Embed Size (px)
Citation preview

대 한 방 사 선 의 학 회 지 1993 ; 29 ( 1) : 165~ 173
Journal of Korean Radiological Society, January, 1993
Radiological Evaluation of Congenital Pulmonary Vein Obstruction *
Woo Sun Kim , M.D. , Kyung Mo Yeon , M.D. , In-One Kim , M.D. ,
Yong 800 Yoon , M.D. **, Yeon-Lim 8uh, M.D. ***, Je G. Chi , M.D. ****
Departmeηt 01 Radiology, Seoμl National [J,ηiversity CoUege 01 M edicine
- Abstract-
Congenital obstruction of pulmonary vein without anomalous drainage can cause long-standing pulmonary
congest ion and pulmonary arterial hypertension , and it may include stenosis of individual pulmonary veins
or total p비monary vein atresia . We reviewed seven cases of pulmonary vein obstruction , fi ve of which ac
companied other cardiac anomalies. Righ t p비monary veins were involved in all seven cases including one
bilateral case . Pulmonary veins were occluded totally in five and partially in three lungs .
Pulmonary catheterization and angiography were done for diagnosis . Chest radiographs of total occlu
sion cases showed decreased lung volume , features ofpulmonary edema , interstitiallesions , and pleural thicken
ing, which were quite specific , whereas pulmonry venous dilatation was dominant findings in partial obstruction
cases. Pulmonary perfusion scans (n = 3) showed total perfusion defects in the cases oftotal occlusion ofveins.
MR imaging (n = 2) demonstrated total occlusion of pulmonary veins in the venoatrial junction in two , and
membranous focal obstruction in one lung. Two patients had pneumonectomy and histological confirma
tion . AJthough catheterization and angiography are essential for the diagnosis , MR imaging is thought to
be useful for the diagnosis of pulmonary ve in obstruction
Index Words: Pulmonary veins
PuJmonary Veins , stenosis
Pulmonary veins, abnormalities
Children , cardiovascular system
INTRODUCTION
a re caused by long-standing pulmonary conges
tion (1-13). Although catheterization and
angiography are essential for the diagnosis of
pulmonary vein obstruction , they do not always
show obstructed pulmonary veins itself, especial
ly in cases with total oclusion (9-13). W e per
formed MR imaging in two recent cases to
Pulmonary vein obstruction can be congenital
o r acquired (1-22). Congenital obstruction of
pulmona ry vein is presented as chronic cough , h emoptysis, and recurrent pneumonias , which
* 이 연구는 1991년도 서울대학교병원 특진연구비 지원에 의한 결과임(과제변호 : 02-91-171)
**서울대학교 의과대학 소아과학교실
** Department 01 Pediatrics, Seoul National Universiψ College 01 Mediciηe
*** 인제대학교 의과대학 병리학교실 *** Departmeηt 01 Pathology, 1ηje University College 01 Medicine
**** 서울대학교 의과대학 병리학교실 **** Department 01 Pathology, Seoul Natioηal University College 01 Mediciηe
이 논문은 1992년 8월 12일 접수하여 1992년 10월 5일에 채택되었음.
Received August 12, Accepted October 5, 1992
뼈

Journal of Korean Radiological Society 1993; 29 (1) 165~ 173
visualize obstructed pulmonary veins. W e
reviewed clinical and radiological features of
seven cases with pulmonary vein obstruction a nd
discussed about the role of MR imaging in this
disease .
MATERIALS AND METHODS
Authors experienced seven cases ofpulmonary
vein obstruction without anomalous drainage in
Seoul Nationa l University Children's H ospita l
frm 1982 to 199 1. Among seven children , four
(case 1-4) h ad mainly pulmonary symptoms of
long. standing cough , rccurrent pneumon ia , a nd
h emoptys is from their infan cy . Their m can agc
was 5 years. The earli est clinical presenta tion was
h emoptysis at seven days of age in case 3. In thc
other three children (case 5-7) cardiac sym ptom s
due to associated cardiac anomalies we rc
predominan t.
Chest radiographs of seven children 씨le re
reviewed. In two cases (case 2 and 4) , follow -up
chest radiographs for three years were available
Cardiac catheterization and cine-angiography in
cluding pulmonary a n giography were perform
ed in all cases . Aortograph ies were also done in
two cases (case 1 a nd 5). Radioi sotope pulmo n-
Table 1. Summary o[ Clinical Features in Seven Cases o[ Pulmonary Vein Obstruction
Patient Age/Sex
5/F
2 lIF
3 9/M
4 5/F
5 0+ 1/F
6 6/M
7 131M
Symptoms & Signs
recurrent hemoptysis
and pneumonia
recurrent hemoptysis
and pneumonia
recurrent hemoptys is and pneumonia
cyanosls
recurrent hemoptysis
and pneumonia
dys pnea
cardiac murmur
dyspnea
PDA
cyanosls growth retardation
Accompanied Anom alies
tracheaJ bronchus
(right upper lobe)
partiaJ cor triatriatu m ,
PDA , biJateral SVC , multipJe hemangioma in
skin , di gital anomaly
left SVC pure red cell apJas ia
( - )
multiple VSD and ASD
PDA , pulmonary sequestration vertebr‘ aJ anomaJy
secundum ASD
PDA
(Eisenmenger complex)
secundum ASD
ear , eye anomaly
undescended testicle
In voJvcd Veins
right
r ight
ri ght left (foca l)
right
right
ri ght u ppel
(fo caJ)
ri ght uppel
(focal)
* PA: pulmonary artery , PV: pulmonary vein , WP: wedge pressure , SVC: superior ve na cava , ASD ‘ atriaJ septal defect. VSD: vetricular septal defect , PDA: patent ductus arteriosus
- 166 -

Woo Sun Kim , et al : Radiological Eva luation of Congenital Pulmonary Ve in Obstruction
ary perfusion scans using technetium-99m
macroaggregate albumin were done in three
cases. 1n recent two cases (case 3 and 4) , MR
imagings were performed with a 2 .OT supercon
ductive system (Spectro-20000; Goldstar, Seoul, Korea) . Axial and coronal T 1 weighted imag
ings with cardiac gating were obtained. 1n case
3 , chest CT (10mm thickness , lOmm interval)
was done. Two cases (case 1 and 4) had
pneumonectomies and histologic studies. 1n two
cases (case 2 and 7) , pulmonary vein obstruc
tion were observed during cardiac surgeries.
RESULTS
The clinical features in seven cases of
pulmona ry vein obstruction is summarized in
table 1. Right pulmonary veins were obstructed
in all seven cases , total occlusion in fi ve cases
(case 1-5) and focal partial obstruction at the
right superior venoatrial junction in two cases
with large atrial septal defects (ASD) (case 6 and
7) . Left pulmonary veins were also partially in
volved in case 3. 1n case 2, left pulmonary venous
drainage was also obstructed partially by a
diaphragm in the left artium (partia l cor
Pulmonary Arterial O 2 Saturation Operations Pressure(mm H g) ( % )
main PA 32/8 79 ri ght pneumonectomv left PA 30/12 77 right PA 40/8 main PA 68/28(48) 64 cord-like right PV left P A 68/28(44) 64 PDA Iigat ion left PA WP (16) resection of abe rrent muscl e
in left atrium main P A 50/28 82 left PA 50/2.1 81 left PV 16 96 left atri um 11 main PA 25/ 12 78 right pneumonectom y right PA 27/18 82 right PA 、VP 29/2 1 88 left PA WP 17/8 Not Availabe
main PA 130/75 left P A 120/80
83 83
main PA 30/15 left PA 25/ 15 right upper PV 26/12 left u pper PV 14/7
left atrium 5
야ω mω %
98
w” 겐
mw LU
객υ
. m m u t
쩍
m f o
@ d
n ·m 뼈 없
w

Journal of Korean Radiological Society 1993 ; 29 ( 1) 165~ 173
tr띠‘
C hest rad비iographs showed decreased lung
volume (6 cases) , small hila (5 cases) , diffues hazy
densities (4 cases) , reticulonodular den sities (4
case) , multiple K erley ’ s lines (4 cases) , cystic le
sions (air cysts) (4 cases) , and pleural changes
(5 cases) in the involved side (Fig. la) . Car-
a b
c
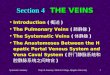
Fig. 1. Patient 4
diomegaly was noted in three cases. In case 7, dila ted pulmon ary vein in the right uppe r lung
fi eld was the only finding . Pulmona ry venou s
dialtation was also n oted in the left lung of case
3 . In two cases , follow up radiographs for three
years showed progressive volume decrease and
d evelopment of reticulonodular densities
d
a. C hest radiograph shows decreased right lung volume with hern iation of left lung(arrows) . The right lung shows reticulonodular densities , multiple Kerley ’ s lines , cystic lesions, and pleural thickening. b . Right pulmonary arteriogram shows small sized arteries without peripheral filling (“dead tree" appearance) (arrows) , ref1 ux of contrast media to the left pulmonary artery , and systemic-pulmonary arterial fistula (arrowheads) c . Levo-phase of pulmonary arteriogram (b) shows the left pulmonary veins and the left atrium without visuali zation of the right pulmonary vein. See the right border of the left atrium (arrowsheads) d . Pulmonary perfusion scan shows a complete perfusion defect in the right lung.
- 168-

Woo Sun Kim , et al : Radiological Evaluation of Congenital Pulmonary Vein Obstruction
le
e. Axial MR imaging on the level 0 1' the left atrium shows cord-like occlusion of the right superior pulmonary vein at its venoatrial junction and extrapulmonic segment (arrowheads). Decreased right lung volume and pleural thickening are also noted . f. CT with lung-window setting shows irregular reticular interstital changes , cystic lesions , and thickening of interlobular septa in the right lung.
Pulmonary catheterization revealed pulmon
ary arterial hypertension in six cases (not
available in case 5). Pulmonary arterial wedge
pressure of the involved lung was available in
case 4 and was elevated. In cases with focal
obstruction , pressure gradients were detected
between the left atrium and obstructed
pulmonary veins (case 7 and the left lung of case
3) (Table 1). Pulmonary arteriography
demonstrated small peripheral pulmonary
arteries of the involved side without peripheral
filling (“dead tree" appearance) (6 cases) , reflux
of contrast media from ipsilateral peripheral
pulmonary arteries (5 cases) , delayed pulmonary
transit time (5 cases) , and systemic - pulmonary
arterial collaterals (2 cases) (Fig. 1 b) . In levo
phase of pulmonary angiography , involved
pulmonary veins were not visualized in five cases
(Fig. 1 c). Left pulmonary veins of case 3 show
ed engorgemerit and delayed drainage to the left
atrium. In case 6 and 7, the right upper
pulmonary venography through ASD demon
strated focal stenoses in the superior pulmonary
veins (Fig. 3). Aortography in case 1 and 5 show
ed multiple systemic collaterals and retrograde
opacification of right pulmonary arteries from
the ir peripheries. Five cases accompanied other
Fig. 2. Coronal MR imaging of Patient 3 with bilateral pulmonary vein obstruction shows septum like structure in the left venoatrial junction (arrow) and engorgement of the left pulmonary vein. No evidence of draining veins in the right border of the left atrium(open arrows).
- 169-

Journal of Korean Radiological Society 1993; 29 (1) 165~ 173
Fig. 3. Right upper pulmonary venogram (four chamber view) ofPatient 6 shows focal narrowing in the right superior pulmonary vein(arrows). Secundum ASD(arrowheads)is also demonstrated.
cardiac anomalies (Table 1)
Pulmonary perfusion scans in 3 cases (case
1,3 , and 4) showed total perfusion defects in the
involved lungs (Fig. 1d) . Perfusion in the left
lun g, however , was preserved in the case o[ par
tial obstruction of the left pulmonary vein (case
3) MR imaging showed total occlusion o[ right
pulmonary veins in their venoatrial junctions and
extra pulmonary segements (case 3 and 4) and
cord- Iike intrapulmonary pulmonary veins (case
4) . In case 3, membranous obstruction at the left
venoatrial junction (Fig. 2) and left -sided
superior vena cava was also demonstrated . MR imaging also showed small right pulmonary
arteries and pleural thickening in both cases. CT
with lung window setting in case 4 demonstrated
decreased right lung volume with diffus haziness , reticular in terstitial densities , multiple small air
cysts, and thickening of interlobular septa, ma
jor fissure , and the pleura (Fig . 1f). Pulmonary vein obstructions were confirm
ed by pneumonectomies and histological ex
aminations in case 1 and case 4. In case 2 , a
cord-like occlusion of right pulmonary veins were
observed during the cardiac surgery. In case 7, a redundant septum obstructing the orfice of the
right upper pulmonary vein was noted and it was
excised during the operation. Each of obstructed
pulmonary vein s had a normal site of connec
tion with the left atrium in all four operated cases.
Gross pathological examinations in case 1 and
case 4 showed consolidated lungs with occluded
cord-Iike pulmonary ve ins, cystic parenchymal
changes , and pleural thickening and adhesion , On histological examination , irregular fibrous
intimal proliferation , m edial hypertrophy , and
organized thrombi were observed in pulmonary
veins , and these changes were more pronounc
ed in larger veins. These change were not observ
ed in pulmonary venules. I-l istological features
were compatible with congenital p비monaryvem
obstructon.
DISCUSSION
Anomalies which can cause pulmonary
arterial hypertension b y obstruction of
pulmonary venous drainage may include con
genital anomalous pulmonary venous connec
tions , cor triatriatum , mitral stenosis or atresia , and pulmonary vein obstuction (1 ,2). Pulmonary
vein obstuction without anomalous return is very rare and may include ste nosis 0 1' individual
pulmonary veins (1-12) and atresia 0 1' pulmonary
vein (1, 2,13). Pulmonary venous obstruction may be acqu ired 1'orm pulmonary veno-occlusive
disease or 1'rom compli cations of some diseases , such as constrictive pericarditis , mediastinitis, pulmonary venous phlebitis (as in tuberculosis) , and invasion by malignant tumor (2 ,5 ,14-23)
Individual pulmonary vein stenosis and 'atresia
of pulmonary vein are thought to be caused by
anomalous incorporation of the common pul
monary veins into the left atrium (1-3). They
may occur in the same patient and one or more
ve ins may be involved (1-5 , 10-13). They may
be present in isolation or in association with other
congenital cardiac anomalies (50 % ) (1,2,1 0-13)
- 170 -

Woo Sun Kim. et al : Radiological Evaluation of Congenital Pulmonary Vein Obstruction
T he obstruction usually occurs at the venoatrial
junction , but it O1ay extend for01 this point to
the periphery (1 ,2,5,10). Obstruction in the for01
of a diaphrag01 (foc띠 stenosis) or occlusion of
varing length O1 ay be present aloneor in coo1-
bination (2 ,5,10). Histologically fibrous inti01al
thickening is present and the ve in O1ay exist as
a fibrous cord (2 ,3 ,5 ,9-10). Thro01bus for01 a
tion in the stenotic veins secondary to stasis of
blood also can be observed (4 ,13). These changes
are discovered O1ainly in large veins with less in
volvement or sparing of small vein s or venules
Interst itial les ions , air-cys t for01ation , fíbrosis , and dilatation 0 1" p비monary lY01pha tics and
bronchial ve in can be noted (3-5 ,11 ,13). The
develop01ent of collateral circulation through the
bronchial vesselleads to early and .severe he01op
tysis (4 ,11 ,13). The O1ost co0101on sY01pto01s of
congenita l pulO1onary vein obstruction are recur
rent respiratory trac t infections and he010ptysis
for01 the earl y i바ancy (4 ,, 8 ,9 ,11 ,13) Radiological features of congenital pulO1onary
vein atres ia and significant stenosis are similar
to each other (11-13). D ecreased lung volu01e, pulO1ona ry ede01a , reticula r densiti es , O1 ultiple
air cysts , O1ultiple Kerley ’s B lines , accentuation
。 f fi ssures , and pleural changes , all of which are
discovered in the in volved lung , are unique
radiographic findings (Fig. 1a) (5 ,11-13). These fïndin gs represe nt chron ic pulO1onary venous
obstuction and fibrotic changes of the lun g. In
cases with on ly pa rtial obstruct ion (case 6,7, and
the left lung of case 3) , these findings were not
shown , and pulO1onary venous congestion or
engorge01ent was the only fínding. PulO1onary
arte r‘ ial catheter ization reveals pulO1 ona ry
arter‘ ial hypertension and elevated arterial 、이ledge
pressu re of the in volved lung (5 ,11). Pul O1onary
angiogra01 shows s01all ipsilateral pulO1onary
artery wi thout peripheral filling producting the
dead tree appearance (Fig. 1 b) , delayed circulatio l1 , and diversion of blood fro01 the affected
pulO1on ar y a rtery (2 ,11 ,12). 111 levo- phase of
pulO1onary angiography, visualization of involv
ed pulO1o l1 ary ve il1 s is ab5ent or delayed (Fig
1 c) (2 ,11-13). Although visualization o ffo call y
obstructing lesion is possible by selective
pulO1onary venography (Fig. 3) (2 ,12) or by
pulO1onary artery wedge angiography (2 ,1 이 , it is not alway possible , especially in cases with ex
tensive occlusion to the perphery (Fig. 1c)
(9 ,11 ,13). Syste01ic-pulO1onary collaterals can be
noted in aortography (3 ,4,11). Radioisotope perfusion scans show abse nt or di01inished perfu
sion of affected lobes (Fig. 1d) (11 ,13)
PulO1onary veno-occlusive disease is an ac
quired disease without difinitely known etiology
(2 ,14-21). The s01all veins or venules (so01eti01es
also the major veins) are predo01inantly narrow
ed or occluded by fibrous tissue on the basis of
organized thro01bi (14-22). It usually involves
the lung bilaterally (14-17 , 20-22). but occa
sionally the involve01ent of O1ajor veins O1ay be
li01ited to one lung (18-19). Cardiac ano01alies
are absent and it usually affects older children
or adults (1 4-15 , 17-20). Radiographic findings
include card io01egaly , pulO1 onary ede01a , K erley ’ s lines and interlobar effusion and/or subpleural ede01a (14-15 , 23). Catheterization
reveals pulO1onary arterial hypertension , nor01al
or only slightly elevated pulO1onary venous
pressure , but pulO1onary wedge pressure is paradoxically nor01al (14-15 ,17 ,21). PulO1onary
angiography reveals dilated pulO1onary arte ries , prolonged ci rculation ti01e , and nor01al
pulmonary vemLung perfusion scan is usually normal in
pulO1onary veno-occlusive disease (14 ,15)
In two cases (case 1 and 4) of tl띠 study who
had operations , history of recurrent infections and he010ptysis fro01 the infancy , unilateral in
volve01ent , decreased lung volu01e with fibrotic
changes , cord-like O1ajor pulmonary veins , unilateral total perfusion defects in perfusion
scan , elevated pulO1onary wedge pressure of the
involved side (case 4) , and involvem ent of large
veins with less changes in small veins and spar
ing of venules on histological exa01 ination sup
ported the congenital nature of pulmonary ve in
obstruction. Other cases in this study also had
m

Journal of Korean Radiological Society 1993; 29 (1 ) 165~ 173
symptoms from the infancy and accompanied
other anomalies (especially cardiac) , which sug
gested the congenital nature of lesions.
MR imaging in the evaluation of pulmonary
vein obstuction has been reported recently , but
mainly in cases with anomalous pulmonary
venous return (24) . Masui et al. (25) reported
that MR imaging can demonstrate anatomic ab
normality in pulmonary vein stenosis and cor
triatriatum. Two MR studies in our study show
ed total occlusion of pulmonary veins at
venoatrial junctions, cord-like veins in their ex
trapulmonary segments (Fig. l e) , and small
pulmonary artery of the involved lung. Mem
branous structure at the venoatrial junction was
demonstrated in the case with focal obstruction
(Fig. 2). In cases with totally occluded pulmonary
veins , MR imaging could visualize the state of
veins which angiography could not show (Fig
le). MR imaging could also reveal other cardiac
anomalies which are often accompanied by this
disease
In summary , we reviewed seven cases of
pulmonary vein obstruction in which right lungs
were involved predorninantly. Findings on chest
radiographs which included decreased lung
volume and pulmonary edema with reticular and
cystic changes were very unique and they could
strongly suggest the possibility of pulrnonary vein
occlusion. Although catheterization and
angiography may be still essential for the
diagnosis of pulmonary vein obstuction , MR irn
aging is thought to be a useful modality for the
diagnosis of this disease .
REF'ERENCES
1. Lucas RV , Anderson RC , Amplatz K , Adams P , EdwardsJE. Congenital causes ofpulmonary venous obstruction. Pediat r Clin North Am
1963 ;10:781 2. Freedom RM , Culham JAG , Moes CAF
Angiocardiography of congenital heart disease , 1st ed. Macmillan publishing company , New York , 1984
3. Sherman FE , Stengel WF , Bauersfeld SR. Con genital stenosis of p비monary veins at theÏl‘ atri al junctions. Am H eart J 1958 ;56 :908
4. Bernstein J , Nolke AC , Reed JO . Ex trapulmonary stenosis of the pulmonary ve ins Circulation 1959 ;19:891
5 . Shone JD , Amplatz K , Anderson RC , Adams P J r , Edwards JE. Congenital stenosis of individual pulmonary veins. Circulation 1962 ; 26:574
6. Singshinsuk J , H artmann AF , Elliott LP.
Stenosis of indi vidua l pulmonary vein s R adiology 1980;87 :514
7. Contis G , Fung RH , Vawter GF , Nadas AS . Stenosis and obstruction of the pulmonry ve in associated with pulmonary artery hypertension. Am J Cardial 1967 ;20:718
8. Mortensson \시, Lundstrom NR. Congenital obstruction of the pulmonary veins at their atrial juncdtions: Review of the literature and a case repor t. Am H eart J 1967;87 :359
9 . Sade RM , Freed MD , Matthews EC , Castaneda AR. Stenosis fo indicidual pulmonary veins Review of the literature and report of a surgical
case. J Thorac Cardiovase Surg 1974;67:95 3 10. Bini RM , Cleveland DC , Ceballos R , Bargeron
LM , Pacifico AD , Kirklin JW. Con genital pulmonary vein stenosis ‘ Am J Cardiol 1984; 54 :369
11. Belcourt CL , Roy DL , Nanton MA , Finley JP , Gillis DA , Krause VW , Aterman K. Stenosis of
individual pulmonary ve ins: Radiologic stucl y Raiology 1986 ; 16 1: 109
12. Adey CK , Soto B, Shin MS. Congeni tal pulmonary vein stenosis: A radiographic study Radiology 1986; 161 :113
13. Swischuk LE , L ’ Heureux PL. U nilateral Pulmonary vein atresia. AJR 1980 ;135:667
14. Heitzman ER. The lung: Radiologic-pathologic correlations , 2nd ed . The C.V.Mosby Company , St. Louis, 1984
15. Scheibel RL , Dedeker KL , Gleason DF , Pliego M , Kieffer SA. Radiographic ancl angiographic characteristics of pulmonary veno-occlusive di sease. Radiology 1972 ;103: 47 -51
16. Wagenvoort CA , Losekoot G , Mulder E Pulmonary veno-occlusive disease of presumably intrauterine origin. Thorax 197 1;26 :429
- 172-

Woo Sun Kim. et al : Radiological Evaluation of Congenital Pulmonary Vein Obstruction
17. Rosenthal A , Vawter G , Wagenovoort CA : ln
trapulmonary veno-occlusive disease. Ar샤 Car
diol 1973;3 1: 78
18. Calderon M , Burdine JA. Pulmonary veno
occlusive disease. J Nucl M ed 1973; 15:455
19 . Pajewski M , Reif R , Manor H , Starinsky R ,
K atzir D. Pulmonary veno-occlusive disease om
a unilateral hypertransradiant lung. Thorax
1981;36 ‘ 397
20. W agenvoort CA. Pulmonry veno-occlusive
d비IS않easeε: Ent냐tlty or syn벼dro아me라? Chest 1976;69:82
2있1. Shacklefo야r띠d GD , Sa값C이hs EJ , Mu띠l니11…liηins JD ,
M cAlister WH. Pulmonary veno-occlusive
disease:Case report and a rev iew of the
literature . AJR 1977 ;128:643-648
〈국문 요약〉
22. Lombard CM , Churg A , Winokur S.
Pulmonary veno-occlusive disease fo11owing
theraphy for m alignant neoplasms. Chest
1987:92-871
23. Budorick NE , M cdonald V , Flisak ME , Mon
cada RM. The pulmonary veins. Semin Roen
tgenol 1989;26: 127
24. Bisset GS II I. M agnetic R esonance lmaging of
congenital heart disease pediatric patients.
Radiol Clin North Am 1991 ;9 :279
25. M asui T , Seelos KC , Kersting-SommerhoffBA ,
Higgins CB. Abnormalities of the pulmonary
veins: Evaluation with MR imaging and com
parisoon with cardiac angiography and echocar
diography 1991 ; 181 : 645
선천성 폐정맥 폐쇄의 방사선학적 고찰
서울대학교 의과대학 방사선과학교실, 소아과학교실* 병리학교실*** 인제대학교 의과대학 병리학교실**
김우선 • 연경모 • 킴인원 • 윤용수* • 서연림** • 지제근***
폐정맥 폐쇄는 만성적 폐울혈과 폐동맥 고혈압을 초래할 수 있으며, 폐정맥 환류이상이 없는 선천성 폐정맥 폐쇄
에는 일측성 폐정맥 폐쇄증 또는 폐정맥 협착증이 포함된다. 저자들이 경험한 폐정맥 폐쇄 7례는 전례에서 우측 폐
정맥에 발생하였으며 l례는 양측성 이었다. 폐쇄 정도는 5례에서 완전폐쇄. 3례(양측성 1례 포함)에서는 부분폐쇄였
다. 5례는 다른 선천성 심장질환을 통반했다. 4례는 유아기부터의 재발성의 폐렴과 각혈이 주증상이었고 이들의 평
균 나이는 5세였다. 나머지 3례는 동반된 심장 질환으로 인한 증상이 주로 나타났다. 단순흉부촬영상 폐정맥 완전폐
쇄시는 동측의 일측성 폐용적 감소, 폐부종, 망상형 간질성병변, 늑막변화가 관찰되었다. 부분폐쇄의 경우는 정맥폐
쇄 부위 폐야의 폐정맥 확장이 주소견이었다. 폐관류 스캔 (n=3)상 폐정맥이 완전 폐쇄된 폐야는 완전관류 결손으로
나타났다. 심도자술(n=6)상 폐동맥 고혈압 소견이 전례에서 있었으며 부분폐쇄의 경우는 폐쇄원위부와 화심방 사이
에 혈압경사가 관찰되었다. 완전폐쇄의 경우 폐동맥 조영술상 병변측 폐동맥의 직경 감소와 원위부로 부터의 조영제
의 역류가 있었고, 말단 폐동맥이 조영되지 않아 “ dead tree" 모양이었으며. levo-phase에는 동측의 폐정맥이 전
혀 관찰되지 않았다. 대동맥 조영술(n=2)상 전신동맥 으로부터 폐동맥으로의 측부혈류가 관찰되었다. 부분폐쇄의
경우 이에 통반된 심방중격결손을 통한 우상 폐정맥조영술(n=2) 로 폐정맥협착이 관찰되었다. 자기공명영상(n=2)
소견상 2례의 폐정맥-좌심방 접합부위의 완전폐쇄와 1례의 막성 부분폐쇄가 관찰되었다(양측성 폐쇄 1례 포함) . 2
례에서수술과조직학적검사가시행되었고1 다른 2례는 심장수술중 폐정맥 폐쇄가 확인되었다. 폐정맥폐쇄 (특히 완전
폐쇄)는 특이한임상적, 방사선학적소견을보여증상과 단순흉부촬영 소견만으로도 이 질환의 가능성을 생각할 수 있
을 것으로 생각된다. 또한 자기공명영상은 폐정맥폐쇄의 진단에 매우 유용할 것으로 예상된다.
_ 1 '7('、


















![Chapter 11 [blood abnormalities n diseases]](https://img.pdfslide.tips/doc/110x75/5477db1fb4af9f7a0f8b45fd/chapter-11-blood-abnormalities-n-diseases.jpg)