Embed Size (px)
DESCRIPTION
İngilizce Tıp 4.sınıf öğrencilerine anlattığım ders slaytı. www.sahmay.com www.jinekolojik.org - PowerPoint PPT Presentation
Citation preview

SŞ
Prof.Dr.Sezai ŞAHMAYİ.Ü.Cerrahpaşa Tıp Fakültesi Kadın hastalıkları ve Doğum
ABDReprodüktif Endokrinoloji Bilim Dalı
www.sahmay.com

SŞ

SŞ
INFERTILITY: DefinitionsINFERTILITY: Definitions
Infertility:
failure to achieve conception over a 12-month period of unprotected intercourse
Primary infertility:
never having had a live birth
Secondary infertility:
failure to achieve a live birth after having had a live birth previously

SŞ
Age and FertilityAge and Fertility
Klein NA et al.:Clin Obstet Gynecol 41:912, 1998
20-24 30-34 35-39 40-440
10
20
30
40
50
60
70
6
15
30
64
%

SŞ
Infertility: factsInfertility: facts
Number of infertile couples globally - >100 million.
Associated with :
• - Female factor * 40%
• - Male factor * 30-40%
• - Common to both partners * 15-20%
• - Unexplained 5-10%

SŞ
Risk factorsRisk factors
• Age
• Tobacco smoking
• Alcohol use
• Being overweight ( BMI>35 )
• Too much exercise
• Caffeine intake

SŞ
3.Uterus faktörü
1.Spermin ulaşamaması
2.Yumurtlama olmaması
4.Tüplerin kapalı olması
Başlıca infertilite nedenleri
SŞ
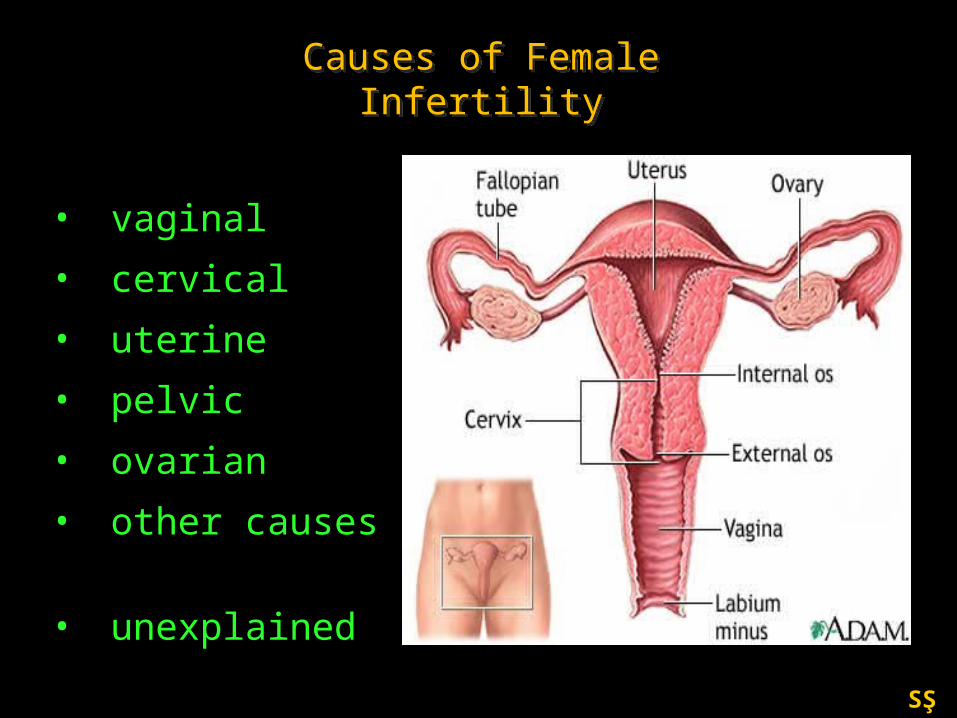
Causes of Female InfertilityCauses of Female Infertility
• vaginal
• cervical
• uterine
• pelvic
• ovarian
• other causes
• unexplained
SŞ
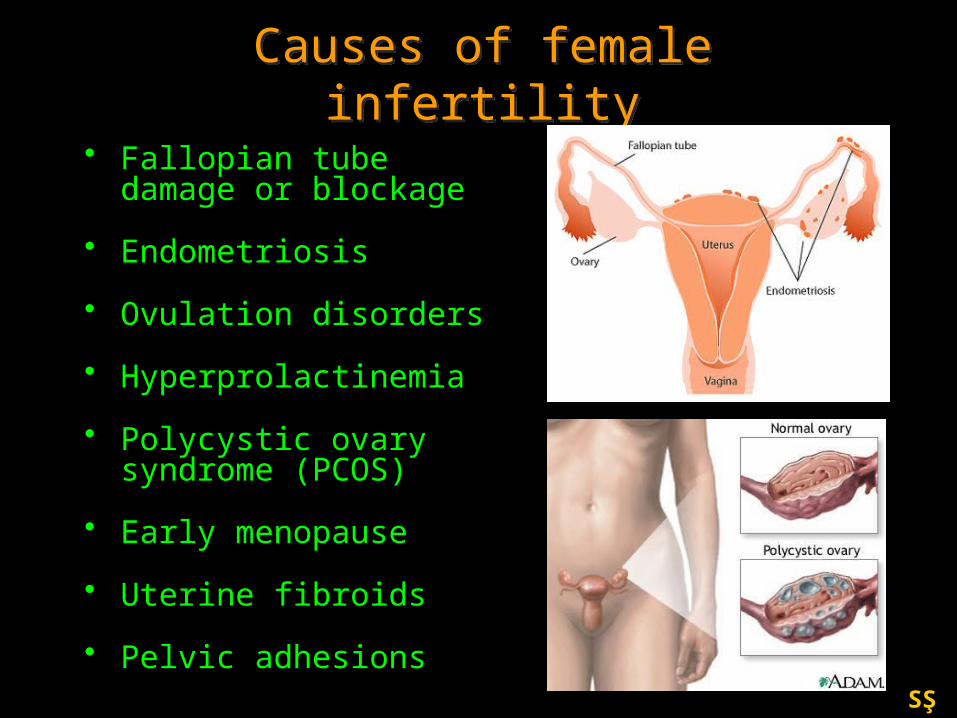
Causes of female infertilityCauses of female infertility
• Fallopian tube damage or blockage
• Endometriosis
• Ovulation disorders
• Hyperprolactinemia
• Polycystic ovary syndrome (PCOS)
• Early menopause
• Uterine fibroids
• Pelvic adhesions

SŞ
coital difficulty
• vaginismus
• vaginal obstruction
• imperforate hymen
• absence of the vagina
• vaginal septum
• gynetresia
• poor erection
• impotence
• premature ejaculation
Vaginal causes

SŞ
cervical infertility
It involves inability of the sperm to pass through the mouth of the uterus due to damage of the cervix.
Causes include the following:
a) Inadequate or inhospitable cervical mucous
b) Cervical narrowing or "stenosis"
c) Infections of the cervix with common sexually transmitted diseases (Chlamydia, gonorrhoea, or trichomonas, as well as mycoplasma hominis and ureaplasma urealyticum)
d) Immune attack of sperm or "sperm allergy" (Antisperm antibodies)
Cervical causes
SŞ
by Leonardo da Vinci of uterus with fetus, circa 1510.

SŞ
• Anatomic problems (polyps, uterine fibroids, abnormal shape of the uterus, septum or "dividing wall" within the uterus)
• Thin or abnormal uterine lining
• Asherman’s syndrome
Uterine causes

SŞ
Tubal DiseaseTubal Disease
•Pelvic Infections•Endometriosis•Pelvic Surgery
SŞ
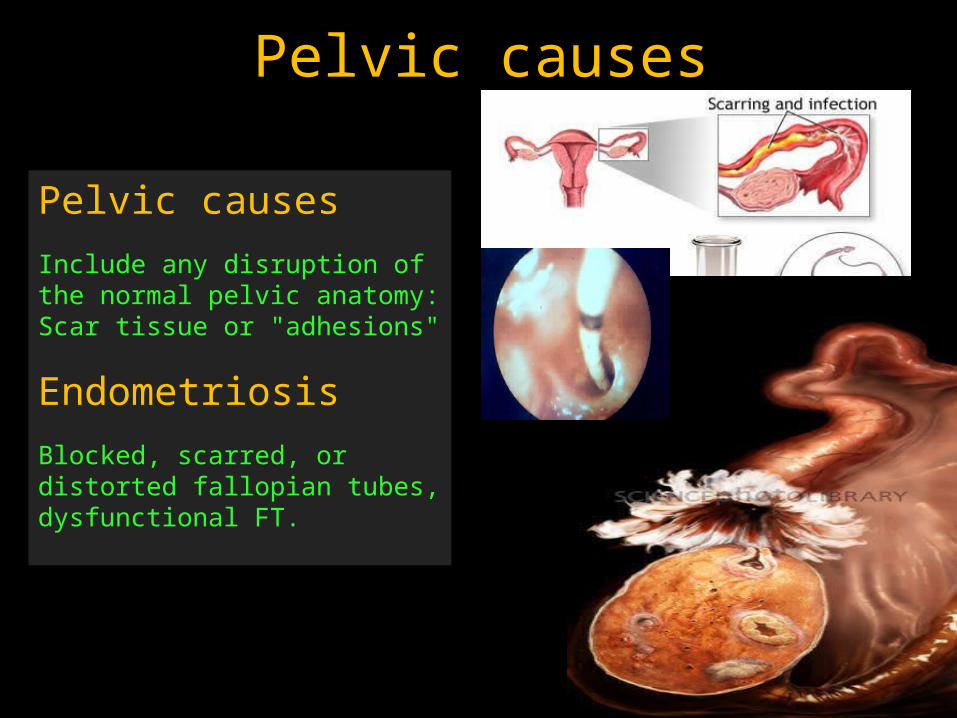
Pelvic causes
Include any disruption of the normal pelvic anatomy: Scar tissue or "adhesions"
Endometriosis
Blocked, scarred, or distorted fallopian tubes, dysfunctional FT.
Pelvic causes

SŞ
Pelvic inflammatory disease (PID) and infertility
Pelvic inflammatory disease (PID) and infertility
Infection of the pelvic organs that cause severe illness and may
lead to tubal blockage and pelvic adhesions leading to infertility
A common sequel to STDs, post-partum and post-abortal
infections and some systematic infections e.g. tuberculosis,
schistosomiasis PID episodes percent
0 1%
1 8%
2 22%
3+ 41%
The risk of tubal factor infertility increases
with each successive episode of PID
SŞ
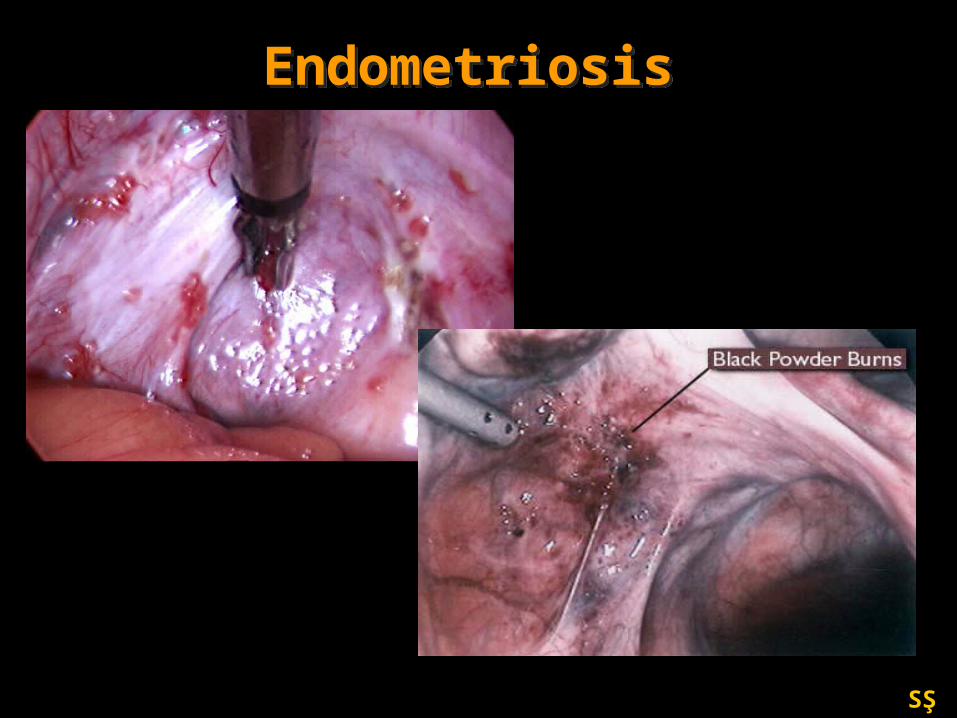
EndometriosisEndometriosis

SŞ
Ovarian Failure PCOS Anovulation Poor ovarian
reserve Premature
Menopause Luteal dysfunction Gonadal dysgenesis Ovarian Cancer
Ovarian Causes of Infertility

SŞ
Cultural and social factorsCultural and social factors
Female genital Mutilation
Early age at marriage or sexual intercourse
Multiple sexual partners (Risk of genital infection)
SŞ
Preventable causesPreventable causes
Infections–STI:
Gonorrhoea,
Syphilis Etc.
Chlamydia,
Infectious And Parasitic Diseases:
Tuberculosis,
Schistosomiasis,
Sickle Cell Disease.

SŞ
Health care practices and policies
Unhygienic obstetric practices
Septic abortion and their complications
Postpartum and postabortal complications
Exposure to potentially toxic substances in:
Environment: arsenic, aflatoxins, pesticides
Diet: caffeine, tobacco, alcohol
Electro-magnetic radiation
Gamma, x-rays etc
Preventable causesPreventable causes

SŞ
PreventionPrevention
Male:
• Avoid alcohol, tobacco and street drugs
• Avoid hot tubs and steam baths
Female:
• Avoid alcohol, tobacco and street drugs
• Exercise moderately
• Avoid weight extremes
• Limit caffeine
• Limit medications
SŞ
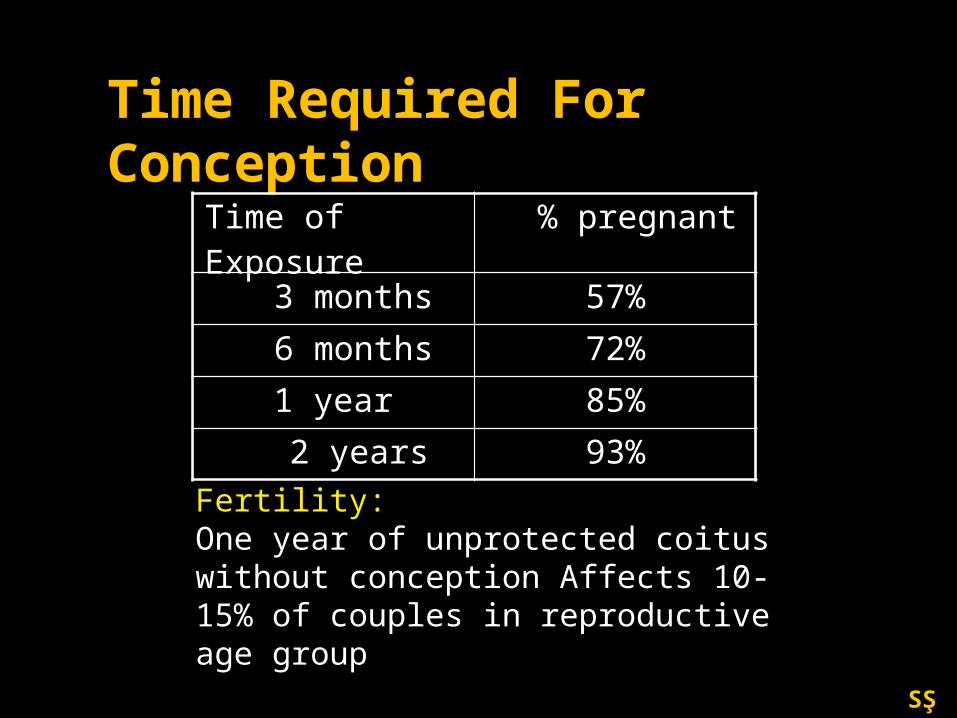
Time Required For Conception
Fertility:One year of unprotected coitus without conception Affects 10-15% of couples in reproductive age group
Time of Exposure % pregnant
3 months 57%
6 months 72%
1 year 85%
2 years 93%

SŞ
When should a work-up begin?
When should a work-up begin?
• Most people need no treatment
• 3 year rule–5% decrease per year in
age –15-25% per year of infertile
• > 35yrs don’t wait• Obvious reasons

SŞ
History and PhysicalHistory and Physical• Sexual History – coital frequency
• Gynecologic History
– menstrual history, pelvic pain, pelvic infections, endometriosis
• Obstetric History
• Medical History
– Thyroid abnormalities, hair growth and acne, nipple discharge
– Childhood illnesses, chicken pox, German measles
• Medications
• Surgical History
– Abdominal and pelvic surgeries
• Social History / Family History

SŞ
Investigations of Infertile CoupleInvestigations of Infertile Couple
• Semen qualitative analysis (sqa)
• Basal Body Temp. charts
• Tubal patency tests (HSG)
• Hormonal tests
• Ultrasonography
• Laparoscopy
• Hysteroscopy

SŞ
Bicornate Polyp
Early Prolif Late Prolif Mid secr

SŞ
Ovulatory dysfunction
Polycystic Ovary
Syndrome (PCOS) 70%
Hyperprolactinemia 10%
Premature ovarian failure 10%
Hypothalamic amenorrhea 10%

SŞ
FOLİKÜLERMATÜRASYON
OVÜLASYON
LÜTEİNİZASYON

SŞ
Infertility: Ovarian FactorInfertility: Ovarian Factor• Menstrual History: 97.7% predictor• BBT
– Thermogenic potential of progesterone (.4-.8)
– Ovulation when see rise (1-5 days after)
– 12 or more days to menses• Progesterone 3-4 ng/mL
– 7-8 days post ovulation– Luteal phase function

SŞ
• Basal Body Temperature• Temperature increases as a result of progesterone
production in the luteal phase of the cycle
• Coincides with an increase in the progesterone level above 4 ng/ml
• A biphasic pattern signifies ovulation
• Temperature taken upon awakening
• Predicts the LH surge only within 2-3 days
First day of the period
Fertile period
Peak luteal P4 level

SŞ
Document Ovulatory Function
• Basal Body Temperature
• Ovulation Predictor Kits
• Day 22-24 Progesterone– Midluteal phase >
3ng/ml
– Preferably >10 ng/ml

SŞ
Velde ER, et al., Maturitas 30 (1998) 119-125
The Declining Follicle Pool

SŞ
• Basal hormonlarFSHÖstradiolİnhibin-BAntimüllerien hormon (AMH)
• Ultrasonik parametrelerAntral Folikül sayısıOver Volümü
• Dinamik testlerCCCT (Clomiphene challenge test)EFORT (Exogenous FSH ovarian reserve test)GAST (GnRH agonist stimulation test)
Over reservinin değerlendirilmesi Over reservinin değerlendirilmesi
Johnson NP et al.:BJOG; 113:1472, 2006

SŞ

SŞ
AMH düzeyi, gebelik oranları ile pozitif ilişkilidir
Sahmay S, Demirayak G, Guralp O, Ocal P, Senturk LM, Oral E, Irez T J Assist Reprod Genet. 29:589–595, 2012

SŞ
Over cevabı-AFS ve AMHOver cevabı-AFS ve AMH
Nelson SM.:Fertil Steril, 2013
SŞ
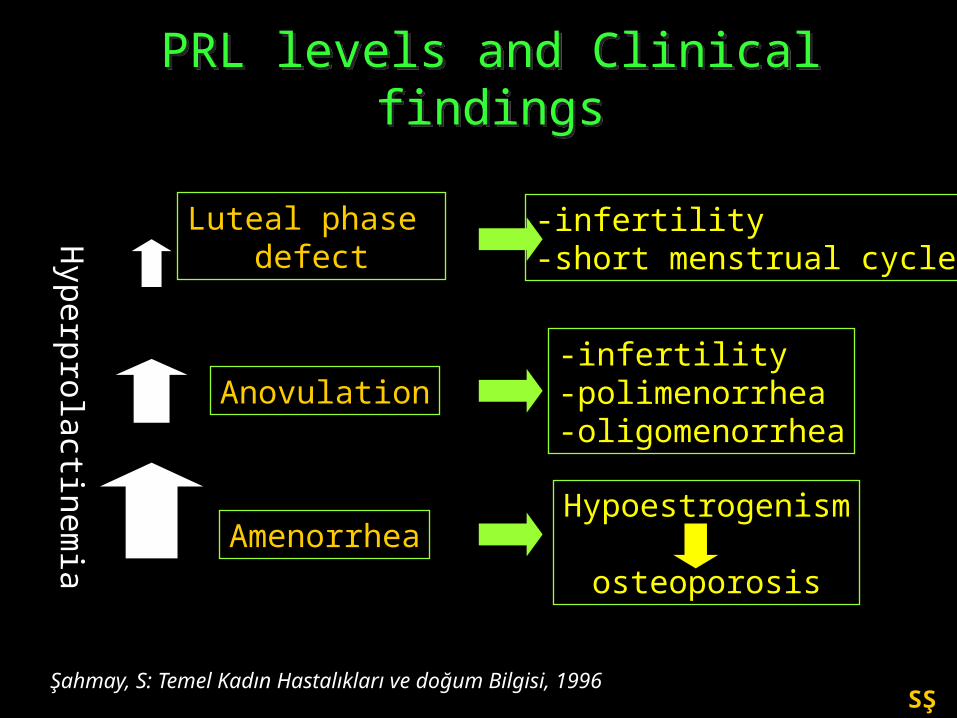
PRL levels and Clinical findingsPRL levels and Clinical findingsH
yperp
rola
ctin
em
ia
AmenorrheaHypoestrogenism
osteoporosis
Anovulation-infertility-polimenorrhea-oligomenorrhea
Luteal phase defect
-infertility-short menstrual cycle
Şahmay, S: Temel Kadın Hastalıkları ve doğum Bilgisi, 1996
SŞ
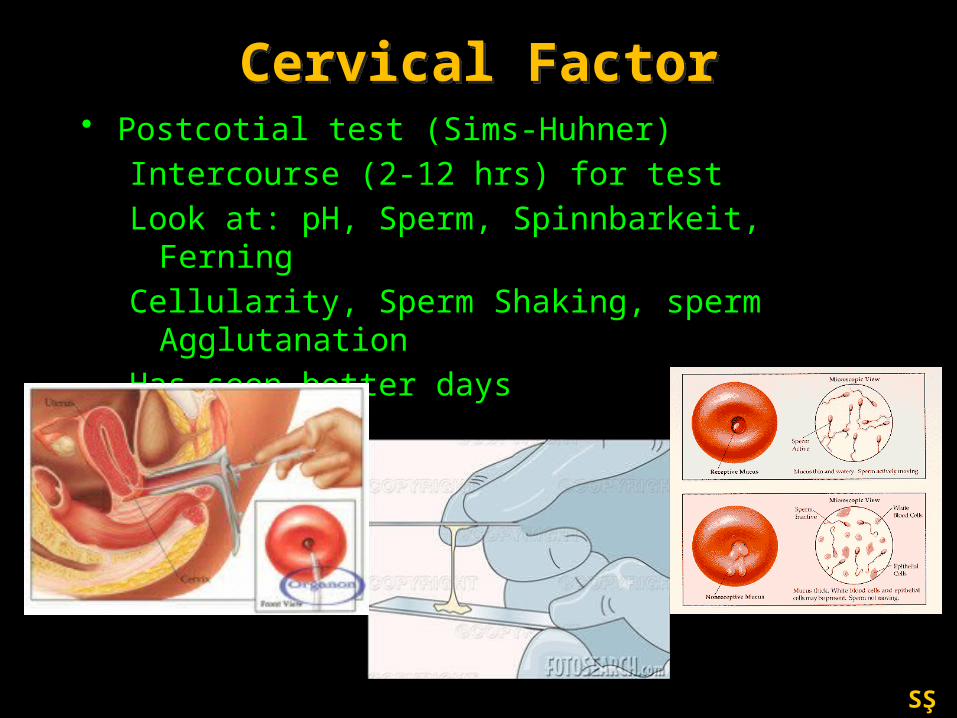
Cervical FactorCervical Factor• Postcotial test (Sims-Huhner)
Intercourse (2-12 hrs) for testLook at: pH, Sperm, Spinnbarkeit, FerningCellularity, Sperm Shaking, sperm
AgglutanationHas seen better days

SŞ
Tubal FactorTubal Factor• Risk factors
–PID; 12%,24%,75%, Ectopic 6 fold
• HSG–2-5 days after menses–1-3 % infection rate high risk– Increase preg rate –False positive obstruction rate
(15-30%)

SŞ
Hydrosalpinges
Myoma
Normal HSG
Anatomic Evaluation Hysterosalpingogram (HSG)

SŞ
LaparoscopyLaparoscopy

SŞ
Hysteroscopy

SŞ
İnfertilitede Tedaviİnfertilitede Tedavi
• Doğru tanı
• Uygun tedavi seçimi
• Yeterli süre tedavi
• Tedavi maliyetinin düşünülmesi
• Çiftin bilgilendirilmesi

SŞ
Gebeliği etkileyen FaktörlerGebeliği etkileyen Faktörler
1. Yaş
2. İnfertilite süresi
3. İnfertilite nedeni
4. Biyolojik belirteçler (AFS, AMH, FSH)
5. Diğer

SŞ
İnfertilitede Tedavi Seçenekleri
İnfertilitede Tedavi Seçenekleri
• Bekle gör
• Ovülasyon belirlenmesi ve ilişki
• Ovülasyon uyarılması
• İntrauterin inseminasyon
• Cerrahi tedavi
• Yardımla üreme teknikleri

SŞ
Ovülasyon İndüksiyonu - TarifOvülasyon İndüksiyonu - Tarif
Ovülasyon İndüksiyonu(Anovülatuar infertil kadınların tedavisi)
Anovülatuar hastalarda, folikül matürasyonu,rüptürü ve fertilize olabilecek nitelikte
oosit oluşumu amacıyla farmakolojik ajanların kullanımı.
Kontrollü Ovarian Hiperstimülasyon(Ovülatuar kadınlarda süperovülasyon)
Ovülatuar veya Anovülatuar hastalarda, Çok sayıda folikül matürasyonu,rüptürü ve fertilize olabilecek nitelikte oosit oluşumu amacıyla farmakolojik ajanların yoğun olarak kullanımı.

SŞ
İntrauterin İnseminasyon (İUİ)

SŞ
Yardımla Üreme TeknolojileriYardımla Üreme TeknolojileriAH (Asisted Hatching)
IVF (In Vitro Fertilization)
GIFT (Gamete Intrafallopian Transfer)
PROST (Pronuclear Stage Tubal Transfer)
TET (Tubal Embryo Transfer )
ZIFT (Zygote Intrafallopian Transfer )
ICSI (Intracytoplasmic sperm injection)
MESA (Microepididymal sperm aspiration)
PESA (Percutaneous epididymal sperm aspiration)PGD (Preimplantation genetic diagnosis)
TESE (Testicular Sperm Extraction)
TET (Tubal embryo transfer)
ZIFT (Zygote intrafallopian transfer)

SŞ
IVF-ET (Tüp Bebek)IVF-ET (Tüp Bebek)
EmbriyoTransferi
ET
Yumurta toplanması
OPU
Yumurtalıkuyarılması
COH
Vücut dışındaDöllenme
IVF

SŞ
Aspirasyon yoluyla Sperm Elde Etmek
Aspirasyon yoluyla Sperm Elde Etmek
Azospermik, nonobstrüktif
hastalarda
TFNA (Testicular Fine Needle Aspiration)
TESA (Testicular Sperm Aspiration)
Azospermik, obstrüktif hastalarda
PESA (Percutaneous epididymal
sperm aspiration)

SŞ
Cerrahi yolla Sperm Elde Etmek
Cerrahi yolla Sperm Elde Etmek
TESE (Testicular sperm extraction)
Mikro-TESE
Azospermik, nonobstrüktif
hastalarda
MESA (Microepididymal sperm
aspiration)
Azospermik, obstrüktif hastalarda

SŞ

SŞ
Complications of infertility treatment
Complications of infertility treatment
• Multiple pregnancy
• Ovarian hyperstimulation syndrome (OHSS)
• Bleeding or infection
• Low birth weight
• Birth defects

SŞ
Summary-1Summary-1
1. Multiple causes must be considered for infertility diagnosis and treatment. Female and male reproductive anatomy and physiology should be reviewed in order to encompass the large differential diagnosis and the different factors that may contribute to infertility or subfertility.

SŞ
Summary-2Summary-2
2. Infertility is defined as one year of unprotected coitus without conception. Infertility may be primary: a woman who has never achieved pregnancy, or secondary: a woman who has achieved pregnancy in the past. Causes of infertility include tubal and pelvic pathology (35%), male problems (35%), ovulatory dysfunctional (15%), unexplained infertility (10%) and unusual problems (10%).

SŞ
Summary-3Summary-3
3. Components of an initial infertility workup include a thorough history and physical examination. Laboratory investigations include a semen analysis to assess male causes of infertility, a method to document that ovulatory cycles are occurring and, often, a hysterosalpingogram to rule out tubal disease.

SŞ
Summary-4Summary-4
4. Disorders of ovulation include polycystic ovarian syndrome (PCOS), hyperprolactinoma, thyroid dysfunction and hypothalamic causes and may be diagnosed by history, as well as laboratory tests that document the occurrence of ovulatory cycles. Basal body temperature recording, urinary LH testing, endometrial biopsy and luteal phase serum progesterone testing are all tests that may help confirm the presence or absence of ovulation.

SŞ
Summary-5Summary-5
5. Dysfunction of the hypothalamic-pituitary-ovarian axis and medical illness, including thyroid disease and pituitary tumors, can cause ovulatory disturbances. Further laboratory workup targeting these problems should be performed when history, examination, and initial laboratory evaluation indicate ovulatory dysfunction. Medication can also cause ovulatory problems.

SŞ
Summary-6Summary-6
6. Ovulatory dysfunction may sometimes be treated with correction of medical disease or change of medications. Most often, ovulatory dysfunction is treated empirically with ovulation induction agents such as clomiphene citrate. A thorough understanding of the normal physiology and pathophysiology of the menstrual cycle aids greatly in the understanding of ovulatory dysfunction.

SŞ
Summary-7Summary-7
7. Management of tubal disease is often surgical, including lysis of adhesions and removal of tubal obstruction via either laparoscopy or laparotomy, depending on the severity of the disease.
8. Male fertility problems include varicocele, duct obstruction, sperm antibodies, hypogonadism, testicular hyperthermia, drug use and industrial pollutants.

SŞ

SŞ
Adaleti çiğneyen devlet adamlarını cezalandırmayan milletler çökmek zorundadır. Hz. MUHAMMED
Fenalıkların ilki ve en büyüğü,haksızlıkların cezasız kalmasıdır. EFLATUN
Adaletin kuvvetli, kuvvetlilerin de adaletli olmaları gerekir.Blaise PASCAL
www.sahmay.com