Embed Size (px)
Citation preview

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 1/37
Graft vs. Host
Disease
(GVHD)
Prepared by : Muhammad Abdullah3rd Year MBBS
Batch#15Roll#22

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 2/37
Transplantation:
To transfer (an organ, tissue, etc.) from one part of the
body to another (Auto graft) or from one person or animal
to another (Allograft).

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 3/37
Steps:
Histocompatibility of Donor
Suppression of host immune system
Replacement
Clinical supervision (e.g. to make sure the
accommodation of graft , to inhibit infections , etc)

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 4/37
Examples of Transplantation: K idney transplant
Corneal transplant
Bone marrow transplant
Coronary artery bypass
Liver transplantation
etc.

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 5/37
Graft:
A portion of living tissue sur gically tra ns pla nted fr om
one part of a n individual to a nother, or fr om one
individual to a nother, f or its adhesion a nd gr owth.
E.g.: Cor neal graft, Skin graft , etc

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 6/37
Use of Grafting:
Cosmetic use (e.g. skin grafting)
To inhibit a tissue Damage (e.g. coronary artery bypass)
To replace a damaged part (e.g. corneal grafting)
To treat malignant or non-malignant conditions (e.g. bone
marrow transplantation )

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 7/37
Graft vs. Host Disease(GVHD):
Graft-versus-host disease (GVHD) is a common
complication of allogenic bone marrow transplantation
in which functional immune cells in the transplanted
marrow recognize the recipient as "foreign" and mount
an immunologic attack.

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 8/37
Causes:1) Non-histocompatible transplantation
2) Over immuno-suppression of recipient

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 9/37
Pathogenesis:
T-cells of allograft take host as foreign
T-cells of graft attack the host tissues
Secrete excess of cytokines including TNF-, INF- & IL-2
CD4+ T cells are crucial for sustaining the secondary
expansion of CD8+ T cells

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 10/37
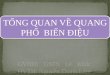
Interaction of factors involved in graft versus host disease (GVHD).Cytokines, such as interleukin-2, tumor necrosis factor-alpha, andgamma interferon, play an important role in the initiation andpropagation of GVHD.

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 11/37

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 12/37
SkinMost often involvedMaculopapular rashPalms and soles initially
LiverH yper-bilirubinemia and increased alkaline phosphatase
GIManifests as diarrhea
Upper GI symptoms - nausea, anorexiaSevere cases - ileus, cramping pain, bleeding
Upper GI tract / oral mucosaRenal (rarely)Eye

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 13/37
F orms of GVHD:
1- H yper Acute Graft vs. Host Disease (haGVHD)2- AcuteGraft vs. Host Disease (aGVHD)
3- Chronic Graft vs. Host Disease (cGVHD)

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 14/37
Hyper Acute GVHD:
Takes place just after the transplantation within minutes
Can be appreciated by the surgeon within some minutesafter the transplantation
Can last up to 24 hours
Can even cause death of the organ

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 15/37
Causes of Hyper Acute GVHD:Preformed antidonor antibodies
In multiparous women, anti-HLA antibodies against paternal
Prior blood transfusion can also lead presensitization
*H yper Acute GVHD is no more significant clinical problem

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 16/37
Acute (aGVHD):
Normally observed within the first 100 days post-transplant
After the hyper acute phaseMajor challenge to transplants owing to associated
morbidity and mortality.
Selective damage to the liver, skin and mucosa ,GIT &
hematopoietic system (e.g. bone marrow and thymus)
Cellular and humoral response

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 17/37
Predictors of acute GVHD:HLA disparitiesIncreasing age (>40)
Gender mismatch / parity of donorMinor histo-compatibility antigensCD34 doseT-cell depletion in host Advanced disease status

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 18/37
Skin rash
Diarrhea
Abnormal liver function
Increased susceptibility to infection
Symptoms usually begin within 2 months after
transplantation

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 19/37

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 20/37
Skin biopsy in acute GVHD:

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 21/37
Acute graf t versus host disease. Tissue stained w ithhematoxylin and eosin show s dy sk eratosis of indi v idualk eratinocy tes and patchy vacuolization of the basement membrane. A moderate superf icial dermal and peri vascularlymphocy tic inf iltrate is also seen.

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 22/37
Skin Biopsy in Acute GVHD

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 23/37
R ectal biops y:

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 24/37
Acute graft versus host disease involvingdesquamating skin lesions in a patient whounderwent allogeneic bone marrowtransplantation for myelodysplasia.

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 25/37
Boy who developed stage 3 skin involvement with acute
graft versus host disease (GVHD).The donor was a sistermatched for human leukocyte antigen.

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 26/37
Chronic (cGVHD):
Normally occurs after 100 days
Along with liver, skin, GIT, hematopoietic system, also
causes damage to the connective tissue and exocrine glands.

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 27/37
Skin rash
Dermatitis
Hair loss
Liver damage
Dry eyes and dry mouth
Increased susceptibility to infections
Possibly lung and gastrointestinal disorders
Chronic symptoms start more than 3 months after
transplant.

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 28/37
Prior acute GVHD
Older donor/recipient age
HLA mismatch V iral infection (e.g., cytomegalovirus)
Splenectomy

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 29/37

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 30/37
Scleroderma causingnail dystrophy.
cGVHD

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 31/37
Oral mucosal changes in a patient with chronic
graft versus host disease (GVHD). Note the skindiscoloration (vitiligo), which can result from
GVHD.

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 32/37
Boy in whom graft versus host disease (GVHD), which progressed to stage
4. High-dose cyclosporine A and methylprednisolone had beenadministered intravenously. The patient later died from chronicpulmonary disease resulting from chronic GVHD.

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 33/37
Primary Treatment: Disrupt the triad Non-specific Immunosuppressive
methylpred 2mg/kg/day Steroid + calcineurin inhibitor (CSA, tacro)
~40% of sib transplants and 24% of MUDs willrespond to steroids R esponse is worse w ith li ver in volvement and w ith
higher grade

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 34/37
Secondary Therapy
Target the IL-2 receptors
No secondary therapy to date provides notable resultsFocus remains on prevention and prediction

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 35/37
Conclusion:
GVHD is the major barrier to successful allogenic stem cell
transplantationThis may be avoided by:More precise matchingOptimum immunosupressing

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 36/37
A costless medicinehaving effects independent of
receptors, therapeutic index,clinical sign & symptoms andhaving no side-effects at all«
So,
Use it!!

8/8/2019 GVHD(M.Abdullah)
http://slidepdf.com/reader/full/gvhdmabdullah 37/37
*for not sleeping ;-)