Embed Size (px)
Citation preview

278
hours. I would like to see a tutorial system introduced, pre-ferably at the end of school, but certainly preclinically andclinically, with the aim of passing responsibility for study fromthe tutor to the pupil. The close relationship and personalsupervision of a tutorial system is the best way for such atransfer to be achieved. It is expensive in time as well asmoney, but it is an essential part of creating the independentdoctor.
Furthermore, if the individual tutorial is the centre of theteaching programme, with the student first and foremost res-ponsible to his tutor, it enables the student to stand outside andappraise the teaching he is receiving. Though he is one of thecrowd on the " nrm ", his personal reaction still counts, andhe has greater independence of action, provided he can convincehis tutor of the honesty of his intentions.Both a tutorial system, and a decrease in numbers on ward
rounds and at outpatient clinics, would mean increasing thecost of medical education more substantially than would thesalary of a Director of Education, but the doctor is a qualityproduct whose individualism must be encouraged, rather thanlost by forced feeding in a battery system.
J. E. P. SIMPSON.St. Thomas’s Hospital,
London S.E.1.
HALLUX VALGUS
SIR,-Dr. Maclennan 1 finds hallux valgus more frequentlyin a barefoot population than have other workers, whom headmonishes for failing to take account of genetics and to giveproper indication of the degree of severity of hallux valgus. Isubmit that his findings are questionable and his admonitionunjust.He translates clinical assessment into degrees of hallux
deviation by analysis of the photographs of 11 out of 1256 feet.
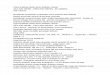
NUMBER OF BARE FEET WITH HALLUX VALGUS AND MEAN SCORE PER FOOT
BY AGE AND SEX FOR NEW GUINEA AND ST. HELENA
Not only is this method of measurement idiosyncratic, but hefails to indicate the numbers in each subset; thus there is noway of telling how many people had severe hallux valgus, whichis, he claims, a defect in other data that express results as meansand standard deviations. Moreover his " mean hallux devia-tion " ignores normal feet and ignores negative values due tohallux varus, thereby giving higher values than those of otherworkers.A summary of the St. Helena data is presented above, con-
verted into his type of score expressed as a mean of all the feetwithin any age-group, to permit easy comparison. (Approxi-mate conversion of score into degrees may be achieved bymultiplying by 10.)By using the same method of analysis on both data, the
different incidence of hallux valgus between St. Helena andNew Guinea largely disappears.
Despite his frequent invocation of genetics it was unclearhow it contributed to Dr. Maclennan’s study. Anyway, it ispointless to evaluate the genetical predisposition to a conditionthat has a powerful environmental cause. For example, if itshould be shown that the variation in susceptibility to elec-
1. Maclennan, R. Lancet, 1966, i, 1398.
trocution 2 was genetically determined, an epidemiologistinterested in prevention would doubtless summon the aid of anelectrician, not a geneticist.
IAN B. SHINE.
Department of Genetics,University of Hawaii,Honolulu, Hawaii.
A CLINICAL STUDY OF SURGICAL SHOCK
SIR,-A point in a recent letter by Mr. R. Yeo 3 mayadd to the therapeutic confusion about the management ofpatients in " shock ".He apparently uses " dextran " and
" low-molecular-weightdextran " (L.M.w.D.) interchangeably as plasma expanders inshock without stating that in effects, other than volume
expansion, they have almost opposite actions.4 5 L.M.W.D, indoses of 2 g. per kg. will significantly lower total peripheralresistance 6 by decreasing the viscosity of blood 4 and hasno effect upon the clotting mechanism,4 whereas the otherdextran tends to raise total peripheral resistance, and has beenknown to cause haemorrhagic diathesis. It would appear,furthermore, that dextrans other than L.M.W.D. would, in fact,be contraindicated in shock from most causes in view of theaccumulated evidence concerning the role of total peripheralresistance in the pathogenesis of the " shock
" state.’ L.M.w.B.
has been shown to be useful in the therapy of " shock states I’
especially pending cardiogenic shock. 8
CHARLES H. PIERCE.
Department of Surgery,University of Saskatchewan,Saskatoon, Saskatchewan.
HYPEROSMOLAR DIABETIC COMA
SIR,-During the past few weeks the discussion about thetreatment of " hyperosmolar diabetic coma," which is charac-terised by gross dehydration, hyperglycaemia, hypernatrxmia,the absence of ketosis, resistance to insulin, and late age ofonset, seems to have resolved into a debate between two schoolsof thought-those who advocate dextrose+ insulin and deplorethe use of saline, and conversely those who advocate saline-insulin and deplore the use of dextrose. Each scheme has pointsto commend it, and it seems that both are in part correct.
It also seems, however, that hard and fast rules cannot be laiddown for the management, which must consist essentially, andin order of importance, of (1) rehydration and (2) decrease ofblood-sugar content.A man, aged 65 years, was recently successfully treated. He
presented semiconscious and grossly dehydrated, with a histor ’vof ten days’ polyuria and polydipsia, precipitated by a minorbout of gastroenteritis which had cleared up after twenty-fourhours. On admission the serum-levels of sodium, potassiumand chloride were 175, 4-75, and 128 mEq. per litre respectivelyThe urea and blood-sugar levels were 135 and 960 mg. per100 ml. respectively. The systolic blood-pressure (B.P.) wa,60 mm. Hg, and the urine output was nil. During the critica.first eighteen hours, treatment consisted of rehydration vitr1 litre of fluid orally, and 10-5 litres of fluid intravenously w;tt30 mEq. potassium, and the giving of 328 units of insulin 0:which 288 units were given intravenously. After six hours, let:ventricular failure necessitated digitalisation and a decrease nthe rate of infusion. Following restoration of normal cardia:function, 1 litre of plasma was transfused over one hour becau"
2. Jex-Blake, A. J. ibid. 1913, i, 1787.3. Yeo, R. ibid. 1966, i, 817.4. Conference of the Evaluation of Low Molecular Weight Dextran
Shock: Pharmacology and Pertinent Rheology; 1963, WashingtonD.C. National Academy of Science, N.R.C.
5. Gronwall, A. Dextran and its Uses in Colloidal Infusions. New York1957.
6. Block, J. H., Pierce, C. H., Manax, W. G., Lyons, G. W., LR. C. Archs Surg., Chicago, 1965, 91, 77.
7. Block, J. H., Pierce, C. H., Lillehei, R. C. A. Rev. Med. 1966, 17. 48. Langsjoen, P. H., Falconer, H. S., Sanchez, S. A., Lynch,
Angiology, 1963, 14, 465.

279
of prolonged hypotension twelve hours.after rehydration began.During the twelve hours preceding the plasma transfusion1 litre of physiological saline solution, 3-25 litres of dextrose-saline, and 1-25 litres of 5% dextrose solution were given, andduring the succeeding five hours 3-5 litres of 5% dextrosesolution, and 0.5 litre of dextrose-saline. Complete rehydrationtook place over four days, the total input minus total outputbeing 22 litres, the patient gaining 22-7 kg. (50 lb.) in weight.The following points emerged from the management of this
patient, calculations being based on the assumption that chlorideis an extracellular ion:
1. Until plasma was transfused, intracellular fluid (r.c.F.) increasedfaster than extracellular fluid (E.C.F.) and the B.P. was not significantlyaltered by mephentermine sulphate (’ Mephine ’).
2. During the plasma transfusion I.C.F. volume remained static, forflwd was held in the extracellular compartment. Thereafter I.C.F.and E.C.F. increased in parallel. During this phase the B.P. was raisedwith mephine and was thereafter maintained. This was reflected inthe commencement of urine secretion.
3. Potassium requirements were small; a total of only 30 mEq. wasgiven during the first eighteen hours, and the cumulative intracellularshift of potassium was only 16 mEq.
4. Large doses of intravenous insulin did not alter the glucose-disappearance rate from the blood, which remained constant at
17’5 g. per hour before plasma and 32-5 g. per hour after plasma.It is therefore concluded that early transfusion of plasma is
essential if dehydration is so severe as to cause hypovol2emicshock. This must be the first consideration in management,since any period of prolonged hypotension will cause manycomplications, not least of these being acute tubular necrosis.Once the B.P. is maintained, infusions of dextrose solution andphysiological saline solution will be required, depending on theelectrolyte and blood-sugar results. Criticism of the use of50 dextrose solution during this phase has been voiced, for itwill tend to perpetuate the diuresis, but as long as rehydrationis proceeding faster than diuresis and the blood-sugar contentis not rising the hyperosmolar state will tend to be cor-
rected. Thus the use of 5% dextrose solution is sound as longas it is covered by sufficient insulin. As has been previouslystated, physiological saline solution is hypotonic to the patient’splasma and its use is equally sound. In fact, both physiologicalsaline solution and dextrose solution will be required, the for-mer to replace any sodium loss which has occurred during theinitial dehydrating diuresis, and both to replace the water loss.The problems of the management of this condition appear
simple when compared with the problems of the pathogenesis.It is consistently observed throughout the published reportsthat while in the hyperosmolar state patients are resistant toinsulin, and that once recovered little if any insulin is requiredfor control. This, together with the absence of ketosis, theobservations from this case that potassium requirements areslight during treatment, and that insulin does not alter the glu-cose-disappearance rate, seem to suggest the possibility that adefect other than that of the insulin mechanism is responsiblein the pathogenesis of this condition.
J. V. WATSON.St. Andrew’s Hospital,
Billericay, Essex.
INTESTINAL HORMONES AND PLASMA-INSULIN
SIR,-Dr. Boyns and his colleagues m their letter (July 9)draw attention to the point that effects of relatively crude pre-parations of secretin may not be attributable to this hormone.In our initial experiments with highly purified secretin weobtained no effects on glucose tolerance, and this led us tobelieve that the effect of the preparation obtained by the methodof Crick, Harper, and Raper was mediated by an agent otherthan secretin.l The highly purified material we used had beenshown to increase bicarbonate secretion into the small intestinein man, but subsequent assays kindly carried out by Prof. J. E.Jorpes in Stockholm showed that the specific activity of thisbatch was grossly diminished. The studies we have recentlyreported were carried out with highly purified secretin of
1. Dupré, J., Beck, J. C. Diabetes, 1965, 14, 440.
verified exocrine activity, supplied by Professor Jorpes, andshow that this agent is capable of producing effects on blood-insulin similar to those obtained with the crude preparation.2Clearly this finding does not exclude the presence of otheragents in intestinal extracts, capable of stimulating insulinrelease. Glucagon was not present in sufficient quantity to
account for the effects of the preparation obtained by themethod of Crick, Harper, and Raper. But Unger and hiscolleagues have shown that highly purified pancreozymin is apatent stimulus to insulin secretion in the dog, and they showedin addition that pancreozymin causes glucagon release in thatanimal.3 3 There is evidence that the crude preparation ofsecretin obtained by the method of Crick, Harper, and Rapercontains some pancreozymin, and it was found that thismaterial sometimes stimulates release of glucagon in dogs.3These effects of pancreozymin in man are at present underinvestigation. Preliminary experiments suggest that porcinepancreozymin does not cause insulin secretion in fasting humansubjects, when administered intravenously in quantities (perka. bodv-weisht) which are effective in dogs.
J. DUPRÉ
J. C. BECK.
McGill University Clinic,Royal Victoria Hospital,
Montreal, Canada.
RESISTANCE OF STAPHYLOCOCCUS AUREUS
SIR,-Dr. Dyke and his co-workers 4 have presentedevidence that penicillinase-negative variants of methicillin-resistant staphylococci are intrinsically resistant to penicillin,a conclusion with which I agree.5 They also found that somepenicillinase-negative variants of methicillin-sensitive strainswere more intrinsically resistant than others. This relativelymodest increase in penicillin resistance was found in somestrains which were also resistant to antibiotics unrelated to the
penicillins (" multiple-resistant "
staphylococci). Their asser-
tion, however, that the distinction between methicillin-sensitiveand methicillin-resistant Staphylococcus aureus is not clear-cutmight be questioned.
Methicillin-resistant strains can be distinguished becausethey consist of mixed populations with respect to methicillinresistance. 6-9 A majority of the organisms in these strains areslightly more resistant than methicillin-sensitive staphylococci,but a minority are able to grow in high concentrations ofmethicillin, 125 g. per ml. or greater.9 Since the minority ofmore resistant elements are slower growing than the others, alarge inoculum, 107-108 organisms, and a 2-day incubationperiod may be needed to detect their presence.9 Such recom-mendations for the detection of resistant strains have been sup-ported by Parker and Jevons 7; but the " border-line " culturesthey have described 4 were reported on the basis of an 18-hourincubation period so that it is not possible to decide whetherthey did indeed contain highly resistant elements.
I have confirmed that colonies growing on high concentra-tions of antibiotic are mutants with greatly increased intrinsicresistance to methicillin.10 Because of the notable heterogeneityin the resistance of the parent culture to methicillin, myco-worker and I have proposed to call these strains hetero-resistant staphylococci.ll Cross-resistance exists with respectto the other penicillins and cephalosporins, but the magnitudeof the heterogeneity is sometimes better demonstrated withmethicillin than with benzylpenicillin.The data presented bv Dr. Dvke and his co-workers do not
2. Dupré, J., Rojas, L., White, J. J., Unger, R. H., Beck, J. C. ibid. 1966,ii, 26.
3. Unger, R. H., Ketterer, H., Eisentraut, A., Dupré, J.. Communicationno. 31 to the American Diabetes Association, June 26, 1966, Chicago.
4. Dyke, K. G. H., Jevons, M. P., Parker, M. T. Lancet, 1966, i, 835.5. Seligman, S. J. Nature, Lond. 1966, 209, 994.6. Knox, R. Br. med. J. 1961, i, 126.7. Parker, M. T., Jevons, M. P. Post-Grad. med. J. 1964, 40 (December
suppl.), 170.8. Rolinson, G. N. Br. med. J. 1961, i, 125.9. Sutherland, R., Rolinson, G. N. J. Bact. 1964, 87, 887.
10. Seligman, S. J. J. gen. Microbiol. 1966, 42, 315.11. Seligman, S. J., Hewitt, W. L. Antimicrobial Agents and Chemo-
therapy—1965; p. 387. 1966.