Embed Size (px)
Citation preview

O
O
Imd
THT
a
Sb
Jc
d
e
R
S
1
d
besity Research & Clinical Practice (2012) 6, e321—e329
RIGINAL ARTICLE
ntracellular lipid content of liver and skeletaluscle in patients with adult growth hormoneeficiency without diabetes mellitus
omoko Satoa, Takuyuki Katabamia,∗, Kentaro Furukawaa,iroshi Narimatsub, Takuo Hashimotoc, Yasuo Nakajimad, Akio Ohtaa,oshiyasu Sasaokae, Yasushi Tanakaa
Department of Internal Medicine, Division of Metabolism and Endocrinology, St. Marianna Universitychool of Medicine, Kawasaki, JapanUniversity Hospital Diagnostic Imaging Center, St. Marianna University School of Medicine, Kawasaki,apanDepartment of Neurosurgery, St. Marianna University School of Medicine, Kawasaki, JapanDepartment of Radiology, St. Marianna University School of Medicine, Kawasaki, JapanDepartment of Clinical Pharmacology, University School of Toyama, Sugitani, Toyama, Japan
eceived 8 June 2011; received in revised form 24 August 2011; accepted 1 September 2011
KEYWORDSAdult growth hormonedeficiency;Intrahepatic lipid;Proton magneticresonance spectroscopy;
SummaryBackground: Insulin resistance (IR) and visceral obesity are often observed in adultgrowth hormone deficiency patients (AGHDs). However, there is little informationregarding the intrahepatic lipid (IHL) or the intramyocellular lipid (IMCL) contentand their association with IR in AGHDs. The aim of this study was to directly assessIHL and IMCL in AGHDs by proton magnetic resonance spectroscopy and to evaluate
Insulin resistancethe association of lipid levels with IR.Methods: Appropriate hormone replacement therapy (RT) other than GH and estro-gen was prescribed before evaluation. Ten AGHDs (aged 23—75 years) withoutdiabetes or elevation of aminotransferases were examined the percent body fat, vis-ceral fat area (VFA), IHL, IMCL, adipokines and glucose metabolism. In two AGHDs,
changes of these parameters were evaluated after GHRT.∗ Corresponding author at: Department of Internal Medicine, Division of Metabolism and Endocrinology, St. Marianna Universitychool of Medicine 2-16-1, Sugao, Miyamae-ku, Kawasaki, Kanagawa 216-8511, Japan. Tel.: +81 44 977 8111; fax: +81 44 976 8516.
E-mail address: [email protected] (T. Katabami).
871-403X/$ — see front matter © 2011 Asian Oceanian Association for the Study of Obesity. Published by Elsevier Ltd. All rights reserved.
oi:10.1016/j.orcp.2011.09.001

e322 T. Sato et al.
Results: Visceral obesity and metabolic syndrome was found in 100% and in 80% ofthe patients, respectively. IHL was significantly higher than that in non-obese healthycontrols (12.5 ± 4.6 vs. 0.69 ± 0.46%, M ± SE, p = 0.0330), while IMCL did not differbetween AGHDs and controls (528.8 ± 137.2 vs. 378 ± 51.1 mM, p = 0.2728). Homeosta-sis model assessment of IR was significantly correlated with IHL (r = 0.896, p = 0.0001)and IMCL (r = 0.749, p = 0.0102), but not with the VFA or percent truncal fat mass.A decrease of IHL and improvement of glucose tolerance were observed in the twopatients after 6 M GHRT.Conclusion: These results demonstrated that IHL, but not IMCL, may increase inAGHDs, and that IHL may associate with IR. GHRT may decrease IHL along withamelioration of IR.
ssociation for the Study of Obesity. Published by Elsevier Ltd.
(s(Adwmc[ttn
AeIoptgiitA
M
S
BTwomen aged from 23 to 75 years) and without type2 diabetes were enrolled. They had a history of
© 2011 Asian Oceanian AAll rights reserved.
Introduction
Previous studies have shown that free fatty acids(FFA) and various adipokines derived from visceraladipose tissue (VAT) are significant risk factorsfor the metabolic complications of obesity, includ-ing insulin resistance, dyslipidemia, nonalcoholicfatty liver disease (NAFLD), type 2 diabetes, andcardiovascular disease [1—3]. These findings andthe anatomical location of VAT connecting theliver through portal vein have led to the con-cept that VAT may be a primary contributor to themetabolic abnormalities associated with hepaticinsulin resistance. However, we previously reportedthat not only VAT, but also the intrahepatic lipid(IHL) content and the intramyocellular lipid (IMCL)content measured by proton magnetic resonancespectroscopy (1H-MRS), were closely related toinsulin resistance, and that lifestyle modificationfor type 2 diabetic patients and obese metabolicsyndrome (MS) subjects resulted in amelioration ofinsulin resistance along with a decrease of IMCLand IHL despite no any change of plasma FFA andadiponectin levels [4,5].
Furthermore, we recently reported that the totalabdominal subcutaneous fat volume (SFV) and totalvisceral fat volume (VFV) measured by our methodusing whole abdominal CT scanning (about 700slices from the top of the liver to the floor ofthe pelvic cavity) [6] were correlated with andIHL measured by 1H-MRS on univariate analysis,while IHL (but not SFV or VFV) was correlatedwith clinical insulin resistance indices [homeostasismodel assessment of insulin resistance (HOMA-IR)and the MATSUDA Index] on multiple regression
analysis in obese Japanese subjects [7]. Thesefindings suggested that IMCL and IHL, as well asVAT, are important factors associated with insulinresistance.hGwi
Patients with adult growth hormone deficiencyAGHD) commonly show changes of body compo-ition that are characterized by excess adipositymainly VAT) and a decrease of lean body mass [8].GHD patients also have various metabolic disor-ers, including insulin resistance and dyslipidemia,hich are similar to MS [9,10], while growth hor-one treatment has a beneficial effect on the body
omposition and insulin resistance of AGHD patients11,12]. Furthermore, Takahashi et al. reportedhat GH replacement therapy led to dramatic his-ological improvement in an AGHD patient withonalcoholic steatohepatitis (NASH) [13].
However, little is known about IMCL and IHL inGHD patients with normal aminotransferase lev-ls. Therefore, the aim of this study was to measureMCL and IHL by 1H-MRS and assess the associationf these parameters with insulin resistance in AGHDatients. Since hyperglycemia potently increaseshe hepatic lipid content through excess influx oflucose into the liver and the prevalence of NAFLDs much higher in people with diabetes [14], wenvestigated AGHD patients who had normal amino-ransferases (reference range: AST 10—40 IU/L andLT 5—45 IU/L) and no evidence of diabetes.
aterials and methods
ubjects
aseline data for the ten patients are shown inable 1. Ten patients with AGHD (four men and six
ypothalamic—pituitary disease, childhood-onsetHD, or cranial irradiation. All of the subjectsere diagnosed as having severe AGHD accord-
ng to the criteria described below, and were

Intracellular lipid content of liver and skeletal muscle i
Table 1 Baseline profile of the subjects.
n (male/female) 10 (4/6)Age (years) 54.1 ± 5.9BMI (kg/m2) 24.9 ± 1.4IGF-I SD score −1.77 ± 0.36Cause of GHD (n)
Pituitary tumor 4Empty sella 2Pituitary stalk interruption syndrome 2Lymphocytic hypophysitis 1Dwarfism 1
Childhood-onset AGHD (n) 2Adult-onset AGHD (n) 8
cgsbpwptdpdstiod
riweociieods(swtleiGp
Mh
BotulTtTSrbJcdwwidomwfdmttlf
M
IdsabSmso2wtottipaof 144 ms, and acquisition number of 128. Thenintracellular lipids (both IMCL and IHL) were quan-tified from the methylene proton peak (—CH2) of
onfirmed not to have diabetes by a 75 g-orallucose tolerance test (OGTT). At least one GHtimulation test (insulin tolerance test and com-ined administration of glucagon or arginine) waserformed to confirm that the peak GH responseas less than 1.8 ng/mL. If the GH releasingeptide-2 (GHRP-2) provocation test was done,he peak GH level indicating severe GHD wasefined as <9.0 ng/mL. The cause of AGHD was aituitary tumor in four patients, empty sella syn-rome in two patients, pituitary stalk interruptionyndrome in two patients, lymphocytic hypophysi-is in one patient, and idiopathic dwarfismn one patient. Two patients had childhood-nset GHD and eight patients had adult-onsetisease.
Before evaluation, appropriate hormoneeplacement therapy other than GH was prescribedn all patients before evaluation except four elderomen (Case 7, 8, 9 and 10) who did not receivedstrogen replacement because of age (beinglder than 60 years) and the patient kept stableondition (Cortisone, l-thyroxine, and testosteronen two patients; and cortisone and l-thyroxinen five patients). Alcohol consumption did notxceed 20 g/day in any subject, and liver diseasesther than NAFLD (e.g., viral hepatitis) were notetected by serological testing and/or imagingtudies. Two patients injected recombinant humanrh) GH (Humatrope®; Eli Lilly, Indianapolis, US).c. daily. The starting dose 0.021 mg/kg/week andas gradually increased up to 0.081 mg/kg/week
o obtain insulin-like growth factor-1 (IGF-1)evels in normal age- and gender-related refer-nce rage and clinical response (i.e., significantmprovement of physical activity). In the event ofH-induced side effects, the dose reduction wasermitted.
fn patients e323
easurement of anthropometric indices,ormones, adipokines, and body fat
lood samples collected before 9 AM after anvernight fast (>12 h) were immediately cen-rifuged at 4 ◦C and then stored at −80 ◦Cntil assay. Insulin was measured by a chemi-uminesent enzyme immunoassay (Fujirebio Inc.,okyo, Japan). The high molecular weight frac-ion of adiponectin (HMW-Ad) (Fujirebio Inc.,okyo, Japan) and leptin (Linco Research, Inc.,t. Charles. Missouri, USA) were measured byadioimmunoassay, while IGF-1 was measuredy immunoradiometric assay (TFB, Inc., Tokyo,apan). All of these assays were done with commer-ially available kits. The baseline IGF-1 standardeviation (SD) score was calculated by comparisonith age- and gender-matched subjects. HOMA-IRas calculated as the product of fasting plasma
nsulin (FPI) and fasting plasma glucose (FPG)ivided by 405. The area of visceral fat and thatf subcutaneous fat at the umbilicus were deter-ined by CT scanning. If the visceral fat area (VFA)as larger than 100 cm2 or the VFA/subcutaneous
at area (SFA) ratio was larger than 0.4, this wasefined as visceral obesity. Body fat mass and leanass were measured by dual energy X-ray absorp-
iometry (DEXA) (Lunar DPX-L, Wisconsin, USA), andhe percent truncal fat mass (%FM trunk) was calcu-ated. The upper limit of %FM trunk was set as 25%or men and 30% for women.
easurement of IMCL and IHL by 1H-MRS
MCL and IHL were measured by 1H-MRS, asescribed previously [4,15,16]. Briefly, imaging andpectroscopy of the tibialis anterior muscle (TA)nd the liver were done with a 1.5-T whole-ody MR system (Intera Achieva; Phillips Medicalystems, Eindhoven, The Netherlands) using aicro coil (4.7 cm in diameter) and a circular
urface coil (17 cm in diameter). The volumesf interest (15 mm × 15 mm × 15 mm for TA and0 mm × 20 mm × 20 mm for the liver) were setithin the right TA (13 cm below the center of
he patella and 1.5 cm lateral) and in segment 6f the liver. The regions of interest were choseno avoid vascular structures and visible adiposeissue. Subjects rested in the supine position dur-ng measurement. Spectra were acquired using aoint-resolved spectroscopy sequence (PRESS) with
repetition time (TR) of 2000 ms, echo time (TE)
atty acids composing intracellular triglycerides at

e324
T. Sato
et al.
Table 2 Clinical characteristics of the subjects.
Subject No. Age (year) Gender BMI(kg/m2)
Waist (cm) AST (IU/L) ALT (IU/L) �-GTP (IU/L) HMW-Ad(�g/mL)
Leptin(ng/mL)
IGF-I SDscore
HOMA-IR VFA (cm2)
1 23 M 18.3 67 18 15 14 2.97 10.1 −1.47 0.58 58.92 24 M 25.7 85 38 18 13 0.5 5.2 −0.88 0.97 99.53 54 M 31.8 95 25 23 15 1.94 4.8 −1.15 0.71 134.34 55 M 22.9 92 31 32 68 0.64 9.1 −0.08 1.42 144.85 46 F 30.5 96 40 34 53 1.16 20.6 −0.78 1.95 92.16 55 F 26.8 85 20 27 26 0.39 14 −3.38 1.99 60.37 64 F 27.8 99 26 30 26 0.65 22.5 −2.47 3.67 160.18 72 F 19.7 80 31 39 16 4.04 9.7 −1.39 0.34 67.29 73 F 22.9 90 24 10 11 5.84 6.4 −3.16 0.44 37.610 75 F 22.3 87 22 8 22 1.46 8.3 −2.91 1.91 115.1Mean 54.1 24.9 87.6 27.7 22.9 26.4 1.96 11.1 −1.77 1.4 97.1SE 5.9 1.4 2.9 2.6 3.6 6.7 0.57 1.9 0.36 0.32 13.1
Subject No. VFA/SFA Body fat(%)
%FMtrunk(%)
IHL(%)
IMCL(mM)
Glucosetolerance
MS Diagnosis Medication other than GH
Cortisone Gonadalsteroids
Thyroxine
1 0.38 34.4 35.5 1.57 280.0 IGT − MPD + + +2 0.58 30.2 31.6 0 571.6 NGT − IGHD − − −3 0.47 33.3 34.7 0.91 131.7 NGT + MPD + + +4 0.99 27.9 30.9 18.1 906.5 NGT + IGHD − − −5 0.21 43.2 42.3 22.2 644.1 NGT + MPD + − +6 0.25 37.5 38.6 22.4 302.3 IGT + IGHD − − −7 0.82 39.7 40 45.4 1550.1 IGT + MPD + − +8 0.43 34.1 35 0 496.1 NGT + MPD + − +9 0.71 32.7 34 9.01 134.8 NGT + MPD + − +10 0.34 31.7 34.4 5.21 271.5 IGT + MPD + − +Mean 0.52 34.5 35.7 12.5 528.8SE 0.08 1.4 1.1 4.6 137.2
BMI, body mass index; HMW-Ad, high molecular weight fraction of adiponectin; VFA, visceral fat area; SFA, subcutaneous fat area; %FM trunk, percent truncal fat mass in the trunkportion; IHL, intrahepatic lipid content; IMCL, intramyocellular lipid content; MS, metabolic syndrome; MPD, multiple pituitary deficiency; IGHD, isolated growth hormone deficiency.

I cle in patients e325
1twwtbIlwlPsowpaattofwrt(
D
TtIstna(saloh(2
S
Rostmadci
Table 3 Results of simple correlation analysis.
HOMA-IR
r p
IHL 0.896 0.0001IMCL 0.749 0.0102VFA 0.585 0.0761VFA/SFA 0.135 0.7199%FM trunk 0.583 0.0775
tS
R
CW(o≥oatpsw(m(6uh(
atast%
ilcHOg7
ntracellular lipid content of liver and skeletal mus
.3 ppm. In skeletal muscle, the methylene pro-on peak of fatty acids from extramyocellular TGithin fat cells infiltrating into the muscle tissueas detected at 1.5 ppm, so we separated these
wo peaks and obtained the specific peak for IMCLy suppression of the water proton peak at 4.6 ppm.n the liver, there was no peak for extracellu-ar free fatty acids, so IHL was measured withoutater suppression. Spectra were fitted and ana-
yzed by using LC-Model software (version 6.2; S.rovencher, PhD, Oakvile, Ontario, Canada) [17],ince Torriani et al. and Skoch et al. have reportedn its use for quantification of IMCL [17,18]. IMCLas estimated by using the unsuppressed watereak as the internal standard, and was expresseds mM. IHL was quantified as a percentage of therea under the methylene proton peak (AUC-CH2)o [AUC-CH2 + that of water peak (AUC-H2O)]. Inen non-obese healthy subjects with normal levelsf transaminases (five men and five women agedrom 23 to 35 years old), the values of IHL and IMCLere 0.69 ± 0.46% and 378.4 ± 51.1 mM (mean ± SE,
espectively). Therefore, we set the mean + 2SD ashe tentative upper limit of normal for IHL and IMCL3.6% for IHL and 685 mM for IMCL).
iagnosis of the metabolic syndrome
he criteria of the modified National Choles-erol Education Program Adult Treatment PanelII (NCEP-ATP III) were used, and metabolicyndrome was diagnosed if at least three ofhe following five were positive: (1) abdomi-al obesity (waist circumference ≥ 90 cm for mennd ≥ 80 cm for women); (2) serum triglyceridesTG) ≥ 150 mg/dL or treatment for dyslipidemia; (3)erum HDL-cholesterol (HDL-C) < 40 mg/dL for mennd <50 mg/dL for women or treatment for dys-ipidemia; (4) systolic blood pressure ≥ 130 mmHgr diastolic blood pressure ≥ 85 mmHg or previousypertension or treatment for hypertension; and5) FPG ≥ 100 mg/dL or previously diagnosed type
diabetes [19].
tatistical analysis
esults are expressed as the mean ± SE. Comparisonf mean values was done by Student’s t-test, Pear-on’s univariate regression analysis was performedo evaluate relationships among obesity-relatedarkers and HOMA-IR. Statistical significance was
ccepted at p < 0.05. All statistical analyses wereone with the Statview 4.5 software package (Aba-us Concepts, Berkeley, CA, USA). All patients gavenformed consent and this study was approved by
msI1
HMW-Ad −0.645 0.0425Leptin 0.795 0.0041
he ethics committee of St. Marianna Universitychool of Medicine.
esults
linical data for the patients are shown in Table 2.hile 50% of the patients were overweight or obese
BMI ≥ 25 kg/m2), 80% of them showed abdominalbesity (waist circumference ≥90 cm for men or80 cm for women). Visceral obesity (VFA ≥ 100 cm2
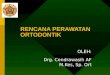
r VFA/SFA > 0.4) was found in 70% of the patientsnd excess of %FM trunk was found in 100% ofhem. IGT was diagnosed in 40% and 80% of theatients met the NCEP-ATP III criteria for MS. Ashown in Fig. 1, the mean IHL of AGHD patientsas significantly higher than that of in controls
12.5 ± 4.6 vs. 0.69 ± 0.46%, p = 0.0330), but theean IMCL did not differ from that of controls
528.8 ± 137.2 vs. 378 ± 51.1 mM, p = 0.2728). While0% of AGHD patients showed a higher IHL than thepper limit for the controls, only 20% of the patientsad an IMCL higher than the upper limit for controlsTable 2).
As shown in Table 3, IHL, IMCL, plasma leptin,nd plasma HMW-Ad, but not VFA, V/S, or %FMrunk, were significantly correlated with HOMA-IR,nd the correlation of IHL with HOMA-IR was thetrongest. IHL was significantly correlated with lep-in (r = 0.858, p = 0.0007), but not with VFA, V/S,FM trunk, or HMW-Ad.
The effects of rhGH treatment for >6 monthsn Cases 1 and 7 are shown in Table 4. Treatmented to a decrease of body weight, BMI, waist cir-umference, VFA, HOMA-IR, TG, and leptin, whileDL-C, HMW-Ad, and IGF-I were increased. TheGTT revealed a marked decrease of 2-h plasmalucose and plasma insulin in both patients. In Case, baseline IHL and IMCL were far higher than the
ean + 2SD of the controls, and both parametershowed a marked decrease after rhGH treatment.n contrast, baseline value of IHL and IMCL in Case
was not above the upper limits for the controls,

e326 T. Sato et al.
Figure 1 Comparison of IHL and IMCL between healthy controls and AGHD patients. Data are expressed as themean ± SE, *p = 0.03301, mean age, mean BMI, and mean waist size in healthy controls were 29.6 ± 1.3 years,20.2 ± 0.7 kg/m2, and 70.6 ± 3.2 cm, respectively.
Table 4 Changes of clinical data with GH replacement therapy.
Case 1 (23 year-old men) Case 7 (64 year-old woman)
Baseline 6M Baseline 6M
BW (kg) 50 48 67.6 63BMI (kg/m2) 18.3 17.6 27.8 26.0Waist (cm) 67 66 99 88VFA (cm2) 58.9 34.5 160.0 112.0VFA/SFA 0.38 0.40 0.82 0.65%FM trunk 35.5 20.0 40.0 41.7IHL (%) 1.57 0 45.4 28.1IMCL (mM) 280 277 1550 726HOMA-IR 0.58 0.53 3.67 1.62TG (mg/dL) 37 25 338 176LDL-C (mg/dL) 124 110 125 146HDL-C (mg/dL) 58 86 43 57HMW-Ad (�g/mL) 2.97 6.64 0.46 0.55Leptin (ng/mL) 10.1 2.3 22.5 10.2IGF-I (ng/mL) 67.0 94.8 86.7 106
Standard value 37—150 85—36975 g-OGTT
Fasting glucose (mg/dL) 88 90 94 91120 min glucose (mg/dL) 147 74 145 88Fasting insulin (�u/mL) 2.7 2.8 14.1 4.4120 min insulin (�u/mL) 69.0 11.7 686 49.8
T
l(ta
Glucose tolerance IGT NG
and IMCL did not change after treatment althoughIHL decreased.
Discussion
The present study had four main findings: (1)most AGHD patients without diabetes or abnormal
Ittt
IGT NGT
evels of aminotransferase showed visceral obesity,2) IHL, but not IMCL, was higher in the patientshan in the controls, and 60% of the patients hadn IHL above the upper limit for controls, (3)
HL was closely correlated with HOMA-IR and lep-in, and (4) a decrease of IHL was observed inwo patients who received 6 M rhGH replacementherapy.
I cle i
sIsCt7dltptritta(fomsaGa(Hadtcto1BdthmthcSa
SepBnpearLm
illiIrphtaoaadiG
giHFmvtHsvapc[vapulf
ipbatrltcvTii
ntracellular lipid content of liver and skeletal mus
Previous studies have shown that visceral obe-ity, MS, and NAFLD are frequent in AGHD patients.chikawa et al. evaluated the presence of hepaticteatosis (defined from the liver/spleen ratio ofT values) in 18 adult patients who had hypopi-uitarism with or without AGHD, and found that
of the 13 patients with AGHD showed liverysfunction, but they did not reported detailedaboratory data or the frequency of diabetes inheir subjects [20]. Hong et al. reported that mostatients with hypopituitarism had fatty liver, butheir liver enzymes were still normal or only slightlyaised [21]. In the present study, we found anncrease of IHL in 60% of AGHD patients, evenhough AST and ALT were in normal, suggestinghat IHL and liver enzymes may not be closelyssociated in AGHD patients. Gamma-GTP levelreference range: <80 IU/L for men and <30 IU/Lor women) was also not elevated in these patientsther than Case 5. The role of GH in hepatic lipidetabolism is currently proposed to be the oppo-
ite of its lipolytic actions in adipose tissue viactivation of hormone-sensitive TG lipase, i.e.,H is thought to induce TG uptake and storagection in the liver by increasing lipoprotein lipaseLPL)/hepatic TG lipase (HTGL) expression [22].owever, GH over-expressing transgenic mice have
decreased hepatic TG content [23], while, GH-eficient humans more frequently have fatty liverhan those with normal GH levels [24]. Moreover,essation of childhood GH therapy on reachinghe final height is associated with developmentf NAFLD in 29% of patients at an average of0 years after stopping therapy [25]. Recently,arkley et al. demonstrated that defective GH-ependent signal transducer and activator ofranscription (STAT)-5 signaling are correlated withepatic steatosis by using dominant-negative STAT5odel mouse hepatoma cells [26]. They proposed
hat GH-dependent STAT5 signaling may preventepatic steatosis, while STAT5 signaling in GH defi-iency may result in the elevation of STAT1 andTAT3 activity and thus lead to intracellular lipidccumulation.
Significant correlation between IHL and IGF-1D score or the GH peak value after insulin tol-rance test (r = −0.221, p = 0.5522 and r = −0.310,
= 0.4326, respectively) was not found in this study.ecause the result is based on the data from smallumber of severe GHD patients, it is impossible torefer true effects of GH depression on IHL. How-ver, there are several reports which GH might have
n essential role in the regulation of the metabolicedox and/or fibrotic status in the liver [13,27,28].arger-scale study including normal subjects andoderate GHD patients is needed.i((a
n patients e327
Nørrelund et al. reported that serum leptin wasncreased in AGHD [29]. Angulo et al. showed thateptin level was correlated with the severity ofiver fibrosis independently of BMI and the sever-ty of insulin resistance in NAFLD patients [30].n the present study, leptin level was closely cor-elated with both IHL and %FM trunk (r = 0.858,
= 0.0004, and r = 0.870, p = 0.0004) and growthormone treatment lowered serum leptin concen-ration, suggesting that a further increase of IHLnd visceral fat in AGHD may lead to aggravationf NAFLD. However, nature of our results does notllow to us to draw conclusions on whether GH have
direct or indirect inhibitory effect of leptin pro-uction. One of the possible mechanism for thencreased leptin level in GHD might be effects ofH on binding proteins or leptin clearance [31].Hypoadiponectinemia also may involve patho-
enesis of IHL accumulation and insulin resistancen GHD patients. Significant correlation betweenMW-Ad and HOMA-IR was observed in this study.urthermore, HMW-Ad (≤4 �g/mL) before treat-ent was low in eight of ten GHD patients with
isceral obesity and it was increased in two GHreated patients. In contrast, Ibánez et al. reportedMW-Ad was high normal in short children bornmall for gestational age who had a normal amountisceral fat [32]. Joaquin et al. showed thatdiponectin level in non-obese or mild obese AGHDatients was comparable to age- and BMI-matchedontrol and it did not change during GH treatment33]. As adiponectin level is strongly influenced byisceral fat mass, difference between our resultnd these studies may result from degree and/orresence of visceral obesity. Consequently it isnlikely that GH deficiency affects adiponectinevel directly and hypoadiponectinemia is a primaryactor of NAFLD in GHD.
In this study, we furthermore found a strong pos-tive correlation of IHL with HOMA-IR (r = 0.896,
= 0.0001) and showed that IHL was decreasedy rhGH treatment in two patients, along with
decrease of HOMA-IR in Case 7 and ameliora-ion of glucose tolerance in both patients. Theseesults suggested that lipid accumulation in theiver may be associated with hepatic insulin resis-ance. Several reports have indicated that IHL canause insulin resistance by promoting the acti-ation of serine kinases in hepatocytes [34,35].he three kinases that are strongly implicated
n the pathogenesis of intracellular fat-inducednsulin resistance are Jun-N-terminal kinase (JNK),
nhibitor of nuclear factor �� (NF-��) kinaseIKK), and novel isoforms of protein kinase CPKC). In the hepatocytes these enzymes arectivated by lipid metabolites generated from
A
WMt1
l
R
[
[
[
e328
intracellular triglycerides, diacylglycerol, long-chain fatty acyl-CoA, ceramide, lisophosphatidicacid, or phosphatidic acid, and phosphorylateregulatory serine residues on the insulin recep-tor substrates IRS-1 and IRS-2, leading to thedown-modulation of insulin-stimulated tyrosinephosphorylation and interfering with the physio-logic actions of insulin in the liver. However, itremains unclear or not whether there is a direct link(not mediated by TG accumulation) between hep-atic insulin resistance and GH deficiency so furtherbasic studies are needed to clarify this point.
Unlike adipose tissue, GH stimulates the uptakeof TG in the skeletal muscle primarily by increas-ing LPL expression, and an excessive muscular TGcontent is found in patients with acromegaly [36].Trepp et al. could not detect any difference ofIMCL measured by 1H-MRS between AGHD patientsand healthy controls, and they observed no changesof IMCL with GH replacement therapy [37]. Thepresent study also showed that IMCL of AGHDpatients was not significantly different from thatof controls, and only 20% of patients were over theupper limit. In Case 7, IMCL decreased after rhGHtherapy, despite no change in Case 2. Exact mech-anism of different change between IMCL and IHL byGH replacement is unknown. Since IMCL may largelydepend on physical activity or diet [37,38], it is dif-ficult to evaluate long term effect of GH on IMCL.It is unclear whether the change observed in Case7 directly reflected the effect of rhGH therapy ornot. Thus, further study of the effect of GH therapyon IMCL is needed.
Previous study demonstrated NAFLD was moreprevalent in postmenopausal and tamoxifen (estro-gen antagonist)-treated women, suggesting thatestrogen deficiency also may associate with NAFLD[39,40]. In this study estrogen was not replaced infour elder women because of age (being older than60 years). However, IHL was increased in patientwith isolated GHD (Case 6). A significant decreaseof IHL was observed in patient (Case 7) who did notreceive estrogen replacement therapy after start-ing rhGH injection. We believe that GHD may playsome role on prevalence and progression of NAFLD.
In conclusion, both visceral fat and IHL (but notIMCL) were increased in non-diabetic AGHD patientswith normal aminotransferase, and IHL was stronglycorrelated with HOMA-IR.
Conflict of interest
The authors state that they have no Conflict ofInterest (COI).
[
T. Sato et al.
cknowledgements
e thank Dr. Yoshifumi Tamura (Department ofedicine, Metabolism, and Endocrinology, Jun-
endo University School of Medicine) for performingH-MRS, and Koji Yasuda (L.A. Systems Inc.) for ana-yzing the LC-Model.
eferences
[1] Gastaldelli A, Miyazaki Y, Pettiti M, Matsuda M, MahankaliS, Santini E, et al. Metabolic effects of visceral fat accu-mulation in type 2 diabetes. J Clin Endocrinol Metab2002;87:5098—103.
[2] Vega GL, Adamas-Huet B, Peshock R, Willett D, Shah B,Grundy SM. Influence of body fat content and distribu-tion on variation in metabolic risk. J Clin Endocrinol Metab2006;91:4459—66.
[3] Korenblat KM, Fabbrini E, Mohammed BS, Klein S. Liver,muscle, and adipose tissue insulin action is directly relatedto intrahepatic triglyceride content in obese subjects. Gas-troenterology 2008;134:1369—75.
[4] Tamura Y, Tanaka Y, Sato F, Choi JB, Watada H, Niwa M, et al.Effects of diet and exercise on muscle and liver intracellu-lar lipid contents and insulin sensitivity in type 2 diabeticpatients. J Clin Endocrinol Metab 2005;90:3191—6.
[5] Sato F, Tamura Y, Watada H, Kumashiro N, Igarashi Y, UchinoH, et al. Effects of diet-induced moderate weight reductionon intrahepatic and intramyocellular triglycerides and glu-cose metabolism in obese subjects. J Clin Endocrinol Metab2007;92:3326—9.
[6] Furukawa K, Katabami T, Nakajima Y, Sato T, Kato H,Koganei R, et al. Evaluation of whole-abdominal fat volumeby 700-slice CT scanning and comparison with the umbili-cal fat area anthropometric indices. Obes Res Clin Pract2010;4:e111—7.
[7] Sada Y, Katabami Y, Asai S, Sato T, Furukawa K, Ishii S, et al.Intrahepatic lipid content is linked to insulin resistance inobese subjects. Obes Res Clin Pract 2011;5:e129—36.
[8] Mersebach H, Feldt-Rasmussen U. Growth hormone andbody composition. Growth hormone deficiency in adults.Front Horm Res 2005;33:185—95.
[9] Jørgensen JO, Pedersen SA, Thuesen L, Jørgensen J,Ingemann-Hansen T, Skakkebaek NE, et al. Beneficialeffects of growth hormone treatment in GH-deficientadults. Lancet 1989;122:1—1225.
10] van der Klaauw AA, Biermasz NR, Feskens EJ, Bos MB, SmitJW, Roelfsema F, et al. The prevalence of the metabolicsyndrome is increased in patients with GH deficiency, irre-spective of long-term substitution with recombinant humanGH. Eur J Endocrinol 2007;156:455—62.
11] Salomon F, Cuneo RC, Hesp R, Sönksen PH. The effects oftreatment with recombinant human growth hormone onbody composition and metabolism in adults with growthhormone deficiency. N Engl J Med 1989;321:1797—803.
12] Chihara K, Shimatsu A, Kato Y, Kohno H, Tanaka T, TakanoK, et al. Growth hormone (GH) effects on central fataccumulation in adult Japanese GH deficient patients: 6-
month fixed-dose effects persist during second 6-monthindividualized-dose phase. Endocr J 2006;53:853—8.13] Takahashi Y, Iida K, Takahashi K, Yoshioka S, Fukuoka H,Takeno R, et al. Growth hormone reverses nonalcoholic

I cle i
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
ntracellular lipid content of liver and skeletal mus
steatohepatitis in a patient with adult growth hormone defi-ciency. Gastroenterology 2007;132:938—43.
14] Targher G, Bertolini L, Padovani R, Rodella S, Tessari R,Zenari L, et al. Prevalence of nonalcoholic fatty liver dis-ease and its association with cardiovascular disease amongtype 2 diabetic patients. Diabetes Care 2007;30:1212—8.
15] Szczepaniak LS, Babcock EE, Schick F, Dobbins RL, Garg A,Burns DK, et al. Measurement of intracellular triglyceridestores by 1H spectroscopy: validation in vivo. Am J Physiol1999;276:E977—89.
16] Provencher SW. Estimation of metabolite concentrationsfrom localized in vivo proton NMR spectra. Magn Reson Med1993;30:672—9.
17] Skoch A, Jíru F, Dezortová M, Dobbins RL, Garg A, BurnsDK, et al. Intramyocellular lipid quantification from 1H longecho time spectra at 1.5 and 3 T by means of the LC-Modeltechnique. J Magn Reson Imaging 2006;23:728—35.
18] Torriani M, Thomas BJ, Halpern EF, Jensen ME, Rosen-thal DI, Palmer WE. Intramyocellular lipid quantifica-tion: repeatability with 1H-MR spectroscopy. Radiology2005;236:609—14.
19] Tan CE, Ma S, Wai D, Chew SK, Tai ES. Can we apply thenational cholesterol education program adult treatmentpanel definition of the metabolic syndrome to Asians? Dia-betes Care 2004;27:1182—6.
20] Ichikawa T, Hamasaki K, Ishikawa H, Ejima E, Eguchi K,Nakao K. Non-alcoholic steatohepatitis and hepatic steato-sis in patients with adult onset growth hormone deficiency.Gut 2003;52:914.
21] Hong JW, Kim JY, Kim YE, Lee EJ. Metabolic parameters andnonalcoholic fatty liver disease hypopituitary men. HormMetab Res 2011;43:48—54.
22] Vijayakurmar A, Novosyadlyy R, Wu Y, Yakar S, LeRoith D.Biological effects of growth hormone on carbohydrate andlipid metabolism. Growth Horm IGF Res 2010;20:1—7.
23] Wang Z, Masternak MM, Al-Regaiey KA, Bartke A. Adipocy-tokines and the regulation of lipid metabolism in GHtransgenic and calorie-restricted mice. Endocrinology2007;148:2845—53.
24] Adams LA, Feldstein A, lindor KD, Angulo P. NAFLD amongpatients with hypothalamic and pituitary dysfunction. Hep-atology 2004;39:909—14.
25] Fukuda I, Hizuka N, Yasumoto K, Morita J, Kurimoto M,Takano K. Metabolic co-morbidities revealed in patientswith childhood-onset adult GH-deficiency after cessationof GH replacement. Endocr J 2008;55:977—84.
26] Barkley JL, Nelson NN, Ishikawa M, Murray LA, Kerr LM,McPhee TR, et al. GH-dependent STAT5 signaling plays animportant role in hepatic lipid metabolism. Endocrinology
2011;152:181—92.27] Loria P, Carulli L, Bertolotti M, Lonardo A. Endocrine andliver interaction: the role of endocrine pathways in NASH.Nat Rev Gastroenterol Hepatol 2009;6:236—47.
[
Available online at www
n patients e329
28] Völzke H, Nauck M, Rettig R, Dörr M, Higham C, BrabantG, et al. Association between hepatic steatosis and serumIGF1 and IGFBP-3 levels in a population-based sample. EurJ Endocrinol 2009;161:705—13.
29] Nørrelund H, Gravholt CH, Englaro P, Blum WF, Rascher W,Chistiansen JS, et al. Increased levels but preserved diur-nal variation of serum leptin in GH-deficient patients: lackof impact of different models of GH administration. Eur JEndocrinol 1998;46:812—7.
30] Angulo P, Alba LM, Petrovic LM, Adams LA, Lindor KD,Jensen MD. Leptin, insulin resistance, and liver fibro-sis in human nonalcoholic fatty liver disease. Hepatology2004;41:943—9.
31] Ozbey N, Algun E, Turgut AS, Orhan Y, Sencer E, MolvalilarS. Serum lipid and leptin concentrations in hypopituitarypatients with growth hormone deficiency. Int J Obes RelatMetab Disord 2000;24:619—26.
32] Ibánez L, López-Bermejo A, Díaz M, Marcos MV, Casano P,de Zegher F. Abdominal fat partitioning and high-molecular-weight adiponectin in short children born small forgestational age. J Clin Endocrinol Metab 2009;94:1049—52.
33] Joaquin C, Aguilera E, Granada ML, Pastor MC, Salinas I,Alonso N, et al. Effects of GH treatment in GH-deficientadults on adiponectin, leptin and pregnancy-associatedplasma protein-A. Eur J Endocrinol 2008;158:483—90.
34] Fabbrini E, Sullivan S, Klein S. Obesity and nonalcoholicfatty liver disease: biochemical, metabolic, and clinicalimplications. Hepatology 2010;51:679—89.
35] Samuel VT, Liu ZX, Wang A, Beddow SA, Geisler JG, Kahn M,et al. Inhibition of protein kinase C epsilon prevents hepaticinsulin resistance in non-alcoholic fatty liver disease. J ClinInvest 2007;117:739—45.
36] Krag MB, Gormsen LC, Guo X, Christiansen JS, Jensen MD,Nielsen S, et al. Growth hormone-induced insulin resistanceis associated with increased intramyocellular triglyceridecontent but unaltered VLDL-triglyceride kinetics. Am JPhysiol 2007;292:E920—7.
37] Trepp R, Fluck M, Stettler C, Boesch C, Ith M, Kreis R, et al.Effect of GH on human skeletal muscle lipid metabolism inGH deficiency. Am J Physiol 2008;294:E1127—34.
38] Tamura Y, Watada H, Igarashi Y, Nomiyama T, Onishi T,Takahashi K, et al. Short-term effects of dietary fat onintramyocellular lipid in sprinters and endurance runners.Metabolism 2008;57:373—9.
39] Gutierrez-Grobe Y, Ponciano-Rodríguez G, Ramos MH, UribeM, Méndez-Sánchez N. Prevalence of non alcoholic fattyliver disease in premenopausal, posmenopausal and poly-cystic ovary syndrome women. The role of estrogens. AnnHepatol 2010;9:402—29.
40] Akhondi-Meybodi M, Mortazavy-Zadah MR, Hashemian Z,
Moaiedi M. Incidence and risk factors for non-alcoholicsteatohepatitis in females treated with tamoxifen forbreast cancer. Arab J Gastroenterol 2011;12:34—6..sciencedirect.com