Embed Size (px)
Citation preview
Kollagenosen Update 2017
Prof. Dr. Oliver Distler
Klinik für Rheumatologie
UniversitätsSpital Zürich

Wir decken die gesamte Rheumatologie ab
Alle rheumatologischen Tätigkeitsfelder
• Entzündliche Gelenkerkrankungen inkl. Ultraschall
• Degenerative Erkrankungen
• Lokale muskuloskelettale Erkrankungen
• Rückenerkrankungen
• Systemerkrankungen
• Biologika-Therapien
• Kapillarmikroskopie
• DEXA
• Wirbelsäuleninfiltrationen
• Stosswellen

Das neue Team in der Rheumatologie
Adrian CiureaArthritiden
Biologika
Britta MaurerKollagenosen und
Vaskulitiden
Lukas WildiArthrosen
Rückenerkrankungen
Sandra BlumhardtUltraschall
Wirbelsäuleninfiltrationen
Stosswellen
Diana FreyOsteoporose

Das neue Team in der Rheumatologie
Julio SanchezNotfallmedizin
Wirbelsäuleninfiltrationen
Stosswellen
Manuela di ChiaraLupus
UltraschallMike BeckerVaskulitiden
Kollagenosen
Andreas KrebsUltraschall

Multimodale Komplextherapie
15 Tage stationäre Intensivtherapie
Umfassendes muskuloskelettales Assessment
Analgetische Einstellung
Physiotherapie, Ergotherapie, Psychiatrie, Sozialdienst, ggf.
Neurochirurgie, Schmerzdienst
Aktive und passive Therapie, Haltungsschulung, Stabilisation
Patientenedukation

Universitäre Klinik für Rheumatologie
Abteilung für Physikalische
Medizin und Rheumatologie
Balgrist
Rheumaklinik
USZ
Forschung
Schlieren
Balgrist
EULAR Center of Excellence
KollagenosenChronisch-entzündliche Systemerkrankungen
• Systemische Sklerose
• Systemischer Lupus erythematodes (SLE)
• Polymyositis/Dermatomyositis
• Sjögren-Syndrom
• Mischkollagenose (U1-RNP-Antikörper)
• Undifferenzierte Kollagenose
• Overlap-Syndrome
Kollagenosen - Klassifikation
SLE Polymyositis SSc Sjögren MCTD
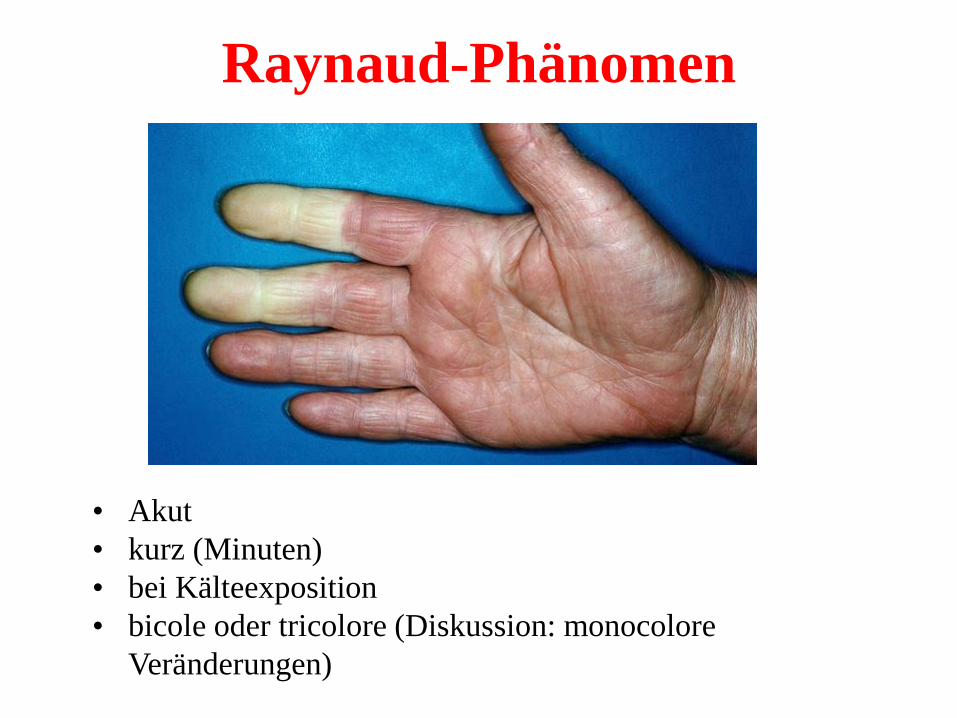
Raynaud-Phänomen
• Akut
• kurz (Minuten)
• bei Kälteexposition
• bicole oder tricolore (Diskussion: monocolore
Veränderungen)
Kein Raynaud-Phänomen
Allgemein kalte Hände
Bei Wärme werden meine Hände rot
Ich habe häufiger weissliche Verfärbungen
Meine Finger kribbeln, vor allem wenn ich mich aufrege
Im Zweifelsfall: Dokumentation (Smartphone)
Häufigkeit Raynaud bei
Kollagenosen
Mischkollagenose: Sehr, sehr häufig
Systemische Sklerose: Sehr, sehr häufig
Systemischer Lupus erythematodes: Seltener
Sjögren-Syndrom: Seltener
Polymyositis/Dermatomyositis: Seltener
Einfacher Ausschluss
Kollagenose bei Raynaud
1. Antinukleäre Antikörper, Spezifizierung
2. Kapillarmikroskopie
Beide negativ: < 1% Wahrscheinlichkeit
Eines positiv: 25% Wahrscheinlichkeit
Beide positiv: 75% Wahrscheinlichkeit

Kapillarmikroskopie zeigt
Mikroangiopathie
SSc
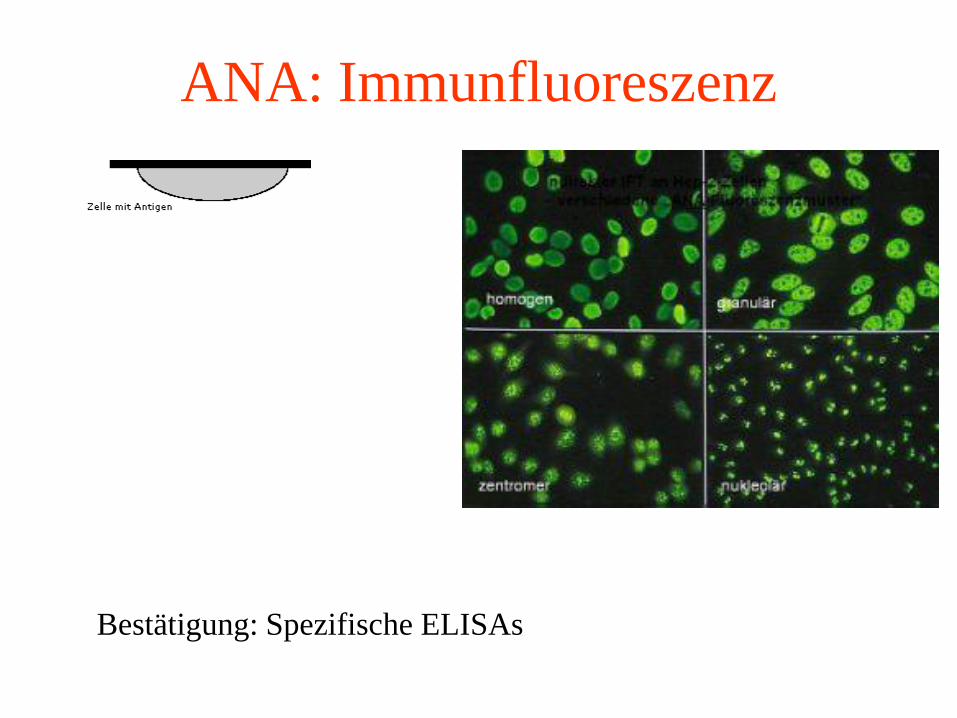
ANA: Immunfluoreszenz
Bestätigung: Spezifische ELISAs
A patient with
A patient with systemic
sclerosis and digital ulcers
Case - background
• 38 yo white female
• Disease duration: 15 years from first non Raynaud symptom
• ANA 1: 5120, anti-Scl-70 antibodies
• Diffuse skin fibrosis, mRSS 22/51, recently progressive (Rituximab)
• Organs:
- Mild ILD (CT Thorax < 10%, FVC 80%, DLCO 63%), echocardiography: unremarkable, NT-pro-BNP 183 (<130), Dyspnoea NYHA 1-2
- GI: Reflux, bloating
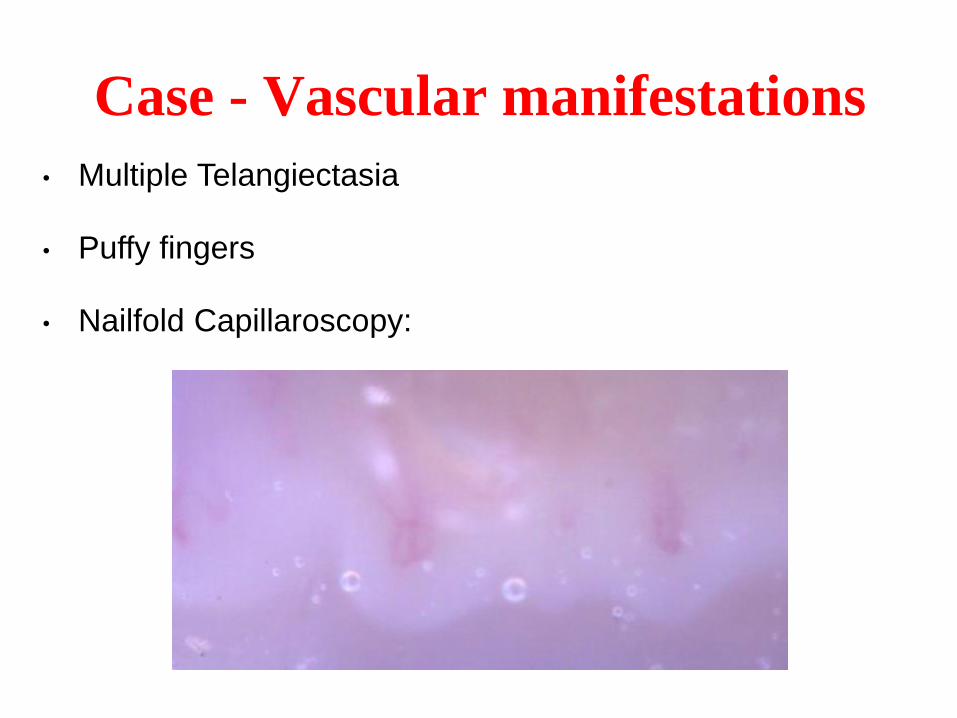
Case - Vascular manifestations
• Multiple Telangiectasia
• Puffy fingers
• Nailfold Capillaroscopy:
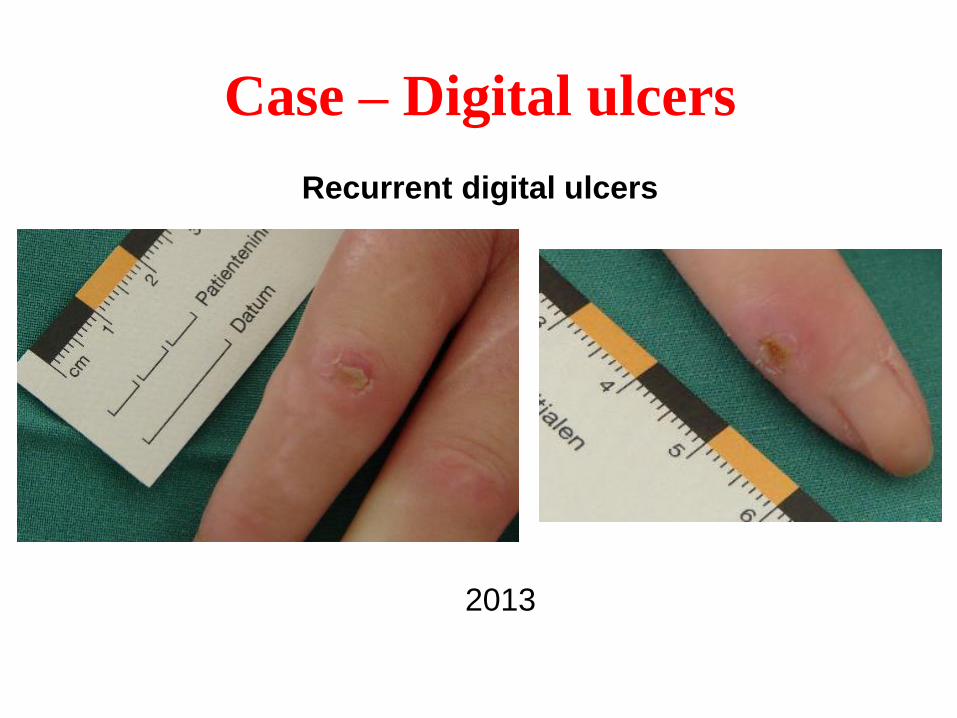
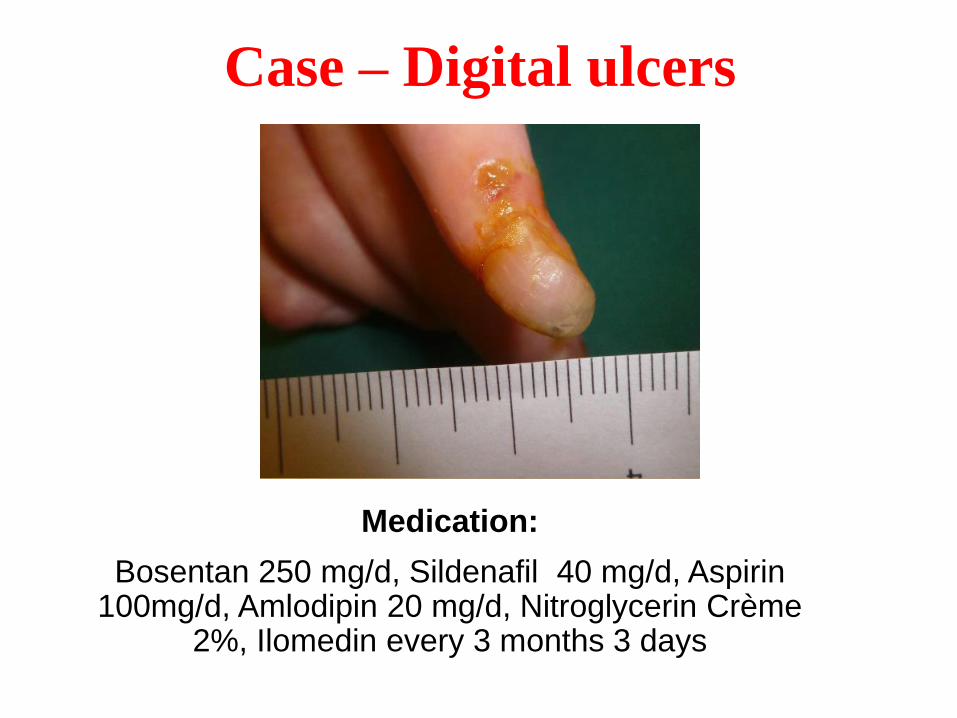
Case – Digital ulcers
Recurrent digital ulcers
2013
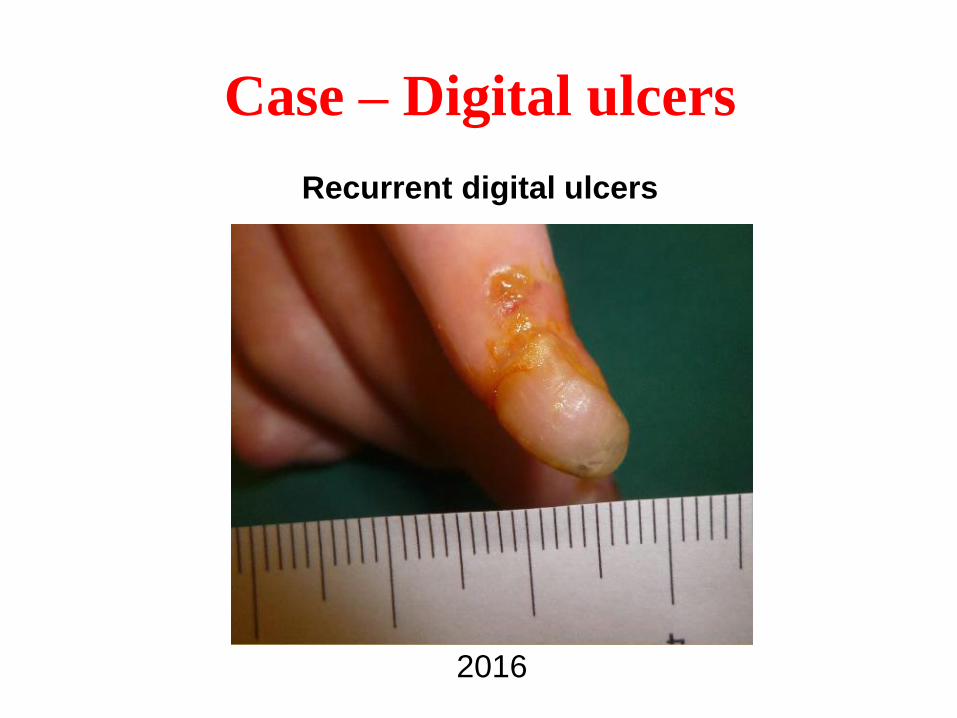
Case – Digital ulcers
Recurrent digital ulcers
2016
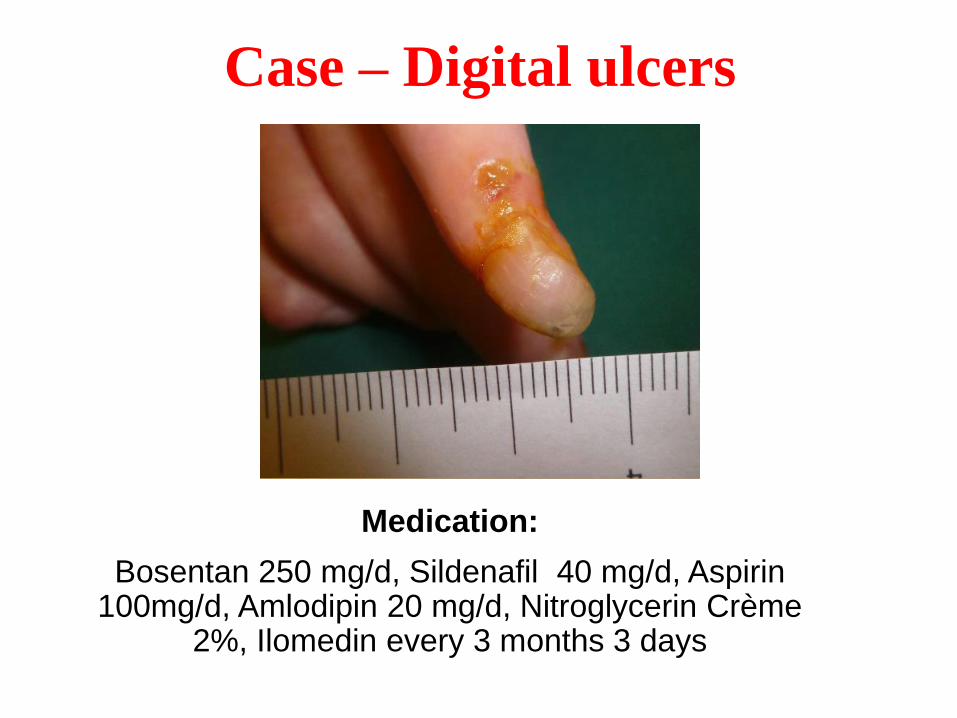
Case – Digital ulcers
Medication:
Bosentan 250 mg/d, Sildenafil 40 mg/d, Aspirin 100mg/d, Amlodipin 20 mg/d, Nitroglycerin Crème
2%, Ilomedin every 3 months 3 days
SSc 4 - 23
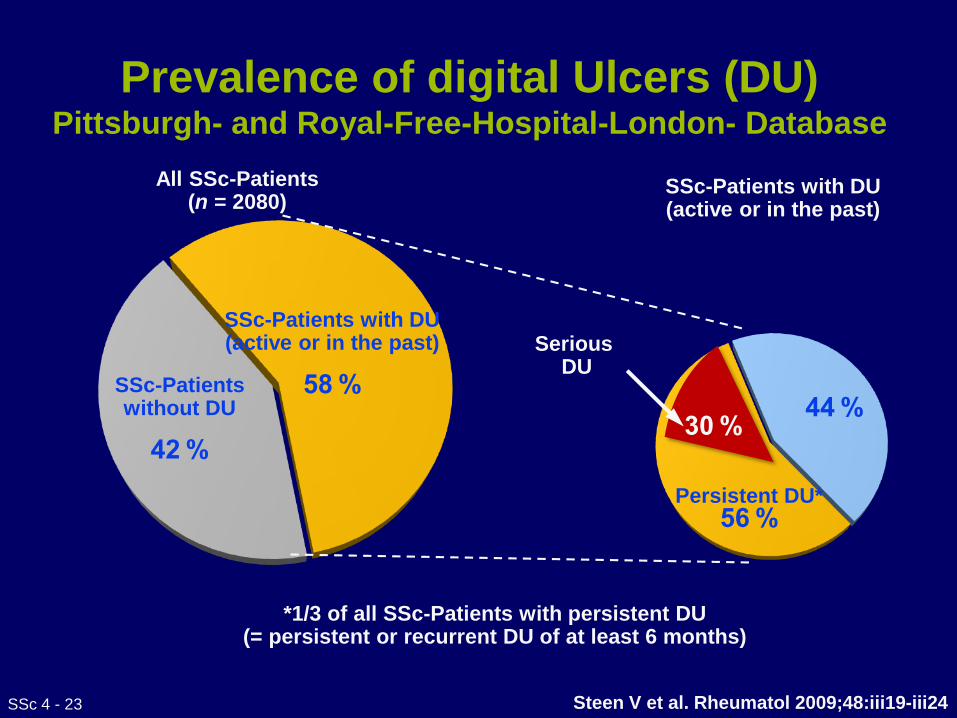
Prevalence of digital Ulcers (DU) Pittsburgh- and Royal-Free-Hospital-London- Database
*1/3 of all SSc-Patients with persistent DU(= persistent or recurrent DU of at least 6 months)
All SSc-Patients(n = 2080)
SSc-Patients with DU (active or in the past)
58 %SSc-Patientswithout DU
42 %
SSc-Patients with DU(active or in the past)
30 %44 %
Persistent DU* 56 %
SeriousDU
Steen V et al. Rheumatol 2009;48:iii19-iii24
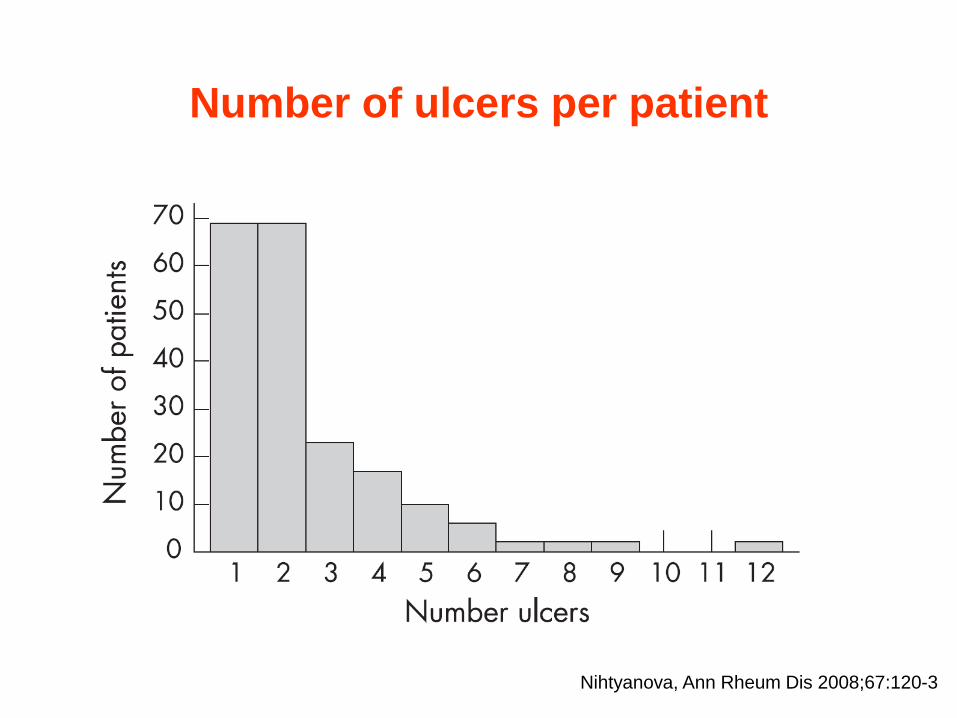
Number of ulcers per patient
Nihtyanova, Ann Rheum Dis 2008;67:120-3
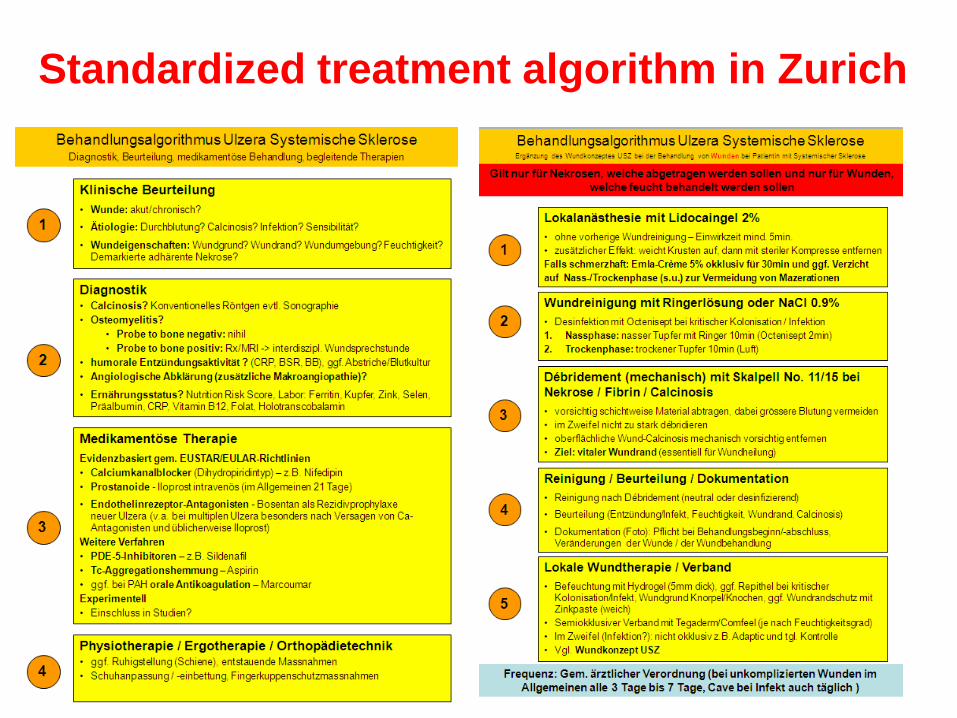
Standardized treatment algorithm in Zurich
EULAR treatment
recommendations 2016
In press
Annals of the Rheumatic Diseases
Two RCTs indicate that intravenous iloprost is efficacious in healing digital ulcers in patients
with SSc.
Intravenous iloprost should be considered in the treatment of digital ulcers in patients with SSc.
Intravenous iloprost should be considered in particular in SSc patients with DUs not responding to oral therapy
SSc 4 - 28
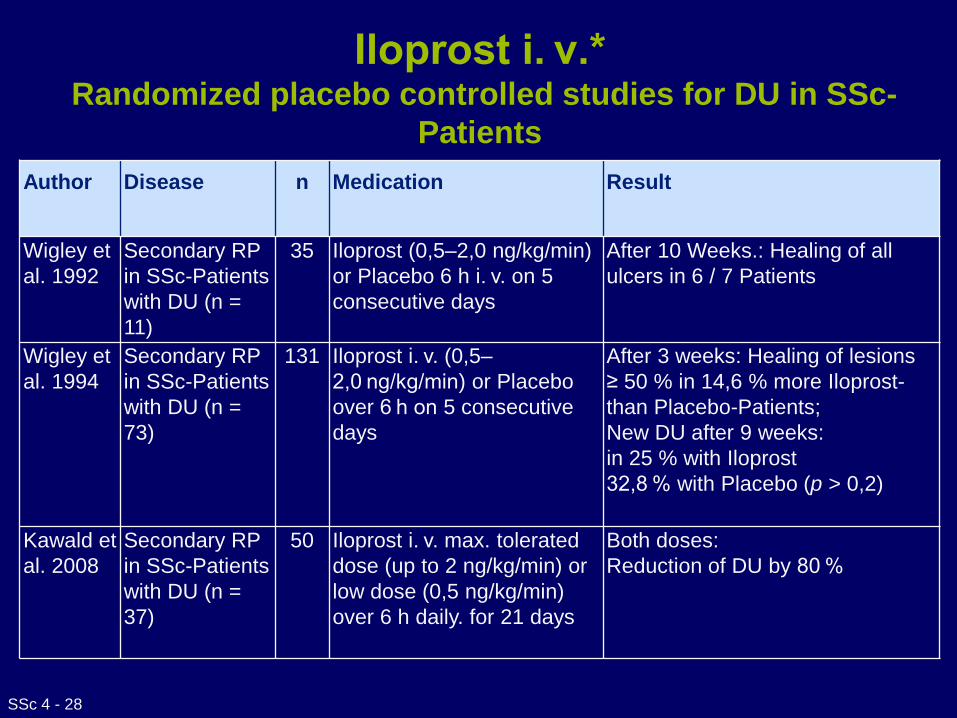
Iloprost i. v.*Randomized placebo controlled studies for DU in SSc-
Patients
Author Disease n Medication Result
Wigley et
al. 1992
Secondary RP
in SSc-Patients
with DU (n =
11)
35 Iloprost (0,5–2,0 ng/kg/min)
or Placebo 6 h i. v. on 5
consecutive days
After 10 Weeks.: Healing of all
ulcers in 6 / 7 Patients
Wigley et
al. 1994
Secondary RP
in SSc-Patients
with DU (n =
73)
131 Iloprost i. v. (0,5–
2,0 ng/kg/min) or Placebo
over 6 h on 5 consecutive
days
After 3 weeks: Healing of lesions
≥ 50 % in 14,6 % more Iloprost-
than Placebo-Patients;
New DU after 9 weeks:
in 25 % with Iloprost
32,8 % with Placebo (p > 0,2)
Kawald et
al. 2008
Secondary RP
in SSc-Patients
with DU (n =
37)
50 Iloprost i. v. max. tolerated
dose (up to 2 ng/kg/min) or
low dose (0,5 ng/kg/min)
over 6 h daily. for 21 days
Both doses:
Reduction of DU by 80 %
A A meta-analysis of 3 RCTs and results of an independent RCT indicate that PDE-5
inhibitors improve healing of digital ulcers in patients with SSc.
Moreover, the results of one small RCT indicate that PDE-5 inhibitors may prevent development of new digital ulcers in SSc.
PDE-5 inhibitors should be considered in the treatment of digital ulcers in SSc patients.
SSc 4 - 30
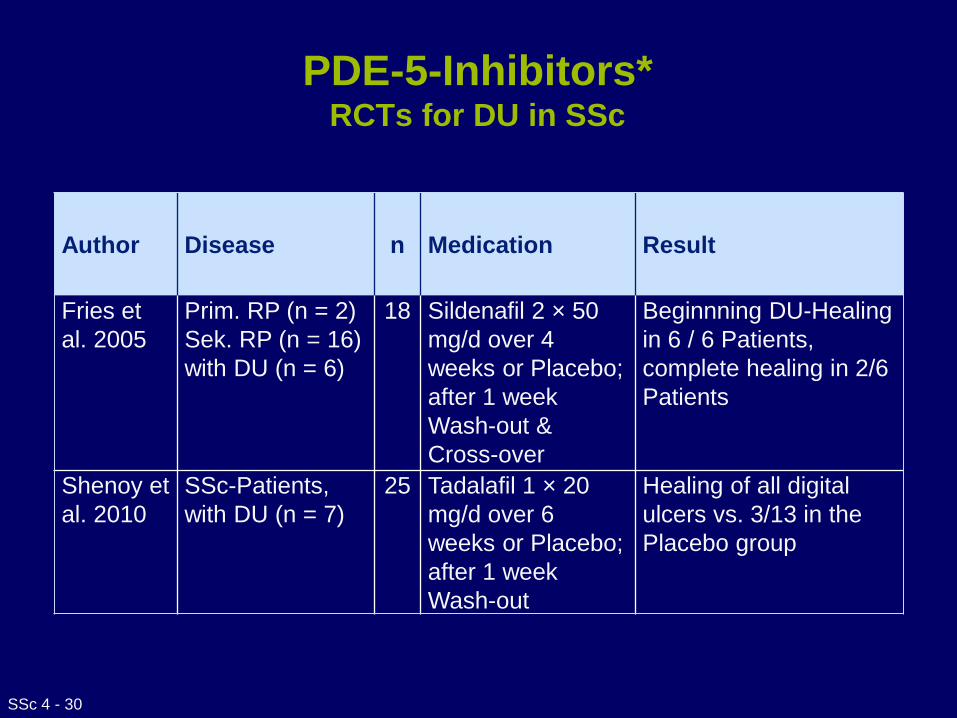
PDE-5-Inhibitors*RCTs for DU in SSc
Author Disease n Medication Result
Fries et
al. 2005
Prim. RP (n = 2)
Sek. RP (n = 16)
with DU (n = 6)
18 Sildenafil 2 × 50
mg/d over 4
weeks or Placebo;
after 1 week
Wash-out &
Cross-over
Beginnning DU-Healing
in 6 / 6 Patients,
complete healing in 2/6
Patients
Shenoy et
al. 2010
SSc-Patients,
with DU (n = 7)
25 Tadalafil 1 × 20
mg/d over 6
weeks or Placebo;
after 1 week
Wash-out
Healing of all digital
ulcers vs. 3/13 in the
Placebo group
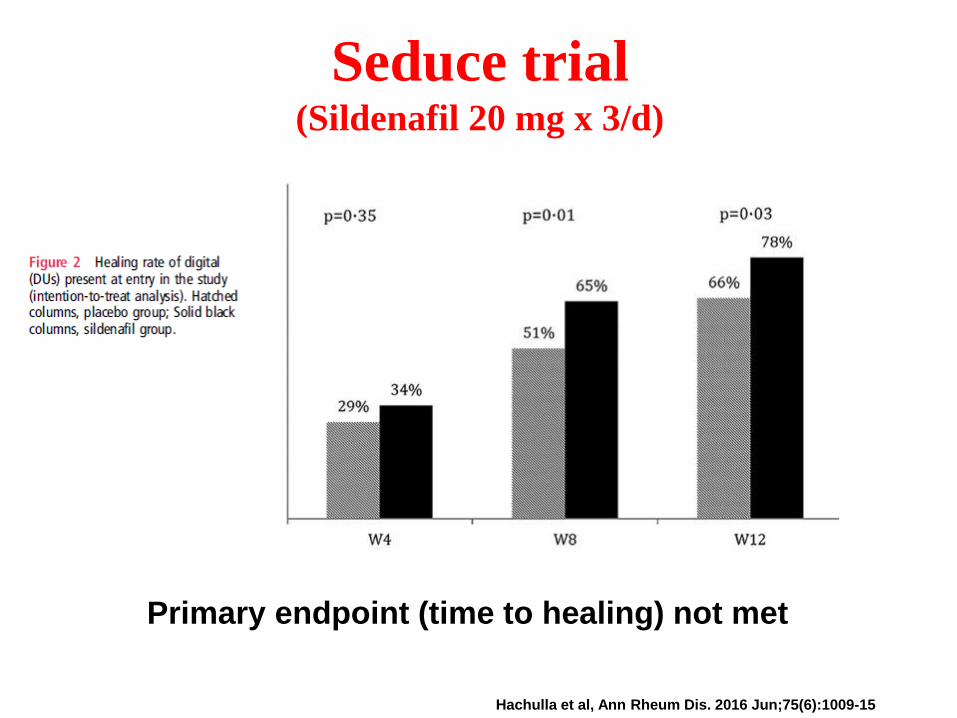
Seduce trial (Sildenafil 20 mg x 3/d)
Primary endpoint (time to healing) not met
Hachulla et al, Ann Rheum Dis. 2016 Jun;75(6):1009-15
Bosentan has confirmed efficacy in two high-quality RCTs to reduce the number of
new digital ulcers in SSc patients.
Bosentan should be considered for reduction of the number of new digital
ulcers in SSc, especially in patients with multiple digital ulcers despite use of
calcium channel blockers, PDE-5 inhibitors or iloprost therapy.
0
10
20
30
40
50
60
70
80
90
100
≥1 ≥4 ≥7 ≥10
Number of new ulcers (n)
Pati
en
ts w
ith
no
r m
ore
ulc
ers
(%
)
0
10
20
30
40
50
60
70
80
90
100
≥1 ≥4 ≥7 ≥10
Number of new ulcers (n)
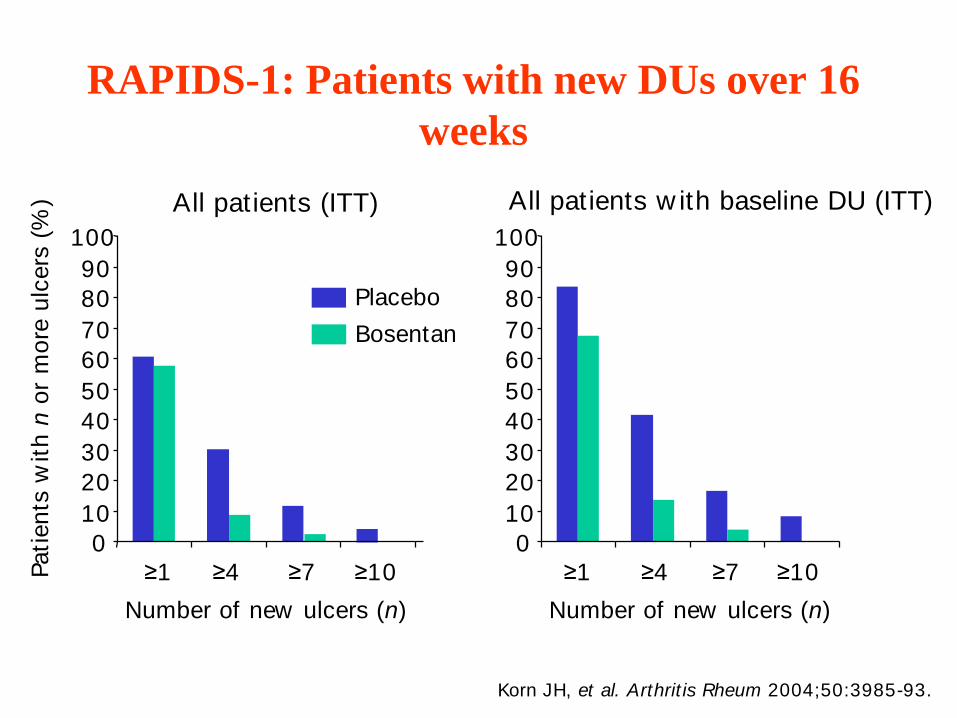
All patients (ITT) All patients w ith baseline DU (ITT)
Placebo
Bosentan
RAPIDS-1: Patients with new DUs over 16
weeks
Korn JH, et al. Arthrit is Rheum 2004;50:3985-93.
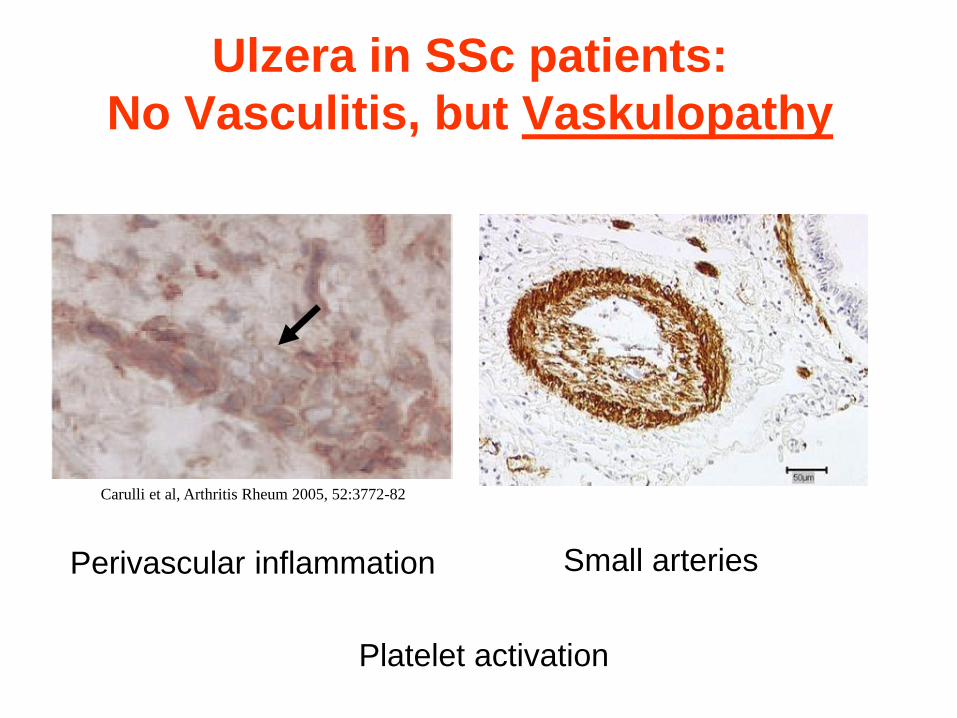
Ulzera in SSc patients:
No Vasculitis, but Vaskulopathy
Carulli et al, Arthritis Rheum 2005, 52:3772-82
Perivascular inflammation Small arteries
Platelet activation
Case – Digital ulcers
Medication:
Bosentan 250 mg/d, Sildenafil 40 mg/d, Aspirin 100mg/d, Amlodipin 20 mg/d, Nitroglycerin Crème
2%, Ilomedin every 3 months 3 days
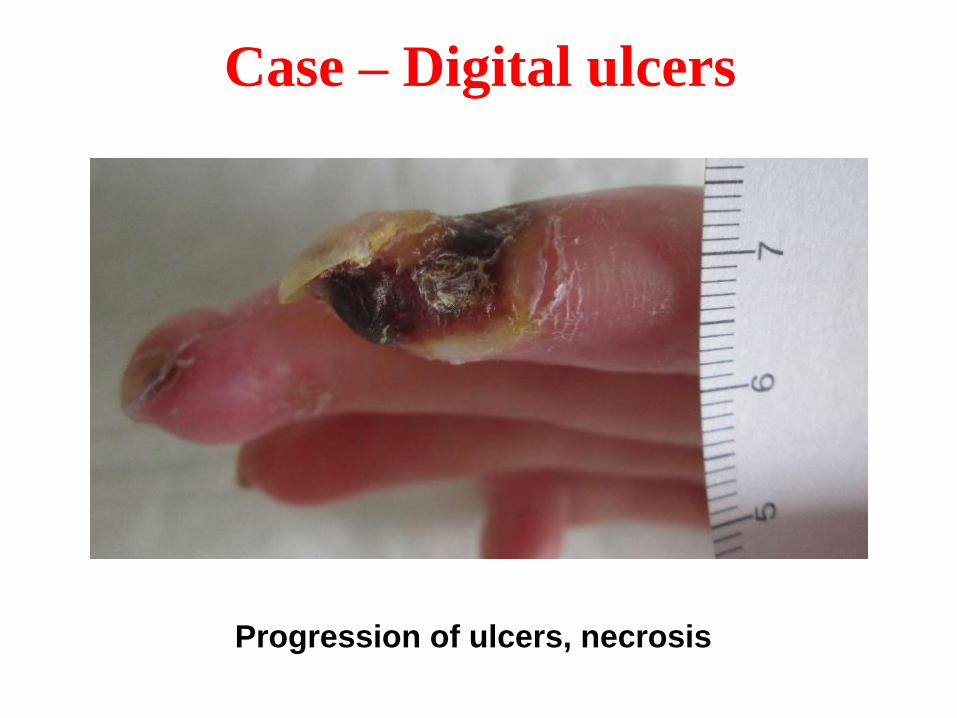
Case – Digital ulcers
Progression of ulcers, necrosis
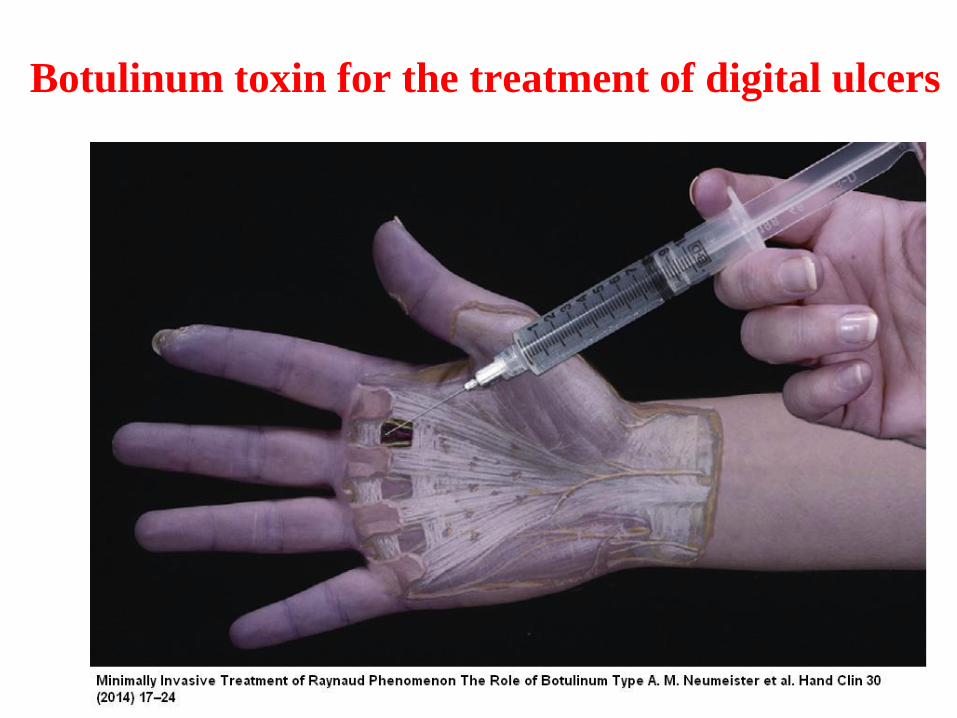
Botulinum toxin for the treatment of digital ulcers
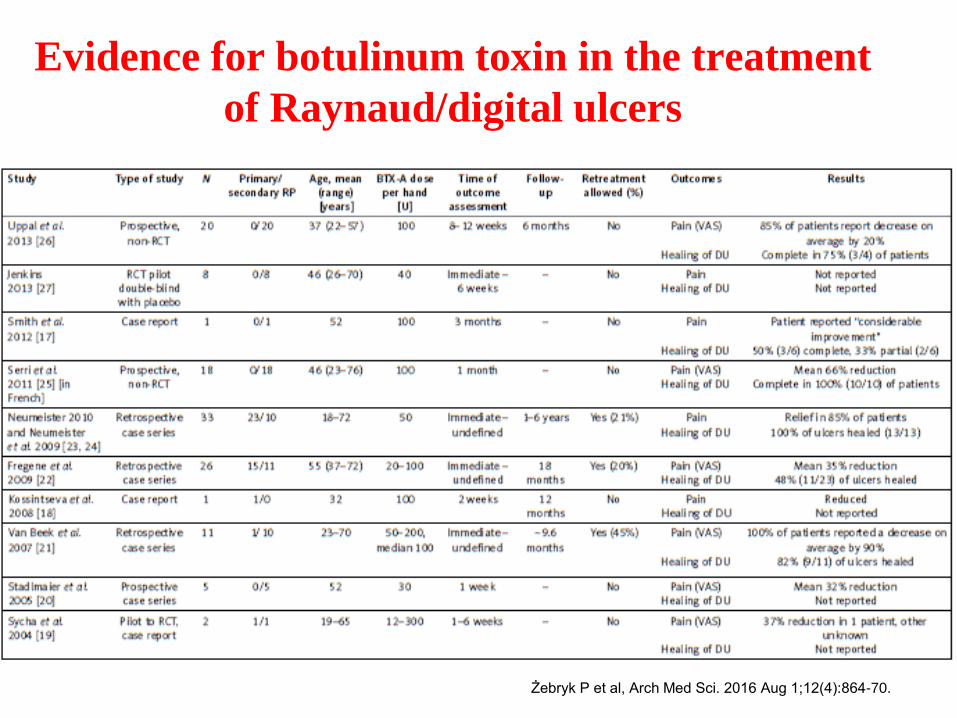
Evidence for botulinum toxin in the treatment
of Raynaud/digital ulcers
Żebryk P et al, Arch Med Sci. 2016 Aug 1;12(4):864-70.
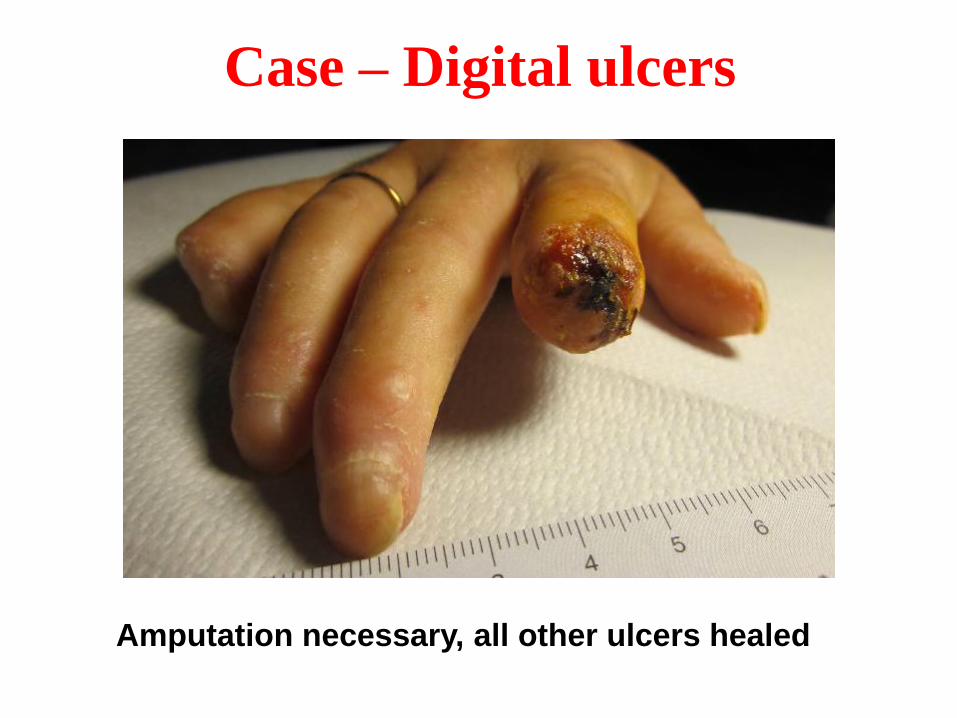
Case – Digital ulcers
Amputation necessary, all other ulcers healed
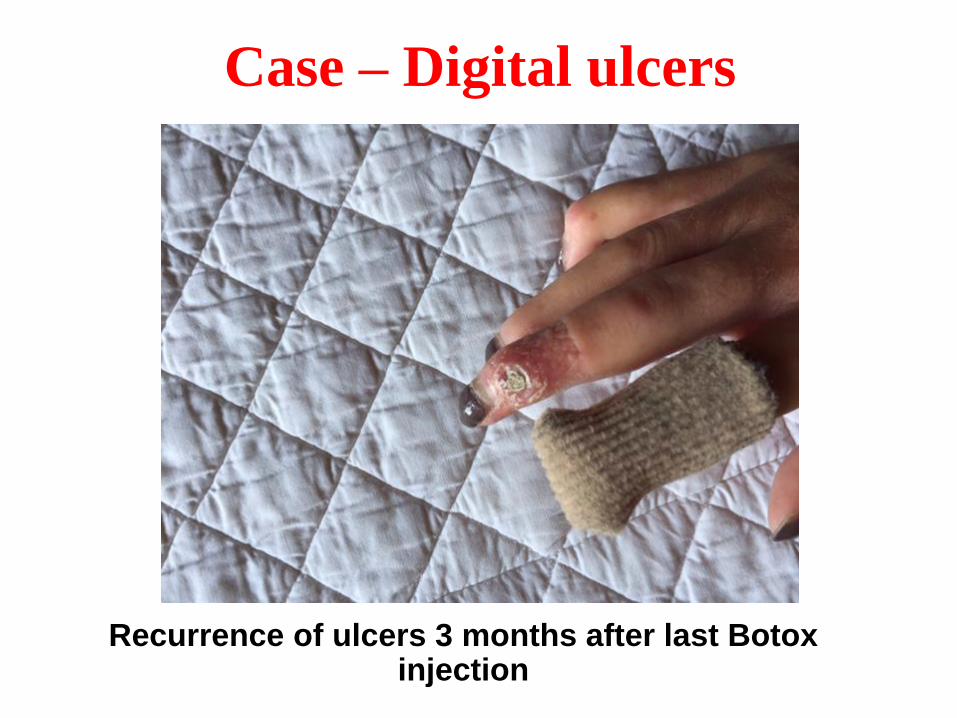
Case – Digital ulcers
Recurrence of ulcers 3 months after last Botox injection
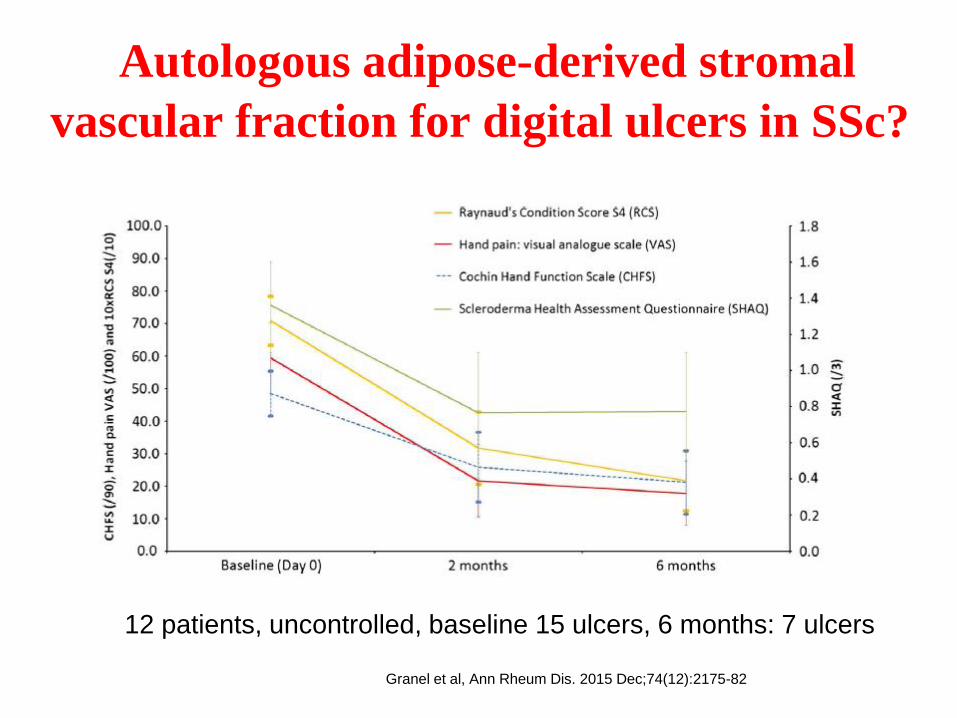
Autologous adipose-derived stromal
vascular fraction for digital ulcers in SSc?
Granel et al, Ann Rheum Dis. 2015 Dec;74(12):2175-82
12 patients, uncontrolled, baseline 15 ulcers, 6 months: 7 ulcers

26.01.2017 42|
Acknowledgments
Center of Experimental Rheumatology
Department of Rheumatology,
University Hospital Zurich
Oliver Distler
Britta Maurer
Gabriela Kania
Astrid Jüngel
Florian Renoux
Janine Schniering
Mara Stellato
Anastasiia Kozlova
Michal Rudnik
Zhongning Guo
Masaya Yokota
Li Guo
Miki Takata
Rucsandra Dobrota
Matthias Brunner
Mike Becker
Caroline Ospelt
Kerstin Klein
Mojca Frank-Bertoncelj
Michel Neidhart
Emmanuel Karouzakis
Agnieszka Pajak
Peter Künzler
Maria Comazzi
Bea Henriques
Dominic Thorley
University Hospital Zurich
University of Zurich
Department of Internal Medicine,
University of Texas Houston
Shervin Assassi
Gloria A. Salazar
Department of Pulmonology,
University Hospital Zurich
Matthias Brock
Department of Rheumatology,
Leiden University Medical Center
Fina Kurreeman
Jeska de Vries-Bouwstra
Tobias Messemaker
Division of Rheumatology&Immunology
Medical University of South Carolina
Carol Feghali-Bostwick
Department of Internal Medicine 3,
Rheumatology and Immunology,
Friedrich-Alexander University
Erlangen-Nuremberg
Jörg HW Distler





























