Embed Size (px)
Citation preview

Les grandes avancées en
Prévention CardiovasculaireQuelles leçons pour la prévention du déclin des
fonctions cognitives?
Jean Ferrières
Fédération de Cardiologie, Service d’Epidémiologie,
INSERM UMR 1027
CHU de Toulouse

Anthropologie

Scanning ancient history for evidence of modern diseases
Lancet 2013 Apr 6;381(9873):1211-22

Physiopathologie

Dysfonction Endothéliale : Étape Initiale des
Lésions Athéroscléreuses
Glass, Cell
2001, 104:
503-516

Progression et Développement des Lésions
Athéroscléreuses
Glass,
Cell 2001,
104:503-516

Complications des Lésions Athéroscléreuses :
Rupture de Plaque
Glass,
Cell 2001,
104:503-516

Traditional Contemporary
Atherosclerosis
Traditional vs. Contemporary Model

Plaque Morphology: Vulnerable vs. Stable
Thick Fibrous Cap Thin Fibrous Cap

Large lipid core
Rich in cholesterol
Rich in activated macrophages
Thin fibrous cap richin inflammatory cells
Poor in smooth muscle cells
Low grade stenosis
The Vulnerable Human Atherosclerotic Plaque

Atherosclerosis and Inflammation
TNF-
IL1, IL6, IL8
M-CSF, GM-CSF
MCP-1
macrophage
mLDL
AGE
smooth muscle cells
monocyte
activation
& differentiation
activation
& proliferation
Cytokine
production
activation
LDL
endothelium
Foam cells
Activation Adhesion Foam cell formation
Ve
sse
l w
all
lum
en

Novel Inflammatory Markers of Coronary Risk
Vascular and extravascular sources
Primary Pro-Inflammatory Cytokines
(e.g. IL-1, TNF-)
Pro-Inflammatory Risk Factors(oxidized LDL, infectious agents, etc)
Liver
IL-6“Messenger” Cytokine
CRP
SAA
Circulation
Endothelium
& other cells
ICAM-1Selectins, HSPs, etc.
Circulation 1999;100(11):1148-50

Clinique

J Am Coll Cardiol 2015;65(8):846-55
The Myth of the "Vulnerable Plaque": Transitioning From a Focus on
Individual Lesions to Atherosclerotic Disease Burden for Coronary
Artery Disease Risk Assessment
Risk Due to Nonobstructive Versus Obstructive Coronary Artery Disease
Annualized risk (percent) of myocardial infarction (MI) or cardiovascular (CV) death in 3,242 patients followed for a median of
3.6 years after baseline computed tomographic coronary angiography, according to the extent and severity of coronary artery
disease. Risk is low in patients with nonobstructive disease (<50% stenosis) involving 4 or fewer coronary artery segments
(limited disease). Conversely, risk is similarly high in patients with nonobstructive disease if more than 4 segments are
affected (extensive disease) compared with patients with obstructive disease (≥50% stenosis). Modified with permission from
Bittencourt et al.

J Am Coll Cardiol 2015;65(8):846-55
The Myth of the "Vulnerable Plaque": Transitioning From a Focus on
Individual Lesions to Atherosclerotic Disease Burden for Coronary
Artery Disease Risk Assessment
Fate of Ruptured Coronary Atherosclerotic Plaques According to Thrombotic Milieu
In the most common scenario, small thrombus formation associated with plaque rupture is contained and vascular
occlusive thrombus is inhibited.

Interventions - RCT

Eur Heart J 2015;36(8):472-4
How does lipid lowering prevent coronary events? New insights from
human imaging trials
The lumen remains largely unchanged, the lipid core shrinks, the amount of fibrous tissue may increase as
a proportion of the intima, but modestly decrease in absolute terms, while the content of calcified tissue
actually rises with lipid lowering.
An integrated depiction of the effects of aggressive lipid lowering on human coronary
plaques as revealed by ‘virtual histology’ and other cross-sectional imaging studies.

Impact of Statins on Serial Coronary Calcification During Atheroma
Progression and Regression
JACC 2015;65(13):1273-82
Natural plaque progression likely involves lipid-pool expansion coupled
with microcalcifications within lipid pools. Following long-term high-
intensity statin therapy, plaque regression manifests as delipidation and
probable vascular smooth muscle cell calcification, promoting plaque
stability.
Plaque Calcification in the Setting of No-Statin Therapy or High-Intensity Statin Therapy

Epidémiologie et
Santé Publique

La continuité de la prévention des maladies chroniques
Amélioration de la prise en charge
des facteurs de risque connus et
utilisation de nouveaux facteurs de
risque (génétique, modes de vie)
Mise au point de nouveaux outils
de dépistage non invasifs et
meilleure prise en charge des
phases précoces de
l’athérosclérose
Meilleur repérage des sujets à risque
de complications et amélioration de
la prise en charge (médicale et
communautaire) des formes
terminales de l’athérosclérose
Prévention
PRIMAIRE
Prévention
SECONDAIRE
Prévention
TERTIAIRE
Diminution de
l’INCIDENCE
Diminution de la
PREVALENCE/SÉVÉRITÉ
Diminution des
SÉQUELLES/HANDICAPS
Sujets malades
asymptomatiques ou
symptomatiques
Sujets dans une
phase avancée
de la maladie
Sujets
à risque
Ferrières J. Sciences Humaines et Sociales. Abrégés PCEM1. MASSON. Paris 2006

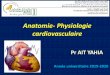
Trends in age-specific coronary heart disease mortality in the
European Union over three decades: 1980–2009
European Heart Journal 2013;34:3017-27
Age-standardized mortality rates, total percentage change, average annual percentage
changes, and Joinpoint analysis by country and sex, all ages combined
Values are unadjusted averages of rates for each 5-year period, or for as many years as datawere available within the period. Exceptions, where data
were not available for all years, are: Belgium (to 2006); Denmark (to 2006); France (to 2008); Italy (no data 2005); Lithuania (no data 1980, 1983,
1984); Portugal (no data 2004 to 2006); and Slovenia (no data before 1985).a25-year total crude change calculated from difference between 1980–84 average rate and 2005–09 average rate.bData for Germany prior to 1990 calculated from raw data for the Former East and West Germany. 1980–84 data for Czech Republic and Slovakia are
combined data from Czechoslovakia, therefore, not directly comparable.
Males
* 25-year crude total % changea
0
20
40
60
80
100
120
140
160
180
200
Italy
Poland
Greece
Portugal
Spain
France
1980-84 1990-94 2000-04 2005-09
-50
-7
-49
-36
-16
-46

Evolution des taux spécifiques de mortalité en France de 1980 à 2008
Taux standardisés sur l’âge (population de référence, France 1990)
InVS. Bulletin Epidémiologique Hebdomadaire,2007;35-36.
InVS. Bulletin Epidémiologique Hebdomadaire,2011;249-55.
2008
194
218
Maladies cardiovasculaires
- 56 % sur 28 ans
Pathologies tumorales
- 15% sur 28 ans
Evolution des causes médicales de décès en France

Evolution du taux proportionnel de mortalité
par maladies cardiovasculaires
en France de 1980 à 2008
1980 2004 2008
%
37.4 %
28.9 %
- 26 % sur 28 ans
Source : CépiDc
27.5 %
2000
30.5 %
Evolution des causes médicales de décès en France

Evolution du taux proportionnel de mortalité par maladies
cardiovasculaires et pathologies tumorales
en France de 1980 à 2008
1980 2004 2008
%
37.4 %
28.9 %
Maladies cardiovasculaires - 26 % sur 28 ans
Source : CépiDc
27.5 %
2000
30.5 %
21.6 %
29.6 %
Pathologies tumorales
+ 37 % sur 28 ans
Evolution des causes médicales de décès en France

Baisse de la
mortalité
cardiovasculaire
Baisse de la létalité des
accidents
cardiovasculaires
Baisse de l’incidence des
maladies
cardiovasculaires


Coronary event ratewith 95% confidence interval, age standardized, age 35-64
WHO MONICA Project
Lancet 1999 ; 353 : 1547-1557

Définition d’un registre
Structure ayant pour but d’enregistrer de façon continue et exhaustive des renseignements sur une
pathologie donnée, dans le cadre d’un territoire géographique déterminé.

Fournir des statistiques sanitaires :
Incidence
Taux de létalité, taux spécifique et proportionnel de mortalité
Evolution dans le temps : effet du dépistage et de la prévention
Disparités géographiques : hypothèses étiologiques


Roger VL, et al. Circulation 2010;121(7):863-9
L’incidence des STEMI a diminué et celle des NSTEMI a augmenté
La mortalité à court terme (≤ 30 jours) a diminué de plus de 50 %
• Objectif de l’étude : Analyser l’impact de l’ajout du
dosage de la troponine pour le diagnostic de l’infarctus
du myocarde
• Méthodologie de l’étude : Étude sur 2 816 patients
hospitalisés pour un infarctus du myocarde(IDM)
Recrutement des patients entre 1987 et 2006
• Critères d’évaluation : Incidence des infarctus du
myocarde, sévérité et survie sur une période
de 6 ans
Tau
x d
’in
cid
en
ce a
justé
su
r
l’âg
e e
t le
sexe
(po
ur
100 0
00)
Avec dosage de la Troponine T
Sans dosage de la Troponine T
On observe une augmentation des NSTEMI
Incidence des hospitalisations pour un IDM, entre 1987 et 2006, dans le
Comté d’Olmsted, Minnesota, selon le statut de l’élévation du segment ST
Comment a évolué l’épidémiologie de l’infarctus du myocarde
depuis 20 ans ?

Incident MI and stroke in France
Average annuel rates per 100 000
Data from the MONICA (MI) and Dijon (stroke) population-based registries
* <45 years for stroke rates.
Data collected in 1997-2000 (MI) and 1995-1997 (stroke)
0
400
800
1200
1600
2000
35-44* 45-54 55-64 65-74 75-84 85 and
over
Myocardial infarction in men
Stroke in men
Myocardial infarction in women
Stroke in women
years
/ 100 000 persons/year
Wolfe CDA, et al. Stroke 2000;31:2074-9.
Montaye M, et al. BEH 2006;62-4.

Age standardized coronary heart disease mortality and event rate in
selected European regions (men, aged 35-64 years)
Population Official CHD CHD mortality Coronary events
mortality rate per 100 000† per 100 000‡
per 100 000*
Glascow (United Kingdom) 332 365 777
Belfast (United Kingdom) 280 279 695
Lille (Northern France) 89 172 298
Strasbourg (North-Eastern France) 80 141 292
Toulouse (South-Western France) 53 91 233
Barcelone (North-Eastern Spain) 63 76 210
Ferrières J. Heart 2004 ; 90: 107
* Based on death-certificate enumeration
† Fatal events included definite, possible and unclassifiable (mainly sudden deaths
with no available diagnostic information) coronary deaths
‡ Coronary events included non-fatal events (definite myocardial infarction) and fatal
events

Les formules de risque
cardiovasculaire

Diagramme SCORE : risque à 10 ans de décès cardiovasculaire dans les pays
à bas risque cardiovasculaire basé sur les facteurs de risque suivants : âge,
sexe, tabagisme, pression artérielle systolique et cholestérol total
Les pays à bas risque sont
l’Andorre, l’Autriche, la
Belgique, Chypre, le
Danemark, la Finlande, la
France, l’Allemagne, la
Grèce, l’Islande, l’Irlande,
Israël, l’Italie, le
Luxembourg, Malte,
Monaco, les Pays Bas, la
Norvège, le Portugal, la
république de Saint Marin, la
Slovénie, l’Espagne, la
Suède, la Suisse, le
Royaume-Uni.
A noter que le risque
d’événements
cardiovasculaires totaux
(fatals + non-fatals) va
être approximativement
3 fois supérieur aux
chiffres donnés

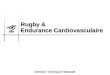
Ten-year risk of all-cause mortality: assessment of a risk prediction
algorithm in a French general population
Independent predictors of 10-year all-cause mortality and corresponding score of
the risk prediction algorithm
Hazard Ratio 95% p ScoreConfidence Interval
Toulouse centre (South-Western France) 1.00 0Strasbourg centre (North-Eastern France) 1.04 [0.67 - 1.61] 0.857 0Lille centre (Northern France) 1.76 [1.21 - 2.58] 0.003 335-44 years old 1.00 045-54 years old 1.64 [1.02 - 2.64] 0.040 355-64 years old 3.89 [2.49 - 6.09] < 0.001 7Women 1.00 0Men 2.11 [1.48 - 3.01] < 0.001 4Educational level ≥ high school completion 1.00 0Educational level < high school completion 1.57 [1.05 - 2.33] 0.026 2Non-smoking 1.00 0Smoking < 15 pack-years 2.61 [1.45 - 4.70] 0.001 5Smoking ≥ 15 pack-years 2.90 [2.01 - 4.17] < 0.001 6Non diabetes 1.00 0Diabetes 1.62 [1.10 - 2.37] 0.014 3Systolic blood pressure < 160 mmHg 1.00 0Systolic blood pressure ≥ 160 mmHg 1.57 [1.03 - 2.39] 0.036 2LDL-cholesterol < 5.2 mmol/l (200 mg/dl) 1.00 0LDL-cholesterol ≥ 5.2 mmol/l (200 mg/dl) 1.62 [1.01 - 2.61] 0.047 3
Bérard et al. Eur J Epidemiol 2011:26(5):359-68

(1) Reference is 35-44 years old; (2) Reference is never smokers; (3) Reference is Southwestern France.
* Educational level < high school completion
** Risk estimate corresponds to 1-unit change in Smoking (in pack-years)
*** LDL-cholesterol ≥ 5.2 mmol/L or ≥ 200 mg/dL [7.8% (168/2162)]
**** Diabetes was assessed for subjects with fasting blood glucose ≥ 7 mmol/l (126 mg/dl) or under hypoglycaemic drug treatment
Predictors of 16-year risk of all-cause mortality
Multivariate survival analysis
Preventive Medicine 2015;81:195-201
HR 95% CI p
45-54 years old (1) 1.33 0.87-2.03 0.181
55-64 years old (1) 3.43 2.32-5.07 <0.001
Men 1.56 1.09-2.22 0.014
Low educational level* 1.75 1.21-2.53 0.003
Former smokers (2) 0.93 0.57-1.50 0.756
Current smokers (2) 2.63 1.71-4.02 <0.001
Smoking (pack-years)** 1.01 1.00-1.01 <0.001
Centre: Northeastern France (3) 0.95 0.56-1.61 0.850
Centre: Northern France (3) 1.77 1.30-2.42 <0.001
Blood pressure ≥ 160/95 mmHg 1.67 1.22-2.30 <0.002
LDL-cholesterol ≥ 5.2 mmol/L*** 1.72 1.09-2.72 0.019
Diabetes**** 2.03 1.36-3.01 <0.001

Conflits d’intérêt:
Amgen, MSD, Sanofi
Blanco et al. 2016


Le risque attribuable en
population générale

0
10
20
30
40
50
60
70
80
90
100
Pression artérielle, LDL-C, HDL-C, triglycérides, tabagisme et
diabète
IMC ≥ 27 (+3%)
76%
%
21% inexpliqué
79%
Risque attribuable au niveau de la population pour la
maladie coronaire
Congress of the European Society of Cardiology. September 1-5, 2007, Vienna (Austria)Eur Heart J 2007;(suppl):147
PAR 16% pour LDL>1,6g/L

Comparison of coronary heart disease and stroke risks attributable to
vascular risk factors: Results from the PRIME Study
Full adjusted population-attributable risks for CHD and stroke events
Bongard et al. Annual Congress of the European Society of Cardiology. August 31-September 4, 2013, Amsterdam (Netherlands).
CHD versus Stroke versus
no event (n=410) no event (n=118)
High blood pressure (BP ≥ 140/90 mmHg) 21.1 [12.1-30.1] 32.8 [17.0-48.6]
Diabetes mellitus 1.9 [0.3-4.1] 6.4 [1.0-11.9]
Current smoking 14.8 [8.5-21.0] 15.9 [4.2-27.6]
Hypercholesterolemia (LDL-c ≥ 4.1 mmol/L) 11.1 [4.3-18.0] -
Low HDL-c (< 1 mmol/L) 9.8 [2.6-17.0] -
Hypertriglyceridemia (≥ 1.7 mmol/L) - -
Obesity (BMI ≥ 30 kg/m²) 5.4 [0.7-10.1] -
Teetotallers 8.5 [2.9-14.1] -
Excessive alcohol consumption - -
Overall † 71.2 [57.4-85.0] 43.7 [24.4-62.9]
BMI: body mass index
† To compute overall PAR for CHD, exposure was defined as high blood pressure or diabetes or current smoking or
hypercholesterolemia or low HDL-c or obesity or no alcohol consumption. To compute overall PAR for stroke, exposure was
defined as high blood pressure or diabetes mellitus or current smoking.
Overall PARs were adjusted for age, centre, antihypertensive drug treatment, and lipid-lowering drug treatment. All other
estimates are adjusted for age, centre, antihypertensive drug treatment, lipid-lowering drug treatment in addition to other
variables significant in the column.

Risk factor distribution
Population strategy High risk strategy
“Threshold of normality”
Risk factor
AFTER BEFORE
AFTER
Preventive Medicine: “High risk” strategy or
population strategy

Benefits, challenges and registerability of the
polypill
– Recognition that the individual titration of each component
does not work on grounds of cost and practibility.
– Costs are lower with generics.
– Easier patient compliance.
– Ensures that all the evidence-based medicines are given.
– More widespread use.
– Potentially very large public health benefits at affordable
costs.
Sleight. Eur Heart J 2006;27:1651

The cost of cardiovascular disease:
rising, declining or staying still?
– Although major cardiovascular disease risk factors such as smoking,
hypercholesterolemia and hypertension are better prevented, detected and
treated, risk factors trends in obesity and associated diabetes are likely to
decelerate the observed cardiovascular disease morbidity and mortality
decreasing trends.
– Even if age-standardised morbidity and mortality might continue to decrease,
demographic factors, both in relation to ageing of the general population and
the relatively faster ageing of ethnic subgroups, may inflate healthcare
expenditure.
– As demand for services and interventions is a major determinant of healthcare
costs, the advent of new and more expensive healthcare technology may
negate the potential for any savings.
– Therefore, epidemiological, demographic and health technology factors
combined are likely to inflate future healthcare cardiovascular disease costs.
Lyratzopoulos. Heart 2006;92:1361
Future trends in epidemiology, demography and new health technology

Primary prevention and risk factor reduction in coronary heart disease mortality among working aged men and women in eastern Finland over 40
years: population based observational study
BMJ 2016;352:i721
Age standardised mortality from coronary heart disease in 1969-2012 (logarithmic scale), for
working aged men and women (age 35-64 years) in eastern Finland

Primary prevention and risk factor reduction in coronary heart disease mortality among working aged men and women in eastern Finland over 40
years: population based observational study
BMJ 2016;352:i721
Predicted and observed reduction (%) in coronary heart disease mortality
in men aged 35-64 years, 1972-2012

Primary prevention and risk factor reduction in coronary heart disease mortality among working aged men and women in eastern Finland over 40
years: population based observational study
BMJ 2016;352:i721
Predicted and observed reduction (%) in coronary heart disease mortality
in women aged 35-64 years, 1972-2012