-
Kim Chong Hwa MD,PhD
Sejong general hospital, Division of endocrine &
metabolism
-
Classification and definition of diabetic neuropathies
Painful diabetic peripheral neuropathy
Diabetic autonomic neuropathy
Emerging markers of DPN: focus on small fiber
st1
-
2
st1 stesfaye, 2010-10-16
-
The Toronto Diabetic Neuropathy Expert Group Meeting - 2009
-
Introduction to TDNEG meeting
Diagnosis of DSPN for clinical practice & research
Risk reduction
Pain treatments
Pathogenic treatments
Conclusions
The Toronto Diabetic Neuropathy Expert Group Meeting - 2009The
Toronto Diabetic Neuropathy Expert Group Meeting - 2009
-
The Toronto Diabetic Neuropathy Expert Group Meeting - 2009The
Toronto Diabetic Neuropathy Expert Group Meeting - 2009
Introduction to TDNEG meeting
Diagnosis of DSPN for clinical practice & research
Risk reduction
Pain treatments
Pathogenic treatments
Conclusions
-
Focal and Multifocal
neuropathies
Diabetic Polyneuropathy (DPN)
Entrapmenteg median ulnar peroneal
Distal Symmetrical Polyneuropathy (DSPN)
(Typical DPN)
Multiple lesionsmononeuritis multiplex
Radiculoplexus neuropathies: LS, thoracic, cervical
Mono-neuropathy
AtypicalDPNs
Autonomic
Classification of Diabetic Polyneuropathy (DPN): Classification
of Diabetic Polyneuropathy (DPN):
The Toronto Diabetic Neuropathy Expert Group Meeting The Toronto
Diabetic Neuropathy Expert Group Meeting
-
1 APN of poor glycemic control
2 APN of rapid glycemic control
Atypical DPNs: Acute Painful NeuropathiesAtypical DPNs: Acute
Painful Neuropathies
Acute onset within weeks; in both Type 1 and 2DM
Persistent burning and shooting pain, allodynia, and
hyperalgesia +++
Nocturnal exacerbation of symptoms and depression
Often severe weight loss
Sensory loss is mild or absent
May be impotence and autonomic neuropathy
Nerve conduction studies are normal or mildly impaired
TDT is usually impaired
Complete resolution of symptoms within 1 year
Treatment: same as chronic PN; BSC; reassurance APN = Acute
painful neuropathies; BSC = Best supportive care; PN =
Polyneuropathy;
TDT = Transmission disequilibrium test.Tesfaye et al.
Diabetologia 1996
-
Distal Symmetrical
Polyneuropathythy
(DSPN) 50% of DM
Associated with retinopathy &
nephropathy
Microvascular complications are
preventable by rigorous glycemic
control
Risk covariates are CVR and chronic
glycemic exposure
strongest risk factor for foot
ulcer(FU) and amputation
Symmetric, length dependent,
sensory-motor neuropathy Diabetes Care 2010; 33: 2285-93
-
1.Clinical practice
- Identification of those at risk for FU
2. Epidemiological studies
3.Research Studies
- RCTs, Longitudinal Studies
- Accurate quantification of severity
Diagnosis of DSPN
Tesfaye et al. Diabetes Care 2010; 33: 2285-93
-
Symptoms of DSPN
Sensory symptoms Numbness
Paraesthesia
Pain (burning, stabbing, shooting, deep aching)
Unusual sensations (tightly wrapped, swelling, etc)
Allodynia
Inability to identify objects in hands
Motor symptoms Difficulty climbing stairs
Difficulty lifting/handling small objects
-
Sensory modality Nerve fiber Instrument
Vibration A (large) 128Hz TF
Pain (pinprick) C (small) Neuro-tips
Pressure A, A (large) 10g MF
Light touch A, A (large) Wisp of cotton
Cold A (small) Cold TF
Examination:Bedside sensory tests
-
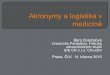
10g Monofilament
Inexpensive, easy to use,
rapid and reproducible.Smieja et al. J Gen Intel Med 1999
Dorsum 1st toe.
Score 0-8.
5/8 - probability of DPNPerkins et al. Diabetes Care 2001
Predicts foot ulceration. 3 year
RR for foot ulceration = 15Rith-Najarian et al. Diabetes Care
1992
-
Clinical assessment: SummaryClinical assessment: Summary
History Signs
Sensory symptoms
Motor symptoms
Assessment of disability
Exclude other causes
of neuropathy
InspectionReflexes
Sensory
vibration
light touch
pinprick
10g Monofilament
Assess footwear
-
Scored clinical assessment: useful in epidemiological
studies
Neuropathy Disability Score(NDS)
Toronto Clinical Scoring System(TCSS)
Michigan Neuropathy Scoring
Instrument(MNSI)
1.
2.
3.
-
Neuropathy Disability Score Neuropathy Disability Score
pain (neuro-tips) 0-1
vibration (128Hz TF) 0-1
warm / cold rods 0-1
ankle reflexes 0-1-2
maximum score = 10
Over 2 years RR CI
Previous FU 3.1 (2.2 - 4.3)
NDS 6/10 2.2 (1.6 - 3.4)
Abnormal 10g MF 1.8 (1.4 - 2.4)
Abnormal ankle reflex 1.6 (1.2 - 2.0)
NW England Study (n=9710)
Young et al. Diabetologia 1993
Abbott et al. Diab Medicine 2002
-
Quantitative sensory tests:Quantitative sensory tests:
Thresholds for:
vibration
thermal
heat - pain
cold - pain
touch - pressure
electrical impulses
Thermal testing small fiber function
cold
warm
provide quantitative measures of sensationprovide quantitative
measures of sensation
-
Strengths
measures both small fibre and large fiber deficit
relatively simple, less discomfort
useful tool for screening large populations
Limitations
less objective (psychophysical)
less reproducible
no standardization of various systems
(reliant on normative values for each lab)
Report of Am Acad Neurol, Neurology 2003
Quantitative sensory testing:Quantitative sensory testing:
-
Vibration Perception Threshold:useful in epidemiological
studiesVibration Perception Threshold:useful in epidemiological
studies
Detects sub-clinical DPN
Predicts foot ulceration
0-15V - low risk
16-25V - intermediate
>25V - high risk (x7)
Young et al. Diabetes Care 1994
Abbott et al. Diabetes Care 1998
Predicts mortality
Coppini et al. J Clin Epidemiol 2000
-
Nerve conduction studies:
Strengths most objective, accurate, reproducible, sensitive
Daube JR 1999
correlate with clinical endpoints Perkins et al. 2001
represent pathological hallmark of DSPN Malik et al. 1989
diagnostic sensitivity improved by incorporation
of anthropometric factors, F-wave testing etc.
Limitations measures only large fiber function
limited availability for routine testing
some discomfort
impact of external factors (eg limb temp. etc)
Essential for research studies of DSPNEssential for research
studies of DSPN
-
Diagnostic certainty of DSPN
Possible
Symptoms or signs of DSPN
Probable
Symptoms and signs of DSPN
Confirmed
Symptoms or signs of DSPN and NC abnormality
Subclinical
NC abnormality only
Possible
Symptoms or signs of DSPN
Probable
Symptoms and signs of DSPN
Confirmed
Symptoms or signs of DSPN and NC abnormality
Subclinical
NC abnormality only
The Toronto Diabetic Neuropathy Expert Group Meeting The Toronto
Diabetic Neuropathy Expert Group Meeting
Tesfaye et al. Diabetes Care 2010; 33: 2285-93
-
Staging DSPNusing confirmed DSPN criteria
Grade 0 = no abnormality of NC, e.g., 5 NC nds < 95th
percentile or
another suitable NC criterion.
Grade 1a = abnormality of NC, e.g., 5 NC nds 95th
percentile,
without symptoms or signs.
Grade 1b = NC abnormality of 1a plus neurologic signs but
without
symptoms.
Grade 2a = NC abnormality of 1a with or without signs (but if
present
less than 2b) and with symptoms.
Grade 2b = NC abnormality of 1a, a moderate degree of
weakness
(i.e., 50%) of ankle dorsiflexion with or without symptoms
Tesfaye et al. Diabetes Care 2010; 33: 2285-93
-
Is clinical examination of the PNS reliable for research
studies?
Clinical vs Neurophysiological Trial 1
Dyck et al., Muscle and Nerve 2010; 42:157-64.
-
1. Clinical diagnoses is not always reprodiceableeven when
performed by experts!
2. Specific approaches to improving proficiency (clinical exam
or NC) are needed and should be tested.
Conclusions from the Clinical vs Neurophysiological Trial 1
Dyck et al., Muscle and Nerve 2010; 42:157-64.
-
Emerging markers of DPN:
Focus on small fibers
Nerve biopsy - unmyelinsted fiber damage, invasive, highly
specilaized procedure-EM
Skin biopsy - minimally invasive, morphometricquantification of
intraepidermal nerve fibers(IENF)-number of IENF per length of
section(IENF/mm)
Corneal confocal microscopy - noninvasive, small sensory corneal
nerve fiber
Nerve axon reflex/flare response C-nociceptivefiber, laser
Doppler imaging flare test
-
Definition of Small fiber neuropathy(SFN)
Possible : presence of length-dependent symptoms and/or clinical
signs of small fiber damage
Probable : presence of length-dependent symptoms, clinical signs
of small fiber damage, and normal sural NC study
Definite : presence of length-dependent symptoms, clinical signs
of small fiber damage, normal sural NC study, and altered IENF
density at the ankle and /or abnormal quantitative sensory testing
thermal thresholds at the foot
-
The Toronto Diabetic Neuropathy Expert Group Meeting - 2009The
Toronto Diabetic Neuropathy Expert Group Meeting - 2009
Introduction to TDNEG meeting
Diagnosis of DSPN for clinical practice & research
Risk reduction
Pain treatments
Pathogenic treatments
Conclusions
-
NeuropathyDiabetic Control
Nerve Fiber Loss: The cause of insensitivity in DPN1
1. Veves A, Giurini JM, Logerfo JW. Diabetic Foot. 2nd Edition,
Chapter: Diabetic Neuropathy, p10529
-
Photomicrographs of capillaries from nerve biopsies showing a
closed capillary in the diabetic nerve
Microvascular defects in DPN1
DPNDiabetic Control
1. Cameron NA, et al. Diabetologia. 2001;44:197388
-
Control DPN
1. Tesfaye S, et al. Diabetologia. 1993;36:126674
Microvascular abnormalities in DPN1
-
Impaired blood flow in established DPN1
Normal Established DPN
1. Tesfaye S, et al. Diabetologia. 1993;36:126674
-
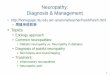
Risk factors for incident neuropathy:The EURODIAB PCS
Risk factors for incident neuropathy:The EURODIAB PCS
Tesfaye et al. N Engl J Med 2005; 352: 341-50
Total cholesterol
Triglycerides
BMI
Diabetes duration
Change in HbA1c
HbA1c
Smoking
Hypertension1.57
1.38
1.48
1.36
1.40
1.27
1.21
1.15
Model 1:
without CVD
and retinopathy
Odds ratios (95% CI)Odds ratios (95% CI)
n=1101 with type 1 DM; FU: 7.30.6 yrs
-
Glycaemic control and
management of cardiovascular
risk factors are important
The Toronto Diabetic Neuropathy Expert Group Meeting - 2009
The Toronto Diabetic Neuropathy Expert Group Meeting - 2009
-
The diagnosis of DSPN depends on whether it is in the context of
clinical practice or research
In research studies: Diagnosis of DSPN does not suffice severity
must also be estimated.
Neurologists and diabetologists need to reconsider how to more
validly and reproducibly diagnose DSPN and estimate severity.
CVR factors appear to be important in the pathogensis of
DSPN
Conclusions
-
Thanks for your attention