Embed Size (px)
DESCRIPTION
tdrt
Citation preview

F.A.S.T.H.U.G I W. Aryabiantara

F.A.S.T.H.U.G
It’s a mnemonic memudahkan seorang praktisi medis dalam memberikan terapi (Jean-Louis Vincent)•F = Feeding•A = AnalgetiK•S = Sedasi•T = tromboemboli profilaksis•H = Head of bed elevasi•U = Ulcer proteksi•G = Glucouse kontrol

FEEDING
• Berikan nutrisi se-segera mungkin setelah resusitasi stabil
• Ideal <72 jam• Nutrisi dini menurunkan angka kematian secara
signifikan• Bisa enteral bisa parenteral

Postprandial Hypotension
Liver
Stomach
Spleen
Pancreas
Smallintestine
ColonAorta
HepaticPortalveinI
300
S
500
200
C
H700
500 1000
From Review of medical physiology, Ganong WF. 2001
Meal400
VASODILATATION
Decrease Venous Returndecrease Stroke Volumedecrease Blood Pressure
vasodilatation
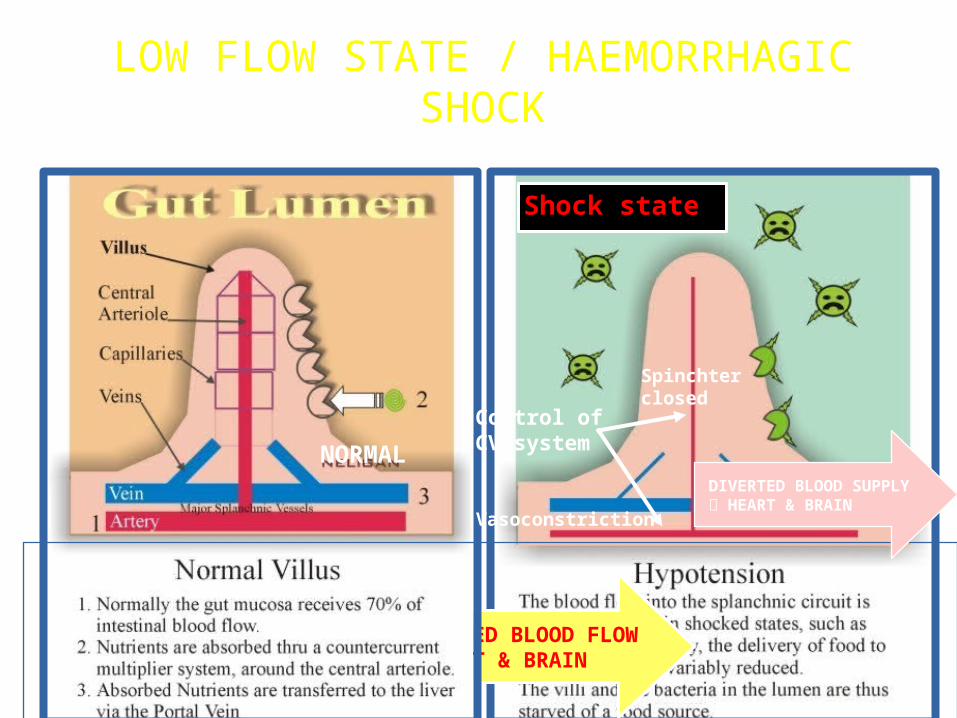
Shock state
DIVERTED BLOOD FLOW HEART & BRAIN
Control of CV system
Spinchterclosed
Vasoconstriction
NORMALDIVERTED BLOOD SUPPLY HEART & BRAIN
LOW FLOW STATE / HAEMORRHAGIC SHOCK

FEEDINGFEEDING

Endogenous vasoconstrictor
2. Ischaemia-Reperfusion injury
Splanchnic Hypoperfusion
1. Gut mucosal barrier disruption
Increased mucosal permeability to bacteria / endotoxin
SIRS MODS
Cardiac failure:- AMI- CHF- Tamponade
Hypovolaemia:- Dehydration- Hemorrhage
Gut mucosal hypoperfusion
Cytokine/ROS
Resuscitation
Gareth Ackland, Michael PW Grocott and Michael G Mythen: Crit Care 2000, 4:269–281
Exogenousvasoconstrictor:NE, Epi, Dopa
The ‘gut-origin hypothesis’



ANALGESIA
• Dasar : nyeri adalah vital sign yang ke-5• Pasien dalam kondisi apapun tidak boleh nyeri• Rangsangan nyeri tersebut dapat mempengaruhi
pemulihan fisiologis dan psikologis kurang tidur, disfungsi paru dan respon stres imunosupresi, hiperkoagulabilitas, katabolisme protein dan meningkatkan oksigen miokard consumption

Repeated episodes of acute pain, localised Surgery / tissue inflammation / immobility Catheter/ apparatus discomfort / naso & orogastric
tubes Endotracheal intubation/ suctioning/ chest tubes Phlebotomy / vascular access / physiotherapy Routine turning & positioning the patient
Source of Pain in ICU

Emergency intubation
Sometimes use only sedation and relaxan
Local anesthetic so
metimes ineffective
Local anesthetic so
metimes ineffective

The most painfull..R
outine turning

Receiving Beta Bloker
Vitals was normal

Critical clinical practice guidelines;
pain assesment and response to therapy should be performed on a regular basis using a scale appropriate to the patient population.
The use of VAS and NRS is recommended
For patients who cannot communicate, pain should be assessed through subjective observation of;
Pain related behaviour
Physiological indicators
Assessment of pain in ICU

Pain Rating ScaleVisual Analogue ScaleNumeric Rating ScaleFaces ScaleMcGill Pain Questionnare
Assessment of pain in ICU

Assasement nyeri



Pharmacologic Management of pain in the ICU
Textbook critical care, M. Fink 2006

Fentanyl: Golden Standard for H
emodynamic stability


SEDASI


TROMBOEMBOLI PROFILAKSIS

Cara Mekanik :
• Perubahan posisi berbaring secara berkala, • Pijat rutin pada tungkai bawah• Early mobilisasi pada pasien sadar • Graduated compression stockings (GCS), • Intermittent pneumatic compression (IPC)
devices • Venous foot pump (VFP).
Terapi medikamentosa :
• dapat berupa Heparin 5000 Unit setiap 8 jam• Enoxaparin 30 Unit setiap 12 jam• Dalteparin 2500 - 5000 Unit setiap 24 jam• Fondaparinux 2,5 mg setiap 24 jam

Head of The Bed Up
• Kemiringan bed 45 derajat• Mencegah regurgitasi• Salah satu komponen bundle pencegahan VAP• Pressure cuff dijaga < 20 mmHg• Sub glotic suction, oral hygiene
ULCER PROTEKSI• H2 Antagonists seperti Cimetidine 300 mg oral
atau IV setiap 6-8 jam• Famotidine 20 mg oral atau IV setiap 12 jam, • Ranitidine 50 mg IV setiap 12 jam• Penghambat pompa proton seperti Lanzoprazole
30 mg setiap 24 jam, omeperazole 20 mg setiap 24 jam atau Pantoprazole 40 mg setiap 24 jam,
• Sucralfat 10 mg setiap 6 jam

Glucosa Control-Hyperglicemia meningkatkan morbiditas, mortalitas dan biaya perawatan.-Dengan mengontrol gula darah akan menurunkan insidens penyembuhan luka yang lama, resiko infeksi, gangguan motilitas usus, gangguan performa kardiovaskuler, resiko polineuropati dan resiko gagal ginjal akut.

- Target gula darah idealnya dipertahankan dilevel 140-180 mg/dL.-Strategi mempertahankan gula darah :Insulin continuous dapat dijalankan setelah 2 kali pemeriksaan dengan interval 1 jam, masih menunjukkan > 180 mg/dL (kadang-kadang memerlukan insulin bolus sebelumnya). Insulin yang digunakan yg short actingHindari penggunaan sub kutan jika hemodinamik pasien belum stabil


Ventilator Bundle
• Patient positioning Elevation Recommended elevation is 30-45 degrees
• Ventilator weaning Periodic “sedative interruptions” and daily assessment of readiness to extubate may reduce the duration of mechanical ventilation and the risk of VAP

ICU Bundle
• Peptic ulcer disease (PUD) prophylaxis Patients with respiratory failure have an increased risk of “stress ulcers” and associated gastrointestinal (GI) bleeding.
• Venous thromboembolism prophylaxis Patients with respiratory failure have an increased risk of deep vein thrombosis. Treatment with anticoagulants (e.g., heparin) has been shown to reduce this risk.






























