-
8/4/2019 Horticultural Therapy has Beneficial Effects on Brain
Functions in Cerebrovascular Diseases
1/14
Vol. 2, No. 3, Page 169-182Copyright 2008, TSI Press
Printed in the USA. All rights reserved
Horticultural Therapy has Beneficial Effectson Brain Functions
in Cerebrovascular
DiseasesYuko Mizuno-Matsumoto
*,1, Syoji Kobashi
2, Yutaka Hata
2, Osamu Ishikawa
3, and
Fusayo Asano4
1University of Hyogo, Graduate School of Applied Informatics,
Kobe, JAPAN
2University of Hyogo, Graduate School of Engineering, Himeji,
JAPAN
3Ishikawa Hospital, Himeji, JAPAN
4Tokyo University of Agriculture, Department of Bio-therapy,
Faculty of Agriculture, Tokyo,
JAPAN
Received 15 May 2008; accepted 30 June 2008
AbstractHorticultural therapy (HT) is gaining attention as a
form of rehabilitations in medical fields
especially such as occupational therapy and nursing care,
although its effectiveness has not been
proven yet. This paper uses a strictly medical point of view to
assess whether or not HT is effective
for improvement of functional activities in the brains of
brain-damaged patients. Five patients in
Ishikawa Hospital with cerebrovascular diseases were invited to
participate in HT for a month in
addition to their routine medication and physical therapy (PT).
The HT program was designed by
horticultural therapists. The original purpose of the HT program
was to monitor its effects on mental
healing, cognitive re-organization, and training of
sensory-motor function. The Functional
Independence Measure (FIM) and the Self-Rating Depression Scale
(SDS) were performed before
and after HT to assess the patients physical activities of daily
living (ADL) and to determine the
patients mental changes in depressive states, respectively.
Functional magnetic resonance imaging
(fMRI) during recognition tasks was also measured before and
after HT. The ADL of all patientssignificantly improved after HT;
however, the depressive states in all patients did not
changeremarkably after the HT. fMRI examinations showed that the
visual area, the inferior temporal area,
the fusiform gyrus, and the supramarginal gyrus (SMG), in
addition to the motor area, thesupplementary motor area (SMA), the
sensory area, and the cerebellum were activated after HT.
These findings suggest that HT can accelerate an improvement of
activities in the visual and colorprocessing areas and the
association areas as well as the sensory-motor areas of the brain
in the
patients with cerebrovascular diseases. HT, therefore,
stimulates parts of brain, that are not alwaysevoked through
routine physical rehabilitation. HT can complement the routine
physical
rehabilitation and help to improve damaged brain function.
*Corresponding author information:
Yuko Mizuno-Matsumoto, M.D., Ph.D. (Medicine &
Engineering)
Graduate School of Applied Informatics, University of Hyogo
Kobe Harborland Center Bldg. 22F, 1-3-3 Higashi-Kawasakichou,
Chuo-ku, Kobe, Hyogo 650-0044, JAPAN,
TEL/FAX: +81-78-367-8616/+81-78-362-0651,
[email protected]
-
8/4/2019 Horticultural Therapy has Beneficial Effects on Brain
Functions in Cerebrovascular Diseases
2/14
170
KeywordsHorticultural therapy (HT), fMRI, Supramarginal gyrus
(SMG), Visual area, Cerebrovascular
disease, Functional independence measure (FIM)
1. INTRODUCTIONHorticulture is defined as the art and science
ofgrowing flowers, fruits, vegetables, and trees
and shrubs resulting in the development of the
minds and emotions of individuals and the
enrichment and health of communities
civilization [1]. Horticultural therapy (HT) is a
remedial process in which plants and
gardening activities are used to improve the
body, mind, and spirits of people [2]. HT is
thought to be an effective and beneficial
treatment for people of all ages, backgrounds,
and abilities. The therapeutic benefits of
peaceful garden environments have beenunderstood since ancient
times. In the 19th
century, Dr. Benjamin Rush, a signer of theDeclaration of
Independence considered to be
the Father of American Psychiatry, reportedthat garden settings
held curative effects for
people with mental illness [2].
Soderback reviewed the literature on HT and
described its use in rehabilitation followingbrain damage [3].
He showed that HT affected
emotional, cognitive and/or sensory motor
functional improvement and increased social
participation, health, well-being andsatisfaction with life.
Jones and Haight
reviewed articles on the use of the natural
environment in the form of plants or plant
material as therapeutic interventions [4]. They
showed that there was a beneficial relationship
between humans and the natural environment
in the current therapeutic uses.
Although HT has been strongly advocated, its
effect is less established. Most papers on HT
have been reported from the view of
occupational therapy and nursing care.
Therefore, the effectiveness of theseinterventionist approaches
from the medical
point of view remains to be proved, and it
would have been desirable to perform
subjective assessment of the approaches.
Ulrich [5] reported the positive influence of
nature on patients in the hospital. Surgicalpatients assigned to
rooms with windows
looking out on a natural scene had shorter
postoperative hospital stays, received fewer
negative evaluative comments in nurses notes,
and took fewer potent analgesics than patients
in similar rooms with windows facing a brick
wall.
Ulrich et al. showed that influences of nature
could reduce the emotional, attentional, and
physiological aspects of stress using the
Zuckerman Inventory of Personal Reactions
(ZIPERS), which is questionnaire using affects(subjective
aspects of feeling or emotion) toassess feelings [6]. Ulrich et al.
also measured
physiological reactions using anelectrocardiogram (ECG), pulse
transit time,
spontaneous skin conductance response, andfrontalis muscle
tension using an
electromyogram (EMG), and documented
physiological changes related to recovering
from stress, including low blood pressure,
reduced muscle tension, and differences in
cardiac responses.
Soderback indicated that HT could categorizefour different
intervention approaches:
virtual, viewing, interaction, and
action [3]. In the routine occupational or
physical therapies, a patient executes actions
only according to the therapists instruction.
On the other hand, in HT the patient can
objectively imagine the growth of vegetation in
his or her own way, actually see that the
vegetation is growing and simultaneously
perform his/her own activities as
rehabilitations. Ulrich suggested that the
benefits of nature such as trees and other
vegetations were positive influences on
emotional and physiological states of the
people, and the benefits came from visualencounters with nature
from urban planning
point of view [7].
-
8/4/2019 Horticultural Therapy has Beneficial Effects on Brain
Functions in Cerebrovascular Diseases
3/14
171
We have investigated the effectiveness of HT
on the hypotheses that (1) imagination,
observation, and participation in growing
vegetation makes a positive effect on a
patients actual activities, and (2) viewing
colorful vegetation in nature under sunlight
improves the visual abilities in the brain. Toprove these
hypotheses, we designed
experimental fMRI protocols that reveal
visual, recognitional, motor, and emotional
functions/abilities. In addition, we used the
questionnaires to measure the activities of
daily living (ADL) and the mental mood of thepatients.
The aim of this paper is to assess whetherhorticulture therapy
is effective for
improvement of brain functional activity inbrain-damaged
patients from the medical point
of view.
2. METHODSCase #1 was a 75-year-old right-handed male
patient who had suffered a right internal
carotid artery occlusion and had left
hemiplegia and dysarthria. Case #2 was a
42-year-old right-handed male patient who had
suffered a left cerebral infarction and had right
hemiplegia and aphasia. Case #3 was a
60-year-old right-handed female patient who
had suffered a right anterior cerebral artery
occlusion and had left hemiplegia. Case #4 was
a 56-year-old right-handed male patient who
had suffered right thalamic bleeding and had
left hemiplegia. Case #5 was a 68-year-old
right-handed female patient who had suffered
bleeding in the right frontal lobe and had left
hemiplegia and dysarthria. Written informed
consent was obtained from all subjects and
patients after a detailed briefing of the
experimental purposes and protocol.
The functional independence measure (FIM) is
an evaluation tool used to quantify the ability
of patients to enter rehabilitation treatment andto chart their
progress until discharged into the
community or to another facility [8]. The FIMis an assessment
instrument rating a patients
level of function in 18 physical and mentaltasks that represent
the basic ADL. The total
score rage is from 18 as a perfect dependent to
126 as a perfect independent. There are 13
motor items ranging from 13 to 91 (eating,
grooming, bathing, dressing the upper body,
dressing the lower body, toileting, bladder and
bowel management, transfers to bed/chair,
toilet and tub/shower, walking/wheelchair, and
stair climbing) and 5 cognitive items rangingfrom 5 to 35
(comprehension, expression,
social interaction, problem-solving, and
memory). Each patients FIM was scored at the
beginning and ending of the HT to assess levels
of ADL.
All patients were evaluated as to whether or notthey suffered
from depression, based on the
DSM IV-TR (Diagnostic and StatisticalManual of Mental Disorders
Fourth Edition
TR) criteria. A medical doctor also evaluatedmental status using
indicators such as mood,
motivation, communication, and expressionwith an observational
study. Moreover, the
Self-Rating Depression Scale (SDS) was used
to evaluate not only depression but also the
patients depressive states influenced by
their mental mood. All patients were rated
using the SDS in scoring only 20 items of the
questionnaire. The relationship between mean
SDS score of patients and diagnosis of major
depression was reported [9]. This report
showed that the SDS had a sensitivity of 80
percent and specificity of 88 percent for
detecting patients with major depression. TheSDS was performed
before and after the HT to
assess changes in depressive state. The SDS
score ranged from 20 to 80. A score of more
than 50 is supposed to show the possibility of a
severe depressive state (possibility of severe
major depression is high), and a score of 40-50
is supposed to show a moderate depressive
state (possibility of a moderate depression ishigh).
Five patients were invited to participate in HTdesigned by
horticultural therapists for a month
in addition to the routine medical and physicaltreatment given
in Ishikawa Hospital. The
purpose of HT program was to bring abouteffects in mental
healing, cognitive
re-organization, and training of sensory motor
function. The HT consisted of three steps:
imagining nature, designing a flowerbed, and
-
8/4/2019 Horticultural Therapy has Beneficial Effects on Brain
Functions in Cerebrovascular Diseases
4/14
172
actually planting a tree. The therapists
instructed the patients in all these processes.
Table 1 shows an example of the HT program
for each session in Case #2. The subject was
able to experience the whole process of
growing flowers including designing a garden,
creating a planting plan, preparing a flowerbed
for seeding, seeding, watering, and making
pressed flowers from his/her own flowers from
the flowerbed. It took about a month to
complete this process. Figure 7 in the
Appendix shows some pictures of scenes from
HT programs in Table 1.
Table 1. Horticultural Therapy Program for Case #2.
Session Description of Programs
1 Flowerbed preparation (weeding)
2 Flowerbed preparation (weeding)
3 Readying the soil
4 Creating a planting plan for flowerbeds
5 Briefing on future activities and selecting seedling
6 Cultivating
7 Terrarium making
8 Planting to the flowerbed according to plan
9 Planting seedling to flowerbed10 Soil readying, watering, and
dividing seedling
11 Watering, and picking up withered flowers
12 Doing crafts using moss, and watering
13 Watering
14 Planting vegetables, weeding, dividing
15 Making name plates for the flowerbeds
16 Watering and weeding
17 Watering, weeding, and appreciating other patients
flowerbeds
18 Making a container garden
19 Making pressed flowers
20 Working in the garden
Functional magnetic resonance imaging
(fMRI) under recognition tasks was measured
before and after HT. The experimental fMRI
protocols were designed to reveal the
hypotheses on the effectiveness of HT as we
mentioned in Introduction. In the other words,
viewing, recognition, movement, and the
emotional functions/abilities of the patients
were trying to be clarified. Subjects performed
two kinds of tasks, in which they fixated on an
image and categorized it into a pleasant
image or an unpleasant image based on theprevious instructions
for each trial. Imagesincluded two kinds of emotional photos: a
girls smiling facial expression (pleasant) or anangry facial
expression (unpleasant) in task 1,
and a healthy forest landscape (pleasant) or a
dying forest (unpleasant) in task 2. Each trial
involved the consecutive presentation of the
photos for 2 seconds proceeded by a crosshair
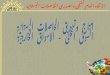
image for 20-30 seconds (Figure 1). Subjects
were instructed to fixate on a photo, and judge
whether or not the photo was pleasant by
moving their right index finger, or unpleasant
by moving both the right index and middle
fingers. Each task consisted of 20 blocks, half
of which were pleasant, and half of which were
unpleasant. Photos were randomly orderedwithin each task. The
duration of each task was516 seconds. In the study, five
patients
performed this experimental protocol using thefMRI scanner
before and after HT.
-
8/4/2019 Horticultural Therapy has Beneficial Effects on Brain
Functions in Cerebrovascular Diseases
5/14
173
Figure 1. Schematic diagram of fMRI measurement task.
MR images were acquired on a 1.5 Tesla
SIGNA CV/i scanner (GE Medical Systems,
Milwaukee, WI). After initial acquisition of T1
structural images, echo planar imaging (EPI)
was used to acquire data sensitive to the BOLD
signal at a repetition time (TR) of 2000 ms andan echo time (TE)
of 40 ms. High-resolution
T1 images were acquired to aid in anatomic
normalization. The spatial resolution of BOLD
images was set by a 64 by 64 voxel matrix
covering 260 260 mm2
with a 5 mm slice
thickness. The image gave an in-plane
resolution of 4.06 by 4.06 mm2. Twenty axial
slices with 5 mm thickness were acquired to
cover the whole brain. During the data
acquisition, 258 images (phases) per slice were
obtained in 516 seconds (= 258 x 2.0 sec). This
produced a 4-D dataset consisting 64 64 20 258 voxels, in which
a voxel is referred to as
(x, y, z, t).
Data analysis was performed with the
Statistical Parametric Mapping analyticpackage (SPM5, Wellcome
Department of
Cognitive Neurology, London, UK). In the
first step, we identified regions that showed
significant activation during the pleasant or
unpleasant images compared to those during
the crosshair image. Activations were reported
if they exceeded p < 0.05 (uncorrected) on thesingle voxel
level in each patient. We showed
images of the activation areas before and after
HT. In the next step, the differences between
the images before and after HT were calculated
using the t-statistic, and contrast maps were
generated for each patient. We extracted the
increased areas in activity after HT compared
to those before HT in each patient (p < 0.1). In
the figures the areas in which activation
decreased or did not change after HT were
omitted.
3. RESULTSThe doctors clinical observations of the whole
process left the impression that all the patientsexpressions and
motivation had improved after
the HT.
1 block
20 blocks (516 sec)
-
8/4/2019 Horticultural Therapy has Beneficial Effects on Brain
Functions in Cerebrovascular Diseases
6/14
174
Table 2 shows date information of subjects:
onset of disorders, beginning of general
rehabilitation, beginning of HT, first, before
HT and second, after HT measurement of
fMRI. HT began 6 months after the onset of
disorder in Case #1 and 2 years and 8 months
after the onset in Case #2 although HT began
2-3 months after the onsets in Cases #3, #4, and
#5.
Table 2. Date Information of subjectsCase #1 Case #2 Case #3
Case #4 Case #5
Onset of disorder 12/6/2003 10/1/2001 6/28/2004 6/21/2004
1/26/2005
Beginning of rehabilitation 4/22/2004 4/2/2002 7/27/2004
8/14/2004 3/11/2005
Beginning of HT 6/8/2004 6/8/2004 9/25/2004 9/25/2004
4/4/2005
First trial 6/1/2004 6/1/2004 9/25/2004 9/25/2004
4/4/2005fMRI
Second trial 7/16/2004 7/16/2004 10/25/2004 10/25/2004
5/19/2005
Table 3 shows the total scores of FIM before
and after the HT. The scores of motor and
cognitive items are also shown in the table. The
total scores of all the cases after HT aresignificantly larger
than those before HT
(paired T test: p < 0.03). The scores on motor
items of all cases after HT are also significantlylarger than
those before HT (paired T test: p