management. [43] Mostperts agree that cerebellar hematomas that are greater than 3 cm in diameter should be emergently evacuated if thetient is deteriorating neurologically or if the hematoma exerts mass effect on the brainstem or causes hydrocephalus.rthermore, based on the results of the International Surgical Trial in Intracerebral Hemorrhage (STICH), surgicalacuation may be considered for patients with superficial (<1 cm from the cortical surface) lobar hematomas. [43]hether minimally invasive surgical techniques (using mechanical devices and/or endoscopy) to remove the hematomafer benefit over conventional craniotomy/craniectomy is unknown and currently under investigation.
Addendum
A new version of this PDF file (with a new case) is uploaded in my web site every week (every Saturday andremains available till Friday.)
To download the current version follow the link "http://pdf.yassermetwally.com/case.pdf ". You can also download the current version from my web site at "http://yassermetwally.com". To download the software version of the publication (crow.exe) follow the link:
http://neurology.yassermetwally.com/crow.zip The case is also presented as a short case in PDF format, to download the short case follow the link:
http://pdf.yassermetwally.com/short.pdf At the end of each year, all the publications are compiled on a single CD-ROM, please contact the author to know
more details.
Screen resolution is better set at 1024*768 pixel screen area for optimum display. Also to view a list of the previously published case records follow the following link (http://wordpress.com/tag/case-
record/) or click on it if it appears as a link in your PDF reader To inspect the patient's full radiological study, click on the attachment icon (The paper clip icon in the left pane) of
the acrobat reader then double click on the attached file. Click here to download the short case version of this case record in PDF format
ferences
New PF, Aronow S. Attenuation measurements of whole blood and blood fractions in computed tomography.adiology 1976;121:635-40.
Atlas SW, Thulbom KR. MR detection of hyperacute parenchymal hemorrhage of the brain. Am J Neuroradiol98;19:1471-507.
Gomori JM, Grossman RI, Goldberg HI, et al. Intracranial hematomas: imaging by high-field MR. Radiology85;157:87-93.
Wilberger JE, Rothfus WE, Tabas J, et al. Acute tissue tear hemorrhages of the brain: computed tomography andnicopathological correlations. Neurosurgery 1990;27:208-13.
Barnett HJM, Yatsu FM, Mohr JP, Stein BM, eds.: Stroke: Pathophysiology, Diagnosis, and Management. 3rd ed.
hurchill Livingstone; 1998.
Bradley WG Jr: MR appearance of hemorrhage in the brain. Radiology 1993 Oct; 189(1): 15-26.
Broderick JP, Brott T, Tomsick T: Intracerebral hemorrhage more than twice as common as subarachnoidmorrhage. J Neurosurg 1993 Feb; 78(2): 188-91.
roderick JP, Brott TG, Duldner JE: Volume of intracerebral hemorrhage. A powerful and easy-to-use predictor of 30-y mortality. Stroke 1993 Jul; 24(7): 987-93.
EFERENCES

8/3/2019 casehg7-101122073056-phpapp01
http://slidepdf.com/reader/full/casehg7-101122073056-phpapp01 12/13
Challa VR, Moody DM, Bell MA: The Charcot-Bouchard aneurysm controversy: impact of a new histologic technique.Neuropathol Exp Neurol 1992 May; 51(3): 264-71.
. Chan S, Kartha K, Yoon SS: Multifocal hypointense cerebral lesions on gradient-echo MR are associated withronic hypertension. AJNR Am J Neuroradiol 1996 Nov-Dec; 17(10): 1821-7.
. Fazekas F, Kleinert R, Roob G: Histopathologic analysis of foci of signal loss on gradient-echo T2*- weighted MRages in patients with spontaneous intracerebral hemorrhage: evidence of microangiopathy-related microbleeds. AJNR
m J Neuroradiol 1999 Apr; 20(4): 637-42.
. Gokaslan ZL, Narayan RK: Intracranial Hemorrhage in the Hypertensive Patient. Neuroimaging Clinics of North
merica 1992; 2: 171-86.
. Gomori JM, Grossman RI: Mechanisms responsible for the MR appearance and evolution of intracranialmorrhage. Radiographics 1988 May; 8(3): 427-40.
. Nelson JS, Parisi JE, Schochet SS Jr: Principles and Practise of Neuropathology. Mosby - Year Book, Inc. St. Louis,O; 1993.
. Robertson CS, Contant CF, Gokaslan ZL: Cerebral blood flow, arteriovenous oxygen difference, and outcome inad injured patients. J Neurol Neurosurg Psychiatry 1992 Jul; 55(7): 594-603.
. Ruscalleda J, Peiro A: Prognostic factors in intraparenchymatous hematoma with ventricular hemorrhage.uroradiology 1986; 28(1): 34-7.
. Spangler KM, Challa VR, Moody DM: Arteriolar tortuosity of the white matter in aging and hypertension. Acroradiographic study. J Neuropathol Exp Neurol 1994 Jan; 53(1): 22-6.
. Taveras JM, Pile-Spellman J: Neuroradiology. 3rd ed. Williams & Wilkins; 1996.
. Welch KMA, Caplan LR, Reis DJ, Weir B, Siesjo BK, eds.: Primer on Cerebrovascular Diseases. Morgan Kaufmann;97.
. Bergstrom M, Ericson K, Levander B, et al.. Variation with time of the attenuation values of intracranial hematomas.Comput Assist Tomogr. 1977;1(1):57–63.
. Kasdon DL, Scott RM, Adelman LS, et al.. Cerebellar hemorrhage with decreased absorption values on computed
mography: a case report. Neuroradiology. 1977;13(5):265–266.
. Inaji M, Tomita H, Tone O, et al.. Chronological changes of perihematomal edema of human intracerebralmatoma. Acta Neurochir Suppl. 2003;86:445–448.
.Messina AV. Computed tomography: contrast enhancement in resolving intracerebral hemorrhage. AJR Am Jentgenol. 1976;127(6):1050–1052.
. Ichikawa K, Yanagihara C. Sedimentation level in acute intracerebral hematoma in a patient receivingticoagulation therapy: an autopsy study. Neuroradiology. 1998;40(6):380–382.
. Pfleger MJ, Hardee EP, Contant CF, et al.. Sensitivity and specificity of fluid-blood levels for coagulopathy in acuteracerebral hematomas. AJNR Am J Neuroradiol. 1994;15(2):217–223.
. Dolinskas CA, Bilaniuk LT, Zimmerman RA, et al.. Computed tomography of intracerebral hematomas. I.ansmission CT observations on hematoma resolution. AJR Am J Roentgenol. 1977;129(4):681–688.
. Fujii Y, Takeuchi S, Sasaki O, et al: Multivariate analysis of predictors of hematoma enlargement in spontaneousracerebral hemorrhage. Stroke 29:1160–1166, 1998
. Kazui S, Naritomi H, Yamamoto H, et al: Enlargement of spontaneous intracerebral hemorrhage. Incidence and timeurse. Stroke 27:1783–1787, 1996

8/3/2019 casehg7-101122073056-phpapp01
http://slidepdf.com/reader/full/casehg7-101122073056-phpapp01 13/13
. Xi G, Keep R, Hoff J. Mechanisms of brain injury after intracerebral haemorrhage. Lancet Neurol. 2006;5:53–63.
. Gebel JM, Jauch EC, Brott TG, et al. Natural history of perihematomal edema in patients with hyperacuteontaneous intracerebral hemorrhage. Stroke. 2002;33:2631–2635.
. Zazulia AR, Diringer MN, Derdeyn CP, et al. Progression of mass effect after intracerebral hemorrhage. Stroke.99;30:1167–1173.
. Metwally, MYM: Textbook of neuroimaging, A CD-ROM publication, (Metwally, MYM editor) WEB-CD agency forctronic publication, version 9.10a October 2010
. Barkovich AJ, Atlas SW. Magnetic resonance imaging of intracranial hemorrhage. Radiol Clin North Am.88;26:801–820.
Atlas SW, Thulborn KR. MR detection of hyperacute parenchymal hemorrhage of the brain. AJNR Am Juroradiol. 1998;19:1471–1507.
. Parizel PM, Makkat S, Van Miert E, et al. Intracranial hemorrhage: principles of CT and MRI interpretation. Euradiol. 2001;11:1770–1783.
. Sessa M. Intracerebral hemorrhage and hypertension. Neurol Sci. 2008;29:S258–S259.
. Kinoshita T, Okudera T, Tamura H, et al. Assessment of lacunar hemorrhage associated with hypertensive stroke byho-planar gradient-echo T2*-weighted MRI. Stroke. 2000;31:1646–1650.
. Brott T, Broderick J, Kothari R, et al. Early hemorrhage growth in patients with intracerebral hemorrhage. Stroke.97;28:1–5.
. Cucchiara B, Messe S, Sansing L, et al. CHANT Investigators. Hematoma growth in oral anticoagulant relatedracerebral hemorrhage. Stroke. 2008;39:2993–2996.
. Fujii Y, Takeuchi S, Sasaki O, et al. Multivariate analysis of predictors of hematoma enlargement in spontaneousracerebral hemorrhage. Stroke. 1998;29:1160–1166.
. Wada R, Aviv RI, Fox AJ, et al. CT angiography “spot sign” predicts hematoma expansion in acute intracerebralmorrhage. Stroke. 2007;38:1257–1262.
. Goldstein JN, Fazen LE, Snider R, et al. Contrast extravasation on CT angiography predicts hematoma expansion inracerebral hemorrhage. Neurology. 2007;68:889–894.
. Kim J, Smith A, Hemphill JC, et al. Contrast extravasation on CT predicts mortality in primary intracerebralmorrhage. AJNR Am J Neuroradiol. 2008;29:520–525.
. Broderick J, Connolly S, Feldmann E, et al. Guidelines for the management of spontaneous intracerebral hemorrhageadults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council,gh Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working
roup. Circulation. 2007;116(16):e391–e413.
. Metwally, MYM: Textbook of neuroimaging, A CD-ROM publication, (Metwally, MYM editor) WEB-CD agency forctronic publication, version 11.4a October 2010