Embed Size (px)
Citation preview

Direct demonstration of small intestinal secretion and site-dependent absorption of the p-blocker talinolol in humans
Objective: To examine the relevance of site-dependent small intestinal absorption for incomplete intestinal absorption of the poorly metabolized P,-adrenergic receptor antagonist talinolol. Methods: The intestinal steady-state perfusion technique (triple lumen tubing system with a 30 cm test segment) for intraluminal measurements was combined with simultaneous determination of talinolol serum concentrations. Dissolved talinolol was perfused over 160 minutes into different parts of the small intestine. The middle of the test segment was located between 95 and 235 cm beyond the teeth. Each of the six healthy subjects was studied twice with a proximal and a more distal site of perfusion to allow for comparisons within an individual subject. Results: The area under the curve for serum concentrations from 0 to 480 minutes [AUC(O-480 min)] and the maximum serum concentration after distal perfusions corresponded to only 15% to 73% and 7% to 90% of the proximal values, respectively. AUC decreased with increasing distance from the teeth. The mean amount of talinolol absorbed from the test segment per unit time (intestinal transport rate) corresponds to only one-tenth of the amount of drug offered to the test segment (perfusion rate). There was a direct correlation between the perfusion rate of talinolol and its transport rate for both regions and in all subjects investigated. However, to achieve the same transport rate in the distal region a higher perfusion rate is required, compared to the proximal small intestine. At perfusion rates lower than 600 pg/min, net secretion of talinolol into the intestinal lumen occurred against a steep concentration gradient blood: lumen of about 1: 4200. Conclussion: Talinolol oral bioavailability of 55% is due to a low absorption rate and a decrease of absorption capabilities along the small intestine. Net absorption of talinolol is reduced by the involvement of active intestinal secretion. (Clin Pharmacol Ther 1996;59:541-9.)
Thomas Gramattk, MD, Reinhard Oertel, PhD, Bernd Terhaag, MD,” and Wilhelm Kirch, MD Dyesden, Gerunany
From the Institute of Clinical Pharmacology, Medical School, Technical University Dresden.
Supported by Arzneimittelwerk Dresden GmbH, Dresden, Ger- many.
Parts of this study were presented at the Third Annual Meeting of the Deutsche Gesellschaft fiir Klinische Pharmakologie und Therapie, Bad Nauheim, Germany, Sept. l-4,1993, and at the Thirty-sixth Spring Meeting of the Deutsche Gesellschaft fiir Experimentelle und Klinische Pharmakologie und Toxikologie, March 14-16, 199.5, Mainz, Germany.
Received for publication Sept. 19, 1995; accepted Dec. 13, 1995.
Reprint requests: Thomas GramattC, MD, Institut fiir Klinische Pharmakologie, Universitatsklinikum der Technischen Univer- sitit, Fiedlerstrasse 27, 01307 Dresden, Germany.
“Present address: Arzneimittelwerk Dresden GmbH, Dresden, Germany.
Copyright 0 1996 by Mosby-Year Book, Inc. 0009.9236/96/$5,00 + 0 13/l/71189
Talinolol [1-(4-cyclohexylureido-phenoxy)-2-hydroxy- 3-tert-butylaminopropane] is a long-acting, highly selec- tive P,-adrenergic receptor antagonist.‘,’ The drug (Cor- danum, Arzneimittelwerk Dresden GmbH, Dresden, Germany) has been frequently used in Germany and Eastern Europe since 1975 for the treatment of hyper- tension, coronav heart disease, and tachydysrhythmias at oral doses of 50 to 300 mg per day.
Talinolol is characterized by an intermediate lipid solubility (n-octanollwater-partition coefficient 12 at pH 7.4, 37” C) and a low water solubility (3.4 mmol/L at pH 7.4, 37” C)” compared with other P-blockers. Its low oral bioavailability of 55% (36% to 69%, 95% confidence interval) is not due to any relevant first-pass metabolism because more than 99% of the amount excreted by the kidneys after intravenous and oral administration was recovered unchanged in urine.4T5 We questioned whether the
541

542 GramattL et al. CLINICAL PHAiUIACOLOGY & THElV.1’EL’TIC.S
hIAY 1996
low bioavailability is attributed to a slow or site- dependent intestinal absorption. Consequently, tali- nolo1 absorption patterns from different regions of the small intestine were investigated. For our pur- poses the disappearance of talinolol from intestinal lumen and its appearance in the circulation (serum concentrations) were measured simultaneously by use of segmental intestinal steady-state perfusion technique in healthy volunteers.
METHODS
Subjects. Six healthy male volunteers participated in this open study. Their ages were between 25 and 29 years, weights between 65 and 90 kg, and heights between 175 and 193 cm. None of the subjects had a history of bowel or cardiovascular disease, and the results of liver and renal function tests were normal. Written informed consent was obtained, and the procedure used was approved by the Ethics Com- mittee of the Faculty of Medicine, Dresden, Ger- many.
Generalprocedure. The intestinal steady-state per- fusion studies were carried out in the standard fash- ion with use of a triple lumen technique6 modified as described recently.7-9 In brief, the tubes were pre- pared by fusing single polyvinyl tubes with tetrahy- drofuran. One lumen ended in a proximal (P) and another in a distal (D) aspiration port, located 15 and 45 cm distal to the perfusion port, respectively. The segment between the perfusion port and the proximal port is termed mixing segment; the segment between the proximal and the distal ports is called the test segment. Racemic talinolol (62.5 &ml) was dissolved in isotonic saline solution (pH, 7.6 to 8.0, 37” C) that contained 145 mmol/L sodium, 5 mmol/L potassium, 10 mmol/L bicarbonate, 140 mmol/L chloride and 3 gm/L polyethylene glycol 4000 (PEG) as a nonabsorbable marker. This per- fusate was infused continuously into the intestine through the perfusion port at 10 ml/min. Each per- fusion lasted for 160 minutes, resulting in an admin- istered dose of 100 mg.
After an equilibration period of 70 minutes, six serial intestinal samples of 15-minute intervals were collected by continuous aspiration at 1.5 ml/min from the proximal and distal ports (aspi- rates Nos. Pl through P6 and Dl through D6, respectively). Sampling from the distal port was delayed by 15 minutes (i.e., staggering), with the intention to sample the same portion of the fluid column as it passed each aspiration port. There- fore a total of five calculations (PlD2 through
P5D6) could be performed for each perfusion. For serum concentration-time profiles, the intes- tinal perfusion procedure described was combined with simultaneous determination of serum con- centrations of talinolol.
Study design. Studies were performed on 2 succes- sive days during which the tube was left in the small intestine. On the first study day subjects swallowed the tube after an overnight fast. The middle of the test segment was positioned 95 to 115 cm beyond the teeth. The correct orthograde passage of the tube from the stomach into the duodenum was moni- tored by measurement of pH change in aspirates from each of the three tube openings. Further progress of the tube was monitored by consecutive appearance of bile-stained intestinal aspirate. Once the tube had reached the desired distance from the teeth, the perfusion was started after tube slacking had been removed. Two hours after the first perfu- sion study the subjects were permitted to eat semo- lina pudding. The tube was left in the intestine and was allowed to move distally under the influence of peristalsis. On the next day, 20 hours after beginning the first perfusion, a second identical procedure was carried out with the middle of the test segment located between 160 and 235 cm beyond the teeth. In this way comparisons of proximal (day 1) with the more distal perfusion study (day 2) were possible within the same subject (for individual locations of the tubes see Table I). No fluoroscopy was per- formed because the exact anatomic location of the tube was not of primary interest. It was important that the tube was positioned more distally on day 2 compared with its position on day 1. In subject 6, no aspiration of intestinal fluids was practicable be- cause of technical difficulties, therefore only serum concentration-time profiles will be reported.
Blood samples (8 ml) were taken before the start of perfusion, at intervals of 10 to 20 minutes up to the end of perfusion (160 minutes), and at intervals of 20 to 60 minutes up to 480 minutes. At least four additional blood samples were taken between 480 minutes after the beginning of the first perfusion and the start of the second perfusion.
Calculations and statistics. For the intestinal per- fusions, steady-state conditions along the test seg- ment were assumed if the concentrations of the marker (PEG) remained nearly constant at both aspiration ports during the six sampling periods, that is, ranging within 520% of the median PEG concentration. Net transport rates were calculated by standard nonabsorbable marker equations”

CLINICAL PHARMACOLOGY & THERAPEUTICS VOLUME 59, NUMBER 5 GraunattL et al. 543
Table I. Individual comparison of pharmacokinetic parameters derived from serum concentrations of talinolol
Subject No.
Location of the AUC perjksion port (proximal/distal)
(cm) * (ng * hriml)
AUC (distal) (70 of the proximal
value)
C (proxim~~distal)
hW)
C,, (distal) (70 of the proximal
value)
1 701135 2111155 73 68/38 56 2 70/180 104159 57 32114 44 3 751165 2141151 71 48143 90 4 751205 96158 60 23112 52 5 851160 257188 34 61120 33 6 651230 253137 15 8216 7
*Distance of the perfusion port from the teeth during the proximal/distal perfusion. AUC. Area under the curve for serum concentrations from 0 to 480 minutes; C,,,,, maximum serum concentration
(for further details see Gramatte and Richters). Accordingly, transepithelial talinolol transport along the test segment (kg/30 cm . min) was ex- pressed as the difference between the amount of talinolol entering the test segment per unit of time and that leaving it. Positive transport rates indi- cated that talinolol had disappeared from the test segment (i.e., absorption), and negative values indicated that more talinolol had left the test segment than had entered (i.e., secretion). The rate of net fluid absorption (ml/30 cm * min) was determined from the differences between the PEG concentrations in the perfused solution and in the aspirates.
The amount of talinolol entering the test segment per unit of time @g/min) is termed the pe&sion rate” of talinolol (Perfusion rate = Fluid volume entering the test segment X concentration of talino- 101 in this fluid). This parameter describes the actual talinolol load reaching the test segment.
The calculated transport rates of talinolol were checked for linear correlation to the perfusion rates and for a correlation to the rates of net fluid absorp- tion. In addition, conventional partial correlation coefficients (rpartia,) were determined’* for the rela- tionships between the following two pairs of vari- ables: (1) talinolol perfusion rate and transport rate (the effect of net fluid absorption was held constant) and (2) rate of net fluid absorption and talinolol transport rate (the effect of the talinolol perfusion rate was held constant). Simultaneous effects of the talinolol perfusion rate and net fluid fluxes on the talinolol transport rate were verified by multiple correlation analysis” (rmuitipie). The transport rate of talinolol was considered to be the dependent variable in all correlations performed. Normality
assumptions were verified to be adequate for the data used in these correlations with Kolmogorov- Smirnov goodness of fit test.‘*
The area under the curve for serum concentra- tions from 0 to 480 minutes [AUC(O-480 min)] was calculated from raw data with use of the linear trapezoidal rule. Maximum serum concentration (C,,,) and the time to reach C,,, (t,,,) were noted directly from the data. Serum concentrations on day 2 were corrected for the residuals of the day 1 perfusion by extrapolation from the decay of con- centrations, according to the elimination rate con- stant calculated from the log-linear regression of the terminal phase of the concentration versus time plot resulting from the first perfusion.
Statistical analysis was performed with the SPSS for Windows computer package (version 5.01, 1992; SPSS Inc., Chicago, Ill.). Data are expressed as mean +- SD and the range, respectively. Compari- sons of mean values were made using Mann and Whitney’s U test. Results were compared with re- gard to the different perfusion sites. Statistical sig- nificance was set a priori at p < 0.05.
Analytical procedures. Serum and intestinal aspi- rates were analyzed for unchanged talinolol by a specific and sensitive HPLC assay.5 In addition, in- testinal samples were screened for hydroxylated tali- nolo1 metabolites.5 PEG concentration in each in- testinal aspirate was determined turbidimetrically.13 Sample volume and pH of all intestinal aspirates were measured. Talinolol instability and adsorption to the tube wall were excluded by prestudy investi- gations. Furthermore, pooled aspirates were sub- jected to equilibrium dialysis14 to examine binding of talinolol to any macromolecular constituents of intestinal content.

544 Gramutt~ et al. CI.1NIC.U PHAKhWCOLOGY & THERAPEL’TICS
hi?.Y 19’96
Table II. Results of talinolol perfusion studies within different regions of the small intestine (mean 2 SD; n = 25 for each region)
Location of the test segment* PH
Net fluid Pet-j&ion rate of absorption rate talinolol
(ml130 cm * min) (CLglmW
Transport rate of talinolol
(~I30 cm * min) f
Proximal perfusions 6.79 -c 0.26 1.30 ? 0.60 573 t 41 34.4 -c 59.0 (-80 to 152) (95-115 cm)
Distal perfusions 7.27 2 0.35$ 1.88 2 0.823: 640 k 53$ 39.4 ? 67.4 (-97 to 145) (160-235 cm)
*Distance of the middle of the test segment from the teeth. ?Values signed negatively represent net secretion of talinolol into the gut lumen @I < 0.05 compared with the mean of the proximal perfusions.
RESULTS No side effects attributable to the intubation or
the direct delivery of dissolved talinolol into the bowel were observed.
Zntestinalperfusion studies. The pH of the aspirates increased significantly with intestinal depth (an av- erage of pH 6.9 at 80 cm to pH 7.5 at 250 cm beyond the teeth; Table II), giving an additional hint for proper position of the tubes according to data re- ported by Evans et al.” and Goebell et aLi6 There was no binding of talinolol to any macromolecular constituents of intestinal fluids, as shown by equilib- rium dialysis of 10 pooled samples. Because no hy- droxylated talinolol metabolites were detectable in the aspirates, all talinolol perfused into the intesti- nal lumen was potentially available for absorption. Disappearance of talinolol from the test segment was therefore not caused by metabolism.
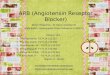
Steady-state conditions along the test segment could be assumed for all perfusions. There was a significantly higher talinolol perfusion rate in the distal study compared with the proximal one for each subject (Fig. 1; see the mean values in Table II). This was attributable to higher fluid volumes entering the test segment per unit of time. Mean talinolol concentrations at the entrance of the test segment were similar during the proximal and distal perfusions (67 + 6 &ml and 68 t 15 p&ml). Mean fluid absorption was significantly more intensive during distal perfusions (Table II). The mean tali- nolo1 transport rates were similar for both intestinal regions investigated (Table II).
The talinolol transport rates were linearly related to the perfusion rates (proximal: r = 0.72; p < 0.01; distal: r = 0.59; p < 0.01). These correlation coeffi- cients remained significant when partial correlation analysis was applied that eliminated the rate of fluid absorption as a potential factor influencing the
transport rate of talinolol simultaneously (rpartial = 0.69 and 0.50, respectively; p < 0.02). The correla- tion between the perfusion rate of talinolol and its transport rate was also found to be valid in the individual evaluations: In 9 of 10 perfusions Spear- man’s rank correlation coefficient was 20.9. How- ever, in each distal perfusion there was a parallel shift of this relationship toward higher perfusion rates (Fig. 1); that is, to achieve the same talinolol transport rate in the distal region a higher perfusion rate is needed, compared to the proximal intestine. Despite higher perfusion rates in the distal regions, there were no higher talinolol transport rates (Table II). Accordingly, the comparison of the results within each individual subject indicated site- dependent transepithelial transport of talinolol.
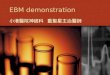
There was a significant positive correlation be- tween the fluid absorption rate and the transport rate of talinolol in the distal regions investigated. This was shown by partial correlation analysis that eliminated the predominant effect of the perfusion rate on the transport rate (Ypartial = 0.65; p < 0.01). Moreover, multiple regression analysis, considering both the perfusion rate and the rate of fluid absorp- tion as variables determining the transport rate of talinolol in the distal small intestine, revealed the effect of fluid fluxes to be high: From the multiple regression equation it follows that the transport rate is modified by 47 t&30 cm . min if the rate of fluid absorption changes by 1 ml/30 cm * min (Tmul~iple = 0.79; p < 0.01). This modification of the talinolol transport rate corresponds to about 120% of the mean value calculated for this region. Fig. 2 shows the respective three-dimensional plot of the perfu- sion rate and the fluid absorption rate versus talino- 101 transport rate.
During six perfusions a total of 12 negative trans- port rates arose (five single values resulting from the

CLINICAL PHARMACOLOGY & THEBAPEUTICS VOLUME 59, NUMBER 5 Grmnuttti et al. 545
talinolol transport rate @g/30cm*min) 150
. l
loo- .
.
50- . .
. 0 f?.
I ’ subject 1 1 subject 2 -50
520 570 620 -100’ I
670 540 590 640
talinolol transport rate @g/30cm*min)
tallnolol perfusion rate wg/min)
talinolol transport rate @ig/30cm*min)
15oc . I
I . v
50 v I
.
-50 570
.
620 670
subject 3
720
talinolol perfusion rate @g/min)
talinolol perfusion rate wg/min)
talinolol transport rate @gPOcm*min)
iooy
::I’ ’ subject4
520 570 620 670 720
talinolol perfusion rate @g/min)
Fig. 1. Comparison of the relation between talinolol perfusion rate and its intestinal transport rate (Spearman’s rank correlation coefficients ~0.9) for the proximal (ttiang~es) and the more distal perfusion (circles). In subject 5 this relation was found only for the distal results. Negative transport rates represent net secretion of talinolol into the intestinal lumen.
proximal perfusions in subjects 2 and 4, respectively, and seven single values resulting from the distal studies in subjects 1, 2, 3, and 4, respectively). This indicated net secretion of talinolol into the test seg- ment. According to a plot of all transport rates measured during these six perfusions, it is deduced that net secretion predominates at perfusion rates lower than about 550 to 600 pg,/min (Fig. 1). This is emphasized for the results of the distal perfusions by the three-dimensional plot in Fig. 2. Accordingly, net secretion into the distal small intestine occurred if both the perfusion rate and the fluid absorption rate were low. Extrapolating the mean of the secre- tion rates measured (-44 t~8/30 cm * min; range, -97 to -14 kg/30 cm * min) to a small intestinal length of 250 cm results in a net amount of about 22 mg that might be secreted per hour. During the occurrence of net secretion the mean intraluminal talinolol concentration (measured in the aspirates from the proximal port) were about 4200-fold higher than the corresponding mean serum concentrations.
Serum concentration-time profiles. All perfusions resulted in measurable serum concentrations of tali- nolol. At the beginning of the second perfusion there was residual concentration detectable in each subject (15.2 +- 5.6 r&ml; n = 6). For each subject there was no difference of serum concentrations at the beginning of aspirate sampling during both per- fusions (2 to 33 q/ml).
AUC and C,,, varied depending on the location of the perfusion port (Table I, Fig. 3). AUC(O-480 min) values after distal perfusions correspond to only 15% to 73% of the proximal AUC (Table I). Distal AUC values decreased with increasing dis- tance from the teeth (Spearman’s rank correlation coefficient -0.94; n = 6). C,,, values paralleled the AUC results: They were reduced distally to 7% to 90% of the proximal values (Table I). The lowest AUC and C,,, values were observed after adminis- tration into regions deeper than 180 cm beyond the teeth. C,,, occurred 50 to 110 minutes (proximal perfusions) and 80 to 140 minutes (distal perfusions)

546 Gmmatt~ et al.
150 1’
100
50
0 I.
-50
transport rate
4 4, 0
perfusion rate ‘“” 750 fluid absorption rate
Fig. 2. Three-dimensional plot of the multiple correla- tion between talinolol perfusion rate (in micrograms per minute), fluid absorption rate (ml/30 cm * min), and the talinolol transport rate (p&30 cm * min) in the distal small intestine (rmultiple = 0.79; p < 0.01). Talinolol secretion rates (i.e., negative transport rates) are depicted by solid circles.
after the end of perfusion (Fig. 3), resulting in t,, values between 210 and 270 minutes and 240 and 300 minutes, respectively.
Although the position of the perfusion port dur- ing the proximal perfusions varied only between 65 and 85 cm beyond the teeth (Table I), there was considerably intersubject variability of AUC and C,,, values (Table I; Fig. 3). For example, the AUC and C,, values of subjects 2 and 4 corresponded to only 50% of the mean value of the other volunteers.
DISCUSSION This is the first report on direct demonstration of
secretory transport of a P-blocker in the human intestine in vivo. The results also show site- dependent small intestinal absorption of the &- adrenergic receptor antagonist talinolol in humans. This is shown by both intraluminal measurements and by serum concentration-time profiles. Despite the small number of subjects included, the results obtained seem to be reliable because of the paired study design and the uniformity of differences ob- served within each individual subject.
Because of the scattering of the perfusion sites along the small intestine, it could be shown that the
CLINICAL PHAlWlACOLOGY&THERAPEUTICS LMAY 1996
amount absorbed (AUC) may decline considerably along quite short distances within the small intes- tine. This conclusion is reliable because the drug was placed initially at different intestinal regions and by this exclusion of different parts the absorption from successive sites could be compared. Accordingly, dropping absorption along the small intestine may be responsible for incomplete bioavailability of tali- nolo1 and its variability of absorption kinetics ob- served after oral administration.4 Comparable to our results, the incomplete bioavailability of the very hydrophilic and poorly metabolized P-blockers atenolol and nadolol might also be caused by site- dependent intestinal absorption.17 In contrast, the rate and extent of intestinal absorption of the more lipophilic metoprolol was shown to be constant along the whole intestinal tract.18’19
Our results suggest that drug or disease factors that accelerate small intestine transit may decrease the bioavailability of talinolol. Accordingly, a signif- icant reduction of the relative bioavailability of tali- nolo1 tablets after concomitant food intake has been reported.”
The site dependency of talinolol absorption could be deduced from the intraluminal results only by comparing data within individual subjects and by relating the individual transport rates to the amounts of talinolol entering the test segment (i.e., the perfusion rates). For each of these comparisons this approach clearly revealed that in the proximal small intestine a lower talinolol load (perfusion rate) is necessary to achieve a transport rate similar to the rate of the distal region.
The overall permeation process of talinolol was found to be slow because the mean amount ab- sorbed along the test segment corresponds to only one-tenth of the amount that had entered it. Tali- nolo1 is a weak base (pKa 9.43) and therefore it should exist mainly (more than 99%) as a cation at the pH measured intraluminally. This might hinder a rapid permeation across the transcellular pathway. Low absorption rate is also indicated by the delay in the occurrence of peak serum levels (50 to 140 minutes after the end of perfusion).
Although there was constant drug supply to the intestine, there was no continuous increase of the serum concentration during the time of drug perfu- sion. However, plateaus and distinct drops occurred occasionally, especially during the proximal perfu- sions (double-peaked blood levels; Fig. 3). Accord- ing to our results, different as well as changing fluid fluxes along quite short distances of the human

CLINICAL PHARMACOLOGY &THERAPEUTICS VOLUME S9, NUMBER 5 Gruvnatt~ et al. 547
-0 60 120 180 240 300 360 420 480 time (mid
concentration (nglml)
-0 60 120 180 240 300 360 420 460 0 60 120 180 240 300 360 420 480 time (mid time (mid
concentration (nglml)
20 subject 4 A
60 120 180 240 300 360 420 480 time (mid
concentration he/ml)
80.
70.
60-
50-
40-
30-
subject 6
Fig. 3. Typical serum talinolol concentration-time profiles after a 160-minute perfusion of dissolved talinolol into different parts of the small intestine. Numbers under the curves correspond to the position of the perfusion site (in centimeters beyond the teeth). Note different scaling on the concentration axes.
small intestine’ should be taken into account as one possible reason for discontinuous absorption, result- ing in irregular serum concentration profiles. In the distal regions, talinolol will be absorbed more rap- idly when fluid is being absorbed along with the drug. Accordingly, talinolol absorption from the most proximal small intestine gives rise to initial peak levels in blood. Subsequently the remaining drug might pass regions that just absorb fluid more extensively. In this way a second distal absorption site would arise functionally, causing an additional peak.
In accordance with the present results, we also observed the intestinal absorption rate of griseoful- vin (a drug with extremely low aqueous solubility) to be correlated with fluid fluxes in the distal small intestine only.” A linkage between fluid fluxes and drug absorption rate is known as solvent drag phe- nomenon.21 The present results emphasize that there are local differences in the effectiveness of this mechanism in the human small intestine7 and that
solvent drag does not affect only hydrophilic drug absorption, as supposed originally.
Talinolol serum concentrations resulted not only from talinolol transport within the test segment but also from the transport at regions beyond the test segment (due to incomplete recovering of the per- fusion solution). Therefore the intraluminal results should not be simply related to serum concentra- tions. Nevertheless, intraluminal results are re- flected by serum concentrations: The extent of ab- sorption decreased markedly with increasing distance of the perfusion site from the teeth, indi- cating the proximal small intestine as the favorite region for talinolol absorption.
Surprisingly, in one-fifth of the measurements the amount of talinolol leaving the test segment was greater than the amount that had entered it. This clearly indicates net secretion (exsorption) of talino- 101 from the circulation into the intestinal lumen. Under the conditions established due to our perfu- sion procedure, a net secretion occurred without

548 Gramattt! et al. CLINICAL PHARMACOLOGY &THERAPEUTICS
MAY 1996
exception below a minimum load of talinolol enter- ing the test segment per unit of time (i.e., below a minimum perfusion rate). Extrapolating the mean secretion rate to the whole length of the small bowel (about 250 cm) results in an net amount secreted per hour that corresponds to more than 40% of the amount absorbed (supposing an oral bioavailability of 50%). This quantity is indicative for an efficient blood-to-lumen transport of talinolol. It has to be taken into account that during the measurements of these secretion rates the intraluminal talinolol con- centrations were about 4200-fold higher than the corresponding serum concentrations. Therefore an active mechanism of talinolol excretion is likely to be involved.
Drug elimination from the general circulation, through nonbiliary pathways, into the intestinal lu- men has seldom been considered to be important. However, intestinal secretion of other organic cat- ions, including P-blockers (acebutolol,22 pafeno- 101,~~ and celiprolo124), has been shown in animals (in vivo and in vitro). Recently we demonstrated small intestinal secretion of the basic drug ranitidine in humans by use of the same procedure described here.7 Moreover, active secretion of celiprolol and, very recently, talinolol was observed in monolayers of human intestinal epithelial cell line (taco-2), and it was proposed that the multidrug resistance gene product (P-glycoprotein) is involved in this transport pathway.25326 Obviously, the recirculation of drugs through the intestinal mucosa is more common than currently believed.
Intestinal secretion of talinolol should be dis- cussed as one reason for the incomplete bioavail- ability of talinolol and for the nonlinear relationship between oral doses and AUC values described re- cently.27 In this context, it seems worth mentioning that the occurrence of talinolol secretion during proximal perfusions (subjects 2 and 4) was accom- panied by extremely low AUC values (Table I), compared with the other subjects. Our results un- derline the potential relevance of site-dependent and secretory intestinal transport for the absorption kinetics of drugs that show incomplete or nonlinear oral bioavailability.
References 1. Haustein KO, Fiehring H, Oltmanns G, Femmer K.
On the clinical pharmacology of talinolol, a new beta l-adrenoceptor blocking agent. Int J Clin Pharmacol Biopharm 1979;17:465-70.
2. de Mey C, Schroeter V, Roll S, et al. Clinical phar-
macology of talinolol, a B-adrenoceptor antagonist with high relative B,-adrenoceptor selectivity in man [Abstract]. Naunyn Schmiedebergs Arch Pharmacol 1994;349:R143.
3. le Petit G. Die pH-abhangige Lipoidloslichkeit bei Arzneimittelgruppen. Pharmazie 1985;40:797-8.
4. Trausch B, Oertel R, Richter K, Gramatte T. Dispo- sition and bioavailability of the B,-adrenoceptor an- tagonist talinolol in man. Biopharm Drug Dispos 1995;16:403-14.
5. Oertel R, Richter K, Trausch B, Bemdt A, Gramatte T, Kirch W. Elucidation of the structure of talinolol me- tabolites in man: determination of talinolol and hydroxy- lated talinolol metabolites in urine and analysis of tali- nolo1 in serum. J Chromatogr 1994;660:353-63.
6. Cooper H, Levitan R, Fordtran JS, Ingelfinger FJ. A method for studying absorption of water and solute from the human small intestine. Gastroenterology 1966;50:1-7.
7. Gramatte T, El Desoky E, Klotz U. Site-dependent small intestinal absorption of ranitidine. Eur J Clin Pharmacol 1994;46:253-9.
8. Gramatte T, Richter K. Paracetamol absorption from different sites in the human small intestine. Br J Clin Pharmacol 1994;37:608-11.
9. Gramatte T. Griseofulvin absorption from different parts in the human small intestine. Biopharm Drug Dispos 1994;15:747-59.
10. Fordtran JS, Rector FC, Ewton MF, Soter N, Kinney J. Permeability characteristics of the human small intestine. J Clin Invest 1965;44:1935-44.
11. Modigliani R, Rambaud JC, Bernier JJ. The method of intraluminal perfusion of the human small intes- tine; I: principle and technique. Digestion 1973;9:176- 92.
12. Snedecor GW, Cochran WG. Statistical methods. 7th ed. Ames, Iowa: University Press, 1980:334-64.
13. Malawer SJ, Powell DW. An improved turbidimetric analysis of polyethylene glycol utilizing an emulsifier. Gastroenterology 1967;53:250-6.
14. Scholtan W. Bestimmungsmethoden und Gesetzmas- sigkeiten der Serumproteinbindung von Arzneimit- teln. Arzneimittelforschung 1978;28:1037-47.
15. Evans DF, Pye G, Bramley R, Clark AG, Dyson TJ, Hardcastle JD. Measurement of gastrointestinal pH profiles in normal ambulant human subjects. Gut 1988;29:1035-41.
16. Goebell H, Klotz U, Nehlsen B, Layer P. Oroileal transit of slow release 5aminosalicylic acid. Gut 1993; 34:669-75.
17. Taylor DC. Sites and mechanisms of intestinal drug absorption. Pharm Int 1986;7:179-83.
18. Vidon N, Evard D, Godbillon J, et al. Investigation of drug absorption from the gastrointestinal tract of man; II: metoprolol in the jejunum and ileum. Br J Clin Pharmacol 1985;19(suppl):107S-12s.

CLINICAL PHARMACOLOGY & THERAPEUTICS \‘OLUMI; 59, NUMBER 5 G~amattti et al. 549
19. Godbillon J, Evard D, Vidon N, et al. Investigation of 24. Kuo SM, Whitby BR, Artursson P, Ziemniak JA. The drug absorption from the gastrointestinal tract of contribution of intestinal secretion to the dose- man; III: metoprolol in the colon. Br J Clin Pharma- dependent absorption of celiprolol. Pharm Res 1994; co1 1985;19(suppl):113S-8s. 11:648-53.
20. Terhaag B, Sahre H, Lange I-J, Richter K, Feller K. Zum Einfluss der Nahrung auf die Absorption von Talinolol (Cordanum) am gesunden Probanden. Z Klin Med 1991;46:1021-3.
21. Ochsenfahrt H, Winne D. The contribution of solvent drag to the intestinal absorption of the basic drugs amidopyrine and antipyrine from the jejunum of the rat. Naunyn Schmiedebergs Arch Pharmacol 1974; 281:175-96.
25. Karlsson J, Kuo SM, Ziemniak J, Artursson P. Trans- port of celiprolol across human intestinal epithelial (Caco-2) cells: mediation of secretion by multiple transporters including P-glycoprotein. Br J Pharmacol 1993;110:1009-16.
22. George CF, Gruchy BS. Elimination of drugs by active intestinal transport. J Pharm Pharmacol 1979;31:643-4.
23. Lennerngs H, Reglrdh CG. Dose-dependent intesti- nal absorption and significant intestinal excretion (ex- sorption) of the beta-blocker pafenolol in the rat. Pharm Res 1993;10:727-31.
26. Wetterich U, Mutschler E, Spahn-Langguth H, Lang- guth P. Evidence for intestinal secretion of the p-adrenoceptor antagonist talinolol: data from hu- mans and studies with Caco-2 cells [Abstract]. Nau- nyn Schmiedebergs Arch Pharmacol 1995;351(suppl): Rl.
27. Wetterich U, Spahn-Langguth H, de Mey C, et al. Pharmacokinetics of talinolol enantiomers after oral racemate dosage [Abstract]. Naunyn Schmiedebergs Arch Pharmacol 1994;349(suppl):R150.
U TUE MOVE? Don’t miss a single issue of the journal! To ensure prompt service when you change your address, please photocopy and complete the form below.
Please send your change of address notification at least six weeks before your move to ensure continued service. We regret we cannot guarantee replacement of issues missed due to late notification.
JOURNAL TITLE: Fill in the title of the journal here.
OLD ADDRESS: NEW ADDRESS: Affix the address label from a recent issue of the journal here. Clearly print your new address here.
Name
Address
City/State/ZIP
COPY AND MAIL THIS FORM TO: Journal Subscription Services Mosbv-Year Book, Inc. 1183O”Westline Industrial Dr. St. Louis, MO 63146-3318
OR FAX TO: 314-432-1158
OR PHONE: l-800-453-4351 Outside the U.S., call 314-453-4351