-
8/8/2019 Presentation Adrenal
1/29
Anatomy, Embryology & Physiology
Sreeja Biswas
-
8/8/2019 Presentation Adrenal
2/29
INTRODUCTION
ADRENALS :
y Two small yellow flattened bodies at the back ofabdomen,
retroperitoneal
yAbove & in front of upper end of each kidneys
y Size varies from 3-5 cm length
4-6 mm thickness
less in width
yAverage weight is about 1.5-2.5 gms each
y Most highly perfused of all organs
(blood flow 2000 ml/kg/min)
-
8/8/2019 Presentation Adrenal
3/29
DEVELOPMENT
ADRENAL CORTEX :
y Celomic mesoderm(near cephalic end of mesonephros)
y Recognizable first at about 4thweek of gestation(series of
buds at root of mesenterysuprarenal ridge)
ADRENAL MEDULLA:
y Sympatho-chromaffin tissue(ectoderm)
y Recognizable first at about 5th to 6thweek of gestation
-
8/8/2019 Presentation Adrenal
4/29
SURGICAL RELEVANCE :
Extra-adrenal sites for cortex & medulla - usually along
thepaths of migration during embryogenesis
-
8/8/2019 Presentation Adrenal
5/29
ANATOMY
RIGHT SUPRARENAL GLAND :
y Triangular in shape
y 2 surfaces - anterior & posterior
y
Anterior surface - forward and laterallyInferior Vena Cava
mediallyRight lobe of liver laterally
y Posterior surface upper part-diaphragm
lower part-right kidney
y Base downwardy Hilum below apex, suprarenal vein emerges from
anterior
border
-
8/8/2019 Presentation Adrenal
6/29
ANATOMY (cont.)
y LEFT SUPRARENAL GLAND :y Larger, crescentric medial &
lateral borders
anterior & posterior surfacesy Medial border convex
y Lateral border concave(upper part of left kidney)y Anterior
surface
upper part-peritoneum of omental bursalower part-tail of
pancreas,lienal artery
y Posterior surface lateral area-left kidneymedial area-left
crus of diaphragm
y Hilum lower end of anterior surface
-
8/8/2019 Presentation Adrenal
7/29
ANATOMY cont.
y The surfaces of the suprarenal glands are surroundedby areolar
tissue containing much fat & closely
invested by a thin fibrous capsule, which is difficult toremove
on account of the numerous fibrous processes& vessels entering
the organ through the furrows on itsanterior surface and base
-
8/8/2019 Presentation Adrenal
8/29
HISTOLOGY
EXTERNAL CORTEX
INTERNAL MEDULLA
y CORTEX 3parts
(outside inwards)
Zona Glomerulosa
Zona Fasciculata
Zona Reticularis
y MEDULLA
-
8/8/2019 Presentation Adrenal
9/29
HISTOLOGY (cont.)
CORTEX:y 1. zona glomerulosa situated just beneath the
capsule,
rounded cells - very granular & stain deeply
y 2. zona fasciculata composed of columns of cells
arranged in a radial manner intracellular finergranules &
lipoid materials
y 3. zona reticularis composed of irregularly
arrangedcylindrical masses of cells intracellular pigment
granules which makes this zone darker than the rest ofthe
cortex
-
8/8/2019 Presentation Adrenal
10/29
HISTOLOGY (cont.)
MEDULLA:y Extremely vascular ,large irregular
polyhedral chromaphil cells finely
granular cytoplasm
y Large anastomosing venous sinusoidsbathing the medullary cells
directly in
blood at some places where the
endothelium is deficient.
y
Loose network of supporting non-striped muscle fibers richly
supplied with non-medullated nerve fibers &occasional
sympathetic ganglia
-
8/8/2019 Presentation Adrenal
11/29
VASCULATURE, LYMPHATICS & NERVES
ARTERIAL :
y 1. superior adrenal branch of inferior phrenic
y 2. middle adrenal branch of aorta
y3. inferior adrenal branch of renal artery
-
8/8/2019 Presentation Adrenal
12/29
VASCULATURE, LYMPHATICS & NERVES
(cont.)
VENOUS : arise from medullary venous plexus
solitary drainage
emerge from the hilum
1. right adrenal (0.5cm) directly to inferior vena cava
2. left adrenal (2.0cm) to left renal vein
y
In 20% of cases right adrenal vein drains to accessoryright
hepatic vein or at the confluence of a vein
-
8/8/2019 Presentation Adrenal
13/29
VASCULATURE, LYMPHATICS & NERVES
(cont.)LYMPHATICS :
to the lumbar glands
NERVES :
from celiac & renal plexus
enters through the lower & medial part ofthe capsule ends in
the medulla
-
8/8/2019 Presentation Adrenal
14/29
PHYSIOLOGY
ADRENAL MEDULLA:y Secretes epinephrine(E), nor-epinephrine(NE)y
In humans,80% of output is epinephriney Effects are same as direct
symphathetic nervous
stimulationy Synthesis of catacholamines begins with tyrosine,
which is
taken up by the chromaffin cells in the medulla &converted
to NE/E .
y NE/E are stored in electron-dense granules along with ATP&
neuropeptides.
y Release is stimulated by ACh from pregangloinicsympathetic
fibers innervating the medulla and Stressfactors
-
8/8/2019 Presentation Adrenal
15/29
-
8/8/2019 Presentation Adrenal
16/29
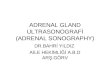
PHYSIOLOGY(cont.)
ADRENAL CORTEX:
Adrenal steroid
biosynthesis pathway-y 1. aldosterone
y 2. cortisol
y 3. androgens
-
8/8/2019 Presentation Adrenal
17/29
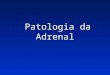
GLUCOCORTICOIDS
CORTISOL : major glucocorticoid
Control of cortisol secretion
-
8/8/2019 Presentation Adrenal
18/29
GLUCOCORTICOIDS(cont.)
CORTISOL :
Mechanism of action
y 1. cortisol binds to cytoplasmic receptor
y 2. hormone-receptor complex is transferred to thenucleus
y 3. complex binds to nuclear DNA response element
y Cortisol circulates in blood bound to transcortin, only10% of
the hormone is in free form.
-
8/8/2019 Presentation Adrenal
19/29
-
8/8/2019 Presentation Adrenal
20/29
GLUCOCORTICOIDS(contd.)
IMMUNOSURPPRESSIVE ACTIONS:
y Reduce lymphocyte & eosinophil countsy Increase neutrophil
count
y Suppress histamine release
y Promote lymphocyte apoptosis
y Reduce prostaglandin synthesis
-
8/8/2019 Presentation Adrenal
21/29
MINERALOCORTICOIDS
ALDOSTERONE : major mineralocorticoid
Control of aldosterone secretion
y 1. K+ concentration in extracellular fluid
(even small increase in K+
strongly stimulates)y 2. angiostensin II level in blood
(the Renin-Angiotensin-Aldosterone-Axis)
y 3. others -
ACTH (short-term stimulation)
Na+ deficiency stimulates
Atrial natriuretic peptide(ANP), high Na+ and lowK+
concentration supress aldosterone secretion
-
8/8/2019 Presentation Adrenal
22/29
MINERALOCORTICOIDS(cont.)
ALDOSTERONE :
Mechanism of action
y 1. renal resorption sodium & water
y 2. renal excretion of potassium
-
8/8/2019 Presentation Adrenal
23/29
MINERALOCORTICOIDS(cont.)
REMOVAL OF THE ADRENALS LEADS TO DEATH
Effects of lack of ALDOSTERONE activity
salt and water wasting & K+/H+ retention
-hyponatremia
-hypovolemia
-hyperkalemia
-acidosis-decreased cardiac outputshock/death
-
8/8/2019 Presentation Adrenal
24/29
DISEASE STATES
ADDISONS DISEASE:
yAdrenal insufficiency
y Characterised by hypoadrenocorticism ie. both
mineralocorticoid(aldosterone) andglucocorticoid(cortisol)
deficiency
y Lethal unless hormonereplacement(mineralocorticoid) treatment
is
institutedy Death due to shock & electrolyte inbalances
-
8/8/2019 Presentation Adrenal
25/29
DISEASE STATES (cont.)
CONNS DISEASE :
y Primary hypersecretion of aldosterone
y High BP is usually the only finding due to salt &
water
retentionyAssociated hypokalemia can present with muscle
fatigue
y Treatment includes spironolactone or surgical removal
of the adrenal adenoma
-
8/8/2019 Presentation Adrenal
26/29
DISEASE STATES (cont.)
CUSHINGS DISEASE :
y Causes exogenous steroidadministration(commonest)
y
Maybe due to ACTH secreting pituitaryadenoma(cushings syndrome)
or ectopic ACTH/CRHsecretion from nonendocrine tumours(small cell
lungcarcinoma,thymic and pancreatic carcinoma) oradrenal
neoplasia.
y Characterised by hyperadrenocorticism ie. increasedlevels of
both glucocorticoids & mineralocorticoids
-
8/8/2019 Presentation Adrenal
27/29
DISEASE STATES (cont.)
CUSHINGS DISEASE (cont.) :
y Typically presents with moon facies, interscapularbuffalo
hump, truncal obesity but thin extremities,
hypertension, muscle fatigue, osteoporosis, glucoseintolerance
etc
y Management depends on the etiology : surgical forneoplastic
causes followed by post-operative radiation
therapy.Ketoconazole decreases adrenalsteroidogenesis.
-
8/8/2019 Presentation Adrenal
28/29
DISEASE STATES (cont.)
PHEOCHROMOCYTOMA:y Adrenal medullary tumour arising from the
chromaffin
cells of the sympathetic nervous system.y Extra-adrenal
pheochromocytomas arise from the celiac,
superior mesenteric & inferior mesenteric gangliay
Epinephrine/Nor-epinephrine secretion causes episodic
tachycardia, hypertension, sweating & flushingy Dopamine
secretion occurs in the familial syndromes(5%
cases autosomal dominant either alone or in associationwith MEN
type Iia/b) & are not associated with
hypertensiony Treatment with alpha-adrenergic blockers
(phentolamine/phenoxybenzamine) and surgical resection
-
8/8/2019 Presentation Adrenal
29/29
y THANK YOU