Embed Size (px)
Citation preview

PL. TemporelliFondazione Salvatore Maugeri, IRCCS, Fondazione Salvatore Maugeri, IRCCS,
Divisione di Cardiologia Riabilitativa, VerunoDivisione di Cardiologia Riabilitativa, Veruno
Curiosare tra le raccomandazioni delle nuove linee guida sulla cardiopatia
ischemica cronica



Spectrum of IHDFihn SD et al. JACC 2012;60:e44-e164

“Non hai veramente
capito qualcosa finché
non sei in grado di
spiegarlo a tua nonna”
Albert Einstein

Ischemia
Popolazione
generale
Coronaropatia
Pregresso IMA,
pregressa PTCA,
pregresso CABG
Angina
“Cardiopatia Ischemica Cronica”

Prognosi a 1 anno in prevenzione primaria e nella cardiopatia ischemica acuta o cronica

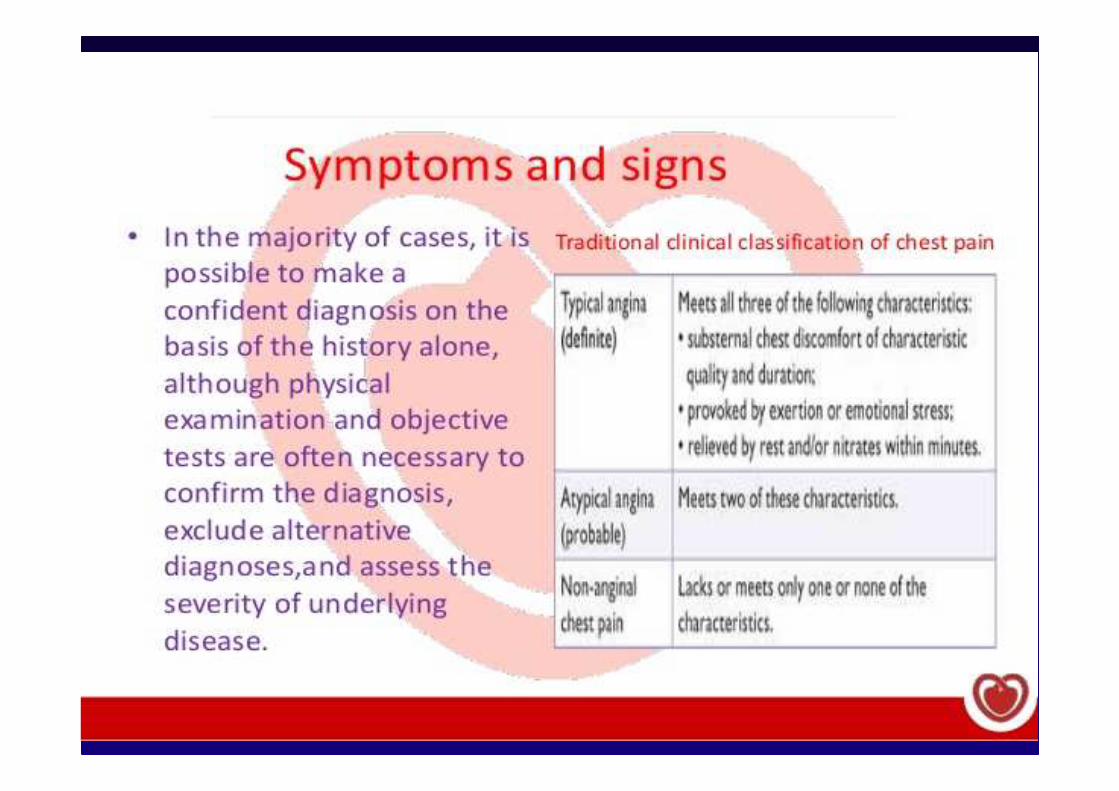
Diagnosis of stable ischemic heart disease
« The clinical examination is the key first step in
evaluating patients with chest pain and should
include a detailed assessment of symptoms…»
Fihn SD et al. JACC 2012;60:e44-e164

Pretest Likelihood of CAD in Symptomatic Patients
According to Age and Sex* (Combined Diamond/Forrester
and CASS Data)
Likelihood increases according to the presence of hypertension, smoking,
hypercholesterolemia and diabetes


High > 85%
Intermediate 15-85%
Low < 15%
Pretest likelihood of CAD in patients with suspected CAD
ESC Guidelines. Eur Heart J 2013; 34: 2949-3003

Risk Assessment in stable CAD
The Challenge
� - To indicate wich patients with CAD are
at risk for coronary events
� - To treat those patients only, in a manner
that reduces the risk of an event

Non-invasive testing in patients with suspected SCAD and an intermediate pre-test probability
ESC Guidelines. Eur Heart J 2013; 34: 2949-3003

Stress testing in patients with stable angina who require noninvasive
testing
Fihn SD et al. JACC 2012;60:e44-e164

Standard exercise ECG testing is recommended for patients with an intermediate pretest probability of IHD who have an interpretable ECG and at least moderate physical functioning or no disabling comorbidity.
I IIa IIb III
I IIa IIb III
Able to Exercise
Exercise stress with nuclear MPI or echocardiography is recommended for patients with an intermediate to high pretest probability of IHD who have an uninterpretable ECG and at least moderate physical functioning or no disabling comorbidity.

Pharmacological stress with nuclear MPI, echocardiography, or CMR is not recommended for patients who have an interpretable ECG and at least moderate physical functioning or no disabling comorbidity.
I IIa IIb III
No Benefit
Able to Exercise (cont.)
I IIa IIb III
No Benefit
Exercise stress with nuclear MPI is not recommended as an initial test in low-risk patients who have an interpretable ECG and at least moderate physical functioning or no disabling comorbidity.

Appropriateness of stress imaging in a large academic cardiology practice
SPECT ECHO
Gibbons et al. JACC 2008; 51: 1283-9
n=284 n=298

The top five inappropriate indications
INDICATION PERCENT
Detection of CAD
Asymptomatic, low CHD risk
46%
Asymptomatic, post-revascularization
< 2 years after PCI
25%
Evaluation of chest pain, low probability pt
Interpretable ECG and able to exercise
16%
Asymptomatic or stable symptoms
< 1 year after cath or abnormal prior SPECT
4%
Gibbons et al. JACC 2008; 51: 1283-9

Coronary angiography is not recommended to assess risk in patients who are at low risk according to clinical criteria and who have not undergone noninvasive risk testing.
I IIaIIb III
No Benefit
Coronary Angiography to Assess Risk After
Initial Workup With Noninvasive Testing

Lin GA JAMA 2008;300:1765-1773
Con quale frequenza viene eseguito un test provocativo di ischemia in un paziente
candidato a PCI elettiva?
Analisi retrospettiva effettuata all’interno di un
campione di 23887 pazienti, estratto dal
sistema Medicare del 2004:
10629 (44.5%) furono sottoposti alla esecuzione
di test per la documentazione di ischemia nei 90 gg precedenti la PCI

Hachamovitch R et al. Circulation 2003;107:2900–7
Benefit of revascularization in terms of survival is proportional to the amount of ischaemia
10 627 patients

pp=0.001=0.001
Rates of death or MI by ischemia reduction in subset of 105 patients with
moderate-to-severe pre-Rx ischemia
(n=68) (n=37)
32.4%
16.2%
Dea
th o
r M
I rat
e (%
)

Relationship between cardiac mortality and extent of ischemia
Risk Assessment in stable CAD
E allora ?

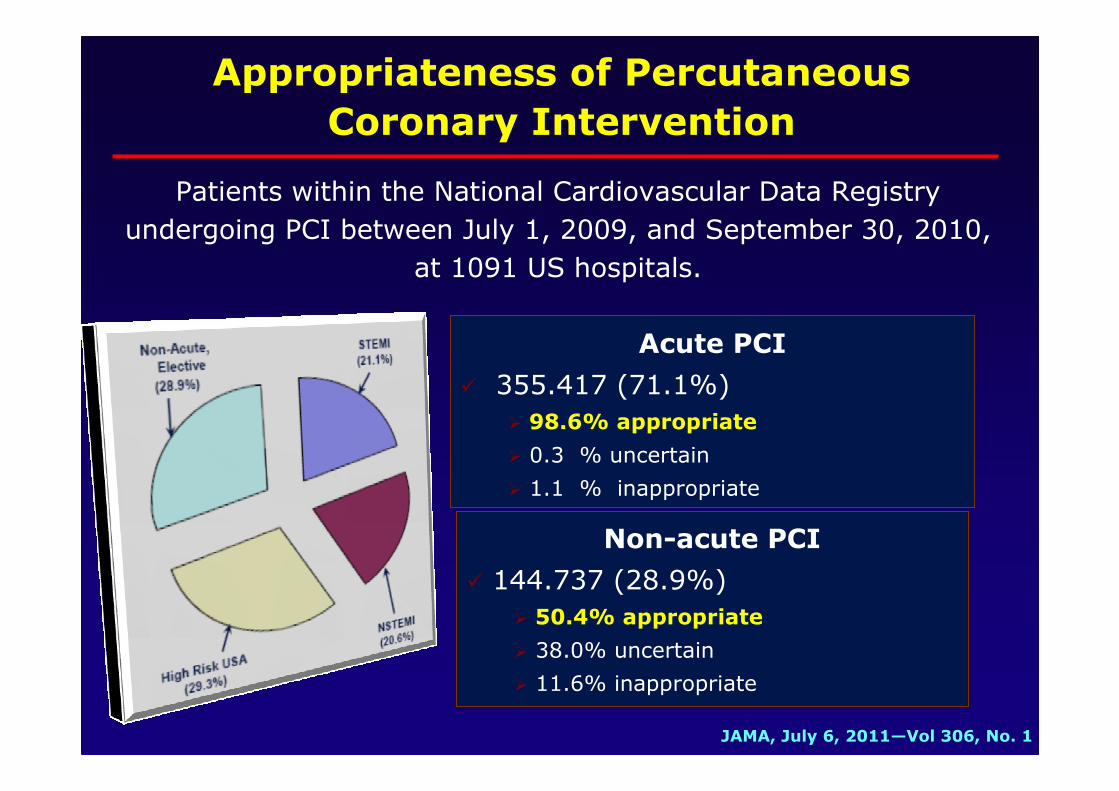
Acute PCI
� 355.417 (71.1%)
� 98.6% appropriate
� 0.3 % uncertain
� 1.1 % inappropriate
Non-acute PCI
� 144.737 (28.9%)
� 50.4% appropriate
� 38.0% uncertain
� 11.6% inappropriate
Appropriateness of Percutaneous
Coronary Intervention
JAMA, July 6, 2011—Vol 306, No. 1
Patients within the National Cardiovascular Data Registry
undergoing PCI between July 1, 2009, and September 30, 2010,
at 1091 US hospitals.

Coronary angiography is not recommended to assess risk in patients who are at low risk according to clinical criteria and who have not undergone noninvasive risk testing.
I IIaIIb III
No Benefit
Coronary Angiography to Assess Risk After
Initial Workup With Noninvasive Testing
I IIaIIb III
No Benefit
Coronary angiography is not recommended to assess risk in asymptomatic patients with no evidence of ischemia on noninvasive testing.





The Heart Team

Medical management of patients with stable coronary artery disease.
ESC Guidelines. Eur Heart J 2013; 34: 2949-3003

Sintomi Prognosi
1 A
Raccomandazioni dei BB (2006)
1 A angina e post-IM
1 B angina senza IM
Sintomi Prognosi
1 A
Raccomandazioni dei BB (2013)
Fig. 4, Pag. 35
β-bloccanti nella SCAD: confronto L.G. ESC 2006 vs 2013

� In stable CAD the debate should not be medical vs. revascularization therapy but rather which patients should be offered revascularization and when.
� PCI of specific stenotic lesions relieves angina more than medical treatment alone, but it does not change atherosclerosis in the rest of the vasculature.
Summary (i)

�Given the existing medical evidence, optimal medical therapy should be the foundation in the management of pts with stable CAD.
�“Medical therapy” today no longer means the absence of revascularisation, but rather the presence of intensive, evidence-based pharmacologic and lifestyle interventions.
�Recent guidelines reinforces the role of new antianginal agents.
Summary (ii)

2010


2010


Key Guideline Messages
• The relatively small proportion of patients who have “high-risk” anatomy (e.g., >50% stenosis of the left main coronary artery), revascularization of with CABG should be considered to potentially improve survival. Most data showing improved survival with surgery compared to medical therapy are several decades old and based on surgical techniques and medical therapies that have advanced considerably. There are no conclusive data demonstrating improved survival following PCI.

ACC/AHA Chronic Angina Guidelines:
Basic Treatment / Education
The initial treatment of the patient should include all elements:
A.A. Aspirin and Antianginal therapy
B.B. Beta blocker and Blood pressure
C.C. Cigarette smoking and Cholesterol
D.D. Diet and Diabetes
E.E. Education and Exercise
ACC/AHA 2007 Guideline Update
for the Management of Patients with Chronic Stable Angina


Key Guideline Messages
• Patients with SIHD should generally receive a “package”of GDMT that include lifestyle interventions and medications shown to improve outcomes which includes (as appropriate):– Diet, weight loss and regular physical activity;– If a smoker, smoking cessation;– Aspirin 75-162mg daily;– A statin medication in moderate dosage;– If hypertensive, antihypertensive medication to achieve a BP
<140/90; If diabetic, appropriate glycemic control.

Anti-ischemic Strategies in Ischemic Stable Heart Disease
Initial therapy
Persistent/Recurrent ischemia
↑↑↑↑ Antianginal drug therapy(uptitrate/add additional
agents)
Repeat revascularization (if possible)
Drug therapy PCI CABG

Freedom from angina in trials comparing a routine invasive with an initial non-
invasive strategy in stable CAD
Simoons ML and Windecker S Eur Heart J 2010; 31; 530–541

Ranolazine in combination with beta blockers can be useful when prescribed for relief of symptoms when initial treatment with beta blockers is not successful in patients with SIHD.
I IIaIIb III
Use of Anti-Ischemic Medications
Ranolazine can be useful when prescribed as a substitute for beta blockers for relief of symptoms in patients with SIHD if initial treatment with beta blockers leads to unacceptable side effects or is ineffective or if initial treatment with beta blockers is contraindicated.
I IIaIIb III

Patients with SIHD should receive periodic follow-up, at least annually, that includes all of the following:a.Assessment of symptoms and clinical function;b.Surveillance for complications of SIHD, including heart failure and arrhythmias;c.Monitoring of cardiac risk factors; andd.Assessment of the adequacy of and adherence to recommended lifestyle changes and medical therapy.
I IIaIIb III
Periodic Follow-Up
I IIaIIb III Assessment of LVEF and segmental wall motion by echocardiography or radionuclide imaging is recommended in patients with new or worsening heart failure or evidence of intervening MI by history or ECG.
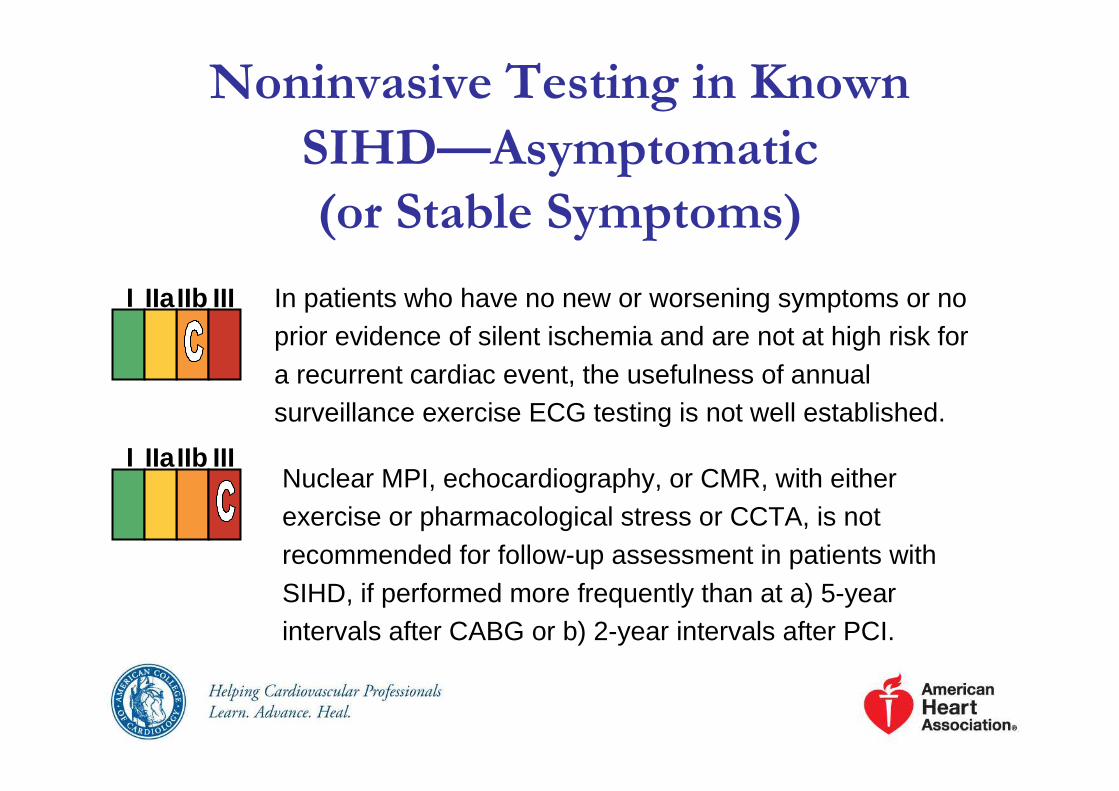
In patients who have no new or worsening symptoms or no prior evidence of silent ischemia and are not at high risk for a recurrent cardiac event, the usefulness of annual surveillance exercise ECG testing is not well established.
I IIaIIb III
I IIaIIb III
Noninvasive Testing in Known
SIHD—Asymptomatic
(or Stable Symptoms)
Nuclear MPI, echocardiography, or CMR, with either exercise or pharmacological stress or CCTA, is not recommended for follow-up assessment in patients with SIHD, if performed more frequently than at a) 5-year intervals after CABG or b) 2-year intervals after PCI.

Conferme

Risk Assessment in CAD
The Challenge
� - To indicate wich patients with CAD
are at risk for coronary events
� - To treat those patients in a manner that
reduces the risk of an event

Stress testing in patients with stable angina
who require noninvasive testing
54
Fihn SD et al. JACC 2012;60:e44-e164

Appropriateness of stress imaging in a large academic cardiology practice
SPECT ECHO
Gibbons et al. JACC 2008; 51: 1283-9
n=284 n=298

The top five
inappropriate indications
INDICATION PERCENT
Detection of CAD
Asymptomatic, low CHD risk
46%
Asymptomatic, post-revascularization
< 2 years after PCI
25%
Evaluation of chest pain, low probability pt
Interpretable ECG and able to exercise
16%
Asymptomatic or stable symptoms
< 1 year after cath or abnormal prior SPECT
4%
Gibbons et al. JACC 2008; 51: 1283-9
Key Guideline Messages
• The relatively small proportion of patients who have “high-risk” anatomy (e.g., >50% stenosis of the left main coronary artery), revascularization of with CABG should be considered to potentially improve survival. Most data showing improved survival with surgery compared to medical therapy are several decades old and based on surgical techniques and medical therapies that have advanced considerably. There are no conclusive data demonstrating improved survival following PCI.

Coronary arteriography is recommended for patients with SIHD whose clinical characteristics and results of noninvasive testing indicate a high likelihood of severe IHD and when the benefits are deemed to exceed risk.
Coronary angiography is reasonable to further assess risk in patients with SIHD who have depressed LV function (EF <50%) and moderate risk criteria on noninvasive testing with demonstrable ischemia.
I IIaIIb III
Coronary Angiography to Assess Risk After
Initial Workup With Noninvasive Testing
I IIaIIb III

Coronary angiography is reasonable to further assess risk in patients with SIHD and inconclusive prognostic information after noninvasive testing or in patients for whom noninvasive testing is contraindicated or inadequate.
Coronary angiography for risk assessment is reasonable for patients with SIHD who have unsatisfactory quality of life due to angina, have preserved LV function (EF >50%), and have intermediate risk criteria on noninvasive testing.
I IIaIIb III
Coronary Angiography to Assess Risk After
Initial Workup With Noninvasive Testing
(cont.)
I IIaIIb III

Coronary angiography for risk assessment is not recommended in patients with SIHD who elect not to undergo revascularization or who are not candidates for revascularization because of comorbidities or individual preferences .
Coronary angiography is not recommended to further assess risk in patients with SIHD who have preserved LV function (EF >50%) and low-risk criteria on noninvasive testing.
I IIaIIb III
No Benefit
Coronary Angiography to Assess Risk After
Initial Workup With Noninvasive Testing
(cont.)
I IIaIIb III
No Benefit
“Cardiopatia Ischemica Cronica”Definizione
1. Pazienti sintomatici con possibile Angina Pectoris stabile da sforzo, o suoi equivalenti
2. Pazienti asintomatici, ma con evidenza clinico-strumentale di pregresso Infarto Miocardico (da oltre 6 mesi)
2. Pazienti asintomatici, ma portatori di patologia ostruttiva coronarica accertata (ad es. pazienti già sottoposti a PCI o CABG) (da oltre 6 mesi)
ACP Clinical Guideline, Ann Intern Med 2004; 141: 562
ACC/AHA Guideline, J Am Coll Cardiol, 2003; 41:159

Continuità assistenziale
post-dimissione
NSTEMI
(n=2912)
STEMI
(n=2833)
Counseling infermieristico
710 (26.4%) 741 (28.5%)
Percorso prevenzione
388 (14.5%) 562 (21.6%)
Riabilitazione cardiologica
213 (7.3%) 325 (12%)
Percorso fumo 95 (3.3%) 174 (6.1%)
Percorso obesi 94 (3.3%) 106 (3.7%)
Percorso diabete 93 (3.2%) 86 (3.0%)

Joint ESC Guidelines. Eur Heart J 2012, May 3
• Maggiori “input” dalla medicina generale e dal nursing
• Maggiore enfasi al controllo degli stili di vita in prevenzione primaria e secondaria
• Analisi più dettagliata dei limiti dei sistemi di “grading” dell’evidenza
• Ri-definizione delle priorità e degli obiettivi
• Revisione dell’approccio al rischio nei soggetti giovani
• Aggiornamento delle sezioni sui “fattori di rischio classici”
• Nuove sezioni dedicate ai “nuovi fattori di rischio”

Percentage of the Decrease in Deaths from CHD
Attributed to Treatments and Risk-Factor Changes
Ford ES et al. N Engl J Med 2007; 356:2388
The use of revascularization for chronic angina resulted in a reduction of approximately 15,690 deaths in 2000, as compared with deaths in 1980, or approximately
5% of the total and only 1.3% was
attributable to PCI.
The Centers for Disease Control

Secondary Prevention As a Multifactorial Approach and Comprehensive Long-term
Services
�Optimized therapy
�Risk stratification
�Risk factors modification
�Counseling and behavioural interventions
�Follow-up
ESC Guidelines, Eur Heart J, 2006;27:1341-1381

Secondary Prevention As a Multifactorial Approach and Comprehensive Long-term
Services
�Optimized therapy
�Risk stratification
�Risk factors modification
�Counseling and behavioural interventions
�Follow-up
ESC Guidelines, Eur Heart J, 2006;27:1341-1381

Comprehensive Medical Therapy For Patients with CHD or Other Vascular Disease
Risk Reduction
� ASA 20-30%
� Beta Blockers 20-35%
� ACE inhibitors 22-25%
� Statins 25-42%
The four medications every atherosclerosis patient should be treated with, unless contraindications exist and are documented
AHA/ACC Guidelines. Circulation 2006

Ivabradine reduces primary end point in angina patients
n=1507P=0.05
Years
0
5
10
15
20
0 0.5 1 1.5 2
Cum
ulat
ive
inci
denc
efo
r P
EP
* (
%)
--24%24%Placebo
IvabradineIvabradine
Primary end point (PEP) : CV death + hospitalizatio n for HF or MI
Fox K, Ford I, et al; BEAUTIFUL Investigators. Effect of ivabradine on cardiovascular outcomes in patients with
stable coronary artery diseaseand left-ventricular systolic dysfunction with limiting angina: a subgroup
analysis of the randomized, controlled BEAUTIFUL trial. Eur heart Jour On line.

Effects of Ranolazine on Recurrent
Cardiovascular Events After ACS
Recurrent Ischemia (%)
Days from Randomization
Ranolazine 17.3%
(N=3,279)
Placebo 20.0%
(N=3,281)
HR 0.87 (95% CI 0.76 o 0.99)
P =0.030
0.0
00
.05
0.1
00
.15
0.2
00
.25
0 180 360 540

Mehta HR et al. Circulation 2005;112:II-793
Medication ComplianceCRUSADE Registry (1-Year)

Interruzione delle “evidence-based medical therapies” e prognosi dopo IMA:
dati del Registro PREMIER
Ho PM, et al. Arch Intern Med. 2006;166:1842-1847
HR

� “A total of 46.2% of the patients in the clopidogrel group
discontinued the study medication temporarily (for more than five
days), as compared with 45.4% in the placebo group”
�“The overall tolerability of prasugrel was comparable to
clopidogrel as demonstrated by a similar incidence of study drug
discontinuation between treatment groups (17.91% vs 17.32%,
p=NS).”
THE TRITON TIMI 38 TRIAL Prasugrel - FDA Advisory Committee Breafing
Document, Jan 2009
�“Premature discontinuation in 23.4% of pts in the ticagrelor
group vs 21.5% of pts in the clopidogrel group (p=0.002)”
THE PLATO TRIAL Wallentin L et al. NEJM 2009; 361: 1045-57
Discontinuation of Clopidogrel, Prasugrel and Ticagrelor
in CURE, TRITON and PLATO
Discontinuation of Clopidogrel, Prasugrel and Ticagrelor
in CURE, TRITON and PLATO
THE CURE TRIAL N Engl J Med 2001;345:494-502

Medication NonadherenceMedication Nonadherence
Baroletti S, Dell'Orfano H. Circulation. 2010;121:1455-8

Secondary Prevention As a Multifactorial Approach and Comprehensive Long-term
Services
�Optimized therapy
�Risk stratification
�Risk factors modification
�Counseling and behavioural interventions
�Follow-up
ESC Guidelines, Eur Heart J, 2006;27:1341-1381

Algorithm for inizial evaluation of patients with stable angina

SI
Duke Treadmill Score
NO
Basso
Follow-Up Clinico
Medio
Stress Imagingsede / estensione / vitalità
-
Follow-Up Clinico
+
Coronarografia
Alto
Stratificazione del rischio nellStratificazione del rischio nell’’Angina StabileAngina Stabile
Incapacita’
esercizio
WPW
PM
BBS
segni di scompenso
valvulopatia nuova o in deterioramento
Ecocardiografia
basale
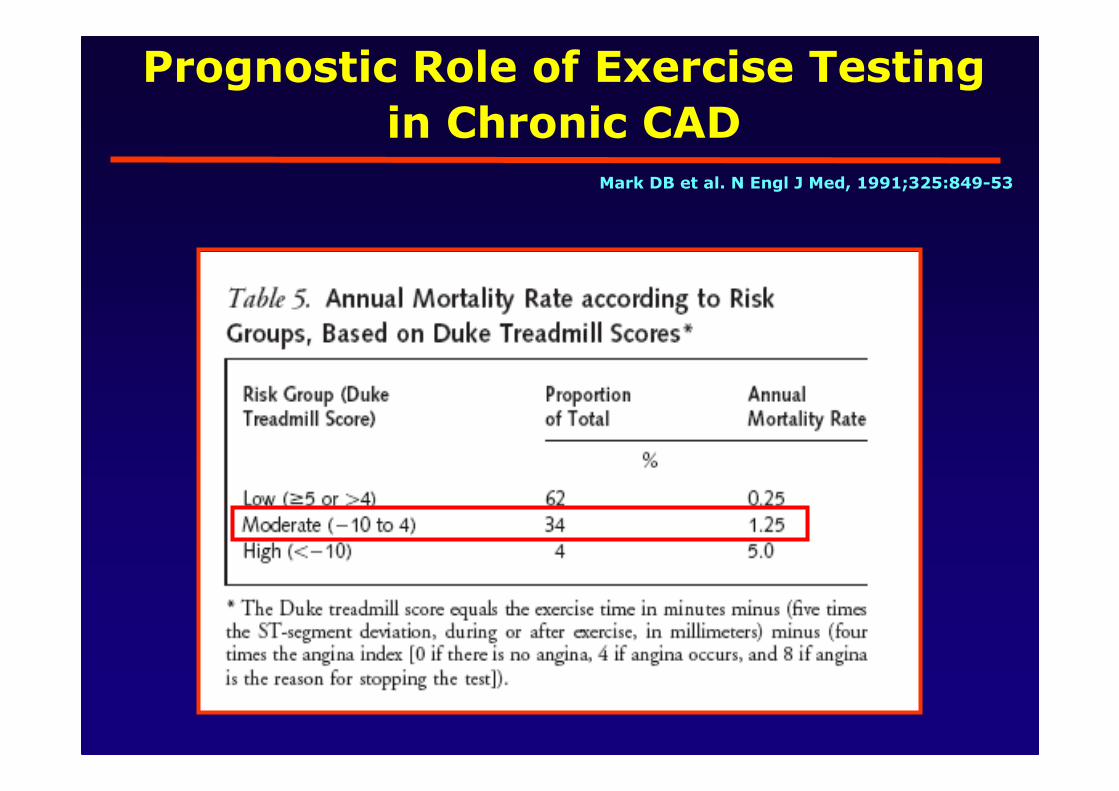
Prognostic Role of Exercise Testing
in Chronic CAD Mark DB et al. N Engl J Med, 1991;325:849-53

Appropriateness in a large academic cardiology practice
64,0%11,0%
14,0%
11,0%
AppropriateUncertainInappropriateUnclassified
64,0%9,0%
18,0%
9,0%
SPECT ECHOSPECT ECHO
Gibbons et al. JACC 2008; 51: 1283-9
n=284 n=284 n=298n=298

The top five inappropriate indications
INDICATION PERCENT
Detection of CAD
Asymptomatic, low CHD risk
46%
Asymptomatic, post-revascularization
< 2 years after PCI
25%
Evaluation of chest pain, low probability pt
Interpretable ECG and able to exercise
16%
Asymptomatic or stable symptoms
< 1 year after cath or abnormal prior SPECT
4%
Gibbons et al. JACC 2008; 51: 1283-9

Hachamovitch R et al. Circulation 2003;107:2900–7
Benefit of revascularization in terms of survival is
proportional to the amount of ischaemia
10 627 patients

2011

Frequency of Stress Testing to Document
Ischemia Prior to Elective PCI
Lin GA et al. JAMA 2008;300:1765-1773
Medicare BICS
44.5%
24%

EuroHeart
Survey
Sirtax BASKET Leaders BICS OSCAR
Italian Survey
PCI for Stable CAD in Recent All-comers
Trials and Registries in Europe

2011


Coronarografia sistematica
-in pazienti affetti da angina tipica stabile e/o ad alto rischio di CAD dopo un test provocativo (per la prognosi e per la scelta terapeutica)
Coronarografia selettiva
-in coloro per i quali il rischio di malattia rimane “intermedio” dopo l’esecuzione di un test
provocativo (ai fini diagnostici)
Coronarografia sistematica o selettiva nella cardiopatia ischemica cronica?
Zoran Olivari, ANMCO 2012Zoran Olivari, ANMCO 2012

Coronarografia
≠
PCI
Coronarografia sistematica o selettiva nella cardiopatia ischemica cronica?
Zoran Olivari, ANMCO 2012Zoran Olivari, ANMCO 2012

Secondary Prevention As a Multifactorial Approach and Comprehensive Long-term
Services
�Optimized therapy
�Risk stratification
�Risk factors modification
�Counseling and behavioural interventions
�Follow-up
ESC Guidelines, Eur Heart J, 2006;27:1341-1381



EUROASPIRE II Study Group
� Il 15% dei fumatori non erano stati informati sulla
necessità di smettere di fumare;
�Alla dimissione solo nel 31% delle relazioni erano
riportate informazioni relative alla attività fisica;
� Il 43% dei malati in sovrappeso non erano stati
informati sulla necessità di ridurre il peso;
� Istruzioni sull’alimentazione erano state fornite al
33% degli ipertesi ed al 61% dei dislipidemici
Cohen, Lancet 2001; 357

Management of Stable Coronary Disease
A 65-year old man with hypertension, obesity, and type 2 diabetes who presented with a 2-week history of exertional angina. He underwent an exercise SPECT which showed a fixed anterior defect and a reversible anterolateral defect, both of moderate size. His subsequent cardiac catheterization revealed an occluded first diagonal branch, a long lesion with 70% stenosis in the midportion of the LAD, a calcified lesion with 80% stenosis in the proximal circ, and 50% stenosis of the PDA. These findings were accompanied by anterior-wall hypokinesis and an EF of 45% by left ventriculography.
N Engl J Med. 2007;357(17):1762-1766
Treatment Option 1Appropriate Medical Management
and Close Follow-up for Adherence and Efficacy
Salim Yusuf, and
Ernest Fallen,
Treatment Option 2Appropriate Medical
Management and PCI
Robert A. Harrington
Treatment Option 3Appropriate Medical
Management and CABG
Robert A. Guyton

Management of Stable Coronary Disease Polling Results
Cheng S and Jarcho J. N Engl J Med 2007;357:e28

Management of Stable Coronary Disease Polling Results

Wallentin L et al. Lancet 2000;356:9–16
Juul-Moller S et al. Lancet 1992;340:1421–1425
Shepherd J et al. N Engl J Med 1995;333:1301–1307
Mor
te/IM
A n
on fa
tale
(%
)
Follow-up (mesi)
Angina instabile/ IMA non Q (FRISC II)
16
12
8
4
0
0 2 4 6 8 10 12
Angina stabile (SAPAT)
Prevenzione primaria (WOSCOPS)
Prognosi nel paziente in prevenzione primaria e con cardiopatia ischemica acuta o cronica

Burden of Stable Angina in the US
� 9.1 million American adults have chronic angina 1
� 500,000 new cases diagnosed per year� 50% experience angina as the initial sign of ischem ic
heart disease� 213 per 100,000 annual US angina incidence in
people >30 years of age� ~50% of patients presenting with MI at the hospital
have preceding angina 2
� > 25% of patients experience angina up to five year s post-PCI with optimal medical care 3
1 Rosamond W, et al. Heart Disease and Stroke Statistics – 2008 Update. Circulation. 2008;117:e25-e146.2 Gibbons RJ, et al. ACC/AHA 2002 guideline update for the management of patients with chronic stable angina. p5
Available at: http://acc.org/qualityandscience/clinical/guidelines/stable/stable_clean.pdf3 Boden WE, et al. Optimal Medical Therapy with or without PCI for Stable Coronary Disease. N Engl J Med 2007;356:1510.

Stress Echocardiography after PCIACC/AHA 2003 Guidelines
Class I
Identification of restenosis in patients with atypical recurrent symptoms
Class IIa
Assessment of restenosis in patients with typical symptoms
Class III
Routine assessment of asymptomatic patients
Cheitlin et al, ACC/AHA Guidelines 2003

Cardiac Nuclear Imaging after PCI: ACC/AHA 2003 Guidelines
Class IIa
Stress myocardial perfusion SPECT
at 3 to 5 months after PCI in
selected, high-risk * asymptomatic
patients
Klocke et al, ACC/AHA Guidelines 2003Klocke et al, ACC/AHA Guidelines 2003
* * IVA prox, multivaso, procedure complicate, IVA prox, multivaso, procedure complicate, stent multipli, diabete, disfunzione ventricolarestent multipli, diabete, disfunzione ventricolare

Evaluating Appropriateness forCardiac Radionuclide Imaging
N=6351N=6351
ACCF/United Healthcare SPECT Pilot Study
Zona Grigia
21%

• ~ 10 million European adults have chronic angina
• 53% of patients with angiographically proven coronary artery disease originally present with sta ble angina 1
• 1 year after diagnosis, 22% have undergone PCI 2
• > 25% of patients experience angina up to 5 years post-PCI with optimal medical care 3
1Lenzen MJ, et al. Management and outcome of patients with established coronary artery disease: the Euro Heart Survey on coronary revascularization. Eur Heart J 2005;26:1169-79. 2Daly C, et al. The impact of guideline compliant medical therapy on clinical outcome in patients with stable angina: findings from the Euro Heart Survey of stable angina. Eur Heart J 2006;27:1298-304. 3Boden WE, et al. Optimal Medical Therapy with or without PCI for Stable Coronary Disease. N Engl J Med 2007;356:1510.
Burden of Stable Angina in Europe

Angina Prevalence One Year Post-MI
• Design− PREMIER (Prospective R egistry E valuating M yocardial
Infarction: E vents and R ecovery) Registry*− Multi-center prospective cohort study
� Objective− Designed to identify patient and treatment factors as sociated
with the prevalence of angina one year post-myocardia l infarction (MI)
• Primary Endpoint− Presence of angina 1 year post-MI hospitalization
� Measured by the Seattle Angina Questionnaire (SAQ)
* Study supported in part by the NIH
Maddox TM, Reid KJ, Spertus JA, et al. Arch Intern Med. 2008;168:1310-1316

• Results (n = 1957)− ~ 1 in 5 patients had angina 1 year post-MI
−Of these, ~ 1 in 5 had angina daily or weekly
− Patients tended to be−Younger−Nonwhite males−Prior CABG or baseline angina− Index hospitalization (recurrent angina)
− Among outpatient variables, patients were more likel y to • Continue smoking• Undergo PCI or CABG after the index hospitalization • Have new, persistent, or transient depression
Angina Prevalence One Year Post-MI
Maddox TM, Reid KJ, Spertus JA, et al. Arch Intern Med. 2008;168:1310-1316

Estimated Direct and Indirect Costs of Major Cardiovascular Diseases and Stroke
2008 Estimates (US$ Billions)
Source: AHA, Heart Disease and Stroke Statistics, 2 008 Update. NHLBIRosamond W, et al. Heart Disease and Stroke Statist ics – 2008 Update. Circulation. 2008;117:e138
CHD; $156,4
HTN; $69,4
Stroke; $65,5
HF; $34,8

Annual Pharmacy Costs in CAD Patients
Kempf J, Shetty S, Nelson M. Resource utilization a nd cost of care for chronic stable angina in the Un ited States. Scientific Forum on Quality of Care and Outcomes Research in Cardiovascular Disease and Stroke.
May 7-9, 2006 Washington, DC.

The Cost of Chronic AnginaAdapted from Javitz H, et al. Am J Managed Care. 20 04;10(11):S367
Direct Costs 2004 Estimates: $1.9 – $8.9 Billion (US)*
* Direct costs for angina $1.9 billion when it is the first-listed diagnosis and $8.9 billion when it is listed in any position

Trends in Cardiovascular Operations and Procedures (United States: 1979-2005)
0
200
400
600
800
1000
1200
1400
79 80 85 90 95 00 05
Pro
cedu
res
in T
hous
ands
Years
Catheterizations Open-Heart
Bypass PCI
Carotid Endarterectomy Pacemakers
Source: AHA, Heart Disease and Stroke Statistics, 2 008 Update. NHLBIRosamond W, et al. Heart Disease and Stroke Statist ics – 2008 Update. Circulation. 2008;117:e136

All of us spend far more time
thinking about “how”to best
perform PCI and much less on
“why”, “when”, and “for whom”
The Bottom Line

Stable CAD: PTCA/BMS vs. Medical Rx
Meta-analysis of 11 randomized trials; N = 2,950
Katritsis DG et al. Circulation. 2005;111:2906-12

Adapted from Boden WE, et al. Optimal Medical Therap y with or without PCI for Stable Coronary Disease . N Eng lJ Med 2007;356:1510
COURAGE: Antianginal Medication Use
PCI + Optimal Medical Therapy (21.1%
Revascularization)
Optimal Medical Therapy (32.6% Revascularization)
Baseline 1 y 3 y 5 y Baseline 1 y 3 y 5 y
Continuing Angina (%) 88 34* 28† 26 87 42 33 28
Beta-blockers (%)
85 85 84 85 89 89 86 86
Calcium Channel Blockers (%)
40 40 43 42 43 49 50 52
Long-acting Nitrates (%) 62 53 47 40 72 67 61 57
*p<0.001 for PCI + OMT vs OMT alone.†p=0.02 for PCI + OMT vs OMT alone.

Angina Symptoms Persist in Many Patients Despite Revascularization
Serruys PW, et al. N Engl J Med. 2001;344:1117-1124
Continued angina and antianginal medication use 12 months after revascularization for angina (n=1205)
100%
Stenting groupSurgery group
Pre
vale
nce
(% o
f pat
ient
s)
21%*
79%* 81%*
11%
59% 62%
0%
20%
40%
60%
80%
Continued angina
Continued antianginalmedication
Continued angina and/or antianginal
medication
*p < 0.001

Odds Ratios for Mortality in Individual Trials Comparing the PCI-Based Strategy With Medical
Treatment Strategy
Schomig, A. et al. J Am Coll Cardiol 2008;52:894-904

Ischemia Reduction Improves Outcomes
Shaw, L. J. et al. Circulation 2008;117:1283

Independent Predictors of Early Decision to Revascularize
Countries With High Rates of Angiography – Patients with Stable Angina
Variable OR 95% CI P-Value
Positive exercise ECG 4.05 2.74–6.00 <0.001
Female 0.57 0.37–0.86 0.007
Invasive center 1.62 1.03–2.55 0.04
Symptom duration >6 months 0.66 0.49–0.99 0.04
Daly CA, et al. Eur Heart J. 2005;26:1011-1022
• Majority of the 3,779 patients had been referred by a primary care physician (71%). • Mean age in the survey was 61 years

Angina Costs Managed Health CareKempf J, Shetty S, Nelson M. Resource utilization a nd cost of care for chronic stable angina in the Un ited States.
Scientific Forum on Quality of Care and Outcomes Research in Cardiovascular Disease and Stroke. May 7-9, 2006 Washington, DC.
Resource Utilization for the Year Following Index D iagnosis (N=171,172)

Objective ischemia predicts benefit of PCI
�Objective evidence of myocardial ischemia is
qualitatively and quantitatively linked to adverse
clinical outcomes
�The degree of myocardial ischemia is directly related
to the magnitude of relative clinical benefit provided by
PCI vs medical Rx
�These findings imply that part of the patients
enrolled in previous trials were unlikely to benefit from
PCI if they had no, or limited myocardial ischaemia and
suggest that functional assessment may help to
identify those who benefit from revascularization

Relationship Between Procedure Indications and
Outcomes of PCI by ACC/AHA Task Force
Class I64%
Class IIa21%
Class IIb7%
Class III8%
Anderson HV et al. Circulation. 2005;112:2786

Incidence of Angina Pectoris by Age and Gender
Framingham Heart Study: 1980/2002-2003
Source: AHA, Heart Disease and Stroke Statistics, 2 008 Update. NHLBIRosamond W, et al. Heart Disease and Stroke Statist ics – 2008 Update. Circulation. 2008;117:e59

Ricoveri ospedalieri 2010
SDO PATOLOGIA N. RICOVERI
127 Insufficienza cardiaca e shock 203885
87 Edema polmonare acuto 110438
14 Emorragia o infarto cerebrale 91307
125 Mal. CV (non IMA) con CC e senza complicanze 66509
524 TIA 59260
139 Aritmie senza complicanze 57488
143 Dolore toracico 42590
138 Aritmie con complicanze 38192
124 Mal. CV (non IMA) con CC e con complicanze 36426
122 IMA senza complicanze 35093
553 Impianti pacemaker 31683
555 PCI con diagnosi CV maggiore 31076
558 PCI senza diagnosi CV maggiore 29392

1. Abolizione del fumo
2. Controllo della dislipidemia
3. Controllo dei valori pressori
4. Regolare attività fisica
5. Controllo del peso corporeo
6. Gestione del Diabete Mellito
7. Terapia anti-aggregante
8. Terapia con ACE-inibitori/Sartani
9. Terapia beta-bloccante
10. Vaccinazione anti-influenzale
11. Cardiologia Riabilitativa
Circulation. November 29,2011


Noninvasive Risk Stratification
*Although the published data are limited; patients with these findings will probably not be at low risk in the presence of either a high-risk treadmill score or severe resting LV dysfunction (LVEF <35%).

Novità

Prevalenza dell’angina stabile
5.000.000
Coronaropatici
* Popolazione di età compresa tra i 65 e 74 anni
Da 11% a 20%*
Da 10% a 15%*
1.500.000
angina stabile
Ital Heart J 2004; 5 (Suppl 3): 49S-92S
Eur Heart J 2006; 27: 1341-81
Osservatorio Epidemiologico
Cardiovascolare Italiano
Prevalenza dall’angina stabile:
30.000/mllione di ab.
Rosamond W, et al. Heart Disease and Stroke Statistics – 2008 Update.
Circulation. 2008;117:e25-e146.
9.1 milioni di adulti americani
soffrono di angina
Daly C, et al. The impact of guideline compliant medical
therapy on clinical outcome in patients with stable angina:
findings from the Euro Heart Survey of stable angina. Eur
Heart J 2006;27:1298-304.
Circa 10 milioni di adulti europei
soffrono di angina
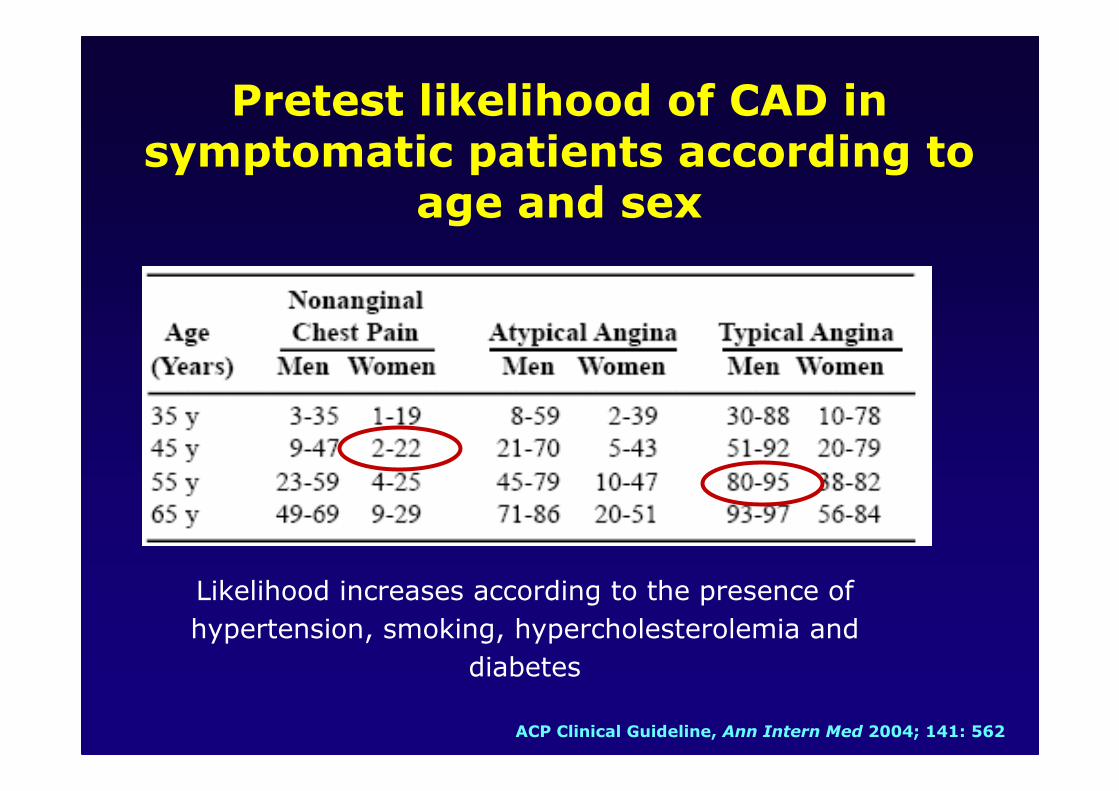
ACP Clinical Guideline, Ann Intern Med 2004; 141: 562
Likelihood increases according to the presence of
hypertension, smoking, hypercholesterolemia and
diabetes
Pretest likelihood of CAD in symptomatic patients according to
age and sex

Parametri del test associati a coronaropatia e prognosi sfavorevole
� Positività a basso carico
� Spiccato sottoslivellamento di ST (>2mm)
� Sottoslivellamento di ST in più di 5 derivazioni
� Persistenza di anomalie ECG di natura ischemica
per più di 5 minuti nel recupero
� Ridotta capacità di esercizio
� Calo PA sistolica durante sforzo
� Aritmie ventricolari maggiori durante sforzo (TV)
ESC Guidelines, Eur Heart J, 2006;27:1341-1381
ACC/AHA Guideline, J Am Coll Cardiol, 2003; 41:159

Standard exercise ECG testing is recommended for patients with an intermediate pretest probability of IHD who have an interpretable ECG and at least moderate physical functioning or no disabling comorbidity.
I IIa IIb III
Able to Exercise

Kligfied P, Circulation 2006Kligfied P, Circulation 2006
Functional capacity, angiographic coronary disease, and risk for death
in 6213 men referred for treadmill exercise testing for clinical
reasons. Functional capacity is a much more powerful predictor of
death than the presence or absence of obstructive coronary lesions.
Exercise Electrocardiogram Testing:
Beyond the ST Segment

Anti-ischemic Strategies in Ischemic Stable Heart Disease
Initial therapy
Persistent/Recurrent ischemia
↑ Antianginal drug therapy(uptitrate/add additional
agents)
Repeat revascularization (if possible)
Drug therapy PCI CABG