Embed Size (px)
Citation preview

A77-year-old woman was admitted tohospital following 2 weeks of malaise,vomiting and decreased oral intake. She
had multiple comorbidities, including coronaryartery disease, cerebrovascular disease, dyslipid -emia and long-standing hypertension, for whichshe was taking a β-blocker and a nondihydro -pyridine calcium-channel blocker. She also had ahistory of adrenal insufficiency treated with long-term prednisone and hypothyroidism treated withlevothyroxine. She had been admitted to hospital5 times over the preceding 2 years because ofhyponatremia. These episodes had been attributedto hypovolemia and relative adrenal insufficiencyand had been treated with intravenous fluids andstress doses of steroids. Complicating her storywas a series of surgical procedures for chronicsinusitis. Kidney disease had been documented,with a baseline serum creatinine of 100 µmol/L(estimated glomerular filtration rate 47 mL/minper 1.73 m2), and ultrasonography had previouslyshown renal asymmetry (6.7 cm v. 9.3 cm on theright); these findings, together with her history ofatherosclerotic events, had suggested renovascu-lar disease. Magnetic resonance angiography per-formed before the current admission had showncritical stenosis of her left renal artery.
On the current presentation, the patient hadhypertension (blood pressure 158/107 mm Hg)but was hypovolemic, with dry mucous mem-branes and a low jugular venous pressure. Find-ings on cardiac, respiratory and abdominalexaminations were otherwise unremarkable.Laboratory findings showed hyponatremia(serum sodium 114 [normal 133–145] mmol/L),hypokalemia (serum potassium 2.9 [normal 3.3–5.1] mmol/L) and an elevated serum creatininelevel (135 [normal 35–100] µmol/L).
We started intravenous treatment with normalsaline, potassium and corticosteroids. The pa -tient’s sodium level returned to normal over thenext 4 days. Results of endocrine tests showed alow morning cortisol level (136 [normal > 500]nmol/L), a normal thyroid-stimulating hormonelevel (0.4 [normal 0.2–6.0] mU/L), but a low level
of free thyroxine (9 [normal 10–25] pmol/L). Hercortisone and levothyroxine doses were increased.However, when we subsequently stopped intra-venous fluids and potassium supplementation,the patient had a recurrence of hyponatremia,hypokalemia and prerenal azotemia. During thistime, she continued to experience polyuria (urineoutput 3–5 L/d) and hypertension (systolic pres-sure 150–165 mm Hg and diastolic pressure 80–105 mm Hg).
What is your diagnosis?
a. Central diabetes insipidus due to traumab. Nephrogenic diabetes insipidus resulting
from hypokalemiac. Panhypopituitarism as a consequence of sinus
surgeryd. Hyponatremic–hypertensive syndrome sec-
ondary to unilateral stenosis of the renal artery
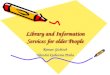
The diagnosis in this case is (d) hyponatremic–hypertensive syndrome secondary to unilateralstenosis of the renal artery. To reach the diagnosis,we first evaluated the cause of the hyponatremia(Figure 1). The patient’s measured serum osmo-lality was 248 (normal 280–300) mmol/kg. Hercalculated serum osmolality — calculated as2(serum sodium) + serum glucose + urea — was2(114) + 5 + 5 = 238 mmol/kg. A low serumosmolality indicated hypo-osmolar hyponatremia,as opposed to iso-osmolar or hyperosmolar hypo -natremia. Neither central nor nephrogenic dia-betes insipidus would be consistent with hypo-osmolar hyponatremia.
Hyponatremia is the result of excessive freewater in relation to body sodium. Although ourpatient presented with mild acute kidney injury onchronic kidney disease, the degree of renal impair-ment was not sufficient to impair excretion of freewater by the kidneys. Some causes of hypona-tremia, namely primary polydipsia or low soluteintake, are associated with low levels of anti -diuretic hormone and appropriately dilute urine.Minimum urine osmolality in healthy individuals
What is your call?
Hyponatremia and polyuria in an older woman
Kevin Afra MD, Matthew T. James MD PhD
Competing interests:Matthew James receivedspeaker fees from Amgenfor a presentation on acutekidney injury at anephrology conference.No competing interestsdeclared by Kevin Afra.
This article has been peerreviewed.
Correspondence to:Matthew T. James,[email protected]
CMAJ 2013. DOI:10.1503/cmaj.121757
PracticeCMAJ
© 2013 Canadian Medical Association or its licensors CMAJ, September 3, 2013, 185(12) 1055
CM
E

is about 50 mmol/kg. In our patient, the urineosmolality was 178 (normal 50–1200) mmol/kg,which indicated antidiuretic-hormone activity.The patient’s urine sodium was 41 mmol/L andurine potassium 20 mmol/L (normal levels arediet dependent).
We next sought to determine whether there wasa physiologic stimulus for secretion of anti diuretichormone, such as hypovolemia, or a low effectivecirculating volume state. A low urine sodium con-centration, generally less than 20 mmol/L, tends toaccompany such conditions; however, our patient’surine sodium level was elevated. Although ele-vated levels may be seen in SIADH (syndrome ofinappropriate antidiuretic hormone secretion),adrenal insufficiency and hypothyroidism, theymay also be seen in the setting of hypovolemiawhen renal sodium losses are present. The recur-rence of hyponatremia and volume depletion in thesetting of cortisone and levothyroxine therapypointed to another cause contributing to our pa -tient’s clin ical presentation.
The features of hypovolemia with concomi-tant polyuria and elevated urine sodium levelssuggested renal losses. The patient had no his-
tory of diuretic use to suggest drug-induced renallosses, which left renal natriuresis as the mostlikely problem. Taking into account her hyper-tension and critical stenosis of the left renalartery, we diagnosed hyponatremic–hypertensivesyndrome.
Which study confirmsthe diagnosis?
a. Urine excretion in a 24-hour collectionb. Elevated renin activityc. Water deprivation studyd. Cosyntropic stimulation test
Hyponatremic–hypertensive syndrome is associ-ated with elevated renin activity generated by theischemic kidney (b). Our patient’s renin activitywas markedly elevated (2.96 [normal 0.08–0.64]ng/L per second), which was consistent with thediagnosis of hyponatremic–hypertensive syn-drome. A water deprivation study would be use-ful to confirm diabetes insipidus if the patienthad polyuria and hypernatremia. Measurementof urine excretion in a 24-hour collection wouldonly confirm the renal sodium losses alreadyrevealed by her polyuria and spot urine sodiumconcentrations. Although a cosyntropin stimula-tion test and thyroid-stimulating hormone levelmay have some diagnostic utility to rule outadrenal insufficiency and hypothyroidism, therecurrence of hyponatremia despite cortisoneand levothyroxine replacement therapy reducedthe likelihood that these tests would help usunderstand the problem.
Discussion
Diagnosis and epidemiologyPatients with hyponatremic–hypertensive syn-drome may present with headache, polyuria,polydipsia, weight loss or seizures. These symp-toms are accompanied by hypertension that isoften severe (mean 228/124 mm Hg in one caseseries) and associated with a postural drop.2
Hyponatremia, hypokalemia, and elevated urineosmolality and urine sodium levels are in keep-ing with the diagnosis (Figure 1). The combina-tion of hypertension, polyuria and hyponatremia,in conjunction with asymmetric renal artery dis-ease and elevated renin activity, confirms thediagnosis of hyponatremic–hypertensive syn-drome. The population-based incidence of thesyndrome is unknown; however, one case seriesidentified 32 people who met criteria for thediagnosis from a source population of 350 000followed for 17 years.2,3
Practice
1056 CMAJ, September 3, 2013, 185(12)
Hypo-osmolarhyponatremia
Rule out severe reduction in glomerular filtration rate
Low ADH activity(low urine osmolality)
• Primary polydipsia• Low dietary solute intake
Elevated ADH activity(elevated urine
osmolality)
Evaluate antidiuretic hormone (ADH) activity
Urine sodium retention(urine sodium < 20 mmol/L)• Gastrointestinal fluid losses• Heart failure• Cirrhosis
No urine sodium retention(urine sodium > 20 mmol/L)• Renal fluid losses
– Diuretics– Renal natriuresis
• SIADH• Adrenal insufficiency• Hypothyroidism
Figure 1: Physiologic approach to hypo-osmolar hyponatremia. SIADH = syn-drome of inappropriate antidiuretic hormone secretion. Source: Wakil et al.1

PathophysiologyThe pathophysiology of the syndrome involvesthe interplay between unilateral renal ischemia,the renin–angiotensin–aldosterone system andresponses in the contralateral kidney (Figure 2).In the setting of severe unilateral renal hypoper-fusion, whether from critical stenosis of a singlerenal artery or asymmetric bilateral stenosis, theischemic kidney generates high levels of renin,which leads to elevated plasma angiotensin II lev-els. Systemic blood pressure rises as a result ofthe angiotensin II activity, a physiologic attemptto restore perfusion to the ischemic kidney. Theunaffected contralateral kidney is exposed to amuch higher perfusion pressure than it requires,which leads to pressure natriuresis in an attemptto autoregulate. The pressure natriuresis leads torenal sodium wasting and the clinical hypo -volemia typically seen in patients with hypona-tremic–hypertensive syndrome. Volume depletionfurther stimulates renin activity, which contrib -utes to a feedback loop.4
Angiotensin II also stimulates aldosterone secre-tion from the adrenal glands, which leads to renalpotassium excretion and resultant hypokalemia.4
Volume contraction and elevated angiotensin II levels stimulate the release of antidiuretic hormone,which results in thirst and polydipsia.2,4 The anti -diuretic hormone activity, along with excess freewater intake from polydipsia relative to urinesodium wasting, results in hyponatremia.
ManagementIn a case report by Atkinson and colleagues,4
blockade of the renin–angiotensin–aldosteronesystem with the angiotensin-converting-enzyme(ACE) inhibitor captopril was effective in treat-ing hyponatremic–hypertensive syndrome in a52-year-old woman with unilateral occlusion ofthe renal artery. The woman underwent unilateralnephrectomy with no recurrence of the syn-drome and no need for ongoing pharmacother-apy. Definitive therapy through surgical or percu-taneous revascularization, or removal of theischemic kidney has been described in most casereports. In the largest case series, involving 32patients,2 many were given antihypertensive ther-apy alone, although the long-term effectivenessof this approach was not reported.
The new class of antidiuretic hormone receptorantagonists (vaptan drugs) have been shown toraise serum sodium concentrations in eu volemicand hypervolemic causes of hyponatremia, includ-ing SIADH, heart failure and cirrhosis. However,antagonism of antidiuretic hormone may be harm-ful in hypovolemic states, and vaptan drugs arethus contraindicated in hypovolemic conditionssuch as hyponatremic–hypertensive syndrome.5
In our patient, medical therapy was startedwith sodium chloride tablets (2 g/d orally) toreplace renal sodium losses and help maintaineuvolemia. Blockade of the renin–angiotensin–aldosterone system with an ACE inhibitor was
Practice
CMAJ, September 3, 2013, 185(12) 1057
Renal artery stenosis
Renin release
Angiotensin II
Hypovolemia ADH
Thirst
Hyponatremia
Polyuria
Increased intake of free water
Aldosterone
Pressure natriuresisfrom contralateral kidney
Hypertension
Unilateral renal ischemia
Hypokalemia
Renal retention of free water
Polydipsia
Figure 2: Schematic representation of the pathophysiology of hyponatremic–hypertensive syndrome. Solidlines indicate positive feedback or stimulus; dotted lines indicate negative feedback or inhibition; and boxesindicate clinically apparent signs and symptoms. ADH = antidiuretic hormone. Source: Atkinson et al.3

begun; however, it was unsuccessful in allowingdiscontinuation of intravenous fluids withoutrecurrent volume depletion and hyponatremia.Following the addition of an angiotensin-receptorblocker to intensify blockade of the renin–angiotensin–aldosterone system, the patient’sblood pressure improved and polyuria resolved,and we were able to successfully stop all intra-venous fluids and potassium supplementation.Our patient declined surgical intervention, andmedical therapy was continued. Following dis-charge, sodium chloride tablets were graduallyreduced and stopped by 6 months. After 1 year offollow-up, our patient has remained well, with norecurrence of hyponatremia, no further hospitaladmissions and well-controlled blood pressure.
Although combination therapy with an ACEinhibitor and angiotensin-receptor blocker is notrecommended for most patients with vasculardisease, given the increased risk of adverseevents reported in the ONTARGET trial,6 ourreport describes a rare case where dual blockade
of the renin–angiotensin–aldosterone system waseffective and well tolerated.
References1. Wakil A, Ng JM, Atkin SL. Investigating hyponatraemia. BMJ
2011;342:d1118.2. Agarwal M, Lynn KL, Richards AM, et al. Hyponatremic–
hypertensive syndrome with renal ischemia: an underrecognizeddisorder. Hypertension 1999;33:1020-4.
3. Kovalski Y, Cleper R, Krause I, et al. Hyponatremic hyperten-sive syndrome in pediatric patients: Is it really so rare? PediatrNephrol 2012;27:1037-40.
4. Atkinson AB, Davies DL, Leckie B, et al. Hyponatraemic hyper-tensive syndrome with renal-artery occlusion corrected by capto-pril. Lancet 1979;2:606-9.
5. Robertson GL. Vaptans for the treatment of hyponatremia. NatRev Endocrinol 2011;7:151-61.
6. Yusuf S, Teo KK, Pogue J, et al. Telmisartan, ramipril, or both inpatients at high risk for vascular events. N Engl J Med 2008;358:1547-59.
Affiliations: Department of Medicine (Afra, James), Univer-sity of Calgary, Calgary, Alta.
Contributors: Both authors were responsible for the concep-tion of the manuscript. Kevin Afra drafted the manuscript,and both authors revised it critically and approved the finalversion submitted for publication.
Practice
1058 CMAJ, September 3, 2013, 185(12)
Call for papers:CMAJ Holiday Reading
‘Twas months before the holidays and allthrough CMAJ house not a submission wasstirring, making editors grouse. “HolidayReading time is nigh!” they cried in despair, inhopes that your papers soon would be there.
Submit your evidence-based research onquirky topics, brilliant missives or holiday-themed visuals at http://mc . manuscriptcentral .com /cmaj. Submissions should be no longerthan 1200 words. For information [email protected]
Deadline: October 1, 2013