Embed Size (px)
Citation preview
La Morte Cardiaca Inaspettata: Si può Prevenire?
Saverio Iacopino, MD, FACC, FESC
Definizione di Morte Improvvisa
Morte naturale, preceduta da improvvisa perdita della conoscenza, che si verifica
entro 1 ora dall’inizio dei sintomi, in soggetti con o senza cardiopatia nota preesistente, ma
in cui l’epoca e la modalità di morte sono inattese
Task-force on SD of ESC. Eur Heart J 2001; 22: 1374-1450
FILIPPIDE muore improvvisamente subito dopo aver annunciato agli Ateniesi la vittoria di MARATONA...
“ … nel corpo umano non si può fermare volontariamente, se non il polmone. Vedi il core fa da sé il suo ofizio, e così lo stomaco e l’altre intestine a quello congiunte…”
“…del core; questo si move da sé e non si ferma se non eternamente”
Leonardo da Vinci
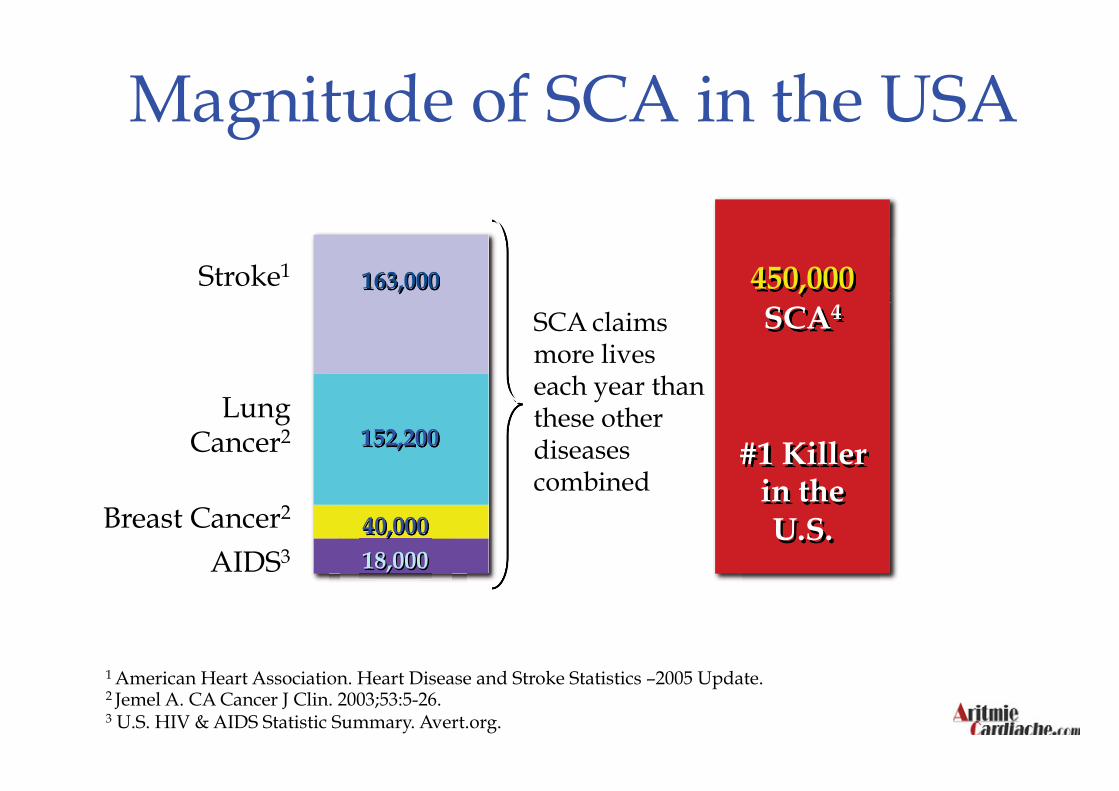
Magnitude of SCA in the USA
AIDS3
Breast Cancer2
Lung Cancer2
Stroke1
SCA4 SCA claims more lives each year than these other diseases combined
450,000 163,000
152,200
40,000
18,000
#1 Killer in the U.S.
1 American Heart Association. Heart Disease and Stroke Statistics –2005 Update. 2 Jemel A. CA Cancer J Clin. 2003;53:5-26. 3 U.S. HIV & AIDS Statistic Summary. Avert.org.

~450,000 per year
1,200 per day 50 every hour; 1 every 80 seconds
Although SCA is the first presentation of cardiac disease in 20-25% of patients, most cases occur in patients with clinically recognized heart disease
1 Zheng Z. Circulation. 2001;104::2158-2163. 2 Myerburg RJ, Heart Disease, A textbook of Cardiovascular Medicine. 6th ed. 2001. W.B. Saunders, Co.
Magnitude of SCA in the USA
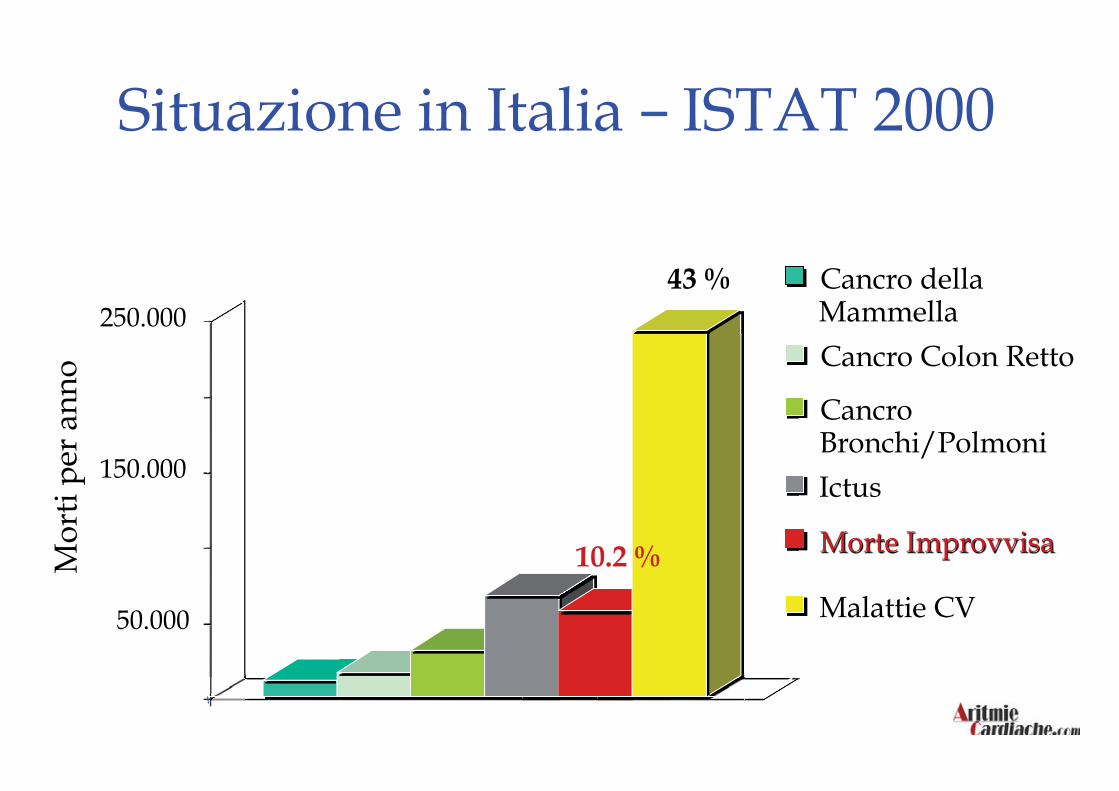
Situazione in Italia – ISTAT 2000 M
orti
per
anno
50.000
150.000
250.000 Cancro della MammellaCancro Colon Retto Cancro Bronchi/Polmoni Ictus Morte Improvvisa
Malattie CV
43 %
10.2 %
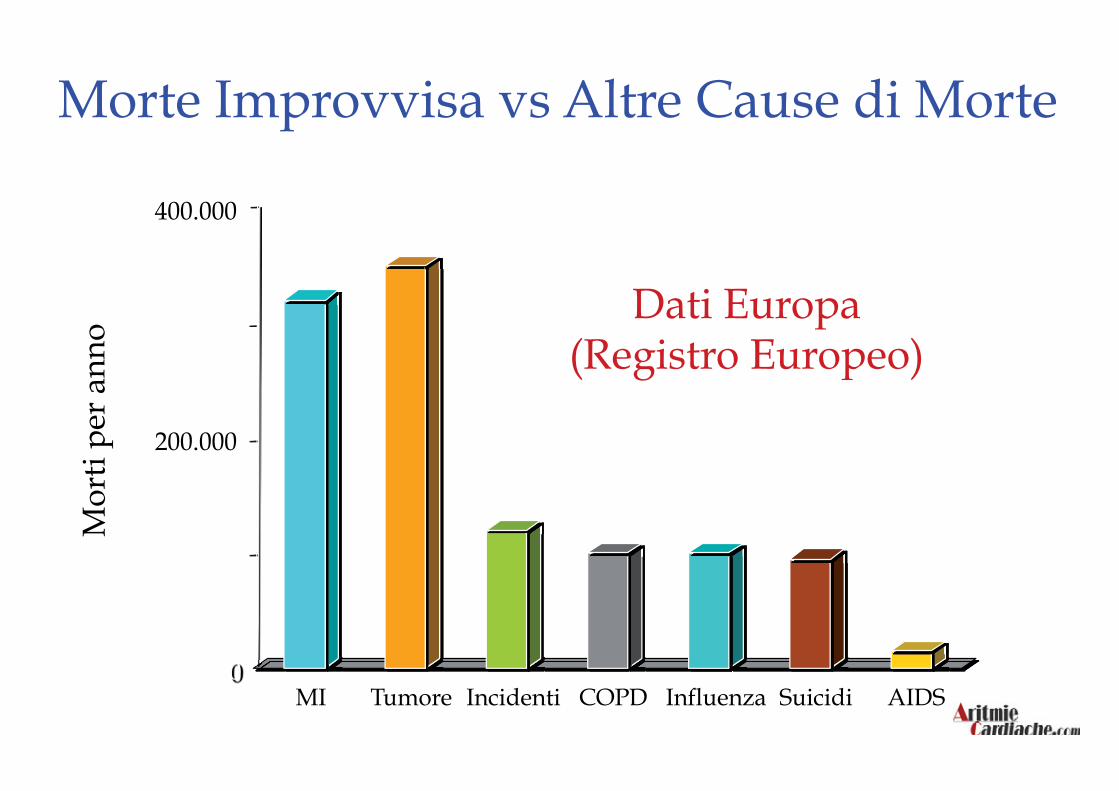
Mor
ti pe
r an
no Dati Europa
(Registro Europeo)
0
200.000
400.000
MI Tumore Incidenti COPD Influenza Suicidi AIDS
Morte Improvvisa vs Altre Cause di Morte
Epidemiologia - Italia Incidenza → 1 x 1000 Abitanti
Numero casi x anno → 57.000
Numero casi x giorno → 156
1 caso ogni 9 minuti
10 % di tutte le cause di morte
40 % di tutti i decessi x causa cardiaca
Trentino →→ 1 caso ogni 9 ore
Lombardia → 1 caso ogni 57 minuti
Friuli → 1 caso ogni 7 ore
Veneto → 1 caso ogni 2 ore
Piemonte → 1 caso ogni 2 ore
Liguria → 1 caso ogni 5 ore
EmiliaRomagna → 1 caso ogni 2 ore e 20
Marche → 1 caso ogni 6 ore
Toscana → 1 caso ogni 2 ore
Epidemiologia - Italia

Umbria →→ 1 caso ogni 10 ore
Lazio → 1 caso ogni ora e 1/2
Abruzzo → 1 caso ogni 9 ore
Campania → 1 caso ogni ora e 20
Puglia → 1 caso ogni 2 ore
Molise → 1 caso ogni 26 ore
Basilicata → 1 caso ogni 14 ore
Calabria → 1 caso ogni 4 ore
Sicilia → 1 caso ogni ora e 1/2
Sardegna → 1 caso ogni 5 ore
Incidenza per Regione
Mortalità intraospedaliera
Anni ‘60 > 30%
Anni ’70-’85 12-13%
Dall’ 85 in poi 7-8%
Mortalità preospedaliera
Da sempre 35 – 50%
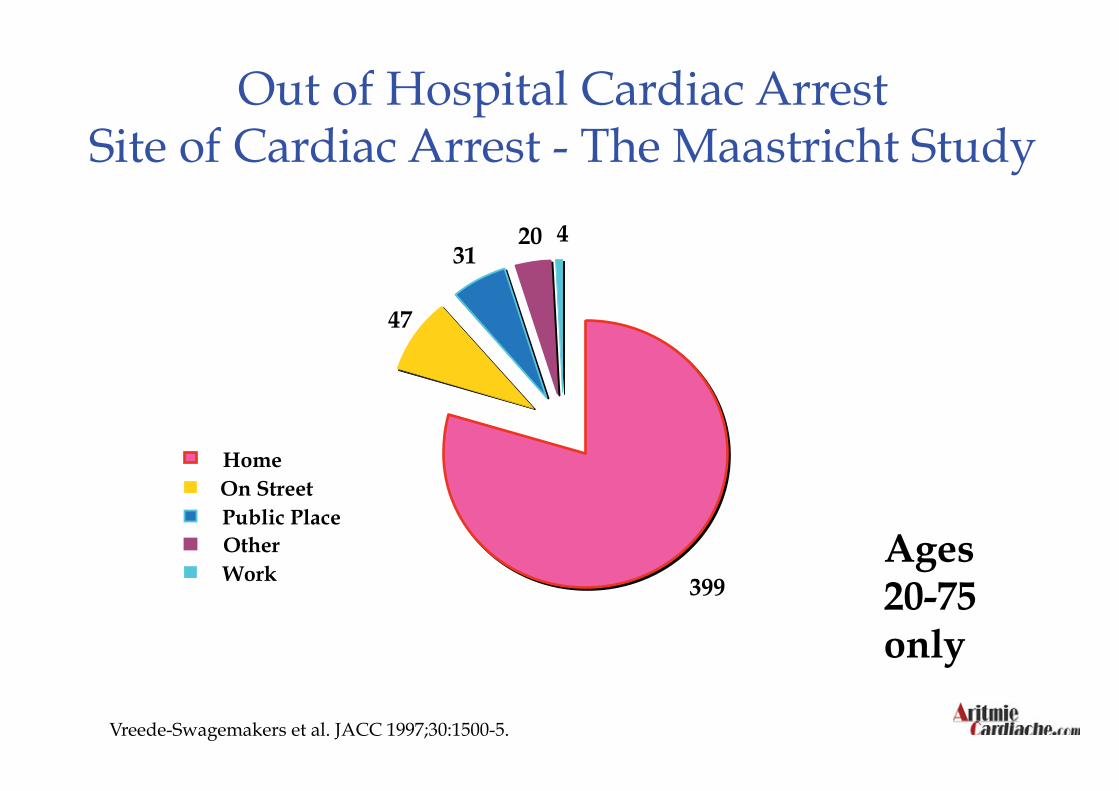
Vreede-Swagemakers et al. JACC 1997;30:1500-5.
Ages 20-75 only
Out of Hospital Cardiac Arrest Site of Cardiac Arrest - The Maastricht Study
399
47
31 20 4
Home On Street Public Place Other Work
A combination of these risk factors further increases the risk of SCA
Risk Factors for SCA
Previous Myocardial Infarction (MI)
Heart Failure and/or decreased LVEF
Previous Sudden Cardiac Arrest Event
Prior Episode of Ventricular Tachyarrhythmia (VT)
Coronary Artery Disease (CAD)
Hypertrophic Cardiomyopathy (HCM)
Long QT Syndrome
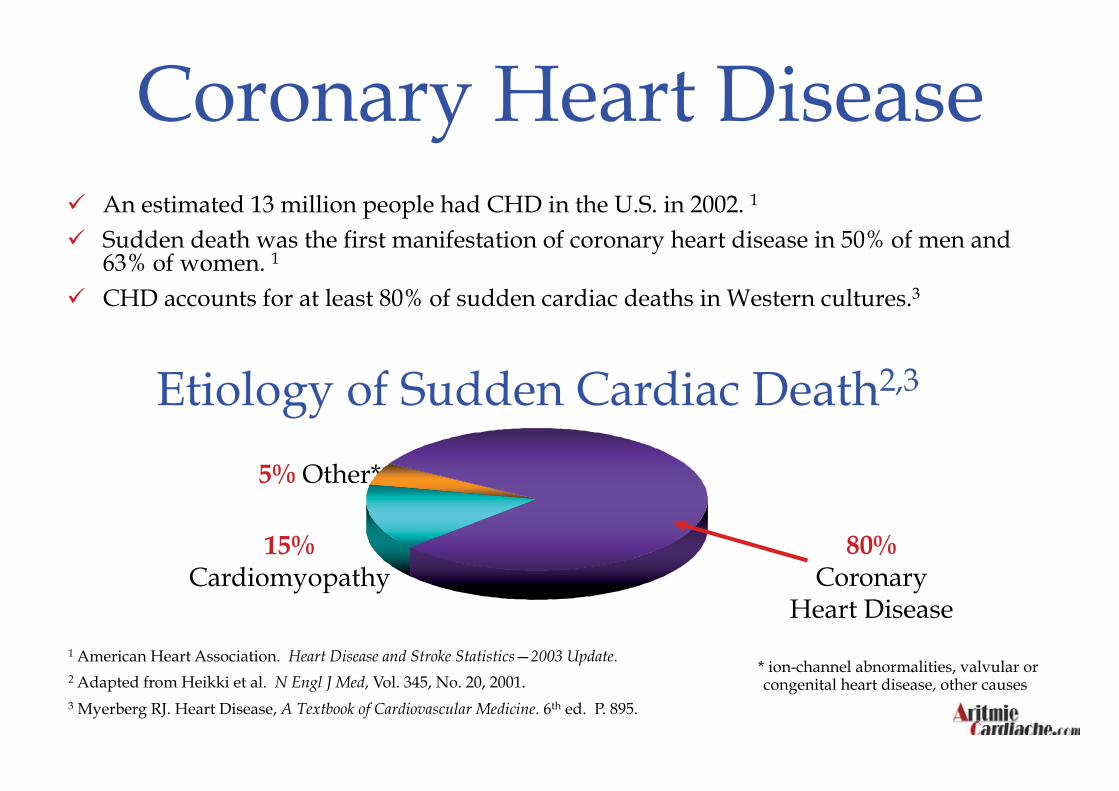
Coronary Heart Disease An estimated 13 million people had CHD in the U.S. in 2002. 1
Sudden death was the first manifestation of coronary heart disease in 50% of men and 63% of women. 1
CHD accounts for at least 80% of sudden cardiac deaths in Western cultures.3
1 American Heart Association. Heart Disease and Stroke Statistics—2003 Update. 2 Adapted from Heikki et al. N Engl J Med, Vol. 345, No. 20, 2001. 3 Myerberg RJ. Heart Disease, A Textbook of Cardiovascular Medicine. 6th ed. P. 895.
Etiology of Sudden Cardiac Death2,3
* ion-channel abnormalities, valvular or congenital heart disease, other causes
80% Coronary
Heart Disease
15% Cardiomyopathy
5% Other*
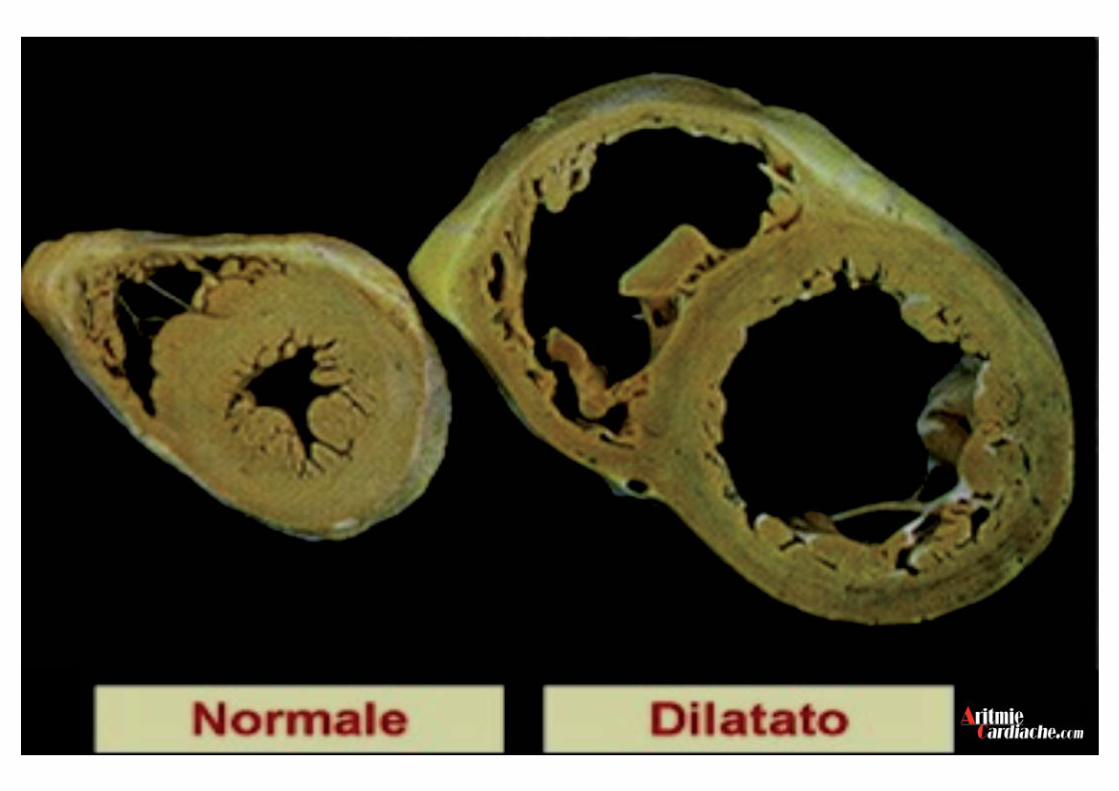
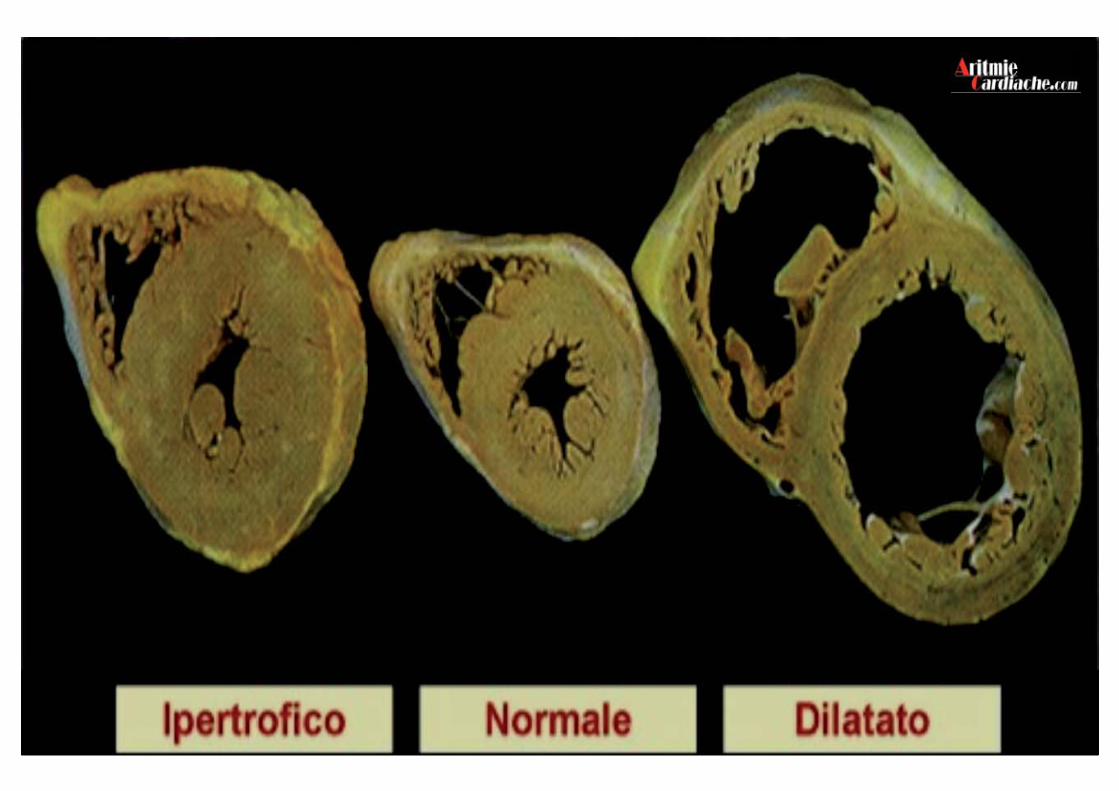
Cardiomiopatia Dilatativa
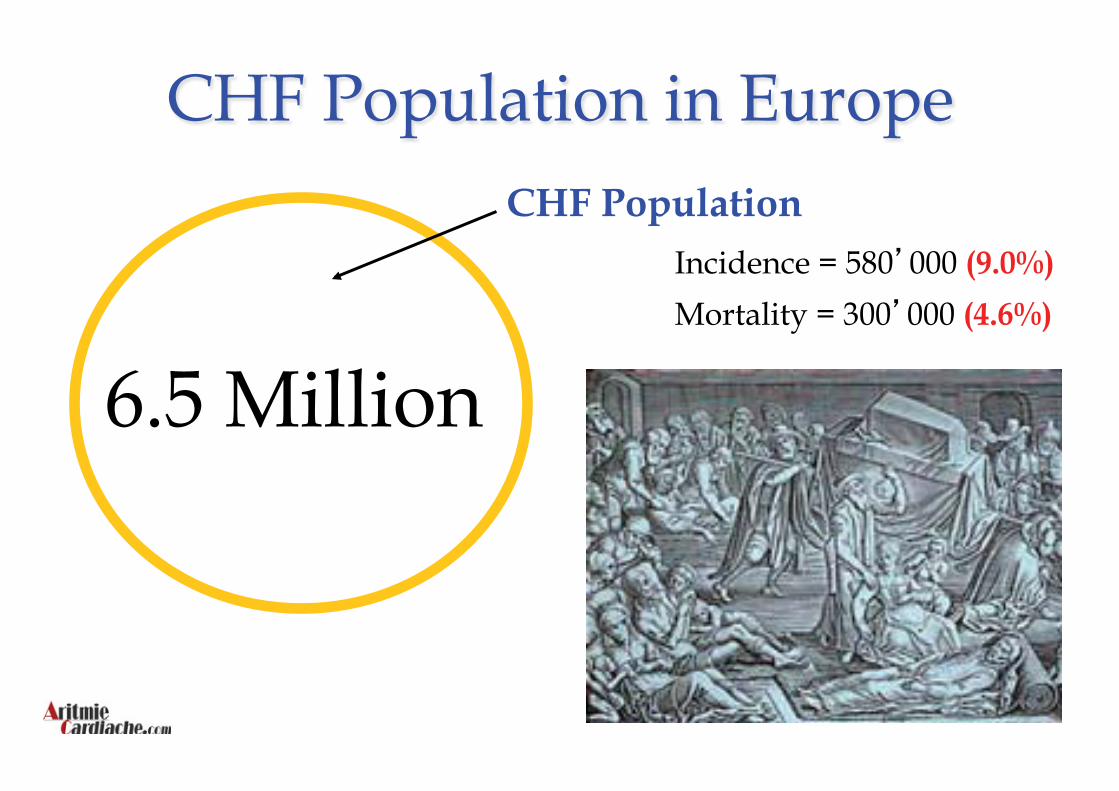
CHF Population
6.5 Million
Incidence = 580 000 (9.0%)
Mortality = 300 000 (4.6%)
CHF Population in Europe
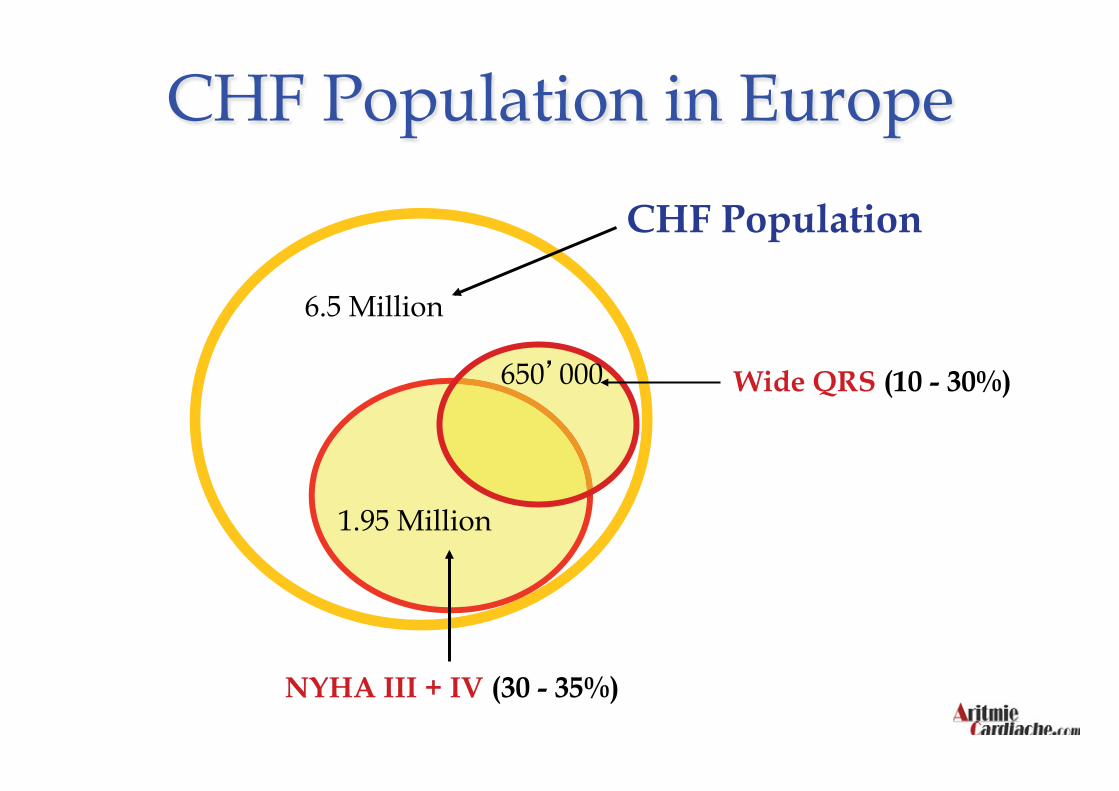
CHF Population
6.5 Million
NYHA III + IV (30 - 35%)
1.95 Million
Wide QRS (10 - 30%) 650 000
CHF Population in Europe
Left Ventricular Dysfunction in Patients With Dilated Cardiomyopathy
Am J Cardiol 1992; 69: 1570-73
Fluid Accumulation Is a common complication of HF Can be chronic or have sudden onset Potentially life-threatening during sudden onset
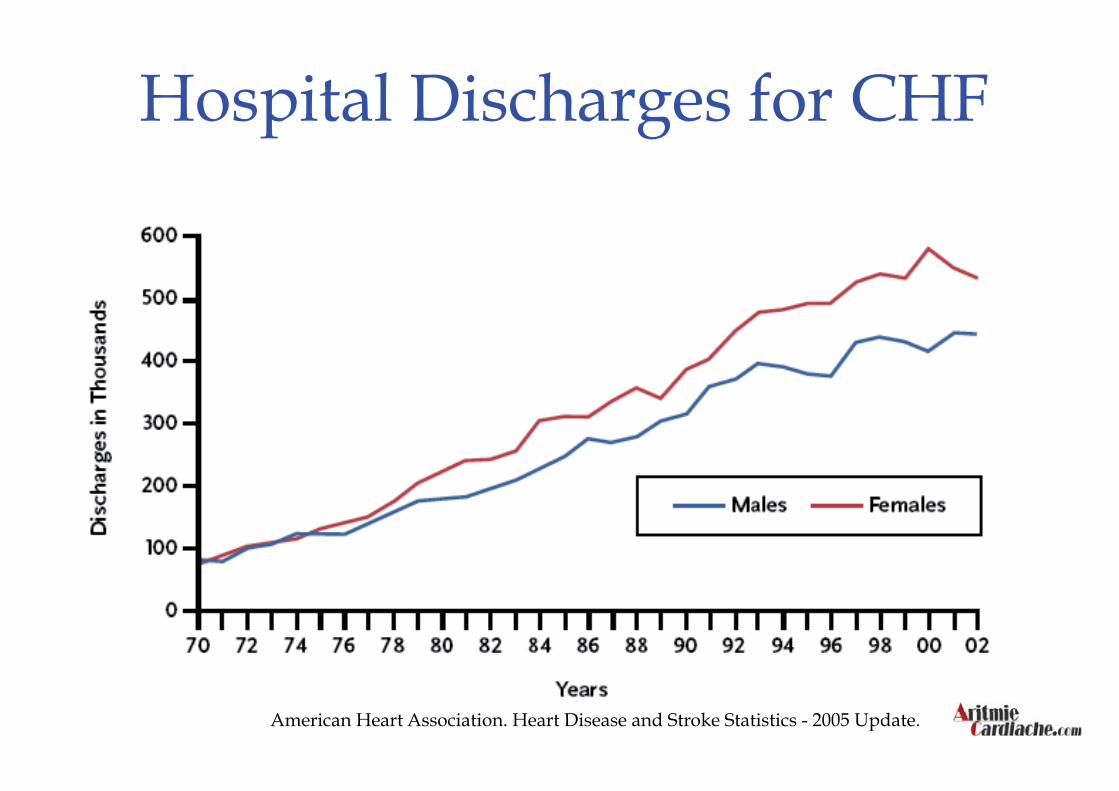
American Heart Association. Heart Disease and Stroke Statistics - 2005 Update.
Hospital Discharges for CHF
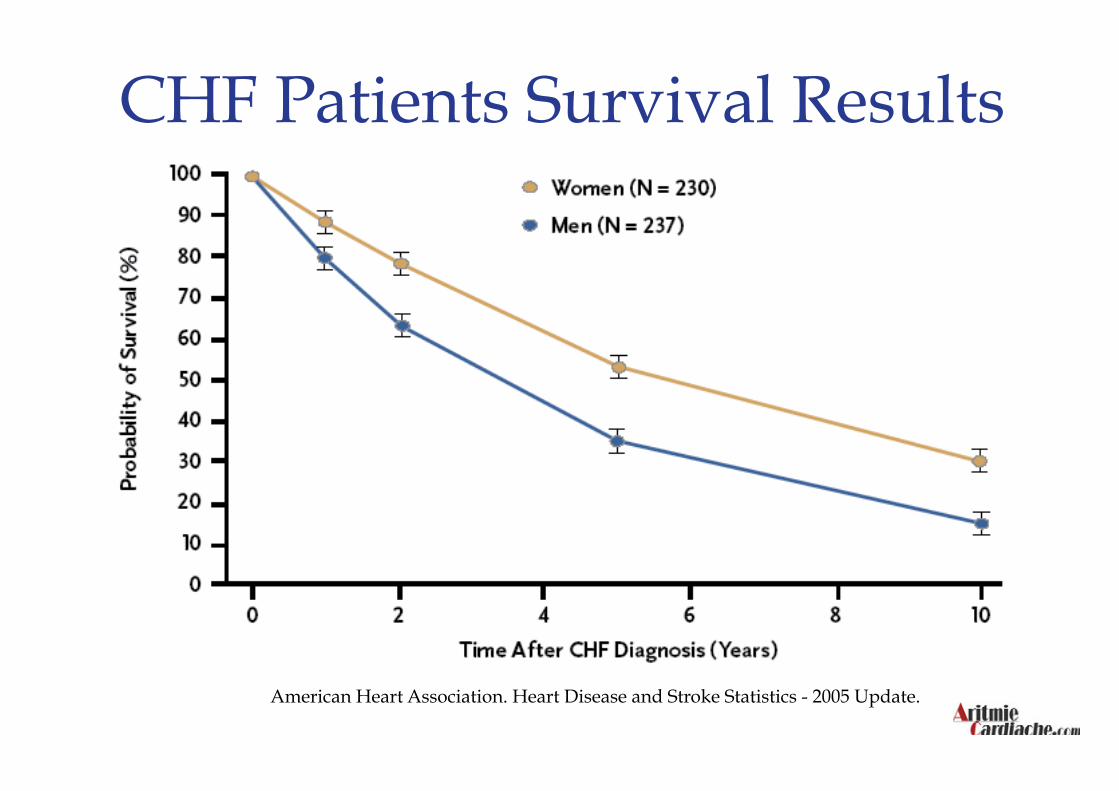
CHF Patients Survival Results
American Heart Association. Heart Disease and Stroke Statistics - 2005 Update.
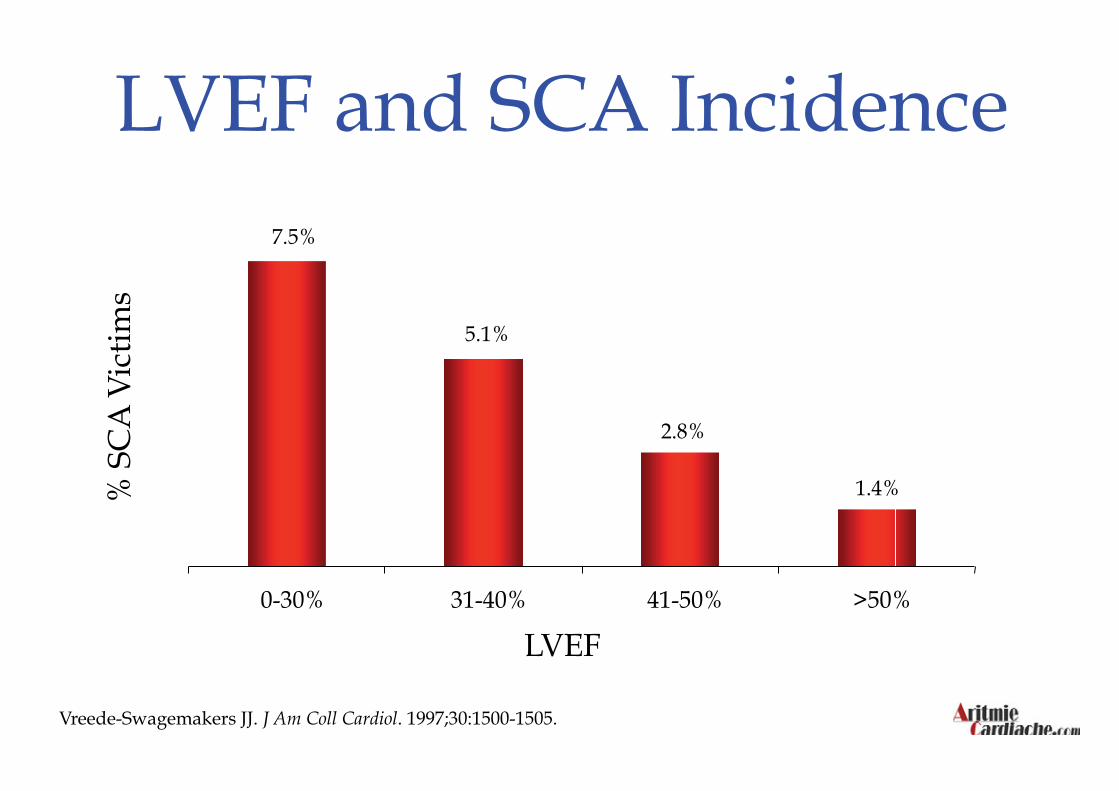
LVEF and SCA Incidence
Vreede-Swagemakers JJ. J Am Coll Cardiol. 1997;30:1500-1505.
LVEF
% S
CA
Vic
tims
7.5%
5.1%
2.8%
1.4%
0 1 2 3 4 5 6 7 8
0-30% 31-40% 41-50% >50%
Severity of Heart Failure
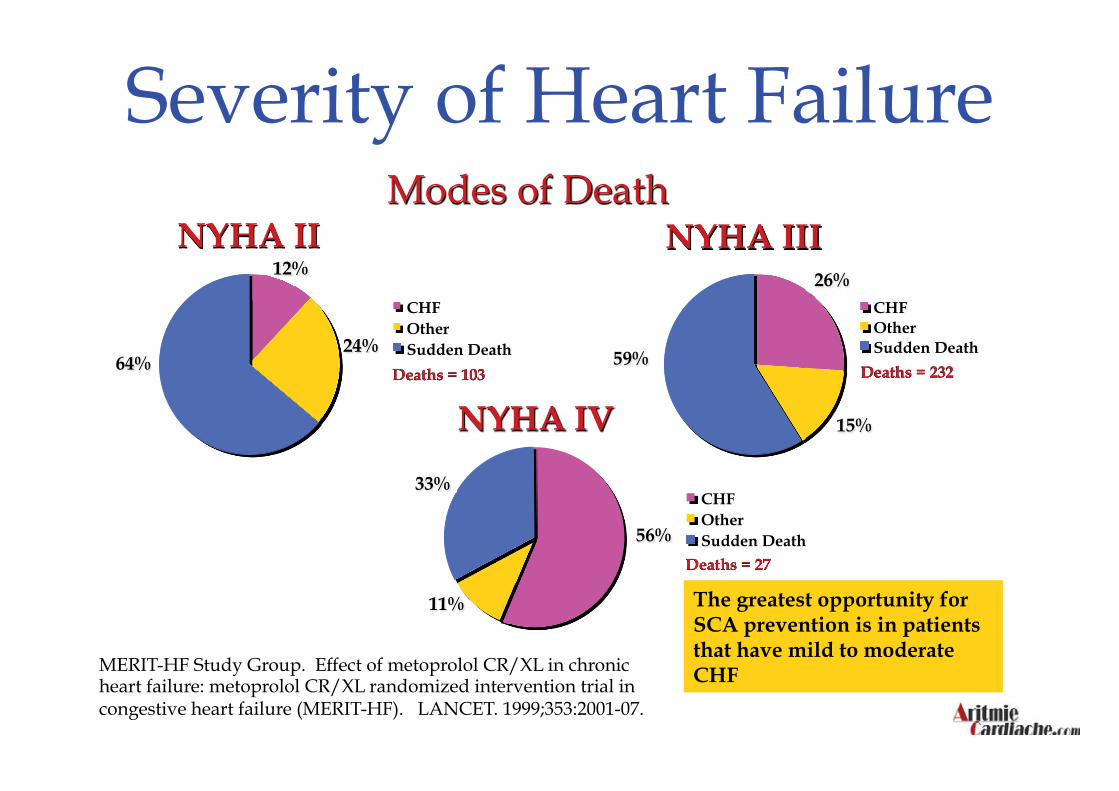
MERIT-HF Study Group. Effect of metoprolol CR/XL in chronic heart failure: metoprolol CR/XL randomized intervention trial in congestive heart failure (MERIT-HF). LANCET. 1999;353:2001-07.
Modes of Death NYHA II
12%
64% 24%
CHF Other Sudden Death
Deaths = 103
NYHA IV
56%
11%
33% CHF Other Sudden Death
Deaths = 27
NYHA III 26%
15%
59%
CHF Other Sudden Death
Deaths = 232
The greatest opportunity for SCA prevention is in patients that have mild to moderate CHF
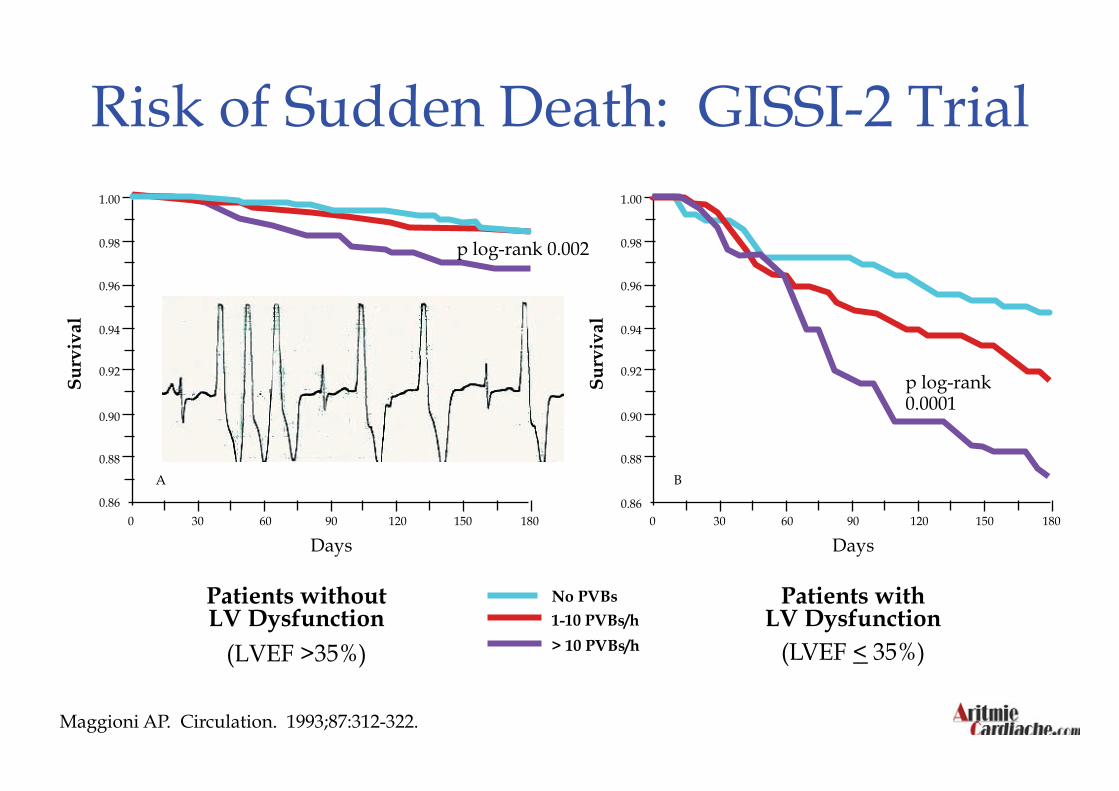
Risk of Sudden Death: GISSI-2 Trial
Patients without LV Dysfunction
(LVEF >35%)
Maggioni AP. Circulation. 1993;87:312-322.
Patients with LV Dysfunction
(LVEF < 35%)
No PVBs
1-10 PVBs/h
> 10 PVBs/h
0.86
A
0.88
0.90
0.92
0.94
0.96
0.98
1.00
0 30 60 90 120 150 180
Days
Su
rviv
al
p log-rank 0.002
0.88
0.90
0.92
0.94
0.96
0.98
1.00
0 30 60 90 120 150 180
Days
Su
rviv
al
B
p log-rank 0.0001
0.86
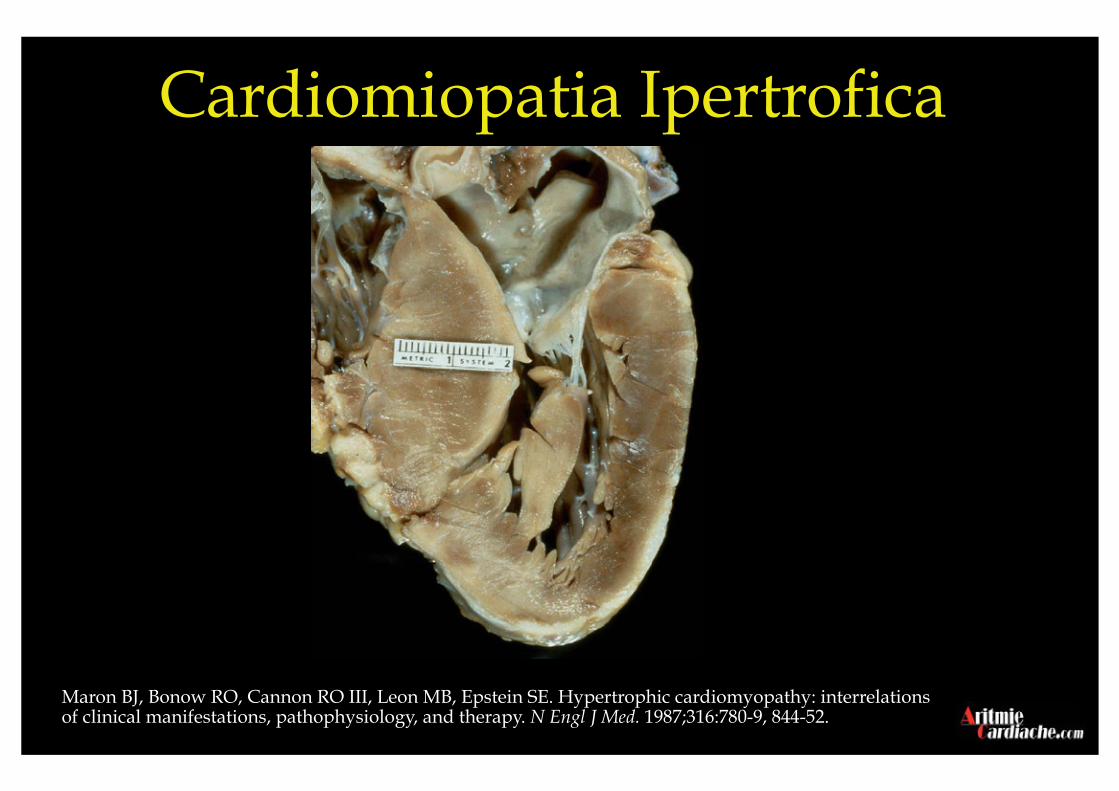
Maron BJ, Bonow RO, Cannon RO III, Leon MB, Epstein SE. Hypertrophic cardiomyopathy: interrelations of clinical manifestations, pathophysiology, and therapy. N Engl J Med. 1987;316:780-9, 844-52.
Cardiomiopatia Ipertrofica

Maron BJ et al. Circulation. 1996;94:850-56.
HCM (36%)
Congenital coronary anomalies
(19%)
Mildly increased cardiac mass (10%)
Ruptured aorta 5%
Tunnelled LAD 5%
Aortic stenosis 4%
Myocarditis 3%
Dilated cardiomyopathy 3%
ARVC 3%
MVP 2%
CAD 2%
Other 6%
Causes of SCA in Young People
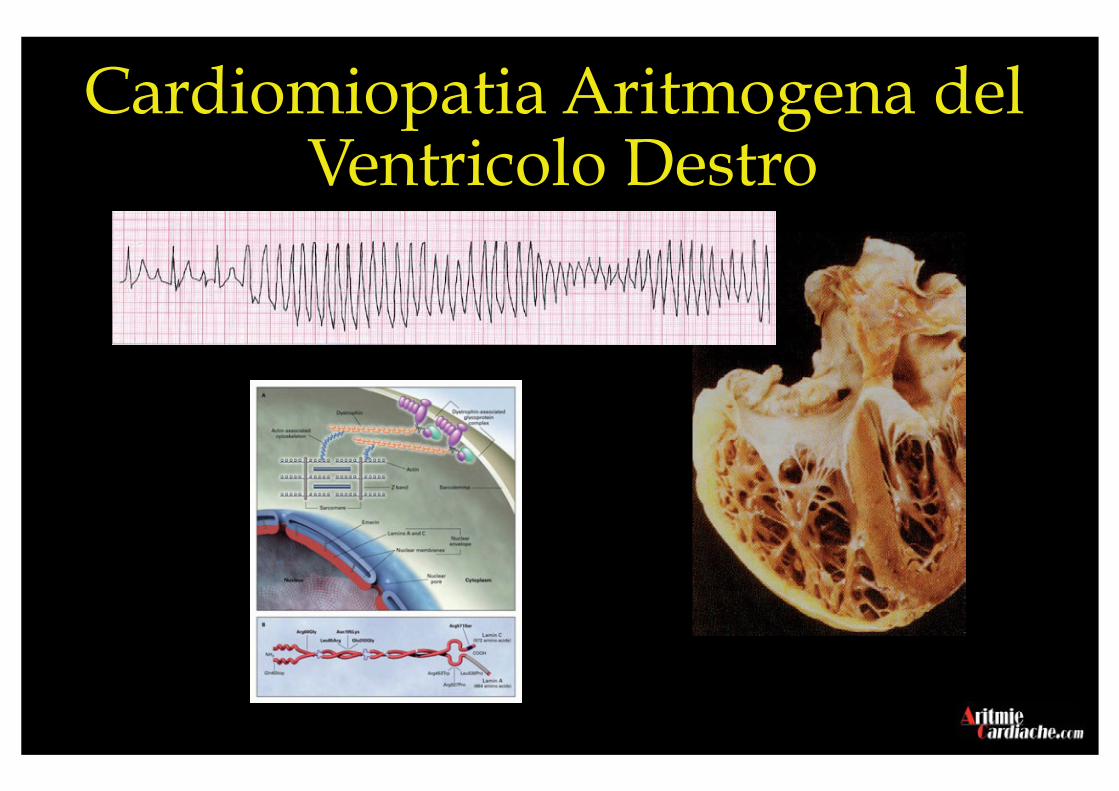
Cardiomiopatia Aritmogena del Ventricolo Destro
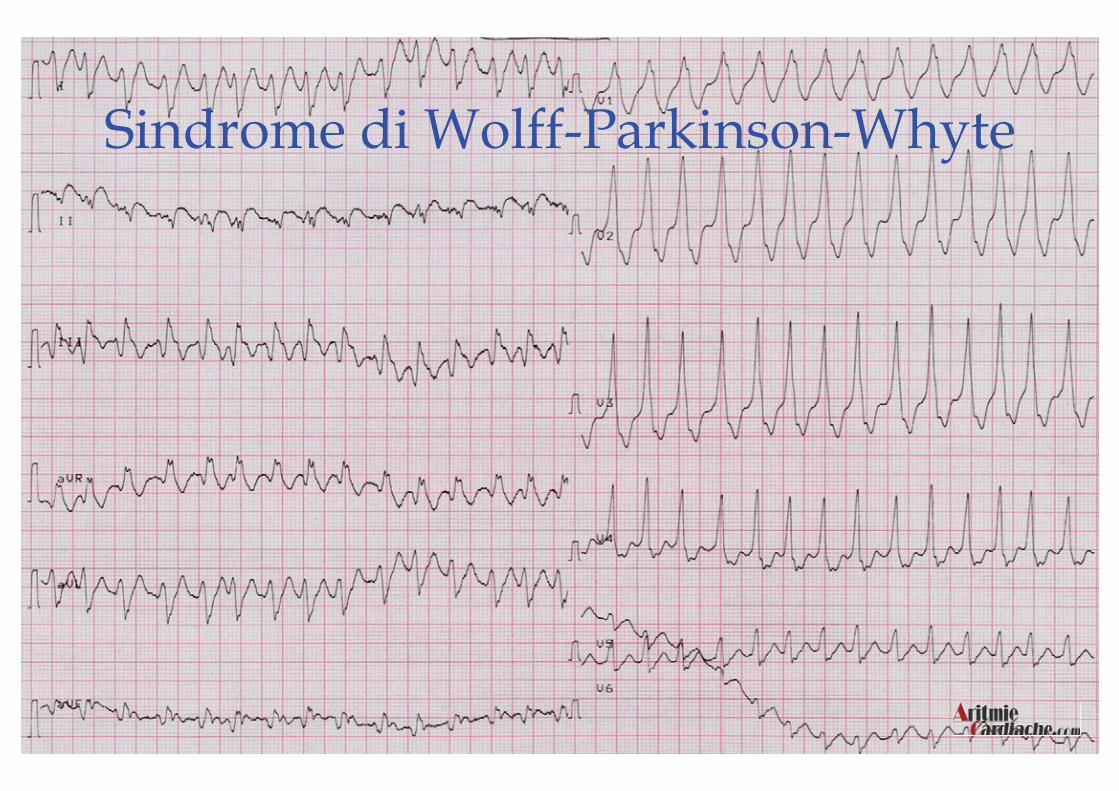
Sindrome di Wolff-Parkinson-Whyte
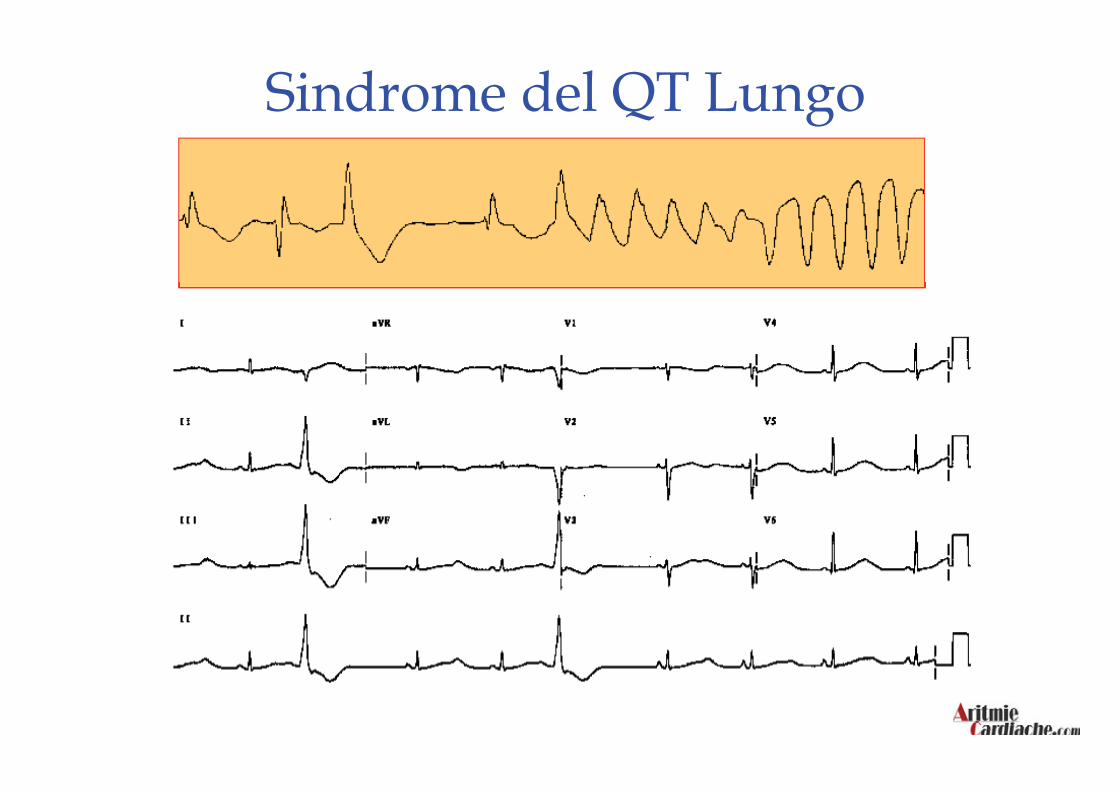
Sindrome del QT Lungo

Sindrome di Brugada

QTc 280 QTc 220 QTc 260 Sindrome del QT Corto
Sudden Infant Death Syndrome
SINDROME DELL IMPROVVISA MORTE NEONATALE INCIDENZA (0,5 per 1000 nati vivi - 3,5 per mille) In Italia nascono ogni anno 500.000 bambini (250 a 3500 morti dovute a SIDS)
FATTORI DI RISCHIO mettere il bambino a dormire a pancia in giù caldo eccessivo fumo della madre in gravidanza fumo passivo infezioni delle vie respiratorie prematurità familiarità
L ALLATTAMENTO AL SENO È UN FATTORE PROTETTIVO
DORMIRE A PANCIA IN SU DETERMINA UNA RIDUZIONE DELLA MORTALITÀ DEL 50%
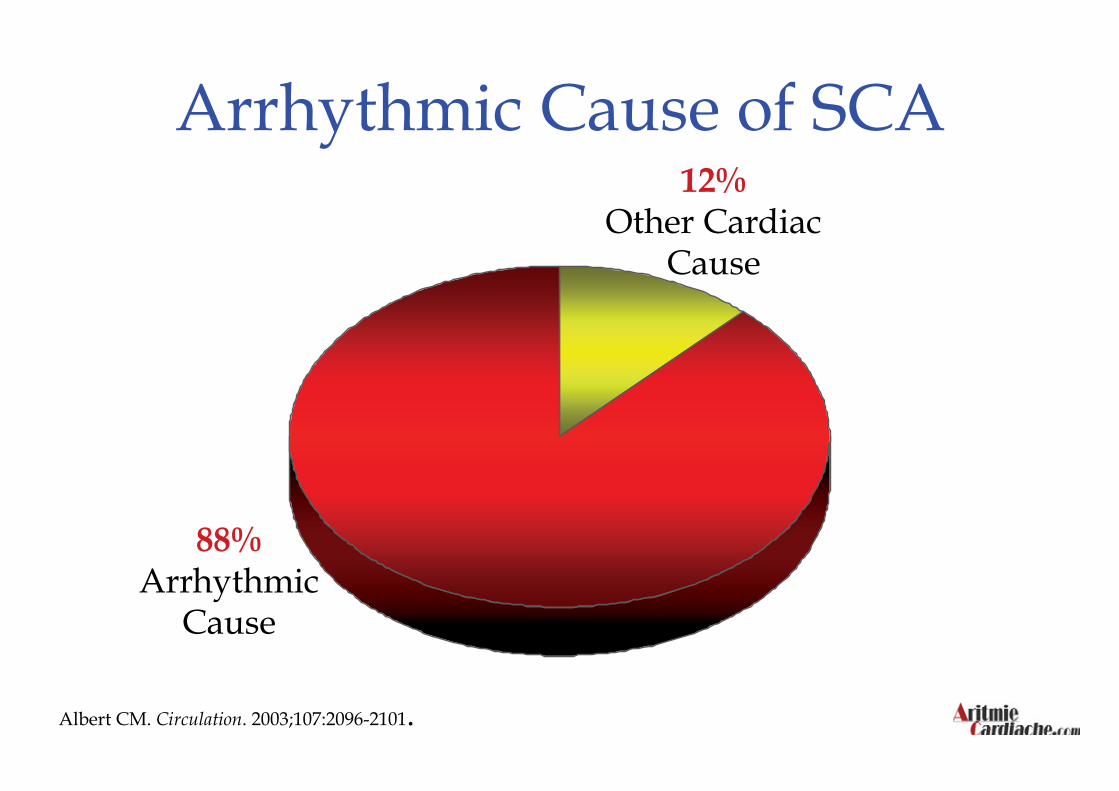
Arrhythmic Cause of SCA
Albert CM. Circulation. 2003;107:2096-2101.
12% Other Cardiac
Cause
88% Arrhythmic
Cause
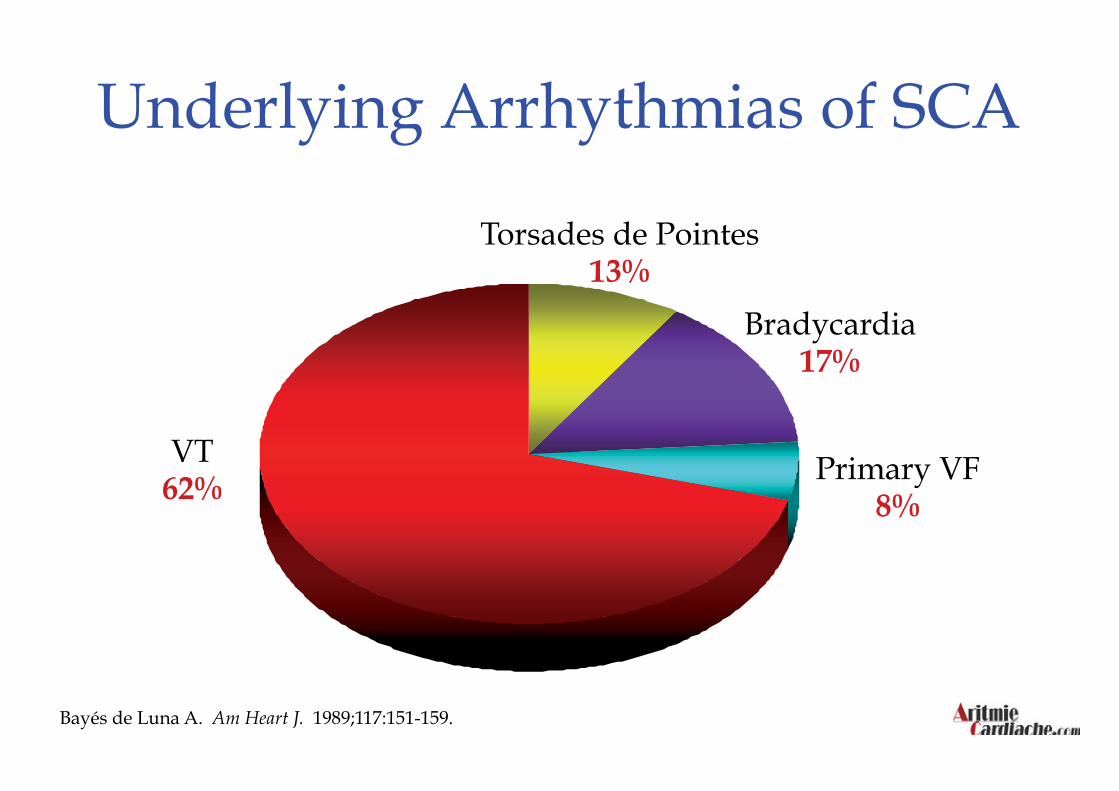
Bayés de Luna A. Am Heart J. 1989;117:151-159.
Underlying Arrhythmias of SCA
Bradycardia 17%
VT 62%
Primary VF 8%
Torsades de Pointes 13%

6:02 AM
6:05 AM
6:07 AM
6:11 AM
Successione di Eventi
Prevenzione della Morte Improvvisa
L’azione sui fattori di rischio (prevenzione primaria)
L’identificazione dei soggetti a rischio (prevenzione secondaria)
La realizzazione di sistemi efficaci di rapido intervento
(defibrillazione precoce)

Prevenzione della Morte Improvvisa L’azione sui fattori di rischio (prevenzione primaria)

La Catena della Prevenzione
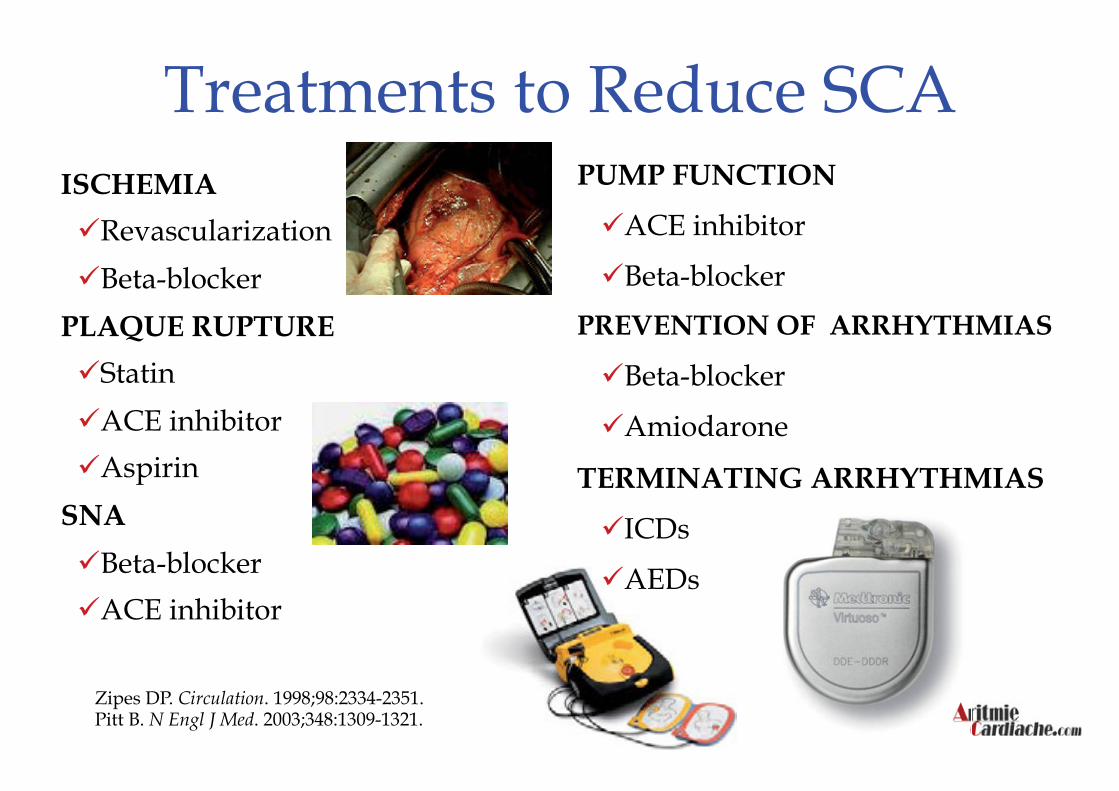
Treatments to Reduce SCA ISCHEMIA
Revascularization
Beta-blocker
PLAQUE RUPTURE
Statin
ACE inhibitor
Aspirin
SNA
Beta-blocker
ACE inhibitor
PUMP FUNCTION
ACE inhibitor
Beta-blocker
PREVENTION OF ARRHYTHMIAS
Beta-blocker
Amiodarone
TERMINATING ARRHYTHMIAS
ICDs
AEDs
Zipes DP. Circulation. 1998;98:2334-2351. Pitt B. N Engl J Med. 2003;348:1309-1321.

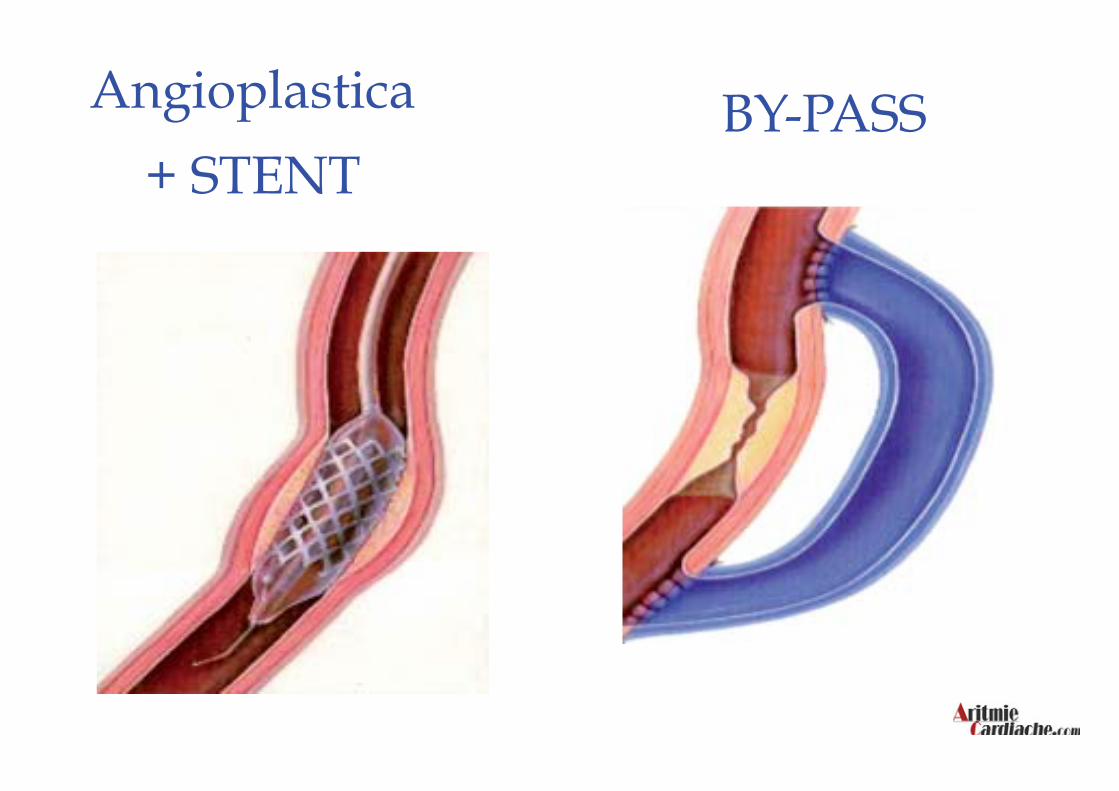
Angioplastica
+ STENT BY-PASS
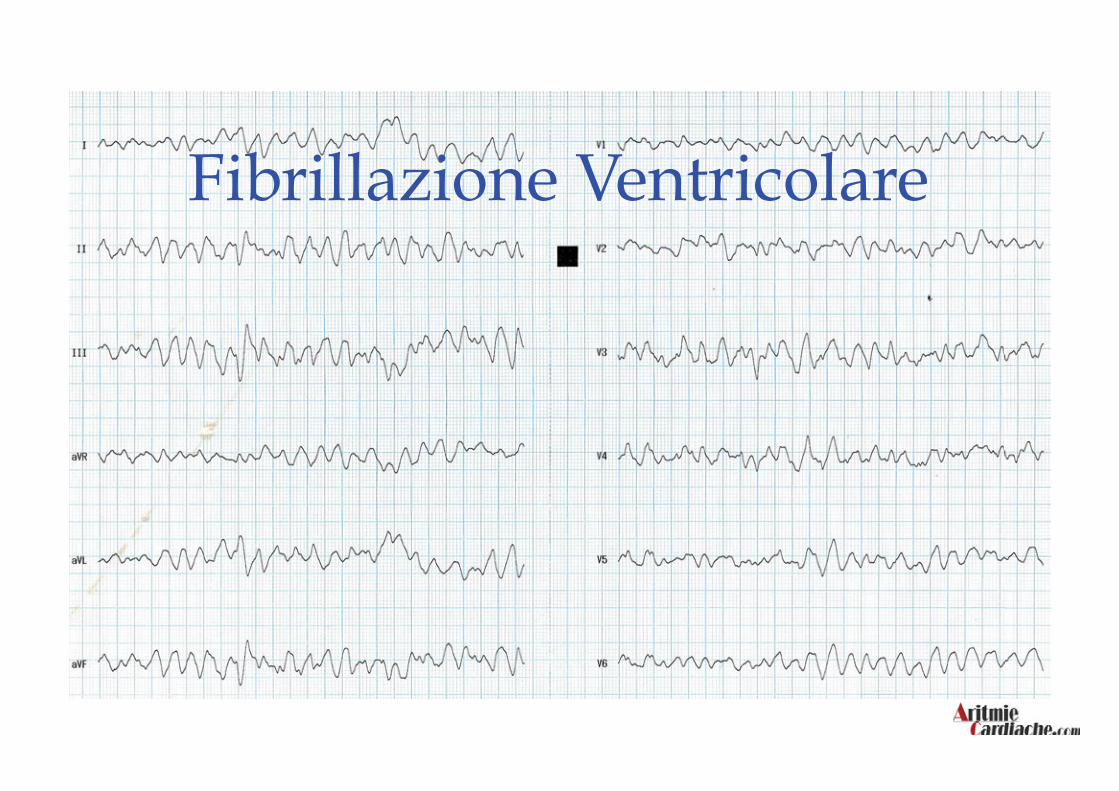
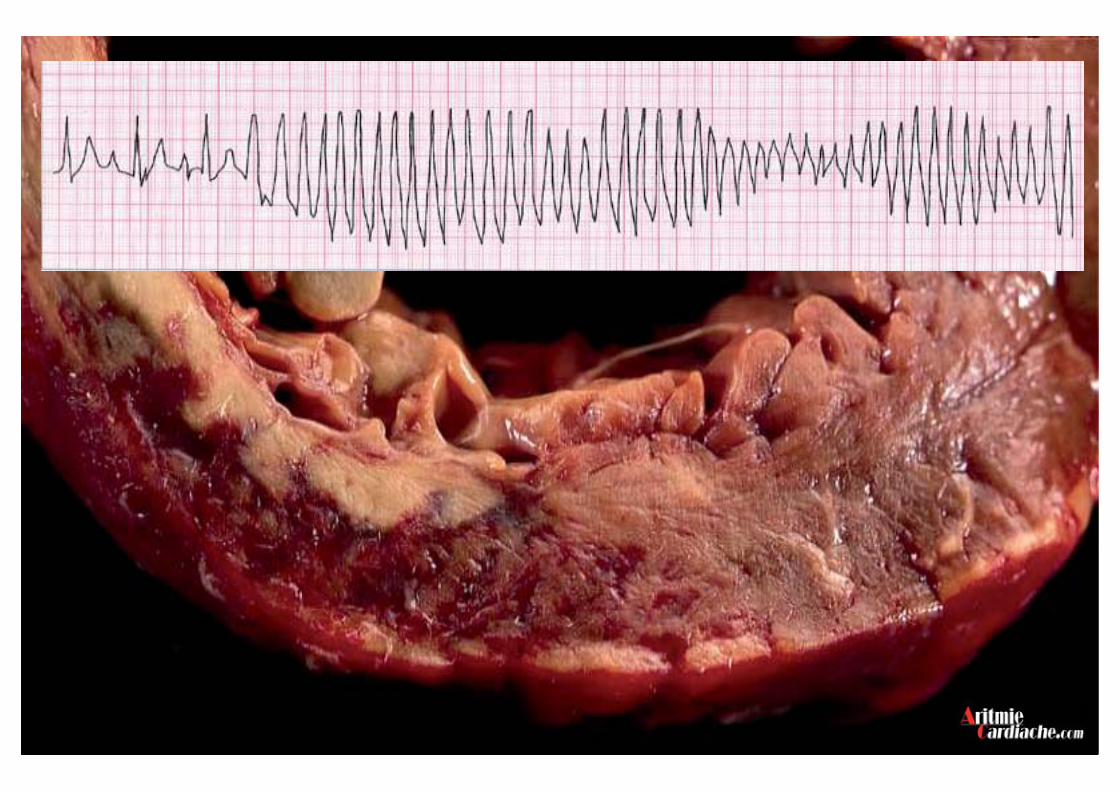
Fibrillazione Ventricolare
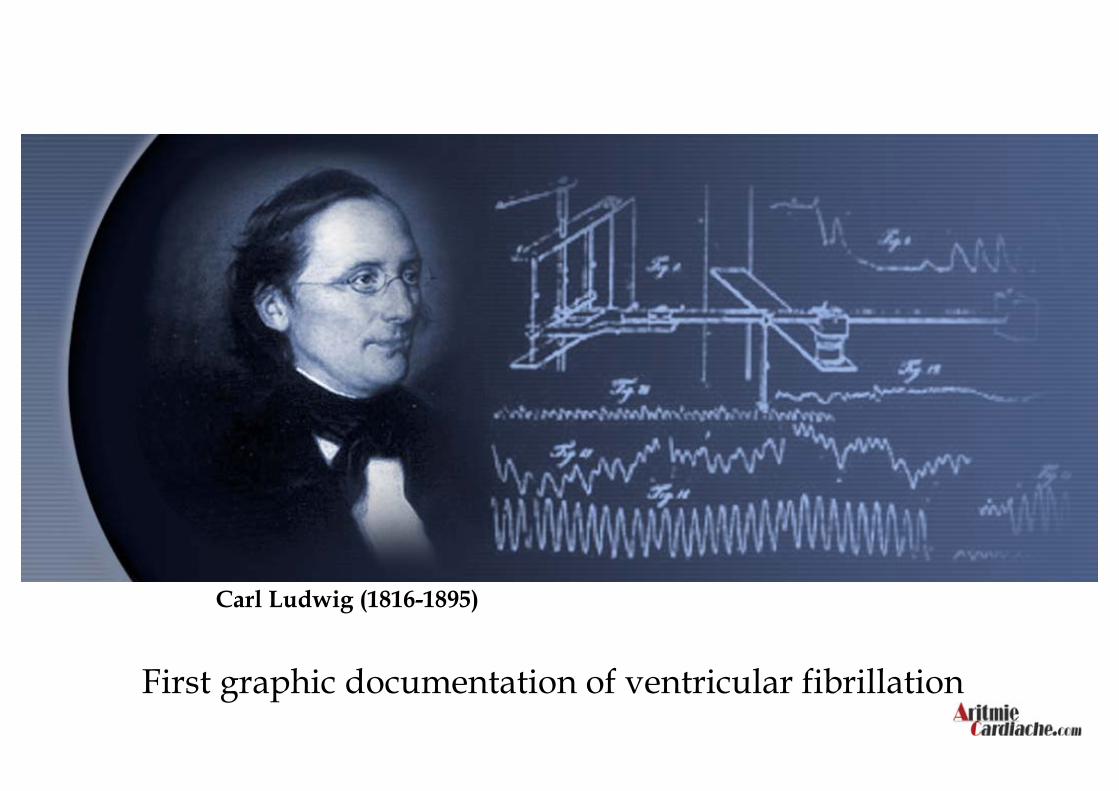
First graphic documentation of ventricular fibrillation
Carl Ludwig (1816-1895)

First successful defibrillation of exposed human heart
Required thoracotomy
ICD Evolution - 1947
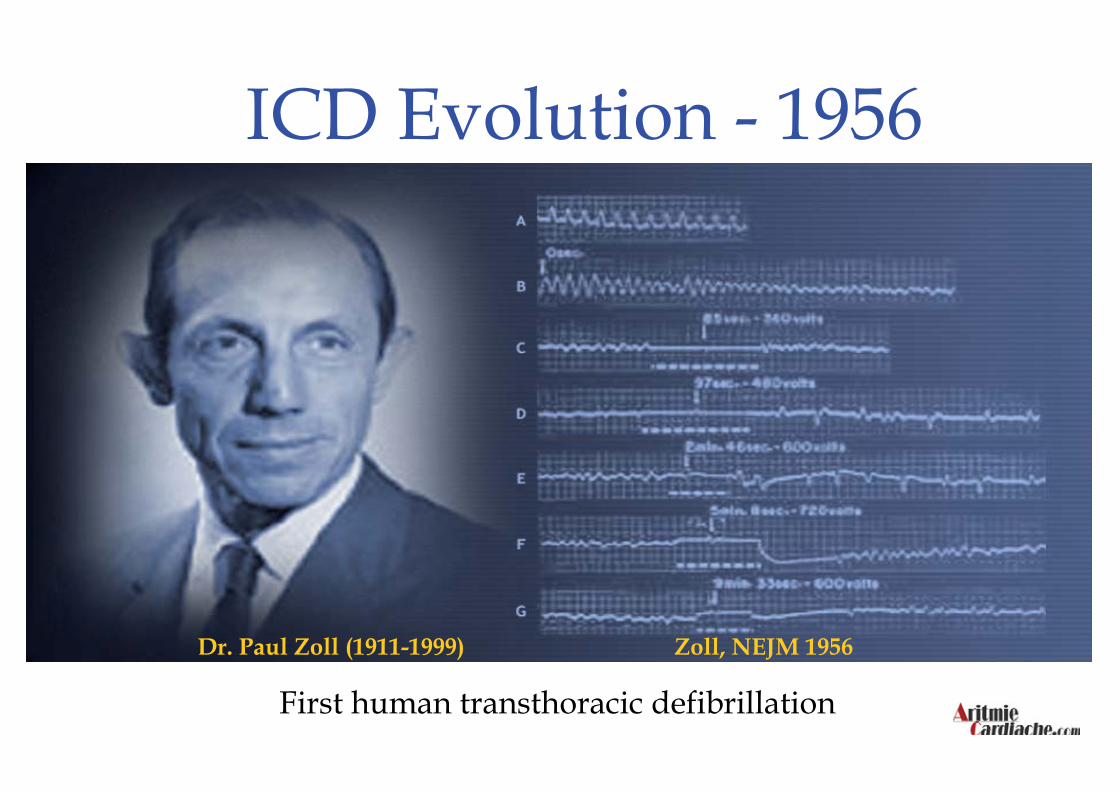
First human transthoracic defibrillation Dr. Paul Zoll (1911-1999) Zoll, NEJM 1956
ICD Evolution - 1956
Primo defibrillatore impiantabile
1970 – Michael Mirowski brevetta il primo defibrillatore totalmente impiantabile. Il sistema utilizzava un catetere per la misurazione delle variazioni di pressione e patch per la defibrillazione

ICD – Evoluzione Tecnologica
ICD – Prima generazione 1980
• Non programmabile
• Terapia solo shock
• Toracotomia
• Indicazione solo per i sopravvissuti a 2 arresti cardiaci
• 1,5 anni di durata
• Meno di 1000 impianti all anno

ICD – Terza Generazione
• Cateteri endocavitari
• Anestesia locale
• Programmabile e terapia Painfree
• Mono, bi e tricamerali
• MVP
• Fino a 6 anni di durata
• Più di 100,000 impianti all’anno
Oggi
0
20
40
60
80
MADIT MUSTT MADIT-II
Overall Death Arrhythmic Death
0
20
40
60
80
AVID CASH CIDS
Overall Death Arrhythmic Death
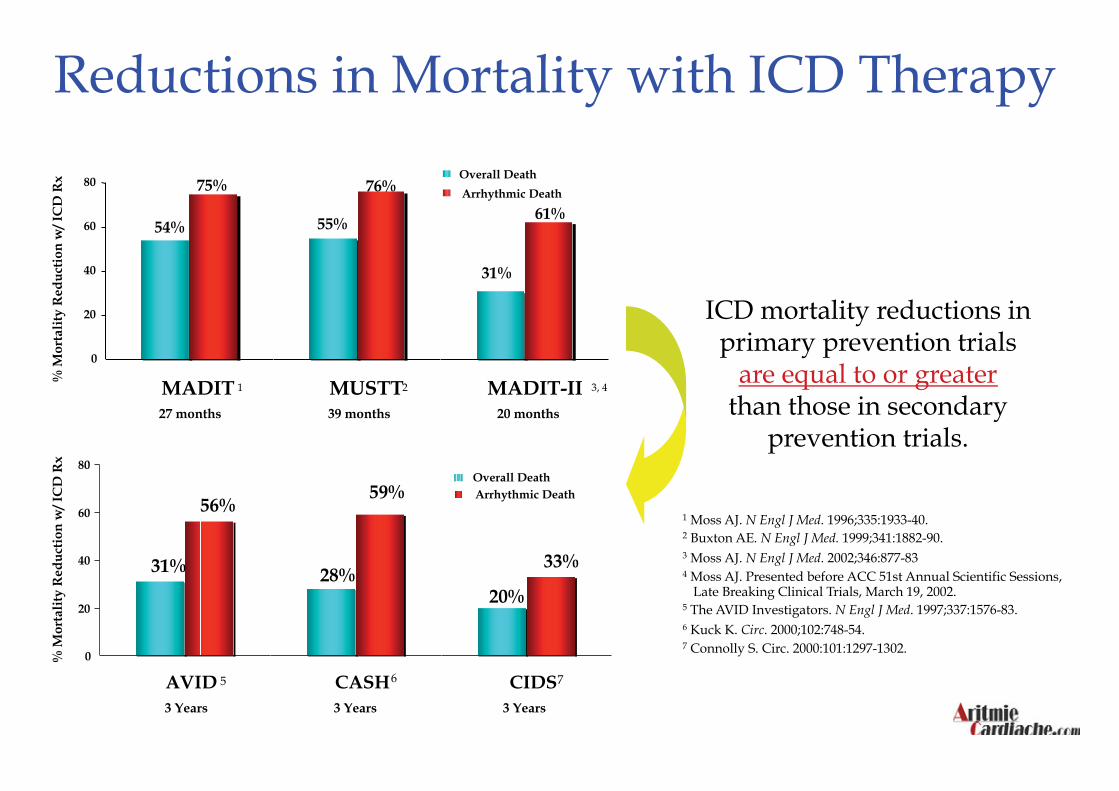
1 Moss AJ. N Engl J Med. 1996;335:1933-40. 2 Buxton AE. N Engl J Med. 1999;341:1882-90. 3 Moss AJ. N Engl J Med. 2002;346:877-83 4 Moss AJ. Presented before ACC 51st Annual Scientific Sessions,
Late Breaking Clinical Trials, March 19, 2002. 5 The AVID Investigators. N Engl J Med. 1997;337:1576-83. 6 Kuck K. Circ. 2000;102:748-54. 7 Connolly S. Circ. 2000:101:1297-1302.
ICD mortality reductions in primary prevention trials
are equal to or greater than those in secondary
prevention trials.
1 3, 4 2
5 7 6
Reductions in Mortality with ICD Therapy
54%
75%
55%
76%
31%
61%
27 months 39 months 20 months
31%
56%
28%
59%
20%
33%
% M
orta
lity
Red
uct
ion
w/ I
CD
Rx
% M
orta
lity
Red
uct
ion
w/ I
CD
Rx
3 Years 3 Years 3 Years

CLASS II
Ischemic Cardiomyopathy (at least 40 days after IMA)
Reduced EF (≤ 30%), NYHA I , Optimal Medical Treatment
(Level B)
Ischemic (at least 40 days after IMA) & Non-Ischemic Cardiomyopathy
31% ≤ EF ≤ 35%, NYHA II/III
Optimal Medical Treatment
(Level B)
Ischemic & Non-Ischemic Cardiomyopathy
(for Ischemic at least 40 days after AMI)
Reduced EF (≤ 30%), NYHA II/III, Optimal Medical Treatment
(Level A)
Ischemic Cardiomyopathy, Reduced EF (≤ 40%)
Non Sustained VT and Sustained Inducible VT
(Level B)
CLASS I
ICD - PRIMARY PREVENTION IN CARDIOMYOPATHY
AIAC Guidelines
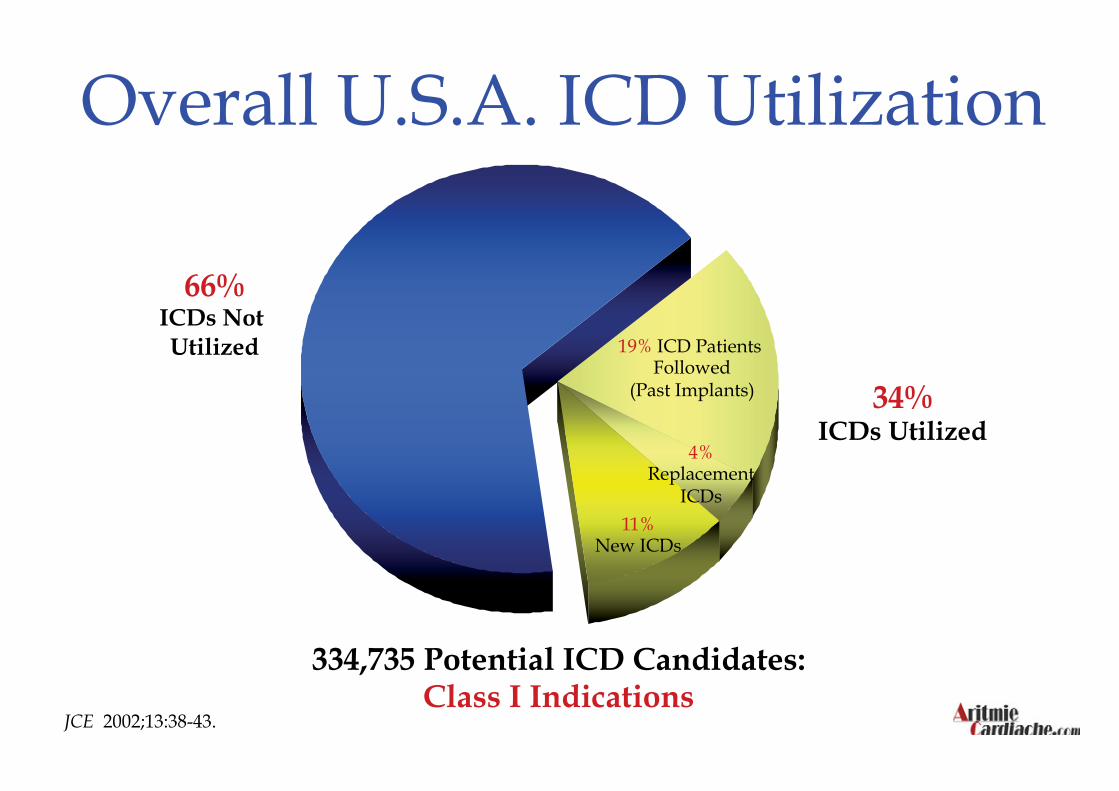
Overall U.S.A. ICD Utilization
66% ICDs Not Utilized
34% ICDs Utilized
334,735 Potential ICD Candidates: Class I Indications
19% ICD Patients Followed
(Past Implants)
4% Replacement
ICDs 11%
New ICDs
JCE 2002;13:38-43.
246.000, secondo le stime basate sulle recenti linee guida internazionali, le persone a rischio di morte cardiaca improvvisa
solo il 5,3% dei pazienti a rischio viene sottoposto ad un impianto di defibrillatore
Nel 2006 in Italia sono stati impiantati appena 13.000 defibrillatori
Situazione Italiana
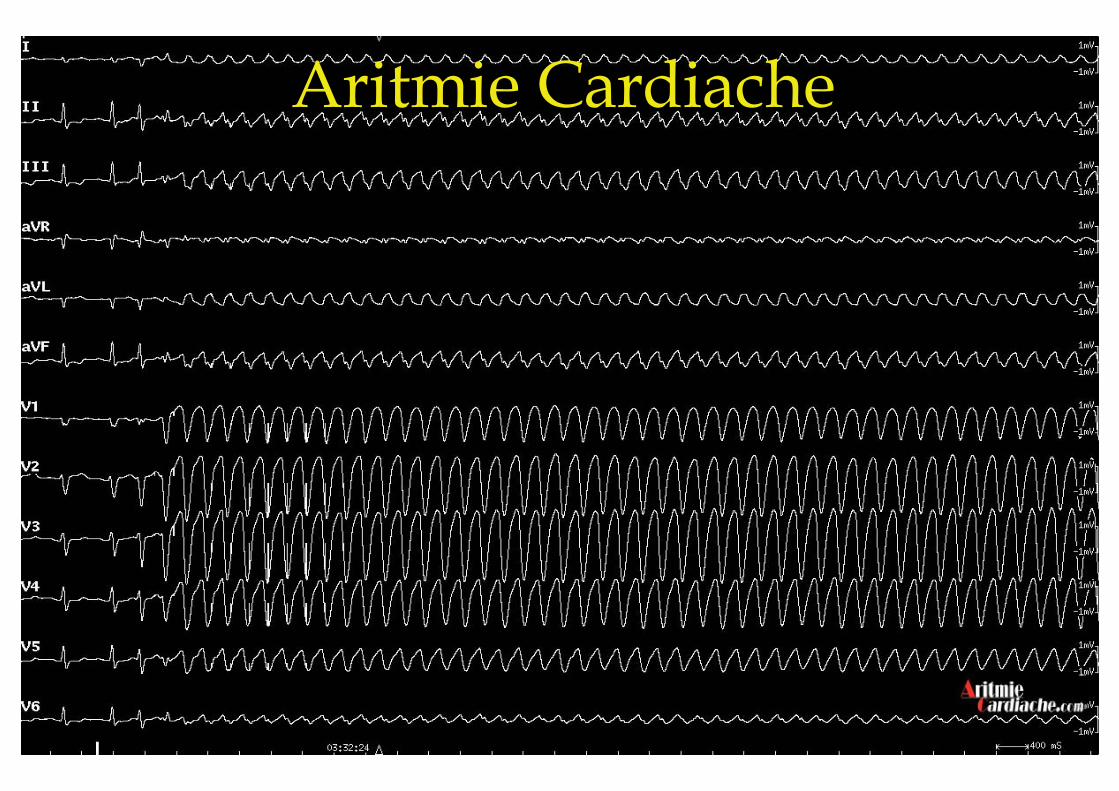
Aritmie Cardiache
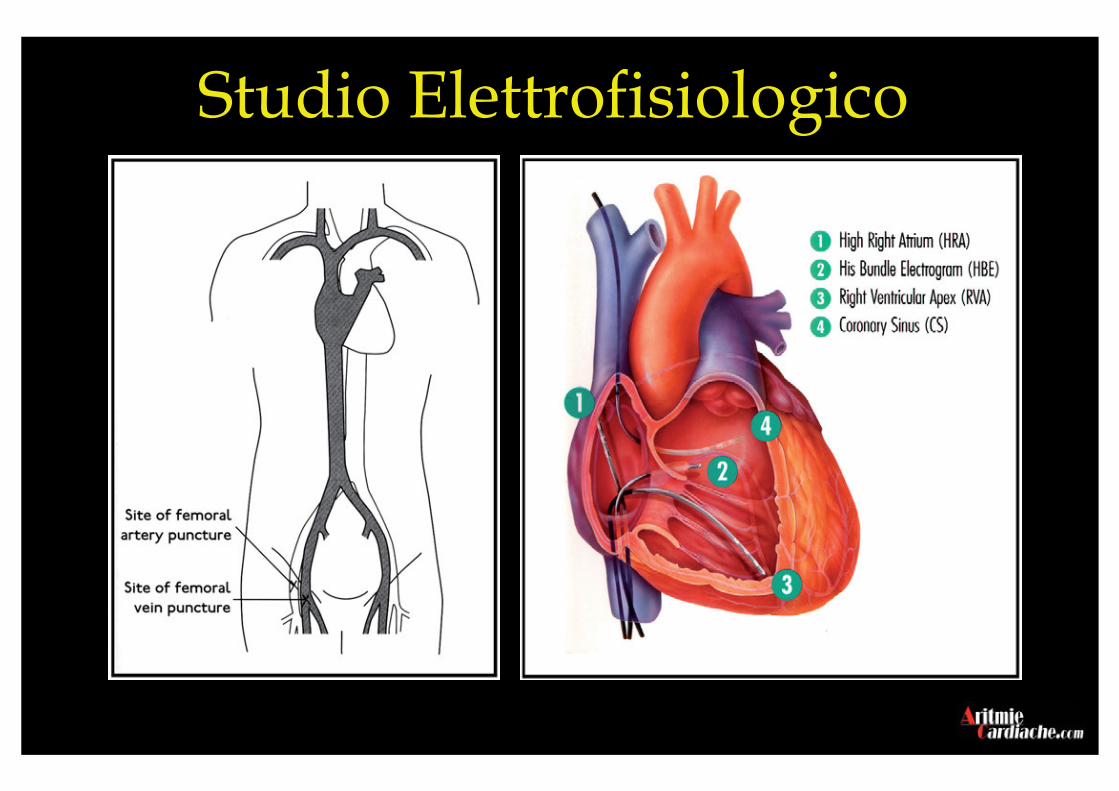
Studio Elettrofisiologico
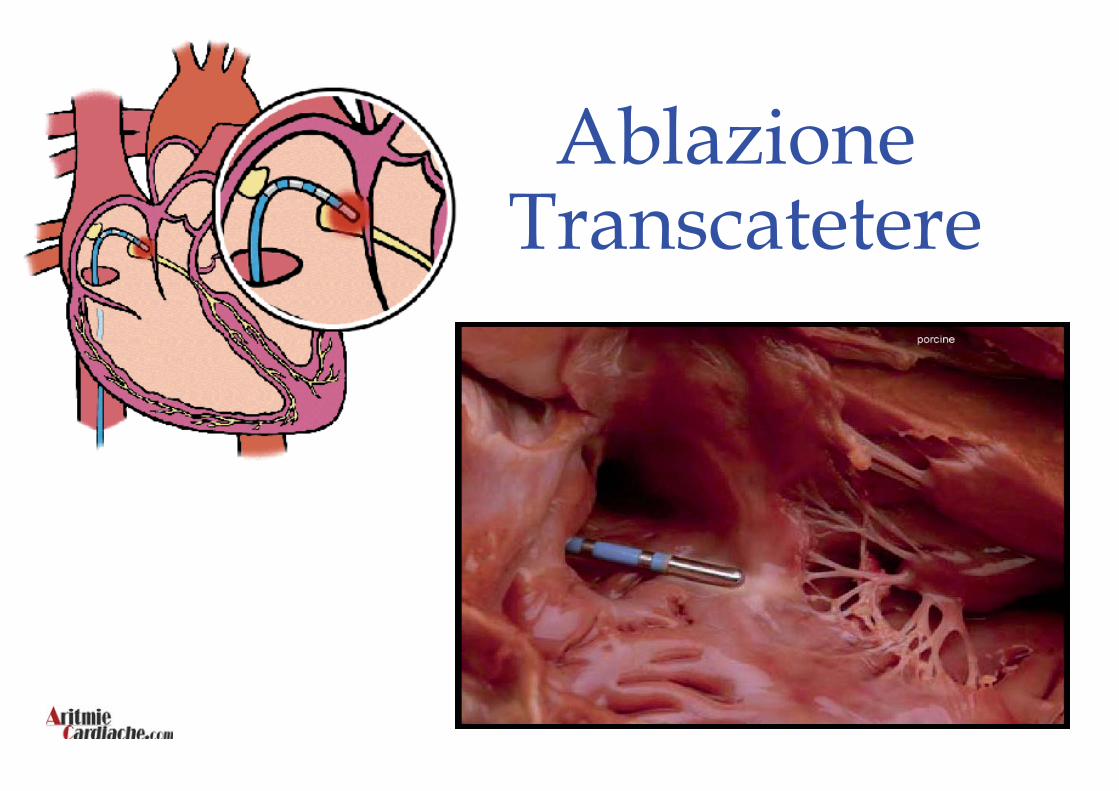
Ablazione Transcatetere
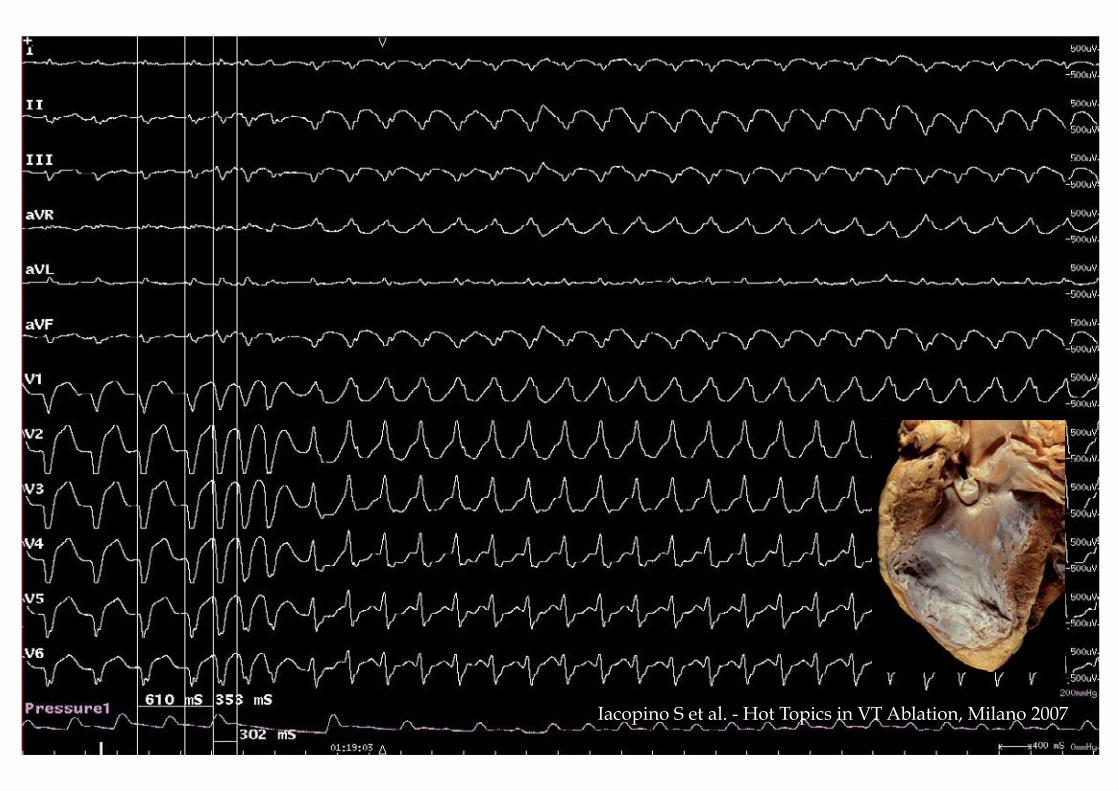
Iacopino S et al. - Hot Topics in VT Ablation, Milano 2007
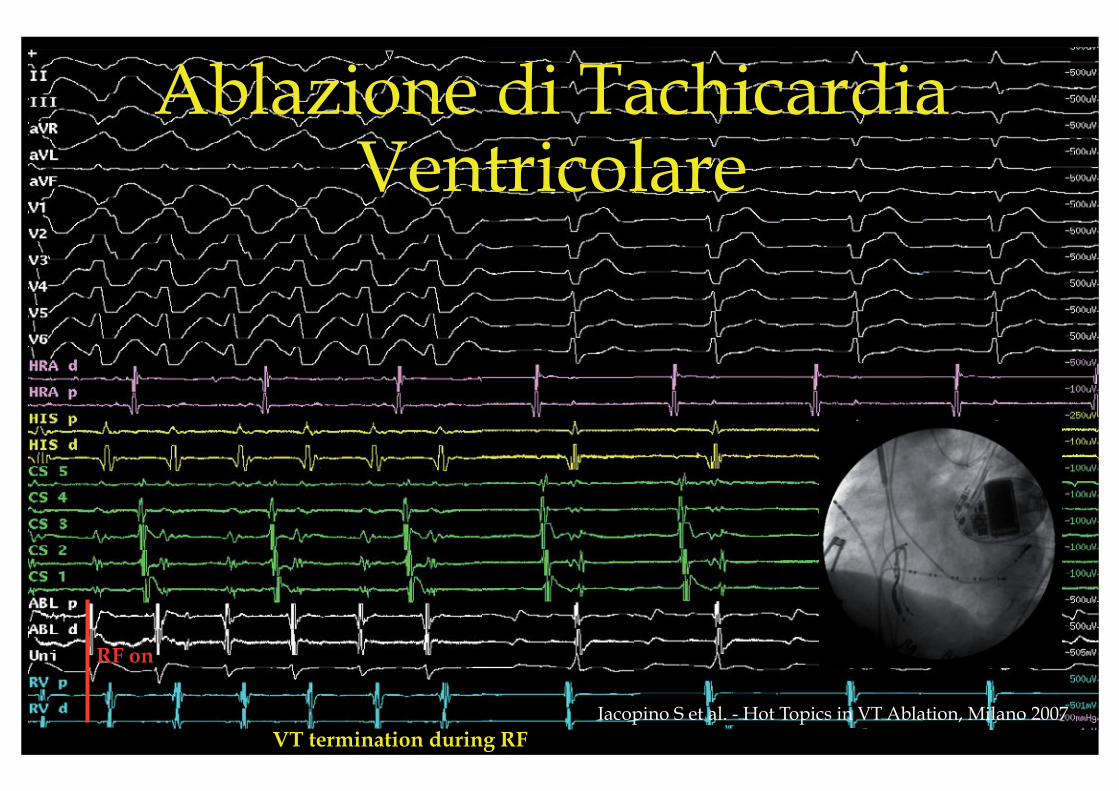
VT termination during RF
RF on
Iacopino S et al. - Hot Topics in VT Ablation, Milano 2007
Ablazione di Tachicardia Ventricolare

Sindrome di Wolff-Parkinson-Whyte
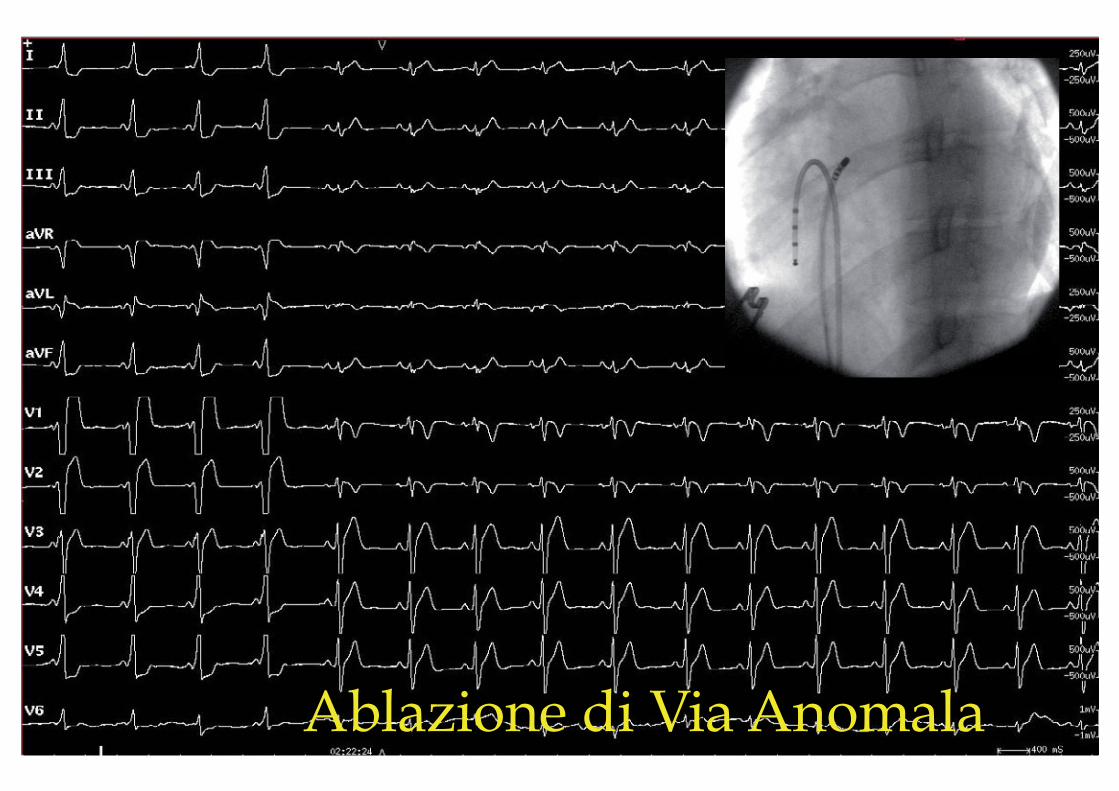
Ablazione di Via Anomala
Despite the evidence-based data and practical recommendations for indications of ICD therapy and ablation, these therapy has not been uniformly implemented worldwide Screening of patients at potential high risk
for arrhythmic death has not become a routine clinical practice It is premature to conclude that the
occurrence of SAD is a random phenomenon that cannot be predicted or prevented

La Catena della Sopravvivenza
I quattro anelli di questa catena sono: – L’accesso precoce al sistema EMS – La CPR precoce – La defibrillazione precoce – Il trattamento avanzato cardiaco precoce (ACLS)
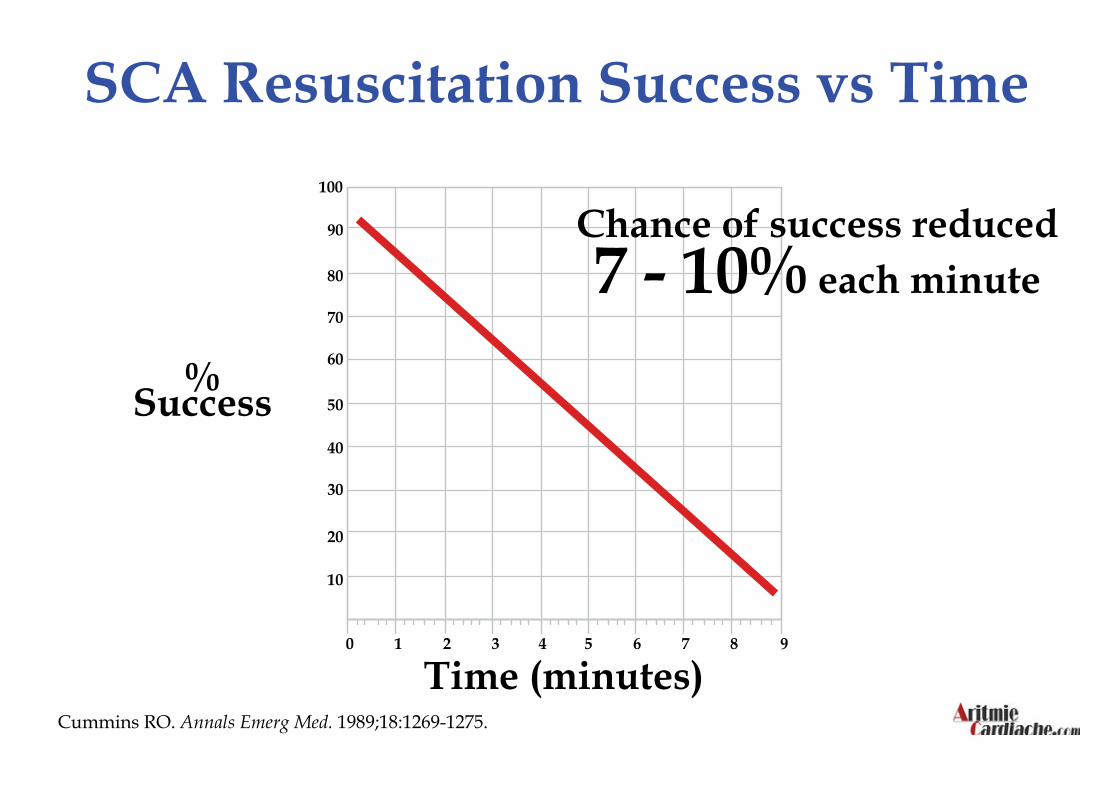
Cummins RO. Annals Emerg Med. 1989;18:1269-1275.
SCA Resuscitation Success vs Time
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9
% Success
Time (minutes)
Chance of success reduced 7 - 10% each minute
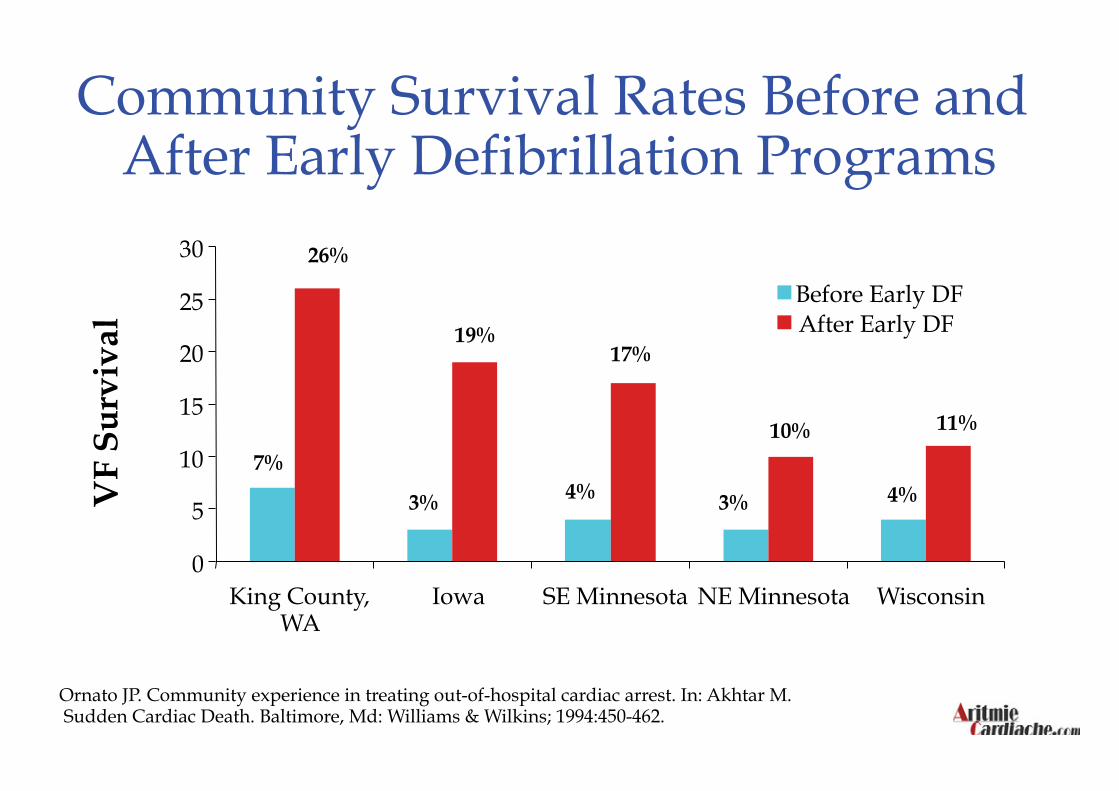
Community Survival Rates Before and After Early Defibrillation Programs
Ornato JP. Community experience in treating out-of-hospital cardiac arrest. In: Akhtar M. Sudden Cardiac Death. Baltimore, Md: Williams & Wilkins; 1994:450-462.
VF
Su
rviv
al
26%
19% 17%
10% 11%
7%
3% 4% 3% 4%
0
5
10
15
20
25
30
King County, WA
Iowa SE Minnesota NE Minnesota Wisconsin
Before Early DF After Early DF


“ Il Tempo è Vita“

Possibile Modello di Integrazione tra Territorio e
Ospedali per la Prevenzione della Morte Improvvisa
Prevenzione Generale
Prevenzione Primaria e Secondaria
Prevenzione sul Territorio