Embed Size (px)
DESCRIPTION
guia de oma 2015
Citation preview

19/10/2015
http://contemporarypediatrics.modernmedicine.com/contemporary-pediatrics/news/acute-otitis-media-update-2015?page=full 1/6
Contemporary PediatricsPediatrics7-valent pneumococcal conjugate vaccineLog in to save to my locker
Acute otitis media: Update 2015
New guidelines have revised diagnostic criteria for acute otitis media. Pediatricians should adopt theseguidelines into practice and, as a result of new findings, should reconsider the antibiotics chosen astreatment in children vaccinated with pneumococcal conjugate vaccine.
March 01, 2015By Michael E Pichichero, MD
By: Janet R Casey, MD, and Michael E Pichichero, MD
In May 2004, the American Academy of Pediatrics (AAP) joined with the American Academy of Family Physicians to publish aclinical practice guideline on the diagnosis and management of acute otitis media (AOM).1 In 2013, the AAP revised theguideline with important changes presented in this review.2
The 2004 guideline was not without critics, and the same is true of the 2013 revision. The main areas of controversy surrounddiagnostic criteria for AOM, the notion of “uncertain diagnosis” and the watchful waiting option, and the selection of empiricantibiotic treatments recommended. Each of these issues will be discussed. We also discuss the otitis-prone child and theemergence of biofilms as a problem contributing to recurrent AOM and chronic otitis media with effusion (OME).
Diagnosis
The 2004 guideline criteria for diagnosis of AOM were insufficiently precise. Children with OME could fit the definitionintended only to identify AOM. In the 2013 guideline, the diagnosis was refined and improved. Table 1 shows the key summarystatements regarding diagnostic criteria from the 2013 guideline.2
The most important diagnostic feature forAOM noted in the new guideline is a bulgingor full tympanic membrane (TM) associatedwith middle ear effusion, and the TM isopaque. Experts in otitis media diagnosis arein consensus supporting this change.3 Thebulging occurs from pressure behind the TMcaused by inflammation in the middle earspace. The AOM is not associated with aretracted TM, so a determination of retractionof the TM with middle ear effusion,regardless of TM opacity, is not AOM. Abulging compared with a retracted TM can bedifficult to distinguish.
Because of the inflammation in the middle earspace during AOM, typically the TM becomesthickened and nontranslucent or completelyopaque. A translucent TM is not seen withAOM. With a translucent or semitranslucentTM and middle ear fluid visualized behind theTM, the likely diagnosis is OME.3
Redness of the TM is not generally a valuable diagnostic sign of AOM. An exception would be the presence of a single red TMand the other TM not red, suggesting inflammation of the TM, consistent with the diagnosis of AOM if there is fluid visualizedbehind the TM. Most likely, such an examination represents an early AOM before inflammation has persisted to cause the TM tobecome more white or yellowish and opaque.
Acute otitis media is not associated with inflammation, so prior diagnostic definitions of OME stipulated absence of symptomsother than hearing loss. A child with OME may feel discomfort, however, and may feel popping noises that may cause eartugging or even crying.4
Recommended: An update on otoacoustic emissions hearing screening
Use of pneumatic otoscopy is very helpful to improve diagnostic accuracy, and its use is advocated in the 2013 guideline.2Positive pressure on insufflation will result in movement backwards by a bulging TM, and negative pressure will result inmovement forward by a retracted TM. Thus, properly used, pneumatic otoscopy can allow the clinician to have a betterappreciation for the position of the TM, a key diagnostic feature.
An otoscope head that permits insertion of an insufflator is also needed. The challenge is to get a good seal with an otoscopespeculum and to restrain the child long enough to perform the insufflation procedure. To achieve a seal, use of a speculum with a

19/10/2015
http://contemporarypediatrics.modernmedicine.com/contemporary-pediatrics/news/acute-otitis-media-update-2015?page=full 2/6
softer rubber sleeve midshaft of the speculum may be helpful.
NEXT: instruments to aid in diagnosis
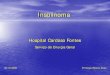
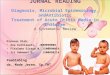
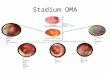
As an adjunct to the otoscopic examination, 2 instruments are available as aids in the diagnosis of AOM and OME. Atympanometer identifies movement of the TM in response to positive and negative pressure. If no movement occurs withpressure, then the tympanogram readout is flat (Figure 1).5 This is the typical case for AOM and OME, so a flat tympanogram isabnormal but does not differentiate between AOM and OME. Infrequently, when the TM is becoming full and before it isbulging, a positive pressure tympanogram (Figure 2) is obtained. This occurs early in the AOM pathogenesis. In some cases, theTM will be retracted, giving a negative pressure tympanogram readout (Figure 3). A viral upper respiratory infection (URI),sometimes with concomitant middle ear fluid and sometimes OME, can result in a negative pressure tympanogram.
A disadvantage of tympanometry is that it requires a seal of theinserted speculum-like device in the external auditory canal. Inchildren aged younger than 2 years, when AOM is most common, thechild often moves and a seal cannot be obtained. Also, if a child iscrying, a tympanogram reading cannot be obtained.
Thesensitivityandspecificityof
tympanometry, using pneumatic otoscopy as a gold standard, hasbeen recently assessed and shows that a normal tympanogram is veryspecific to rule out AOM and OME.6 An abnormal tympanogramshould prompt a second visual look at the TM, because the test is notsensitive to detect AOM or OME.
Another instrument to assist in diagnosis of AOM and OME is thespectral gradient acoustic reflectometer (SGAR). This device relieson emittance of a sonar sound wave that bounces off the TM andback to the device to produce a reading. If the wave passes through athickened TM, the wave is slowed giving a lower reading as occurswith AOM and OME. If the wave passes through fluid of any type, itslows the wave with thicker fluid (pus with AOM) impeding thewave more than thinner fluid (OME).
This instrument does not require a seal in the external auditory canal,and readings can be obtained in the crying child. The main limitationis the presence of wax in the external auditory canal. Cerumen thatblocks the sonar wave emitted by the acoustic reflectometer ismisinterpreted by the device, and false readings occur.
More: An essential update on cystic fibrosis
The sensitivity and specificity of SGAR, using pneumatic otoscopy as a gold standard, has been recently assessed and shows thata normal SGAR reading is very specific to rule out AOM and OME.6 Similar to the tympanogram, an abnormal reading shouldprompt a second visual look at the TM because the test is not sensitive to detect AOM or OME. The charges for tympanometryand SGAR are usually the same as reimbursed by most insurance companies. Most often, however, reimbursement is notavailable for both measurements on the same patient at the same visit.
Uncertain diagnosis and observation option
The notion that the clinical manifestations of AOM and OME are distinct from those of a viral URI s not accurate: AOM almostalways occurs in the context of a viral URI, typically between the third and seventh day of a URI.7 Therefore, children withAOM and OME and a URI have rhinorrhea, nasal congestion, and elevated body temperature. When children have a viral URI,AOM, or OME, they are cranky, and they feed and sleep poorly. Clinicians (and parents) presume that a child pulling at the earshas an AOM. Even pulling the ear, however, is not a clear clinical manifestation of AOM or OME.4 When the TM becomesretracted, as often occurs with viral URIs, the change in position of the TM causes discomfort and ear tugging.
As a consequence of the vagueness of symptoms of AOM and their similarity to the symptoms of a viral URI or OME, as well asdifficulties in visualizing the TM and performing pneumatic otoscopy, the recent AAP guideline maintains that sometimes thereis an uncertain diagnosis of AOM.2 This is especially true in infants and young children, in whom symptoms are either mild oragain overlap with the symptoms of a viral URI. Cerumen may certainly impede a proper visualization of the TM, which alsomay only show subtle changes. As well, apart from the factor of clinician inexperience with removing cerumen and performingpneumatic otoscopy, diagnostic equipment may be suboptimal and the child being evaluated may not always cooperate in theprocess.2

19/10/2015
http://contemporarypediatrics.modernmedicine.com/contemporary-pediatrics/news/acute-otitis-media-update-2015?page=full 3/6
In those cases in which uncertainty occurs, if the child is not in pain and does not have a fever in excess of 102.2°F, thenobservation becomes an option.2 Utilizing observation as initial management in these instances requires the elements of easyfollow-up and continuity of care. Absent either of those elements, the observation option is not advisable.
NEXT: What's the course of antibiotic treatment?
Empiric antibiotic treatment
The 2013 AAP guideline recommends high-dose amoxicillin (80-90 mg/kg/day in 2 divided doses) for 5 to 10 days as thetreatment of first choice in most patients.2 Recommended optimal duration of therapy for children aged younger than 2 years andfor those who have severe symptoms is a standard 10-day course; for children aged 2 to 5 years with mild or moderate AOM, a7-day course appears adequate; and for those aged 6 years and older with mild or moderate AOM, a 5- to 7-day course iseffective. The selection of high-dose amoxicillin has been made on the basis of long-term safety of the drug; a first intention-to-treat penicillin-resistant Streptococcus pneumoniae because that organism can cause the most morbidity; and the recognition thatoverdiagnosis of AOM is commonplace. This recommendation is unchanged from the 2004 guideline.1,2
An alternative recommended first-line treatment is amoxicillin-clavulanate (90 mg/kg/day amoxicillin and 6.4 mg/kg/dayclavulanate in 2 divided doses). This alternative treatment is recommended in patients who have been given amoxicillin in theprevious 30 days or in those who have otitis-conjunctivitis syndrome (Table 2).2
More: Child with fever after foreign travel
We have been tracking the etiology of AOM by performing tympanocentesis in our practice since 1996, before the introductionof 7-valent pneumococcal conjugate vaccine (PCV7). As a consequence of PCV7, and more recently PCV13 (substituted April2010), the etiology of AOM has changed over time.8 Our data suggest that empiric amoxicillin treatment of AOM would beeffective in eradication of about one-third of the current mix of otopathogens, because of the predominance of Haemophilusinfluenzae and Moraxella catarrhalis and their resistance to amoxicillin (Table 3).9 The diminished presence of S pneumoniaeunder vaccine-induced selection pressure may change over time, but in 2015 our data indicate that amoxicillin/clavulanate or asecond- or third-generation cephalosporin with beta-lactamase stability should be the preferred treatment of AOM.
There are no other data describing the otopathogen mix and antibiotic susceptibilities because our center currently is the only onein the United States routinely performing tympanocentesis with bacterial cultures of middle ear fluid. Two recent seminal studiesthat compared antibiotic to placebo and concluded that antibiotics were of significant benefit in hastening resolution of infectionboth used amoxicillin/clavulanate as the treatment choice.10,11 A third more recent study showed that antimicrobial treatment ofAOM significantly hastened the disappearance of middle ear effusion in a placebo-controlled trial.12
The oral cephalosporins of choice for treatment of AOM as designated by the AAP guideline are cefdinir, cefuroxime axetil, andcefpodoxime proxetil.2 Among these choices, cefdinir has emerged as the most frequently used in the United States largelybecause of its taste advantage. Cefdinir can be dosed once or divided twice daily (14 mg/kg/day). The duration of treatment withcefdinir can be 5 days with twice-daily dosing or 10 days with once-daily dosing.
We recently published a head-to-head comparison of amoxicillin/clavulanate 80 mg/kg/day divided twice daily for 10 daysversus cefdinir 14 mg/kg/day divided twice daily for 5 days. Amoxicillin/clavulanate demonstrated superior efficacy (86.5% vs71%, respectively; P=.001).13 Outside the context of a clinical trial, however, the adherence characteristics favor cefdinir (bettertaste and fewer diarrhea episodes). The taste of cefuroxime and cefpodoxime can be masked with chocolate syrup, but theaddition of flavorings at the pharmacy or at home should not be advised because these antibiotics have been shown to precipitatechanges in pH and chemical reactions between the active drug and the flavoring ingredients.9
Ceftriaxone by injection (50 mg/kg/dose) is effective as a single injection against all penicillin-susceptible S pneumoniae andagainst beta-lactamase-producing H influenzae and M catarrhalis. Killing of penicillin-resistant S pneumoniae causing AOM hasbeen proven to require 3 doses of ceftriaxone for 3 days.14 The sequential doses can be spaced every other day or even everythird day if weekends or holidays dictate an alternative regimen.
NEXT: Treating the otitis-prone child
Otitis-prone child
Some children experience repeated AOM episodes and reach a threshold where they are termed “otitis prone.” The definition ofotitis prone has varied among investigators in the field. However, the most frequently used definition currently is 3 episodes ofAOM within 6 months or 4 episodes within 1 year’s time. Children with recurrent AOM are generally treated with broader-spectrum antibiotics as additional cases of infection occur. We have recently shown that repeated antibiotic treatment does notchange the mix of otopathogens causing AOM, but it significantly increases the proportion of strains that display amoxicillinresistance.15
In recent years, we have been studying the immune response to AOM to explain susceptibility to an increased frequency ofAOM in otitis-prone children. We have discovered that the child who experiences frequent AOM has an immature immunesystem, resembling a neonate.16-20 After an AOM, the immune system of the otitis-prone child fails to generate an immunememory response. Therefore, the child remains susceptible to another AOM following antibiotic treatment, even by the sameotopathogen residing in the nasopharynx that caused a preceding AOM.

19/10/2015
http://contemporarypediatrics.modernmedicine.com/contemporary-pediatrics/news/acute-otitis-media-update-2015?page=full 4/6
More guidelines: Diagnosing and managingbronchiolitis
Biofilms
When children have recurrent AOM ordevelop chronic OME (>3 months’ duration),there is now ample evidence to suggest thatthe otopathogens form biofilms.21,22 Bacteriain biofilms cover themselves with a shield ofa plastic-like material that prevents thepenetration of antibiotics and antibodies. Mostclinicians are familiar with biofilms asbacteria that grow on implanted catheters.When bacteria are in biofilms, they do notelicit much of an immune response andtherefore their presence is not apparentclinically.
We have recently shown that biofilmsinvolving H influenzae require low oxygenconditions such as occur during chronic OMEor recurrent AOM, but they do not form atnormal oxygen concentrations.23 This newobservation provides a new explanation as towhy tympanocentesis and tympanostomytubes provide therapeutic benefit.
Conclusion
The diagnosis of AOM should not be madeunless the TM is full/bulging. Usingpneumatic otoscopy, tympanometry, and/orSGAR should improve diagnostic accuracy.When the diagnosis of AOM is uncertain, thecurrent AAP guideline proposes observationas an option and amoxicillin as empiric first-line treatment. The evidence does not supportamoxicillin as the best treatment when theresults of cultures of middle ear fluid taken inrecent years are considered.Amoxicillin/clavulanate or a recommended
cephalosporin should provide better efficacy. The biologicand immunologic basis of the otitis-prone condition points tonew areas for research and alternative treatments.
REFERENCES
1. American Academy of Pediatrics Subcommittee onManagement of Acute Otitis Media. Diagnosis andmanagement of acute otitis media. Pediatrics.2004;113(5):1451-1465.
2. Lieberthal AS, Carroll AE, Chonmaitree T, et al. Thediagnosis and management of acute otitis media. Pediatrics.2013;131(3):e964-e999.
3. Shaikh N, Hoberman A, Kaleida PH, et al. Otoscopic signsof otitis media. Pediatr Infect Dis J. 2011;30(10):822-826.
4. Rothman R, Owens T, Simel DL. Does this child haveacute otitis media? JAMA. 2003;290(12):1633-1640.
5. Welch Allyn Inc. Welch Allyn MicroTymp 2 Portable

19/10/2015
http://contemporarypediatrics.modernmedicine.com/contemporary-pediatrics/news/acute-otitis-media-update-2015?page=full 5/6
Tympanometric Instrument. User manual. Available at:
http://intl.welchallyn.com/documents/EENT/Tympanometric%20Systems/MicroTymp%202/servicemanual_20070320_microtympII.pdf.Accessed February 6, 2015.
6. Puhakka T, Pulkkinen J, Silvennoinen H, Heikkinen T. Comparison of spectral gradient acoustic reflectometry andtympanometry for detection of middle-ear effusion in children. Pediatr Infect Dis J. 2014;33(8):e183-e186.
7. Revai K, Dobbs LA, Nair S, Patel JA, Grady JJ, Chonmaitree T. Incidence of acute otitis media and sinusitis complicatingupper respiratory tract infection: the effect of age. Pediatrics. 2007;119(6):e1408-e1412.
8. Xu Q, Casey JR, Chang A, Pichichero ME. When co-colonizing the nasopharynx Haemophilus influenzae predominates overStreptococcus pneumoniae except serotype 19A strains to cause acute otitis media. Pediatr Infect Dis J. 2012;31(6):638-640.
9. Pichichero ME. Otitis media. Pediatr Clin North Am. 2013;60(2):391-407.
10. Hoberman A, Paradise JL, Rockette HE, et al. Treatment of acute otitis media in children under 2 years of age. N Engl JMed. 2011;364(2):105-115.
11. Tähtinen PA, Laine MK, Huovinen P, Jalava J, Ruuskanen O, Ruohola A. A placebo-controlled trial of antimicrobialtreatment for acute otitis media. N Engl J Med. 2011;364(2):116-126.

19/10/2015
http://contemporarypediatrics.modernmedicine.com/contemporary-pediatrics/news/acute-otitis-media-update-2015?page=full 6/6
12. Tapiainen T, Kujala T, Renko M, et al. Effect of antimicrobial treatment of acute otitis media on the daily disappearance ofmiddle ear effusion: a placebo-controlled trial. JAMA Pediatr. 2014;168(7):635-641.
13. Casey JR, Block SL, Hedrick J, Almudevar A, Pichichero ME. Comparison of amoxicillin/clavulanic acid high dose withcefdinir in the treatment of acute otitis media. Drugs. 2012;72(15):1991-1997.
14. Gahanno P, Nguyen L, Barry B, et al. Eradication by ceftriaxone of Streptococcus pneumoniae isolates with increasedresistance to penicillin in cases of acute otitis media. Antimicrob Agents Chemother. 1999;43(1):16-20.
15. Casey JR, Kaur R, Friedel VC, Pichichero ME. Acute otitis media otopathogens during 2008 to 2010 in Rochester, NewYork. Pediatr Infect Dis J. 2013;32(8):805-809.
16. Kaur R, Casey JR, Pichichero ME. Serum antibody response to three non-typeable Haemophilus influenzae outer membraneproteins during acute otitis media and nasopharyngeal colonization in otitis prone and non-otitis prone children. Vaccine.2011;29(5):1023-1028.
17. Kaur R, Casey JR, Pichichero ME. Serum antibody response to five Streptococcus pneumoniae proteins during acute otitismedia in otitis-prone and non-otitis-prone children. Pediatr Infect Dis J. 2011;30(8):645-650.
18. Sharma SK, Casey JR, Pichichero ME. Reduced memory CD4+ T-cell generation in the circulation of young children maycontribute to the otitis-prone condition. J Infect Dis. 2011;204(4):645-653.
19. Sharma SK, Casey JR, Pichichero ME. Reduced serum IgG responses to pneumococcal antigens in otitis-prone children maybe due to poor memory B-cell generation. J Infect Dis. 2012;205(8):1225-1229.
20. Sharma SK, Pichichero ME. Cellular immune response in young children accounts for recurrent acute otitis media. CurrAllergy Asthma Rep. 2013;13(5):495-500.
21. Post JC. Direct evidence of bacterial biofilms in otitis media. Laryngoscope. 2001;111(12):2083-2094.
22. Torretta S, Marchisio P, Drago L, et al. Nasopharyngeal biofilm-producing otopathogens in children with nonsevererecurrent acute otitis media. Otolaryngol Head Neck Surg. 2012;146(6);991-996.
23. Osgood R, Salamone F, Diaz A, et al. Effect of pH and oxygen on biofilm formation in acute otitis media associated NTHiclinical isolates. Laryngoscope. 2015; in press.
Dr Casey is a partner and co-director of research, Legacy Pediatrics, Rochester, New York, and clinical associate professor ofpediatrics, University of Rochester. She has nothing to disclose in regard to affiliations with or financial interests in anyorganizations that may have an interest in any part of this article. Dr Pichichero, also at Legacy Pediatrics, Rochester, is director,Center for Infectious Diseases and Immunology, Rochester General Hospital Research Institute, and research professor, HealthSciences and Technology, Rochester Institute of Technology, New York. He discloses that he is a limited partner in a businessentity that provided a loan to Innovia Medical LLC to make technical improvements in a spectral gradient acoustic reflectometer(SGAR) device.
Subscribe to Contemporary Pedatrics to get more like this.