Embed Size (px)
Citation preview

Immunosuppressive Agents in Heart Transplantation
Intern 許育偉2008.02.04

Questions Before This Topic
常見的免疫抑制劑,分成哪幾類 ?Monoclonal 和 Polyclonal Ab 有什麼差別 ?何時要用 Induction Therapy ?AZA 和 MMF 哪一個比較好 ?CsA 和 Tacrolimus 哪一個比較好 ?在腎功能惡化的情況下的用藥原則 ?什麼是 Rescue Therapy ?

Outlines of Today’s Topic
Immuno-suppression mechanism
(1) Induction therapy
(2) Maintenance therapyImmunosuppressive agents in renal fun
ction impairmentRescue therapyCurrent regimens worldwide

Kobashigawa JA and Patel JK (2006) Immunosuppression for heart transplantation: where are we now?Nat Clin Pract Cardiovasc Med 3: 203–212 doi:10.1038/ncpcardio0510
Corticosteroids1. Nonspecific anti-inflammatory agents2. Block T cell and APC derived cytokine and cytokine-receptor expression
Calcineurin Inhibitors1. (1) Cyclosporine (CsA) Neoral (2) Tacrolimus (FK-506) Prograf2. Binds to calcineurin3. Key function in current immunosuppressive agents4. Nephrotoxicity !!!
Anti-proliferative Agents1. (1) Azathioprine Imuran (2) Mycophenolate Mofetil (MMF) Cellcept2. Block the cell cycle (De Novo synthesis)
Proliferation Signal Inhibitors1. (1) Sirolimus Rapamycin (Rapa) (2) Everolimus Certican2. Block signaling downstream IL-2R
Monoclonal Antibodies1. (1) Muromonab OKT3 (2) Basiliximab Simulect (3) Daclizumab Zenapax2. Block TCR, CD3, CD4, or IL-2R
Polyclonal Antibodies1. (1) Rabbit antithymocytes globulin RATG (2) Horse antithymocytes globulin ATGAM2. Various amounts of specific Ab against T cells

Induction Therapy
Upstream Ab Immunologic ablation
Division of Cardiology, Department of Medicine, University Of Maryland, Baltimore, Maryland.J Heart Lung Transplant 2007;26:205–9.

Polyclonal vs. Monoclonal Ab
Division of Cardiac Surgery, University of Ottawa Heart Institute, 40 Ruskin Street, Ottawa, Ontario, K1Y-4W7, CanadaInteract CardioVasc Thorac Surg2005;4:415-419
Average mean time to first rejection

Polyclonal vs. Monoclonal Ab
Division of Cardiac Surgery, University of Ottawa Heart Institute, 40 Ruskin Street, Ottawa, Ontario, K1Y-4W7, CanadaInteract CardioVasc Thorac Surg2005;4:415-419
Graft Rejection
Infection
One-Year Survival

Polyclonal vs. Monoclonal Ab
Side-effects more in monoclonal Ab (OKT3)
☆ Fever
☆ Headaches
☆ Acute respiratory distress
☆ Hypotension
Division of Cardiac Surgery, University of Ottawa Heart Institute, 40 Ruskin Street, Ottawa, Ontario, K1Y-4W7, CanadaInteract CardioVasc Thorac Surg2005;4:415-419

Monoclonal Ab : OKT3 vs. IL-2R
2006, SIMCOR Study Randomized Multicenter Comparison of Basiliximab a
nd Muromonab (OKT3) in Heart Transplantation 99 heart transplant recipients No difference in (1) Severity of acute rejection episodes (2) Timing of acute rejection episodes (3) Incidence of infection (4) Actuarial survival. OKT3 had a higher incidence of adverse events such
as fever, pulmonary edema, and hypotension
A randomized multicenter comparison of basiliximab and muromonab (OKT3) in heart transplantation: SIMCOR study. Transplantation 2006;81:1542–8.

Induction Therapy : Who ?
Mehra MR, Uber PA, Uber WE, Scott RLCurr Opin Cardiol 2003;18:153–8.
1. Multiparous women 2. Reoperative sternotomy patients 3. Posttransfusions patients 4. Supported with left ventricular assist devices.
Higgins R, Kirklin JK, Brown RN, et al; Cardiac Transplant Research Database (CTRD). 1990~2001, enrolled 6553 patients J Heart Lung Transplant 2005;24:392–400.
1. Ventricular assist device 2. Black ethnicity, 3. Extensive human leukocyte antigen mismatching
Division of Cardiology, Department of Medicine, University Of Maryland, Baltimore, Maryland.J Heart Lung Transplant 2007;26:205–9.

Maintenance Therapy
Three-combined regimen
--- Glucocorticosteroids (1~2 mg/kg/day)
--- Calcineurin inhibitors (5 mg/ kg/ day)
Ex : CsA, Tacrolimus (FK-506)
--- Purine inhibitors
Ex : AZA, MMF
or added Sirolimus, EverolimusDepartment of Surgery, Louisiana State University Health Sciences Center
CRITICAL CARE NURSING QUARTERLY/JANUARY–MARCH 2004

Maintenance Therapy~CNI
Calcineurin inhibitors
1. Cornerstone of immunosuppressive therapy
2. High doses of CsA, Keep trough level : 250~350 μg/L in initial 6~12 months
3. Trough 150~250 250~350 ≒ μg/L
Department of Cardiovascular Surgery, Centre Hospitalier Universitaire de Sherbrooke, Sherbrooke, Quebec, CanadaAnn Thorac Surg 2004;77:363–71

Maintenance ~ MMF and AZA
MMF 3000 mg/ day AZA 1.5~3 mg/kg/day MMF vs. AZA
1. Reduction of mortality at 1 year (p=0.03)
2. Less requirement for treatment of rejection within the first 6-months after transplantation (p=0.03)
3. Rejection free at 6 months (p=0.04)
Department of Cardiovascular Surgery, Centre Hospitalier Universitaire de Sherbrooke, Sherbrooke, Quebec, CanadaAnn Thorac Surg 2004;77:363–71

Maintenance Therapy
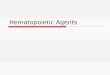
Cohort study, included 317 HT patients.(1) OKT3 7 days + CsA + MMF + S(2) OKT3 7 days + CsA + AZA + S(3) OKT3 10 days + CsA + MMF + S(4) OKT3 10 days + CsA + AZA + S(5) IL-2 antagonists + CsA + MMF + S(6) IL-2 antagonists + tacrolimus + MMF + S
(Daclizumab)Transplantation Proceedings, 38, 2550–2552 (2006)

Maintenance Therapy
Transplantation Proceedings, 38, 2550–2552 (2006)

Maintenance Therapy
(5) IL-2 antagonists + CsA + MMF + S (91.2 %) (6) IL-2 antagonists + tacrolimus + MMF + S (84.6 %) (1) OKT3 7 days + CsA + MMF + S (75.8 %) (3) OKT3 10 days + CsA + MMF + S (63.6 %) (2) OKT3 7 days + CsA + AZA + S (51.2 %) (4) OKT3 10 days + CsA + AZA + S (25.3 %)
1. (5) > (6) CsA >FK-506 (???)
2. (1) > (2) and (3) > (4) MMF > AZA
3. (5) > (1) IL-2 ant > OKT3
4. (1) > (3) OKT 7 days > 10 days
Transplantation Proceedings, 38, 2550–2552 (2006)

Tacrolimus vs. Cyclosporine
Europe : Favored Cyclosporine
America : Favored Tacrolimus
J Heart Lung Transplant 2007;26:769–81.

Tacrolimus vs. Cyclosporine
A large, prospective studyRandomized Clinical TrialTacrolimus vs. Cyclosporine (each 157)
American Journal of Transplantation 2006; 6: 1387–1397

Tacrolimus vs. Cyclosporine
Tacrolimus 0.075 mg/kg/dayCyclosporine 4~6 mg/kg/day
★ Target trough levelTacrolimus 10~20 ng/mL for 1~3 month
s, followed by 5~15 ng/mLCyclosporine 200~350 ng/mL, followed
by 100~200 ng/mLAmerican Journal of Transplantation 2006; 6: 1387–1397

Tacrolimus vs. Cyclosporine
American Journal of Transplantation 2006; 6: 1387–1397

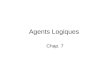
Tacrolimus vs. Cyclosporine
American Journal of Transplantation 2006; 6: 1387–1397
Creatinine
Lipid (TG)
SBP
DBP

Tacrolimus vs. Cyclosporine
American Journal of Transplantation 2006; 6: 1387–1397

Tacrolimus vs. Cyclosporine
American Journal of Transplantation 2006; 6: 1387–1397

Studies in Renal Impairments
Calcineurin inhibitors is the cornerstone of immunosuppressive therapy
Nephrotoxicity !!!Odium et al : the level of pre-transplantation r
enal dysfunction that would lead to an increase in postoperative renal failure and mortality Ccr< 40 ml/min
Goal : To minimize the usage of CNI
Division of Cardiology, Department of Medicine, University Of Maryland, Baltimore, Maryland.J Heart Lung Transplant 2007;26:205–9.

Induction Therapy with Delayed CNI
1. High risk patients (Ccr 33~50 mL/min)
Basiliximab + CsA (Day 4) + MMF + S2. Low risk patients (Ccr > 50 mL/min)
Basiliximab + CsA (Day 0) + MMF + S3. High risk patients
Basiliximab + CsA (Day 0) + MMF + S
Ccr : 2 > 1 >> 3≒Basiliximab vs. RATG No difference
Division of Cardiology, Department of Medicine, University Of Maryland, Baltimore, Maryland.J Heart Lung Transplant 2007;26:205–9.

Sirolimus
Retrospective study, enroll 38 patientsSirolimus loading dose : 2.0 mgSirolimus level : 8.0 ng/mL
P<0.01
University Health Network, Toronto General Hospital, Toronto, Ontario, Canada.J Heart Lung Transplant 2007;26:998–1003.
Months 0 1 3 6
Ccr 22.9 25.9 25.6 28.8

Everolimus
2007 Prospective study5 medical centersEnrolled 60 patients, 6-month follow-upLoading dose : 0.75 mg BID
+ CNI, MMF, Steroids in the first weekIn the second week CNI ↓ 30 %After second week DC CNI
J Heart Lung Transplant 2007;26:250–7.

Everolimus
J Heart Lung Transplant 2007;26:250–7.

Everolimus
J Heart Lung Transplant 2007;26:250–7.
Tremor Peripheral edema
Hirsutism Gingival hyperplasia

Rescue Therapy
Rescue treatment involves any type of therapy introduced once the first-line treatment has failed.
CorticosteroidsPolyclonal and monoclonal AbMycophenolate MofetilTacrolimus
Department of Cardiovascular Surgery, Centre Hospitalier Universitaire de Sherbrooke, Sherbrooke, Quebec, CanadaAnn Thorac Surg 2004;77:363–71

Rescue Therapy~ Corticosteroids
High doses corticosteroidsFirst choice for first-line rescue therapyA pulse of 1g methylpredisolone iv for 3
days.( 500mg or 250 mg/day maybe ok )
Keep low dose oral form 0.5~1 mg/kg/d
Department of Cardiovascular Surgery, Centre Hospitalier Universitaire de Sherbrooke, Sherbrooke, Quebec, CanadaAnn Thorac Surg 2004;77:363–71

Rescue Therapy~ Antibodies
Steroid resistant AbOKT3 in rescue therapy 10~14 daysBasilizumab and Daclizumab not stu
dy well yet
Department of Cardiovascular Surgery, Centre Hospitalier Universitaire de Sherbrooke, Sherbrooke, Quebec, CanadaAnn Thorac Surg 2004;77:363–71

Rescue Therapy~ MMF
Steroids + Cyclosporine + Azathioprine
Steroids + Cyclosporine + MMFMMF oral dose : 1000~3000 mg/ dayRescue 2000 mg~3000mg /day
Department of Cardiovascular Surgery, Centre Hospitalier Universitaire de Sherbrooke, Sherbrooke, Quebec, CanadaAnn Thorac Surg 2004;77:363–71

Rescue Therapy~ Tacrolimus
Cyclosporine Tacrolimus (FK-506)139 patients, 15 of Grade III or above
Conversion rate : 14 in 15 patients
Department of Cardiovascular Surgery, Centre Hospitalier Universitaire de Sherbrooke, Sherbrooke, Quebec, CanadaAnn Thorac Surg 2004;77:363–71

Transplantation worldwide
ISHLT, >76000 heart transplantation patients
J Heart Lung Transplant 2007;26:769–81.

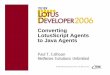
World Trends ~ Induction
J Heart Lung Transplant 2007;26:769–81.
42
52
20
<3
31
16
0

World Trends ~ Maintenance (1)
J Heart Lung Transplant 2007;26:769–81.
40
54
13
63
MMF dominant

World Trends ~ Maintenance (5)
J Heart Lung Transplant 2007;26:769–81.
39
33

World Trends ~ Maintenance
J Heart Lung Transplant 2007;26:769–81.

Questions After This Topic
常見的免疫抑制劑,分成哪幾類 ?
Monoclonal 和 Polyclonal Ab 有什麼差別 ?何時要用 Induction Therapy ?AZA 和 MMF 哪一個比較好 ?CsA 和 Tacrolimus 哪一個比較好 ?在腎功能惡化的情況下的用藥原則 ?什麼是 Rescue Therapy ?

Thanks For Your Attention