Embed Size (px)
Citation preview

8/9/2019 PJP Pneumonia
http://slidepdf.com/reader/full/pjp-pneumonia 1/7
O R I G I N A L A R T I C L E
Analysis of clinical features of non-HIV Pneumocystis jirovecii
pneumonia
Yusuke Ainoda • Yuji Hirai • Takahiro Fujita •
Noriko Isoda • Kyoichi Totsuka
Received: 2 December 2011/ Accepted: 11 March 2012/ Published online: 30 March 2012
Japanese Society of Chemotherapy and The Japanese Association for Infectious Diseases 2012
Abstract Pneumocystis jirovecii pneumonia (PCP) is
classified as PCP with human immunodeficiency virus(HIV) and non-HIV PCP, and the two forms differ in
progression and prognosis. Although early treatment is
necessary, the diagnosis of non-HIV PCP is often difficult
because of the underlying diseases. However, the outcome
with treatment delay remains unclear because there are no
concrete data indicating a worsened clinical situation or
increased complications related to delayed therapy initia-
tion. We retrospectively examined patients with non-HIV
PCP admitted to Tokyo Women’s Medical University
Hospital from November 2008 to October 2010. The
relationship between intubation with mechanical ventila-
tion (within 1 week after starting treatment) and treatment
delay was investigated. Treatment delay was defined as the
period, in days, from onset to therapy initiation. In total, 24
confirmed non-HIV PCP cases were included. Median
treatment delay was 7 ± 4.83 days (1–20 days). Twelve of
24 cases (50 %) were intubated, and 11 (45.8 %) died of
their underlying diseases within 90 days. Treatment delay
was more than 7 days in the intubation group, but was
within 7 days in 9 of 12 nonintubation cases. The differ-
ence in treatment delay was significant ( p = 0.0071)
between the intubation and nonintubation groups, but there
were no significant differences in survival rate at 90 daysor other findings. We conclude that starting treatment
within 7 days after onset is important because intubation
and mechanical ventilation may be avoided in many cases.
Keywords Non-HIV Pneumocystis jirovecii pneumonia
(non-HIV PCP) Treatment delay Intubation Mortality
Introduction
Pneumocystis jirovecii (P. jirovecii) pneumonia (PCP), a
pulmonary infection caused by P. jirovecii, is among the
opportunistic infections associated with cellular immuno-
deficiency [1–3]. P. jirovecii infections usually occur in
childhood, but PCP does not develop in the absence of
cellular immunodeficiency [4, 5]. PCP is classified as PCP
with HIV and non-HIV PCP, and the two forms differ in
progression and prognosis [6–9]. PCP with HIV shows
relatively slow progression, and mortality is well below
10 %, but non-HIV PCP is rapidly progressive and severe,
and expedited treatment initiation is recognized as being
essential [1]. Despite the necessity of early treatment, the
diagnosis of non-HIV PCP is often difficult because of the
underlying disease [10]. However, the outcome of treat-
ment delay remains unclear because concrete data and
reports indicating a worsened clinical situation or an
increase in complications, based on how long therapy ini-
tiation is delayed, are lacking. A reliable means of
assessing the likelihood of intubation and mortality at the
initiation of non-HIV PCP therapy, based on the period
from onset until the therapy initiation, would allow deter-
mination of when and if to start intensive care without
delay and could be expected to improve both the
Y. Ainoda (&)
Y. Hirai
T. Fujita
K. TotsukaDepartment of Infectious Disease, Tokyo Women’s Medical
University, 8-1 Kawada-cho, Shinjuku-ku,
Tokyo 162-8666, Japan
e-mail: [email protected]
Y. Hirai K. Totsuka
Department of Hematology, Tokyo Women’s Medical
University, Tokyo, Japan
N. Isoda
Department of Laboratory, Tokyo Women’s Medical University
Hospital, Tokyo, Japan
1 3
J Infect Chemother (2012) 18:722–728
DOI 10.1007/s10156-012-0408-5

8/9/2019 PJP Pneumonia
http://slidepdf.com/reader/full/pjp-pneumonia 2/7
management and the prognosis of PCP patients [11–13].
Thus, we analyzed non-HIV PCP retrospectively and
especially investigated the relationship between the time
from onset until therapy initiation (treatment delay) and the
severity of non-HIV PCP.
Patients and methods
Patients
We retrospectively examined patients with non-HIV PCP
admitted to Tokyo Women’s Medical University Hospital
(a 1,423-bed facility) from November 2008 to October
2010 using the laboratory results database. The relationship
between intubation with mechanical ventilation and treat-
ment delay was investigated. Data regarding physical and
laboratory findings at treatment initiation were also studied.
In addition, we examined the relationships of mortality
within 90 days to treatment delay, intubation, and otherparameters [white blood cell count (WBC), C-reactive
protein (CRP), lactate dehydrogenase (LDH), and
(1 ? 3)b-D-glucan levels]. This study was approved by the
Ethics Committee of Tokyo Women’s Medical University.
Because informed consent had not been obtained, the
information obtained in this study was published during the
investigative period according to the guidelines of the
Ministry of Health, Labour and Welfare of Japan.
Definition of treatment delay
Treatment delay was defined as the period, in days, from
onset until therapy initiation. The date of non-HIV PCP
onset was defined as the first day that fever ([37.0 C),
dyspnea, or other findings associated with PCP were noted
in medical records by an infectious disease specialist [1, 2].
Inclusion criteria
Non-HIV PCP was defined according to the following five
criteria (with reference to a previous report) [14]: (1)
background of cellular immunodeficiency (without HIV),
(2) hypoxemia, (3) abnormality on chest images [X-ray or
computed tomography (CT)], (4) positive by polymerase
chain reaction (PCR) or fluorescent antibody staining, (5)
positive for (1 ? 3)b-D-glucan (Table 1). Hypoxemia was
defined as PaO2 of less than 70 torr and/or SpO2 less than
94 % on room air. Abnormalities on chest images were
determined by radiologists using either chest X-rays or
chest plain CT [15, 16]. In our institution, all suspected
PCP cases were tested for P. jirovecii by PCR or fluores-
cent antibody staining of specimens from the respiratory
tract (sputum or bronchoalveolar lavage) and were
included if either test was positive [17, 18]. A Fungi-Fluor
Kit Pneumocystis Kit (Polysciences Inc.) was used for
fluorescent antibody staining, and results were checked by
a trained laboratory technician. (1 ? 3)b-D-glucan was
examined using FangitecG MK (Seikagaku Corp.), and the
cutoff was 20 pg/ml, a value set by our institution’s labo-
ratory department [19, 20]. Cases not meeting even one of
these five criteria and with a treatment period of less than1 week were excluded. The need for intubation was judged
by intensive care specialists.
Statistical analysis
For the statistical analysis, continuous data were compared
using Welch’s t test or Student’s t test, and noncontinuous
dichotomous data were compared employing Fisher’s exact
test, as appropriate. All p values were two sided, and sta-
tistical significance was accepted for p\ 0.05. To assess
mortality, survival curves were devised by the Kaplan–
Meier method, using the log-rank test. We also evaluate thesensitivity and specificity of treatment delay for predicting
intubation.
Results
Patients and backgrounds
In total, 25 confirmed cases of non-HIV PCP met the
inclusion criteria. However, 1 case was excluded because
the treatment duration was less than 1 week. Thus, 24 cases
were ultimately included.
The median age was 66.5 ± 18.62 years old, and male to
female ratio was 10:14. None received chemoprophylaxis.
Nine of the 24 patients (37.5 %) had rheumatoid arthritis
(RA), 5 (20.8 %) had undergone kidney transplantation
(UKT), and the remaining patients were immunocompro-
mised by other diseases [malignant lymphoma (ML), inter-
stitial pneumonia(IP), renal cellcarcinoma (RCC), ulcerative
colitis (UC), membranoproliferative glomerulonephritis
(MPGN), and hemodialysis (HD)] (Table 1).
All RA patients were treated with methotrexate
(6 mg ± 3.01 mg/week, but there was no description of dose
for two patients), and seven were treated with prednisolone
(6 mg ± 2.52 mg/day). The UKT patients had been treated
with mycophenolate mofetil (750 ± 391.66 mg/day),
methylprednisolone (6 ± 2.33 mg/day), and tacrolimus
hydrate (3.5 ± 0.83 mg/day) or cyclosporine (75 mg). The
duration from renal transplantation to the onset of PCP was
58 ± 23.93 months. One of the ML patients was treated with
rituximab (375 mg/m2, on the first day of chemotherapy) and
prednisolone (45 mg/day from the first day of chemotherapy
to day 5), and PCP developed after the first chemotherapy
J Infect Chemother (2012) 18:722–728 723
1 3
8/9/2019 PJP Pneumonia
http://slidepdf.com/reader/full/pjp-pneumonia 3/7
course. The otherwas treated with prednisolone (20 mg/day).
The MPGN patient was treated with prednisolone (15 mg/ day). The UC patient was treated with prednisolone (25 mg/
day) and azathioprine (50 mg/day). The IP patient was trea-
ted with prednisolone (11 mg/day) and azathioprine (50 mg/
day). The RCC patient was treated with betamethasone
(2 mg/day). In HD patients only, the duration of HD was
26 years and in those receiving HD combined with prednis-
olone (5 mg/day) 12 years and 3 months.
As for initial symptoms, fever was noted in 13 patients
(54.2 %), followed by dyspnea in 7 (29.2 %). The median
treatment delay was 7 ± 4.83 days (1–20 days). The median
WBCcountwas 6,900 ± 3,672.18/ ll,CRP8.44 ± 4.52 mg/dl,
LDH 429 ± 209.48 IU/l (reference range for LDH, 119–229),and median (1? 3)b-D-glucan was 89.3 ± 2,110.77 pg/ml
(Table 1).
Treatment and mortality
In treating PCP, 21 of the 24 patients were started on SMX/
TMP at a dose of approximately 15 mg/kg/day of tri-
methoprim (SMX/TMP was reduced by half if the patient’s
creatinine clearance was below 50 ml/min). Three patients
were started with lower doses of SMX/TMP. Eleven of the
24 patients were started on combinations with prednisoloneat doses of 80 mg/day (or 1 mg/kg/day) and decreased
gradually later. Ten patients were started with a methyl-
prednisolone pulse (250–1,000 mg/day), and 3 were started
with low-dose prednisolone or dexamethasone. Treatment
was started when the definition of PCP was met or PCP was
strongly suspected. Ten of 24 patients (41.7 %) started
therapy within 24 h after consultation. The median treat-
ment period was 21 ± 5.14 days. Four of 24 patients
(16.7 %) died of their underlying diseases within 30 days
and 11 (45.8 %) within 90 days (Table 1).
Correlations of intubation with treatment delayand mortality
The intubation group was composed of 12 patients (50 %).
Three of the 12 had RA, 3 had UKT, 2 had ML, and the
others IP, RCC, ULT, and MPGN. The treatment delays in
the intubation group were 7–20 days (median, 9 ± 4.08
days). The remaining 12 patients (50 %) constituted the
nonintubation group. Six of the 12 had RA, 2 had UKT,
2 had HD with PSL, and the others UC and HD only.
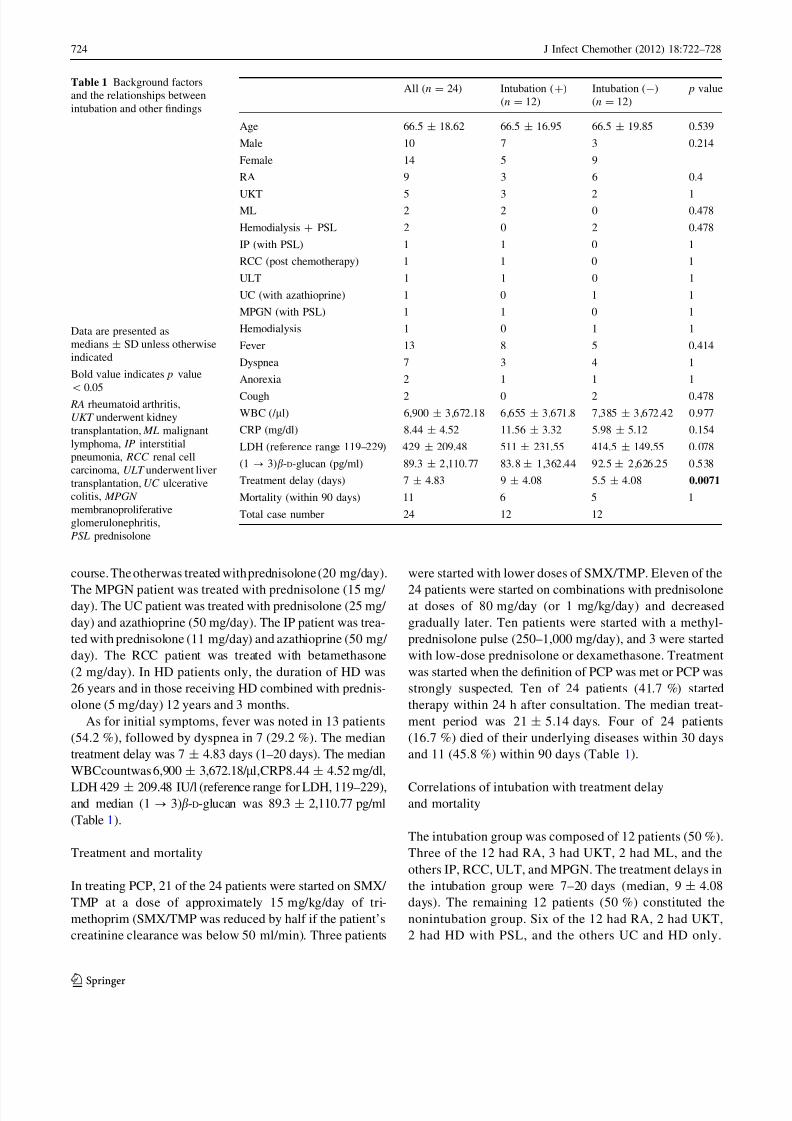
Table 1 Background factors
and the relationships between
intubation and other findings
Data are presented as
medians ± SD unless otherwise
indicated
Bold value indicates p value
\
0.05 RA rheumatoid arthritis,
UKT underwent kidney
transplantation, ML malignant
lymphoma, IP interstitial
pneumonia, RCC renal cell
carcinoma, ULT underwent liver
transplantation, UC ulcerative
colitis, MPGN
membranoproliferative
glomerulonephritis,
PSL prednisolone
All (n = 24) Intubation (?)
(n = 12)
Intubation (-)
(n = 12)
p value
Age 66.5 ± 18.62 66.5 ± 16.95 66.5 ± 19.85 0.539
Male 10 7 3 0.214
Female 14 5 9
RA 9 3 6 0.4
UKT 5 3 2 1ML 2 2 0 0.478
Hemodialysis ? PSL 2 0 2 0.478
IP (with PSL) 1 1 0 1
RCC (post chemotherapy) 1 1 0 1
ULT 1 1 0 1
UC (with azathioprine) 1 0 1 1
MPGN (with PSL) 1 1 0 1
Hemodialysis 1 0 1 1
Fever 13 8 5 0.414
Dyspnea 7 3 4 1
Anorexia 2 1 1 1
Cough 2 0 2 0.478
WBC (/ ll) 6,900 ± 3,672.18 6,655 ± 3,671.8 7,385 ± 3,672.42 0.977
CRP (mg/dl) 8.44 ± 4.52 11.56 ± 3.32 5.98 ± 5.12 0.154
LDH (reference range 119–229) 429 ± 209.48 511 ± 231.55 414.5 ± 149.55 0.078
(1 ? 3)b-D-glucan (pg/ml) 89.3 ± 2,110.77 83.8 ± 1,362.44 92.5 ± 2,626.25 0.538
Treatment delay (days) 7 ± 4.83 9 ± 4.08 5.5 ± 4.08 0.0071
Mortality (within 90 days) 11 6 5 1
Total case number 24 12 12
724 J Infect Chemother (2012) 18:722–728
1 3
8/9/2019 PJP Pneumonia
http://slidepdf.com/reader/full/pjp-pneumonia 4/7
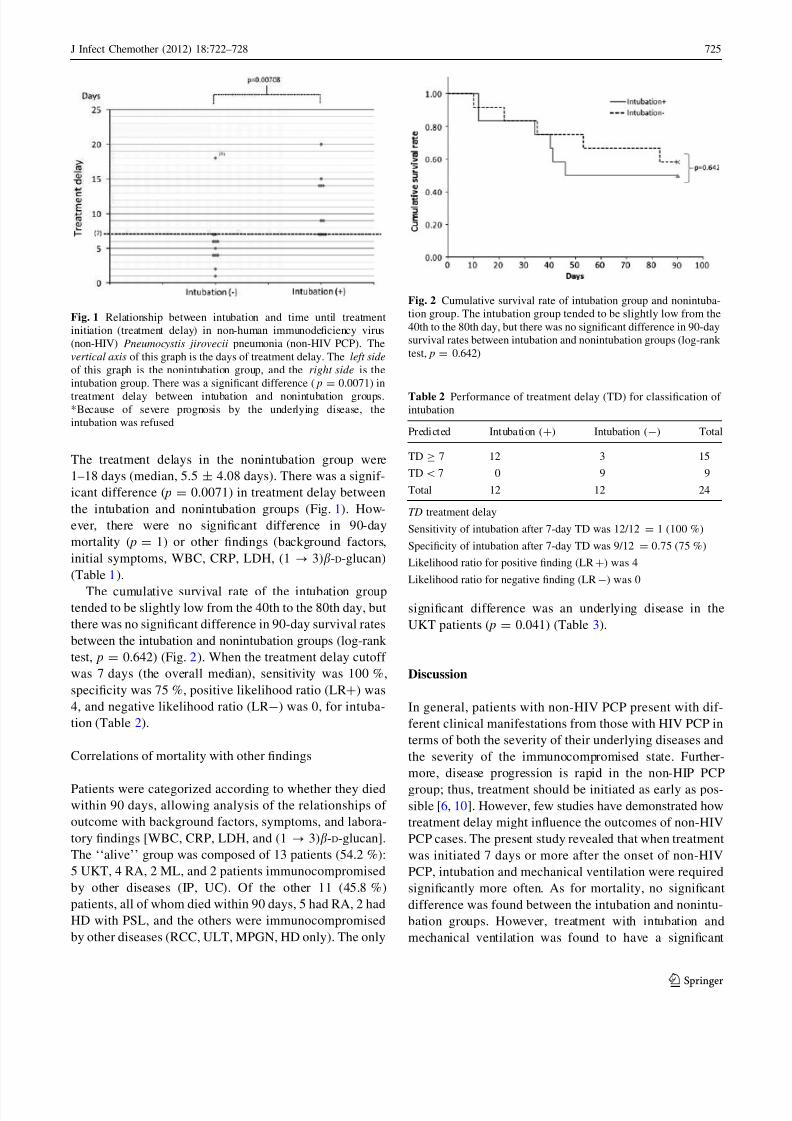
The treatment delays in the nonintubation group were
1–18 days (median, 5.5 ± 4.08 days). There was a signif-
icant difference ( p = 0.0071) in treatment delay between
the intubation and nonintubation groups (Fig. 1). How-
ever, there were no significant difference in 90-day
mortality ( p = 1) or other findings (background factors,
initial symptoms, WBC, CRP, LDH, (1 ? 3)b-D-glucan)
(Table 1).
The cumulative survival rate of the intubation grouptended to be slightly low from the 40th to the 80th day, but
there was no significant difference in 90-day survival rates
between the intubation and nonintubation groups (log-rank
test, p = 0.642) (Fig. 2). When the treatment delay cutoff
was 7 days (the overall median), sensitivity was 100 %,
specificity was 75 %, positive likelihood ratio (LR?) was
4, and negative likelihood ratio (LR-) was 0, for intuba-
tion (Table 2).
Correlations of mortality with other findings
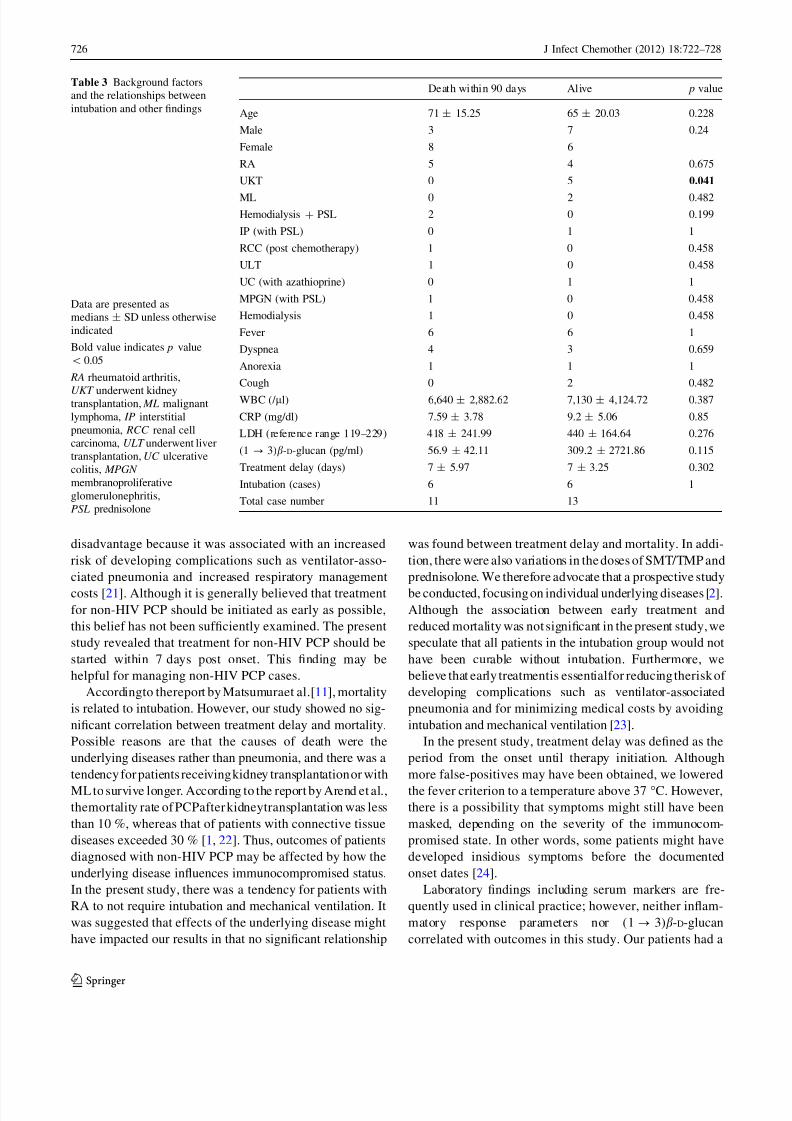
Patients were categorized according to whether they diedwithin 90 days, allowing analysis of the relationships of
outcome with background factors, symptoms, and labora-
tory findings [WBC, CRP, LDH, and (1 ? 3)b-D-glucan].
The ‘‘alive’’ group was composed of 13 patients (54.2 %):
5 UKT, 4 RA, 2 ML, and 2 patients immunocompromised
by other diseases (IP, UC). Of the other 11 (45.8 %)
patients, all of whom died within 90 days, 5 had RA, 2 had
HD with PSL, and the others were immunocompromised
by other diseases (RCC, ULT, MPGN, HD only). The only
significant difference was an underlying disease in the
UKT patients ( p = 0.041) (Table 3).
Discussion
In general, patients with non-HIV PCP present with dif-
ferent clinical manifestations from those with HIV PCP in
terms of both the severity of their underlying diseases and
the severity of the immunocompromised state. Further-
more, disease progression is rapid in the non-HIP PCP
group; thus, treatment should be initiated as early as pos-
sible [6, 10]. However, few studies have demonstrated how
treatment delay might influence the outcomes of non-HIV
PCP cases. The present study revealed that when treatment
was initiated 7 days or more after the onset of non-HIV
PCP, intubation and mechanical ventilation were required
significantly more often. As for mortality, no significant
difference was found between the intubation and nonintu-
bation groups. However, treatment with intubation and
mechanical ventilation was found to have a significant
Fig. 1 Relationship between intubation and time until treatment
initiation (treatment delay) in non-human immunodeficiency virus
(non-HIV) Pneumocystis jirovecii pneumonia (non-HIV PCP). The
vertical axis of this graph is the days of treatment delay. The left side
of this graph is the nonintubation group, and the right side is the
intubation group. There was a significant difference ( p = 0.0071) in
treatment delay between intubation and nonintubation groups.*Because of severe prognosis by the underlying disease, the
intubation was refused
Fig. 2 Cumulative survival rate of intubation group and nonintuba-
tion group. The intubation group tended to be slightly low from the
40th to the 80th day, but there was no significant difference in 90-day
survival rates between intubation and nonintubation groups (log-rank
test, p = 0.642)
Table 2 Performance of treatment delay (TD) for classification of intubation
Predicted Intubation (?) Intubation (-) Total
TD C 7 12 3 15
TD\7 0 9 9
Total 12 12 24
TD treatment delay
Sensitivity of intubation after 7-day TD was 12/12 = 1 (100 %)
Specificity of intubation after 7-day TD was 9/12 = 0.75 (75 %)
Likelihood ratio for positive finding (LR?) was 4
Likelihood ratio for negative finding (LR-) was 0
J Infect Chemother (2012) 18:722–728 725
1 3
8/9/2019 PJP Pneumonia
http://slidepdf.com/reader/full/pjp-pneumonia 5/7
disadvantage because it was associated with an increased
risk of developing complications such as ventilator-asso-
ciated pneumonia and increased respiratory management
costs [21]. Although it is generally believed that treatment
for non-HIV PCP should be initiated as early as possible,
this belief has not been sufficiently examined. The present
study revealed that treatment for non-HIV PCP should be
started within 7 days post onset. This finding may be
helpful for managing non-HIV PCP cases.
Accordingto thereport by Matsumuraet al.[11], mortality
is related to intubation. However, our study showed no sig-
nificant correlation between treatment delay and mortality.
Possible reasons are that the causes of death were the
underlying diseases rather than pneumonia, and there was a
tendency for patients receiving kidney transplantation or with
ML to survive longer. According to the report by Arend et al.,
themortality rate of PCPafter kidneytransplantation was less
than 10 %, whereas that of patients with connective tissue
diseases exceeded 30 % [1, 22]. Thus, outcomes of patients
diagnosed with non-HIV PCP may be affected by how the
underlying disease influences immunocompromised status.
In the present study, there was a tendency for patients with
RA to not require intubation and mechanical ventilation. It
was suggested that effects of the underlying disease might
have impacted our results in that no significant relationship
was found between treatment delay and mortality. In addi-
tion, there were also variations in the doses of SMT/TMP and
prednisolone. We therefore advocate that a prospective study
be conducted, focusing on individual underlying diseases [2].
Although the association between early treatment and
reduced mortality was not significant in the present study, we
speculate that all patients in the intubation group would not
have been curable without intubation. Furthermore, we
believe that early treatmentis essentialfor reducing therisk of
developing complications such as ventilator-associated
pneumonia and for minimizing medical costs by avoiding
intubation and mechanical ventilation [23].
In the present study, treatment delay was defined as the
period from the onset until therapy initiation. Although
more false-positives may have been obtained, we lowered
the fever criterion to a temperature above 37 C. However,
there is a possibility that symptoms might still have been
masked, depending on the severity of the immunocom-
promised state. In other words, some patients might have
developed insidious symptoms before the documented
onset dates [24].
Laboratory findings including serum markers are fre-
quently used in clinical practice; however, neither inflam-
matory response parameters nor (1? 3)b-D-glucan
correlated with outcomes in this study. Our patients had a
Table 3 Background factors
and the relationships between
intubation and other findings
Data are presented as
medians ± SD unless otherwise
indicated
Bold value indicates p value
\ 0.05
RA rheumatoid arthritis,
UKT underwent kidneytransplantation, ML malignant
lymphoma, IP interstitial
pneumonia, RCC renal cell
carcinoma, ULT underwent liver
transplantation, UC ulcerative
colitis, MPGN
membranoproliferative
glomerulonephritis,
PSL prednisolone
Death within 90 days Alive p value
Age 71 ± 15.25 65 ± 20.03 0.228
Male 3 7 0.24
Female 8 6
RA 5 4 0.675
UKT 0 5 0.041
ML 0 2 0.482
Hemodialysis ? PSL 2 0 0.199
IP (with PSL) 0 1 1
RCC (post chemotherapy) 1 0 0.458
ULT 1 0 0.458
UC (with azathioprine) 0 1 1
MPGN (with PSL) 1 0 0.458
Hemodialysis 1 0 0.458
Fever 6 6 1
Dyspnea 4 3 0.659
Anorexia 1 1 1
Cough 0 2 0.482
WBC (/ ll) 6,640 ± 2,882.62 7,130 ± 4,124.72 0.387
CRP (mg/dl) 7.59 ± 3.78 9.2 ± 5.06 0.85
LDH (reference range 119–229) 418 ± 241.99 440 ± 164.64 0.276
(1 ? 3)b-D-glucan (pg/ml) 56.9 ± 42.11 309.2 ± 2721.86 0.115
Treatment delay (days) 7 ± 5.97 7 ± 3.25 0.302
Intubation (cases) 6 6 1
Total case number 11 13
726 J Infect Chemother (2012) 18:722–728
1 3

8/9/2019 PJP Pneumonia
http://slidepdf.com/reader/full/pjp-pneumonia 6/7
variety of backgrounds, and these differences might have
influenced the results. At a minimum, the magnitude of the
inflammatory response may not be a useful indicator of
prognosis in PCP patients. Although (1 ? 3)b-D-glucan is
reportedly useful for clinically diagnosing PCP, in contrast to
past studies, we did not identify a significant relationship
between the(1 ? 3)b-D-glucan value andoutcomes [19, 25].
The inclusion criteria applied herein were establishedbased on previous domestic reports, because internationally
standardized diagnostic criteria for PCP are lacking [8]. We
employed a strict inclusion strategy, i.e., the subjects had to
meet all five criteria. These strict criteria may have limited
the detection of patients with mild symptoms. Inclusion of
patients with mild PCP might have yielded different
results. Further studies are needed to clarify this issue.
In the present study, not all our patients received
prophylaxis. The efficacy of chemoprophylaxis against
non-HIV PCP is still unclear. However, there are reports
indicating that prophylaxis reduces the incidence of PCP
[26]. With greater immunosuppression, or in the situationof an outbreak with human-to-human transmission, it may
be necessary to consider more prophylaxis [27–31].
Although the present study has the aforementioned
limitation, patients with non-HIV PCP appear to be likely
to develop respiratory failure requiring intubation and
mechanical ventilation if they do not receive treatment
within 7 days after the onset. Therefore, we consider early
diagnosis and treatment to be essential for patients with
non-HIV PCP. Furthermore, it is also important that we
consider PCP in the differential diagnosis, and that we
educate patients with immunocompromised status to con-
sult a hospital promptly if symptoms manifest that suggest
PCP. We especially emphasize the importance of starting
treatment within 7 days after symptom onset. Achieving
this goal may allow many patients to avoid intubation and
mechanical ventilation.
Acknowledgments The authors thank the laboratory department staff
and directors of Tokyo Women’s Medical University Hospital. We
express our deep appreciation to Makoto Kawashima (Department of
Laboratory), Toru Kotani (Department of Intensive Care Unit), Hisashi
Yamanaka (Department of Rheumatology), Satoshi Teraoka (Depart-
ment of Surgical Nephrology), Toshiko Motoji (Department of Hema-
tology), Keiko Tatemoto (Department of Gastroenterology), Kosaku
Nitta (Department of Nephrology), Atsushi Nagai (Department of Pulmonology), and Nobuhisa Hagiwara (Department of Cardiology) of
Tokyo Women’s Medical University Hospital.
Conflict of interest None.
References
1. Sepkowitz KA. Opportunistic infections in patients with and
patients without acquired immunodeficiency syndrome. Clin
Infect Dis. 2002;34:1098–107.
2. Yale SH, Limper AH. Pneumocystis carinii pneumonia in
patients without acquired immunodeficiency syndrome: associ-
ated illness and prior corticosteroid therapy. Mayo Clin Proc.
1996;71:5–13.
3. Wang J, Wright TW, Gigliotti F. Immune modulation as
adjunctive therapy for Pneumocystis pneumonia. Interdiscipl
Perspect Infect Dis. 2011;. doi:10.1155/2011/918038.
4. Morris A, Wei K, Afshar K, Huang L. Epidemiology and clinical
significance of Pneumocystis colonization. J Infect Dis. 2008;197:
10–7.
5. Thomas CF Jr, Limper AH. Pneumocystis pneumonia. N Engl J
Med. 2004;350:2487–98.
6. Mansharamani NG, Garland R, Delaney D, Koziel H. Manage-
ment and outcome patterns for adult Pneumocystis carinii
pneumonia, 1985 to 1995: comparison of HIV-associated cases to
other immunocompromised states. Chest. 2000;118:704–11.
7. Enomoto T, Azuma A, Kohno A, Kaneko K, Saito H, Kametaka
M, et al. Differences in the clinical characteristics of Pneumo-
cystis jirovecii pneumonia in immunocompromised patients with
and without HIV infection. Respirology. 2010;15:126–31.
8. Wang XL, Wang XL, Wei W, An CL. Retrospective study of
Pneumocystis pneumonia over half a century in mainland China.
J Med Microbiol. 2011;60:631–8.
9. Fujii T, Nakamura T, Iwamoto A. Pneumocystis pneumonia in
patients with HIV infection: clinical manifestations, laboratory
findings, and radiological features. J Infect Chemother.
2007;13:1–7.
10. Catherinot E, Lanternier F, Bougnoux ME, Lecuit M, Couderc
LJ, Lortholary O. Pneumocystis jirovecii pneumonia. Infect Dis
Clin N Am. 2010;24:107–38.
11. Matsumura Y, Shindo Y, Iinuma Y, Yamamoto M, Shirano M,
Matsushima A, et al. Clinical characteristics of Pneumocystis
pneumonia in non-HIV patients and prognostic factors including
microbiological genotypes. BMC Infect Dis. 2011;11:76.
12. Roblot F, Godet C, Le Moal G, Garo B, Faouzi Souala M, Dary
M, et al. Analysis of underlying diseases and prognosis factors
associated with Pneumocystis carinii pneumonia in immuno-
compromised HIV-negative patients. Eur J Clin Microbiol Infect
Dis. 2002;21:523–31.
13. Aoki Y, Iwamoto M, Kamata Y, Nagashima T, Yoshio T,
Okazaki H, et al. Prognostic indicators related to death in patients
with Pneumocystis pneumonia associated with collagen vascular
diseases. Rheumatol Int. 2009;29:1327–30.
14. Tokuda H, Sakai F, Yamada H, Johkoh T, Imamura A, Dohi M,
et al. Clinical and radiological features of Pneumocystis pneu-
monia in patients with rheumatoid arthritis, in comparison with
methotrexate pneumonitis and Pneumocystis pneumonia in
acquired immunodeficiency syndrome: a multicenter study.
Intern Med. 2008;47:915–23.
15. Bollee G, Sarfati C, Thiery G, Bergeron A, de Miranda S,
Menotti J, et al. Clinical picture of Pneumocystis jiroveci pneu-
monia in cancer patients. Chest. 2007;132:1305–10.
16. Tasaka S, Tokuda H, Sakai F, Fujii T, Tateda K, Johkoh T, et al.
Comparison of clinical and radiological features of pneumocystispneumonia between malignancy cases and acquired immunode-
ficiency syndrome cases: a multicenter study. Intern Med.
2010;49:273–81.
17. Atzori C, Agostoni F, Angeli E, Mainini A, Orlando G, Cargnel
A. Combined use of blood and oropharyngeal samples for non-
invasive diagnosis of Pneumocystis carinii pneumonia using the
polymerase chain reaction. Eur J Clin Microbiol Infect Dis.
1998;17:241–6.
18. Leigh TR, Wakefield AE, Peters SE, Hopkin JM, Collins JV.
Comparison of DNA amplification and immunofluorescence for
detecting Pneumocystis carinii in patients receiving immuno-
suppressive therapy. Transplantation. 1992;54:468–70.
J Infect Chemother (2012) 18:722–728 727
1 3

8/9/2019 PJP Pneumonia
http://slidepdf.com/reader/full/pjp-pneumonia 7/7
19. Tasaka S, Hasegawa N, Kobayashi S, Yamada W, Nishimura T,
Takeuchi T, et al. Serum indicators for the diagnosis of pneu-
mocystis pneumonia. Chest. 2007;131:1173–80.
20. Watanabe T, Yasuoka A, Tanuma J, Yazaki H, Honda H,
Tsukada K, et al. Serum (1?3) beta-D-glucan as a noninvasive
adjunct marker for the diagnosis of Pneumocystis pneumonia in
patients with AIDS. Clin Infect Dis. 2009;49:1128–31.
21. American Thoracic Society, Infectious Diseases Society of
America. Guidelines for the management of adults with hospital-
acquired, ventilator-associated, and healthcare-associated pneu-
monia. Am J Respir Crit Care Med. 2005;171:388–416.
22. Arend SM, Kroon FP, van’t Wout JW. Pneumocystis carinii
pneumonia in patients without AIDS, 1980 through 1993. An
analysis of 78 cases. Arch Intern Med. 1995;155:2436–41.
23. Wachter RM, Luce JM, Safrin S, Berrios DC, Charlebois E,
Scitovsky AA. Cost and outcome of intensive care for patients
with AIDS, Pneumocystis carinii pneumonia, and severe respi-
ratory failure. JAMA. 1995;273:230–5.
24. Buttgereit F, Burmester GR, Straub RH, Seibel MJ, Zhou H.
Exogenous and endogenous glucocorticoids in rheumatic dis-
eases. Arthritis Rheum. 2011;63:1–9.
25. Nakamura H, Tateyama M, Tasato D, Haranaga S, Yara S, Higa
F, et al. Clinical utility of serum beta-D-glucan and KL-6 levels
in Pneumocystis jirovecii pneumonia. Intern Med. 2009;48:
195–202.
26. Green H, Paul M, Vidal L, Leibovici L. Prophylaxis for pneu-
mocystis pneumonia (PCP) in non-HIV immunocompromised
patients. Cochrane Database Syst Rev. 2007;3:CD005590.
27. Rabodonirina M, Vanhems P, Couray-Targe S, Gillibert RP,
Ganne C, Nizard N, et al. Molecular evidence of interhuman
transmission of Pneumocystis pneumonia among renal transplant
recipients hospitalised with HIV-infected patients. Emerg Infect
Dis. 2004;10:1766–73.
28. Hocker B, Wendt C, Nahimana A, Tonshoff B, Hauser PM.
Molecular evidence of Pneumocystis transmission in pediatric
transplant unit. Emerg Infect Dis. 2005;11:330–2.
29. de Boer MG, Bruijnesteijn van Coppenraet LE, Gaasbeek A,
Berger SP, Gelinck LB, van Houwelingen HC, et al. An outbreak
of Pneumocystis jirovecii pneumonia with 1 predominant geno-
type among renal transplant recipients: interhuman transmission
or a common environmental source? Clin Infect Dis. 2007;44:
1143–9.
30. Schmoldt S, Schuhegger R, Wendler T, Huber I, Sollner H,
Hogardt M, et al. Molecular evidence of nosocomial Pneumo-
cystis jirovecii transmission among 16 patients after kidney
transplantation. J Clin Microbiol. 2008;46:966–71.
31. Yazaki H, Goto N, Uchida K, Kobayashi T, Gatanaga H, Oka S.
Outbreak of Pneumocystis jirovecii pneumonia in renal transplant
recipients: P. jirovecii is contagious to the susceptible host.
Transplantation. 2009;88:380–5.
728 J Infect Chemother (2012) 18:722–728
1 3
![PJP ja PJU esitys (2).pptx [Vain luku] - rakennusteollisuus.fi · Eroja, onko niitä? • PJP / PJU suurin ero on siinä kumman osapuolen nimiin hankinnat laaditaan. o Eli päätoteuttaja](https://img.pdfslide.tips/doc/110x75/5d29d59b88c99339328d3908/pjp-ja-pju-esitys-2pptx-vain-luku-eroja-onko-niitae-pjp-pju-suurin.jpg)



![0/ · b SrWn MSf nYu r u f oWnY` w Sw.X]b P[P P[P[P PjP P[P P[P[P P[P PjP P[P[P P[P P[PjP P[P P[P P[P[P PjP ? D _ G0C G0 xG | NGIKd t = H L= D FLN J D ~H WFK 4L=D K7DMJ F ~](https://img.pdfslide.tips/doc/110x75/5ecbc746a6fdbb3d9c7673f6/0-b-srwn-msf-nyu-r-u-f-owny-w-swxb-pp-ppp-pjp-pp-ppp-pp-pjp-ppp-pp.jpg)