Embed Size (px)
Citation preview

A
K
I
d
0d
Applied nutritional investigation
Diacylglycerol oil ingestion in type 2 diabetic patients withhypertriglyceridemia
Kunio Yamamoto, M.S.a, Masao Takeshita, M.S.b,*, Ichiro Tokimitsu, Ph.D.b,Hiroyuki Watanabe, Ph.D.c, Tomohito Mizuno, M.S.d, Hideki Asakawa, M.D., Ph.D.e,
Katsuto Tokunaga, M.D., Ph.D.f, Tatsuya Tatsumi, B.S.g, Mitsuyo Okazaki, Ph.D.h, andNoriko Yagi, Ph.D.a
a Department of Nutrition, Koshien University, Takarazuka, Hyogo, Japanb Health Care Products Research Laboratories No.1, Kao Corporation, Bunka, Sumida-ku, Tokyo, Japanc Department of Food and Nutritional Science, Toita Women’s College, Shiba, Minato-ku, Tokyo, Japan
d Biological Science Laboratories, Kao Corporation, Ichikai-machi, Haga-gun, Tochigi, Japane Department of Internal Medicine, Suita Municipal Hospital, Suita, Osaka, Japan
f Department of Internal Medicine, Itami City Hospital, Itami, Hyogo, Japang Department of Nutrition, Itami City Hospital, Itami, Hyogo, Japan
h College of Liberal Arts and Sciences, Tokyo Medical and Dental University, Ichikawa, Chiba, Japan
Manuscript received January 10, 2005; accepted April 26, 2005.
bstract Objective: Coronary arteriosclerotic heart disease frequently develops in patients with diabetes.Decreased serum high-density lipoprotein cholesterol concentration and low-density lipoprotein(LDL) particle size, accompanied by hypertriglyceridemia, are associated with the onset of athero-sclerosis. We recently reported that hypertriglyceridemia was significantly improved in patients withtype 2 diabetes who ingested diacylglycerol (DAG) oil. The effect on variables, including LDLparticle size related to lipid metabolism, however, was not examined. The present study investigatedthe effects on these variables in more detail.Methods: Patients with type 2 diabetes (n � 24) were assigned to receive DAG oil or triacylglyc-erol oil, and a 3-mo, single-blind, controlled study was performed. Patients replaced cooking oil intheir daily diet with DAG or triacylglycerol oil, and anthropometry and blood sampling wereperformed at monthly intervals.Results: There were no significant differences in calorie intake or amount of test oil ingestedbetween groups. Waist circumference and serum triacylglycerol concentrations were significantlylower and serum concentrations of high-density lipoprotein cholesterol and apolipoprotein-AI weresignificantly higher in the DAG oil group than in the triacylglycerol oil group. Plasma plasminogenactivator inhibitor-1 concentrations were significantly lower in the DAG oil group. LDL particle sizetended to increase in the DAG oil group and was significantly larger in patients who had a smallinitial LDL particle size (�25.5 nm). There were no significant differences in variables related toglucose metabolism or in serum concentration of free fatty acids or total ketone bodies.Conclusions: These results indicate that DAG oil may be useful for patients who have type 2 diabetesin the management of obesity and lipid abnormalities. © 2006 Elsevier Inc. All rights reserved.
Nutrition 22 (2006) 23–29www.elsevier.com/locate/nut
eywords: Diacylglycerol; Humans; Diabetes; Hypertriglyceridemia; Low-density lipoprotein particle size
rpshal
ntroduction
Coronary arteriosclerotic heart disease (CHD) frequentlyevelops in patients who have diabetes [1]. Decreased se-
* Corresponding author. Tel.: �81-3-5630-7266; fax: �81-3-5630-9436.
mE-mail address: [email protected] (M. Takeshita).899-9007/06/$ – see front matter © 2006 Elsevier Inc. All rights reserved.oi:10.1016/j.nut.2005.04.009
um high density and decreases in serum high-density li-oprotein cholesterol (HDL-C) concentration and low-den-ity lipoprotein (LDL) particle size, accompanied byypertriglyceridemia and postprandial hyperlipidemia, aressociated with the onset of arteriosclerosis [2–4]. Severalarge-scale epidemiologic studies have suggested that a re-
ission in hypertriglyceridemia prevents CHD [5,6]; there-
ft
ltfsftsr
irt(iegp
tpp
M
S
wPTd1tt
ufo(t5ToDitr
T
otwpoaDgD
D
sbcrMcopaD
TC
NMAHWBM
ak
TF
F
A
24 K. Yamamoto et al. / Nutrition 22 (2006) 23–29
ore, an improvement in hypertriglyceridemia might be par-icularly important for patients who have diabetes.
Small, dense LDL particles are more atherogenic thanarger, less dense particles [4]. Recent evidence reported inhe Quebec Cardiovascular Study, in which there was a 5-yollow-up, has suggested that an increased proportion ofmall LDL particles (�25.5 nm) is closely associated withuture cardiovascular disease, even in the presence of rela-ively normal LDL-C concentration, and that LDL particleize might be a factor that can be used to accurately predictisk of ischemic heart disease [7].
A diet low in fat, low in glucose, and high in food fibers recommended for diabetics. Clear-cut efficacy is noteadily achieved by dietary therapy alone in clinical prac-ice. We previously reported the efficacy of diacylglycerolDAG) oil in patients who had diabetes and hypertriglycer-demia in a parallel group study [8] in which hypertriglyc-ridemia was significantly improved in patients who in-ested DAG oil daily as a cooking oil compared withatients who used conventional cooking oil.
In the present study, we examined the influence of long-erm ingestion of DAG oil on variables including LDLarticle size related to lipid metabolism in more detail inatients with type 2 diabetes.
aterials and methods
ubjects and study design
The randomized, single-blind, controlled parallel trialas conducted at the Itami City Hospital, Itami, Japan.otential subjects were screened during visits to the clinic.his study with human volunteers was performed in accor-ance with the Helsinki Declaration of 1975 as revised in983. The procedures were fully explained to the volun-eers. All subjects gave their signed informed consent before
able 1haracteristics of subjects*
TAG group DAG group
o. of subjects 13 11ale/Female 7/6 4/7ge (y) 54.3 � 13.1 61.5 � 6.2eight (cm) 163.5 � 10.8 154.5 � 8.1eight (kg) 75.7 � 21.2 65.2 � 8.9
MI (kg/m2) 28.0 � 5.9 27.3 � 3.4edicationNon-drug 5 3Statin 1 0EPA 1 0SU 3 6Insulin preparation 3 2
BMI, body mass index; DAG, diacylglycerol; EPA, eicosapentaenoiccid; SU, sulfonylurea drug; TAG, triacylglycerol (Nissin Oil Mills, To-yo, Japan)* Values are means � standard deviations.
he start of the study.
The subjects included 24 outpatients ages 38 to 79 ynder continuous nutritional counseling (dietary therapy)or diabetes (Table 1). These patients were assigned to onef two groups: a DAG oil group comprised of 11 patientsmean age 61.5 � 6.2 y, four men and seven women) and ariacylglycerol (TAG) oil group of 13 patients (mean age4.3 � 13.1 y, seven men and six women). The DAG andAG oil groups replaced their usual cooking oil with DAGil and TAG oil, with the same fatty acid composition as theAG oil, respectively, and ingested the oil with a target
ntake of 10 g/d. The study period was 3 mo after initiatinghe use of the test oil in both groups. Patient medication iseported in Table 1.
est oils
The test DAG oil was prepared from rapeseed and soyils in the presence of an immobilized lipase, according tohe method reported by Huge-Jensen et al. [9], and TAG oilith the same fatty acid composition as DAG oil wasrepared by mixing rapeseed oil, soybean oil, and saffloweril. The fatty acid compositions of the DAG and TAG oilsre listed in Table 2. DAG oil comprised 84.4 g/100 g ofAG, 14.1 g/100 g of TAG, and 1.2 g/100 g of monoacyl-lycerol (MAG). The ratio of 1,3-DAG to 1,2-DAG (2,3-AG) was 7:3.
ietary record
Subjects were instructed to record their daily meals andnacks in a dietary diary for 3 consecutive days at theeginning and end of the test period. At the time of eachlinic visit, a dietitian reviewed the food diaries and mealecord after clarifying the results by patient interviews.
ean daily intakes of energy, fat, and cooking oil werealculated from the dietary record by a dietitian on the basisf the 5th Revision of the Standard Tables of Food Com-osition in Japan. DAG intake was estimated from themount of DAG oil ingested and the DAG content of theAG oil (80 g/100 g).
able 2atty acid and acylglycerol compositions of test oils (wt%)
TAG oil DAG oil
atty acidC16:0 5.7 3.1C18:0 2.1 1.3C18:1 35.8 37.4C18:2 46.4 48.2C18:3 8.1 7.0
cylglycerolTAG 90.7 14.1DAG 4.8 84.4Monoacylglycerol 0.0 1.2Free fatty acid ND ND
DAG, diacylglycerol; ND, not determined; TAG, triacylglycerol

A
ehwoTSreSeTuCmDtKcsrA(tL(mShTuI
A
nfupA
tL(m0ttpc
iaSop
S
tdtctc(ptPwtS
R
nwsFnw
TA
EFFT
i
25K. Yamamoto et al. / Nutrition 22 (2006) 23–29
nthropometry and blood tests
Anthropometry and fasting blood sampling were performedach month after the initiation of the test ingestion at theospital. In anthropometry, body weight, body mass index, andaist circumference were measured. Plasma and serum werebtained by centrifugation at 1500g for 15 min at 4°C. SerumAG concentration was measured using an enzymatic assay kiterum (Daiya Auto TG, Daiya Chemical, Tokyo, Japan). Se-um total cholesterol concentration was measured using annzymatic assay kit (Daiya Auto T-cho, Daiya Chemical).erum free fatty acid concentration was measured using annzymatic assay kit (Determiner NEFA, Kyowa Medex,okyo, Japan). Serum LDL-C concentration was measuredsing an enzymatic assay kit (Cholestest LDL, Daiichi Purehemicals, Tokyo, Japan). Serum HDL-C concentration waseasured using an enzymatic assay kit (Cholestest N HDL,aiichi Pure Chemicals). Serum total ketone body concentra-
ion was measured using an enzymatic assay kit (3-HB Kainos,ainos Laboratories, Inc., Tokyo, Japan). Serum insulin con-
entration was measured using a solid-phase radioimmunoas-ay kit (INSULINRIABEAD II, Dinabot, Tokyo, Japan). Se-um concentrations of apolipoprotein (Apo) AI, ApoB, andpoE were measured using a turbidimetric immunoassay kit
N-asssay TIA ApoAI-H Nittobo, N-assay TIA ApoB-H Nit-obo, and N-assay TIA ApoE-H Nittobo, Nitto Boseki Co.,td, Tokyo, Japan). Plasma plasminogen activator inhibitor-1
PAI-1) concentration was measured using an enzymatic im-unoassay kit (TintElize PAI-1, Biopool International, Umea,weden). Plasma glucose was measured using a glucose-de-ydrogenase assay kit (CicaLiquid GLU; Kanto Chemicals,okyo, Japan). Serum glycohemoglobin A1c was measuredsing a latex agglutination kit (Rapidia Auto HbA1c, Fujirebionc., Tokyo, Japan).
nalysis of serum LDL size
Several methods have been established for the determi-ation of serum LDL size. This study employed high-per-ormance liquid chromatography using a gel filtration col-mn, as reported by Usui et al. [10,11]. The high-erformance liquid chromatographic system consisted of anS-8020 auto-injector, CCPS and CCPM-II pumps, and
able 3nalysis of dietary record in 24 patients with type 2 diabetes*
TAG group (n � 13)
Before A
nergy (kcal/day) 1774 � 299 1at (% energy) 24.3 � 5.8at (g/d) 48.7 � 17.3est oil (g/d) 13.2 � 10.1
DAG, diacylglycerol; TAG, triacylglycerol* Values are means � standard deviations. There were no significant d
ngestion for either group. There were no significant differences between the TA
wo UV-8020 detectors (Tosoh Corp., Tokyo, Japan) [12].ipoproteins were separated on a Superose 6HR column
300 � 10 mm; Pharmacia, Uppsala, Sweden) with 50mol/L of phosphate buffered saline (pH 7.4) containing
.15 mol/L of NaCl at a flow rate of 0.5 mL/min. Lipopro-ein particle size was determined based on individual elutionimes corresponding to the peaks on the chromatographicattern of the cholesterol profile and were computed using aalibration curve.
The procedure for this method is simple and reproduc-bility is very high, allowing for an accurate and quantitativenalysis within a short time using a small amount of serum.era collected before the study and 3 mo after the initiationf the study were stored at �80°C until used in high-erformance liquid chromatographic analysis.
tatistical analyses
Data are presented as the mean � standard deviation ofhe measured values or changes from the initial values. Aifference from the initial value was analyzed using pairedtest and Dunnett’s multiple comparison test. An intergroupomparison was performed using Student’s t test, and sta-istical difference between groups with the time-lapsehange was tested using two-way analysis of varianceANOVA). Data were analyzed on intention-to-treat sam-les. Skewed variables such as TAG were logarithmicallyransformed. Correlation coefficients were assessed usingearson’s product-moment correlation test. Differencesere considered statistically significant at P � 0.05 using a
wo-tailed test. Statistical analyses were performed withtatView 5.0 (SAS Institute, Cary, NC, USA).
esults
Based on judgments made by the physicians in charge,o aggravation of physical conditions or adverse effectsere noted after ingestion of the test oils throughout the
tudy period in any patient in the DAG or TAG oil group.urther, no liver, renal, or pancreatic abnormalities wereoted in the blood tests. No changes in medication or doseere made during the study period. Based on the dietary
DAG group (n � 11)
Before After
322 1652 � 356 1668 � 2744.0 28.6 � 6.5 29.4 � 6.115.8 52.5 � 16.1 55.2 � 17.37.3 12.5 � 5.6 15.5 � 8.2
es in any parameter between before and after initiation of the dietary oil
fter
777 �27.8 �55.9 �14.6 �
ifferenc
G and DAG groups before the study.
di3
A
eWDuewicg1mg
B
eV
geelg5AmdamdgsTf(nApgwATu
TE
B
W
TE
G
H
I
I
H
s
26 K. Yamamoto et al. / Nutrition 22 (2006) 23–29
iary, there were no differences in daily energy intake, fatntake, or amount of test oil ingested between groups (Table).
nthropometry
Table 4 lists the anthropometric values measured ev-ry month after the initiation of ingestion of the test oil.aist circumference was significantly decreased in theAG oil group compared with the TAG oil group whensing ANOVA, although there were no significant differ-nces in changes from initial values in the DAG oil grouphen using paired t test and Dunnett’s multiple compar-
son test. Changes from the initial values in waist cir-umference were also significantly different betweenroups when using ANOVA (DAG oil group: �1.2 cm atmo, �1.1 cm at 2 mo, and �1.5 cm at 3 mo). Bodyass index was not significantly different between
roups.
lood test
Tables 5 to 7 present blood chemistry values measuredvery month after the initiation of test oil ingestion.ariables related to glucose metabolism, such as blood
able 4ffects of body measurements in 24 patients with type 2 diabetes*
Groups 0 mo
MI (kg/m2) TAG (n � 13) 28.0 � 5.9DAG (n � 11) 27.3 � 3.4
aist (cm) TAG (n � 13) 95.1 � 14.6DAG (n � 11) 89.6 � 7.3
ANOVA, analysis of variance; DAG, diacylglycerol; NS, not significan* Values are means � standard deviations.† Significantly different from the initial value by paired t test: P � 0.05‡ Significantly different from TAG oil group by ANOVA: P � 0.05.
able 5ffects on glucose metabolism-related parameters in 24 patients with type
Groups 0 mo
lucose (mmol/L) TAG (n � 13) 6.69 � 1.56DAG (n � 11) 6.92 � 1.71
bA1c (%) TAG (n � 13) 6.3 � 1.1DAG (n � 11) 6.3 � 0.8
nsulin (pmol/L) TAG (n � 13) 62.3 � 26.0DAG (n � 11) 51.8 � 20.8
nsulin (pmol/L)‡ TAG (n � 10) 55.8 � 24.3DAG (n � 9) 49.3 � 22.4
OMA-R TAG (n � 13) 3.1 � 1.5DAG (n � 11) 2.6 � 1.1
ANOVA, analysis of variance; DAG, diacylglycerol oil; HbA1c, glycohignificant; TAG, triacylglycerol oil
* Values are means � standard deviations.† Significantly different from the initial value by paired t test: P � 0.05
‡ Subjects on an insulin preparation were excluded.lucose and insulin levels, were not significantly differ-nt between groups (Table 5), and there was no differ-nce in the homeostasis model assessment index calcu-ated from the blood glucose and insulin levels betweenroups (Table 5). Changes in each variable listed in Tablewere not significantly different between groups usingNOVA. Decreases in serum TAG concentrations after 3o of consumption of the DAG oil were significantly
ifferent from the initial values according to paired t testnd the decreasing tendency was shown with Dunnett’sultiple comparison test (P � 0.08). Serum TAG levels
ecreased and serum HDL-C increased in the DAG oilroup compared with the TAG oil group and there wereignificant differences in the two variables (Table 6).here were no significant differences in concentrations of
ree fatty acids or total ketone bodies between groupsTable 6). Changes in each variable listed in Table 6 wereot significantly different between groups usingNOVA. Serum ApoAI was significantly increased andlasma PAI-1 was significantly decreased in the DAG oilroup (Table 7). Changes from the initial value in PAI-1ere also significantly different between groups usingNOVA. Changes in each variable except PAI-1 listed inable 7 were not significantly different between groupssing ANOVA.
2 mo 3 mo ANOVA
6.1 28.1 � 6.2 28.1 � 6.0 NS3.4 27.3 � 3.5 27.2 � 3.613.9 96.7 � 15.0† 95.1 � 15.4 ‡
6.7 88.5 � 6.7 88.1 � 6.9
, triacylglycerol
etes*
o 2 mo 3 mo ANOVA
� 1.72 6.95 � 2.20 7.05 � 2.05 NS� 1.37 6.82 � 1.71 6.93 � 0.75� 1.1† 6.2 � 1.2 6.2 � 1.2 NS� 0.8 6.3 � 1.0 6.3 � 0.8� 28.4 53.5 � 22.0 62.8 � 34.8 NS� 21.8 56.2 � 21.5 54.5 � 24.7� 28.8 52.2 � 25.1 61.2 � 38.2 NS� 23.6 54.7 � 23.7 55.3 � 27.1� 1.6 2.8 � 1.3 3.4 � 2.3 NS� 1.4 2.8 � 1.2 2.9 � 1.4
bin A1c; HOMA-R, revised homeostasis model assessment index; NS, not
1 mo
27.9 �27.4 �95.6 �88.4 �
t. TAG
.
2 diab
1 m
6.656.746.26.3
63.252.958.852.73.12.7
emoglo
.

Lc
tdpnig
Ra
Tw
dT
D
owwApasbcD
TE
T
T
F
T
L
H
c
TE
A
A
A
A
P
t
27K. Yamamoto et al. / Nutrition 22 (2006) 23–29
DL particle size analysis by high-performance liquidhromatography
Table 8 lists the LDL particle sizes before and 3 mo afterhe initiation of test oil ingestion. There were no significantifferences across patients. In patients whose initial LDLarticle size was no larger than 25.5 nm, there was a sig-ificant difference in the third month; LDL particle sizencreased in the DAG oil group compared with the TAG oilroup.
elation between changes in serum TAG concentrationsnd LDL particle size
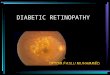
Figure 1 shows the relation between changes in serumAG concentrations and LDL sizes for all patients. Thereas a strong negative correlation between parameters, in-
able 6ffects on serum lipids in 24 patients with type 2 diabetes*
Groups 0 mo
G (mmol/L)� TAG (n � 13) 1.91 � 1.07DAG (n � 11) 2.55 � 1.65
otal ketone bodies (�mol/L) TAG (n � 13) 92.6 � 70.5DAG (n � 11) 103.2 � 131.7
FA (mmol/L) TAG (n � 13) 0.82 � 0.32DAG (n � 11) 0.78 � 0.31
C (mmol/L) TAG (n � 13) 5.56 � 0.98DAG (n � 11) 5.72 � 0.95
DL-C (mmol/L) TAG (n � 13) 3.49 � 0.94DAG (n � 11) 3.42 � 1.33
DL-C (mmol/L) TAG (n � 13) 1.25 � 0.34DAG (n � 11) 1.02 � 0.18
ANOVA, analysis of variance; DAG, diacylglycerol oil; FFA, free fatty aholesterol; NS, not significant; TAG, triacylglycerol oil; TC, total choles
* Values are means � standard deviations. Significantly different from� TG was evaluated by logarithmic transformation.§ Significantly different from TAG group by ANOVA: P � 0.05.
able 7ffects on serum lipoproteins and PAI-1 in 24 patients with type 2 diabet
Groups 0 mo
poA1 (mg/dL) TAG (n � 13) 152 � 21DAG (n � 11) 135 � 11§
poB (mg/dL) TAG (n � 13) 115 � 21DAG (n � 11) 121 � 22
poE (mg/dL) TAG (n � 13) 4.8 � 1.0DAG (n � 11) 5.5 � 2.4
poB/ApoA1 TAG (n � 13) 0.77 � 0.18DAG (n � 11) 0.91 � 0.21
AI-1 (ng/mL) TAG (n � 13) 42.6 � 17.7DAG (n � 11) 40.3 � 17.0
ANOVA, analysis of variance; Apo, apolipoprotein; DAG, diacylglyriacylglycerol oil
* Values are means � standard deviations. Significantly different from§ Significantly different from TAG oil group by Student’s t-test: p � 0
� Significantly different from TAG oil group by ANOVA: p � 0.05.icating that LDL size increased with a decrease in serumAG concentration.
iscussion
When outpatients with type 2 diabetes under continu-us nutritional counseling ingested DAG oil in this study,aist circumference, serum TAG, and plasma PAI-1ere significantly decreased, and serum HDL-C andpoAI were significantly increased after the 3-mo testeriod compared with the TAG oil group, despite equiv-lent nutritional value throughout the study period and noignificant differences in the amount of test oil ingestedetween groups. In addition, LDL particle size was in-reased in patients with a small initial LDL particle in theAG oil group. There were no significant differences in
1 mo 2 mo 3 mo ANOVA
1.97 � 1.73 1.68 � 0.81 1.83 � 0.95 §
2.46 � 1.32 2.06 � 1.19 1.98 � 1.14†
107.3 � 96.0 96.1 � 84.1 92.1 � 121.6 NS95.7 � 100.7 66.9 � 38.6 65.3 � 42.30.77 � 0.28 0.83 � 0.31 0.77 � 0.38 NS0.73 � 0.25 0.73 � 0.22 0.75 � 0.255.46 � 0.84 5.60 � 0.91 5.55 � 1.04 NS5.71 � 1.04 5.87 � 0.98 5.96 � 0.973.41 � 1.01 3.57 � 0.89 3.46 � 0.94 NS3.43 � 1.27 3.61 � 1.05 3.67 � 1.031.30 � 0.43 1.31 � 0.30 1.27 � 0.35 §
1.03 � 0.20 1.10 � 0.26 1.17 � 0.27‡
L-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoproteinG, triacylglycerolial value by paired t test: † P � 0.05, ‡ P � 0.01.
2 mo 3 mo ANOVA
27 155 � 22 158 � 25 �
16 141 � 18 145 � 15†
21 115 � 24 118 � 26 NS23 123 � 23 122 � 251.2 4.5 � 0.8 4.8 � 0.9 NS1.9 5.1 � 1.8 5.1 � 1.70.22 0.75 � 0.16 0.77 � 0.22 �
0.21 0.89 � 0.21 0.85 � 0.2119.6† 53.9 � 16.5† 58.5 � 20.1‡ �
18.4 38.4 � 18.5§ 46.2 � 13.8
l; NS, not significant; PAI-1, plasminogen activator inhibitor-1; TAG,
ial value by a paired t-test: † P � 0.05, ‡ P � 0.01.
cid; HDterol; Tthe init
es*
1 mo
155 �138 �112 �121 �4.8 �5.4 �
0.75 �0.89 �51.4 �38.6 �
cerol oi
the init.05.

sb
icvHDtFcsidcc
pthpia
iruisfcdtH
wimTPdMcvT
fmtTKt1avfsiTsrtp[ta
Fcl
TE
A
I
.05.
28 K. Yamamoto et al. / Nutrition 22 (2006) 23–29
erum concentrations of free fatty acids or total ketoneodies between groups.
Several studies have reported that hypertriglyceridemias derived from increased TAG-rich lipoprotein and de-reased serum HDL-C concentration and LDL particle sizeia the lipid transport system [13,14]. Increases in serumDL-C concentration and LDL particle size observed in theAG oil group in the present study might have been related
o an improvement in hypertriglyceridemia. As shown inig. 1, there was a significant negative correlation betweenhanges in serum TAG concentrations and LDL particleize, strongly suggesting that the serum TAG concentrations a potent regulatory factor related to LDL particle size iniabetes. There were no changes observed in serum ApoBoncentrations in either group, indicating that the number ofirculating LDL particles did not change.
Several cross-sectional studies have demonstrated that aredominance of small, dense LDL particles is associated withhe presence of CHD [15–17]. Further, prospective studiesave demonstrated that abnormalities in LDL particle sizereceded the onset of CHD [7,18,19]. Considering these find-ngs, it is suggested that the increase in LDL particle sizechieved in this study by DAG oil ingestion might be mean-
ig. 1. Correlation between changes in serum TG concentrations andhanges in LDL particle size. DAG, diacylglycerol oil; LDL, low-density
able 8ffect on LDL size (nm) in 24 patients with type 2 diabetes*
Groups
ll subjects TAG (n � 13)DAG (n � 11)
nitial LDL size � 25.5 nm TAG (n � 10)DAG (n � 9)
DAG, diacylglycerol oil; LDL, low-density lipoprotein; TAG, triacylgly* Values are means � standard deviations.† Significantly different from the initial value by paired t test: P � 0.05‡ Significantly different from TAG oil group by Student’s t test: P � 0
ipoprotein; TAG, triacylglycerol oil; TG, triacylglycerol.
ngful as it relates to a therapeutic strategy for decreasing theisk of CHD in patients with diabetes. However, it may remainnknown whether insulin resistance or other factors related tonsulin resistance directly regulate LDL particle size. In thistudy, LDL particle size was increased, whereas the levels ofasting glucose, glycohemoglobin A1c, and insulin were un-hanged. These results suggest that LDL particle size is moreirectly influenced by TAG metabolism than by insulin sensi-ivity. These findings are consistent with results reported byirano et al. [20].There is a correlation between the amount of visceral fat
ith waist circumference and plasma PAI-1 concentrationn humans [21–23]. Dietary DAG oil decreases the accu-ulation of visceral fat compared with TAG oil [24,25].herefore, the decreases in waist circumference and plasmaAI-1 concentration observed in this study might have beenue to a decrease in the amount of abdominal visceral fat.oreover, because the accumulation of visceral fat is
losely related to TAG synthesis in the liver [26], decreasedisceral fat may have played a role in the decreased serumAG concentration in the DAG oil group.
Although the mechanisms of action of DAG on visceralat are not fully elucidated, the unique metabolism of DAGight contribute to its action because the heat of combus-
ion and rate of absorption of DAG are similar to those ofAG, which has the same fatty acid composition [27].ondo et al. [28] reported that the initial products of diges-
ion of TAG are 2-MAG and fatty acids and those for,3-DAG are mainly 1(3)-MAG and fatty acids. Because theffinities of 2-MAG and 1(3)-MAG for the enzyme in-olved in TAG resynthesis, monoacylglycerol acyltrans-erase, are markedly different [29], TAG resynthesis inmall intestinal epithelial cells might be delayed after DAGngestion, and this might suppress the increase in serumAG concentration after DAG ingestion. Recent humantudies have indicated that the increase in postprandial se-um TAG concentration was smaller in the DAG oil grouphan in the TAG oil group [30,31]. Because impaired post-randial TAG clearance is associated with visceral obesity32,33], the specific metabolism of DAG in the small intes-ine might, at least in part, be involved in the decreasedmount of visceral fat. Further investigation is necessary.
o 3 mo Changes
4 � 0.69 24.77 � 0.66 �0.06 � 0.271 � 1.07 24.92 � 0.61 0.31 � 0.598 � 0.56 24.53 � 0.54 �0.05 � 0.309 � 0.91 24.77 � 0.58† 0.48 � 0.51‡
il
0 m
24.824.624.524.2
cerol o
.
Based on these above findings, ingestion of DAG oil in

tpWtstalt
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
29K. Yamamoto et al. / Nutrition 22 (2006) 23–29
he daily diet might suppress an increase in TAG-rich li-oprotein and improve abnormal lipoprotein metabolism.hile dietary therapy for diabetes has been recommended
o be low in fat, low in glucose, and high in fiber for the lifepan. In patients who have diabetes, the continuous inges-ion of DAG oil in dietary therapy might not only preventrteriosclerotic diseases but also improve their quality ofife because the properties of DAG oil are comparable tohose of conventional cooking oil.
eferences
[1] Clark LT, Ferdinand KC, Flack JM, Gavin JR III, Hall WD, Kuma-nyika SK, et al. Coronary heart disease in African Americans. HeartDis 2001;3:97–108.
[2] Fontbonne A, Eschwege E, Cambien F, Richard JL, Ducimetiere P,Thibult N, et al. Hypertriglyceridaemia as a risk factor of coronaryheart disease mortality in subjects with impaired glucose tolerance ordiabetes. Results from the 11-year follow-up of the Paris ProspectiveStudy. Diabetologia 1989;32:300–4.
[3] Groot PH, van Stiphout WA, Krauss XH, Jansen H, van Tol A, vanRamshorst E, et al. Postprandial lipoprotein metabolism in normo-lipidemic men with and without coronary artery disease. ArteriosclerThromb 1991;11:653–62.
[4] Austin MA, Breslow JL, Hennekens CH, Buring JE, Willett WC,Krauss RM. Low-density lipoprotein subclass patterns and risk ofmyocardial infarction. JAMA 1988;260:1917–21.
[5] Frick MH, Elo O, Haapa K, Heinonen OP, Heinsalmi P, Helo P, et al.Helsinki Heart Study: primary-prevention trial with gemfibrozil inmiddle-aged men with dyslipidemia. Safety of treatment, changes inrisk factors, and incidence of coronary heart disease. N Engl J Med1987;317:1237–45.
[6] Ericsson CG, Hamsten A, Nilsson J, Grip L, Svane B, de Faire U.Angiographic assessment of effects of bezafibrate on progression ofcoronary artery disease in young male postinfarction patients. Lancet1996;347:849–53.
[7] St-Pierre AC, Ruel IL, Cantin B, Dagenais GR, Bernard PM, DespresJP, Lamarche B. Comparison of various electrophoretic characteris-tics of LDL particles and their relationship to the risk of ischemicheart disease. Circulation 2001;104:2295–9.
[8] Yamamoto K, Asakawa H, Tokunaga K, Watanabe H, Matsuo N,Tokimitsu I, Yagi N. Long-term ingestion of dietary diacylglycerollowers serum triacylglycerol in type 2 diabetic patients with hyper-triglyceridemia. J Nutr 2001;131:3204–7.
[9] Huge-Jensen B, Galluzzo DR, Jensen RG. Studies on free and im-mobilized lipases from mucor miehei. J Am Oil Chem Soc 1988;65:905–10.
10] Usui S, Hara Y, Hosaki S, Okazaki M. A new on-line dual enzymaticmethod for simultaneous quantification of cholesterol and triglycer-ides in lipoproteins by HPLC. J Lipid Res 2002;43:805–14.
11] Okazaki M, Usui S, Hosaki S. Analysis of plasma lipoproteins by gelpermeation chromatography. In: Rifai N, Warnick GR, Dominiczak MH,editors. Handbook of lipoprotein testing. 2nd ed. Washington, DC:American Association of Clinical Chemistry Press; 2000, p. 647–69.
12] Usui S, Nakamura M, Jitsukata K, Nara M, Hosaki S, Okazaki M.Assessment of between-instrument variations in a HPLC method forserum lipoproteins and its traceability to reference methods for totalcholesterol and HDL-cholesterol. Clin Chem 2000;46:63–72.
13] Patsch JR, Karlin JB, Scott LW, Smith LC, Gotto AM Jr. Inverserelationship between blood levels of high density lipoprotein subfrac-tion 2 and magnitude of postprandial lipemia. Proc Natl Acad SciUSA 1983;80:1449–53.
14] Ikeda Y, Ashida Y, Takagi A, Fukuoka T, Tsuru A, Tsushima M,
Yamamoto A. Mechanism of the production of small dense LDL (sLDL)in hypertriglyceridemia. In: Jacotot B, Mathe D, Fruchart JC, editors.Atherosclerosis XI. Singapore: Elsevier Science; 1998, p. 777–88.
15] Slyper AH. Low-density lipoprotein density and atherosclerosis. Un-raveling the connection. JAMA 1994;272:305–8.
16] Krauss RM. Dense low density lipoproteins and coronary arterydisease. Am J Cardiol 1995;75:53B–7.
17] Austin MA, Hokanson JE, Brunzell JD. Characterization of low-density lipoprotein subclasses: methodologic approaches and clinicalrelevance. Curr Opin Lipidol 1994;5:395–403.
18] Gardner CD, Fortmann SP, Krauss RM. Association of small low-density lipoprotein particles with the incidence of coronary arterydisease in men and women. JAMA 1996;276:875–81.
19] Stampfer MJ, Krauss RM, Ma J, Blanche PJ, Holl LG, Sacks FM,Hennekens CH. A prospective study of triglyceride level, low-densitylipoprotein particle diameter, and risk of myocardial infarction.JAMA 1996;276:882–8.
20] Hirano T, Yoshino G, Kazumi T. Troglitazone and small low-densitylipoprotein in type 2 diabetes. Ann Intern Med 1998;129:162–3.
21] Ribeiro-Filho FF, Faria AN, Azjen S, Zanella MT, Ferreira SR.Methods of estimation of visceral fat: advantages of ultrasonography.Obes Res 2003;11:1488–94.
22] Mertens I, van der Planken M, Corthouts B, Wauters M, Peiffer F, deLeeuw I, van Gaal L. Visceral fat is a determinant of PAI-1 activityin diabetic and non-diabetic overweight and obese women. HormMetab Res 2001;33:602–7.
23] Shimomura I, Funahashi T, Takahashi M, Maeda K, Kotani K, Naka-mura T, et al. Enhanced expression of PAI-1 in visceral fat: possiblecontributor to vascular disease in obesity. Nat Med 1996;2:800–3.
24] Nagao T, Watanabe H, Goto N, Onizawa K, Taguchi H, Matsuo N, etal. Dietary diacylglycerol suppresses accumulation of body fat com-pared to triacylglycerol in men in a double-blind controlled trial. JNutr 2000;130:792–7.
25] Maki KC, Davidson MH, Tsushima R, Matsuo N, Tokimitsu I,Umporowicz DM, et al. Consumption of diacylglycerol oil as part ofa reduced-energy diet enhances loss of body weight and fat in com-parison with consumption of a triacylglycerol control oil. Am J ClinNutr 2002;76:1230–6.
26] Kuriyama H, Yamashita S, Shimomura I, Funahashi T, Ishigami M,Aragane K, et al. Enhanced expression of hepatic acyl-coenzyme Asynthetase and microsomal triglyceride transfer protein messengerRNAs in the obese and hypertriglyceridemic rat with visceral fataccumulation. Hepatology 1998;27:557–62.
27] Taguchi H, Nagao T, Watanabe H, Onizawa K, Matsuo N, TokimitsuI, Itakura H. Energy value and digestibility of dietary oil containingmainly 1,3-diacylglycerol are similar to those of triacylglycerol. Lip-ids 2001;36:379–82.
28] Kondo H, Hase T, Murase T, Tokimitsu I. Digestion and assimilationfeatures of dietary DAG in the rat small intestine. Lipids 2003;38:25–30.
29] Cheng D, Nelson TC, Chen J, Walker SG, Wardwell-Swanson J,Meegalla R, et al. Identification of acyl coenzyme A: monoacylglyc-erol acyltransferase 3, an intestinal specific enzyme implicated indietary fat absorption. J Biol Chem 2003;278:13611–4.
30] Tada N, Watanabe H, Matsuo N, Tokimitsu I, Okazaki M. Dynamicsof postprandial remnant-like lipoprotein particles in serum after load-ing of diacylglycerols. Clin Chim Acta 2001;311:109–17.
31] Taguchi H, Watanabe H, Onizawa K, Nagao T, Gotoh N, YasukawaT, et al. Double-blind controlled study on the effects of dietarydiacylglycerol on postprandial serum and chylomicron triacylglycerolresponses in healthy humans. J Am Coll Nutr 2000;19:789–96.
32] Couillard C, Bergeron N, Prud’homme D, Bergeron J, Tremblay A,Bouchard C, et al. Postprandial triglyceride response in visceralobesity in men. Diabetes 1998;47:953–60.
33] Mekki N, Christofilis MA, Charbonnier M, Atlan-Gepner C, DefoortC, Juhel C, et al. Influence of obesity and body fat distribution onpostprandial lipemia and triglyceride-rich lipoproteins in adult
women. J Clin Endocrinol Metab 1999;84:184–91.