-
高三酸甘油脂血症之臨床 意義與治療
Chau-Chung Wu (吳造中), M.D., Ph.D.
Department of Internal Medicine (Cardiology Section)National
Taiwan University Hospital
Taipei, Taiwan
-
Lipoproteins in Human Plasma
Correlation with Lipoprotein Major Lipid Atherosclerosis
Chylomicron TG No
VLDL TG Minimal
IDL TG
C Direct
LDL C Direct
HDL C Inverse
Lp(a) C Unclear
“Remnants” TG
C Direct
Dense LDL C Direct
Selected Characteristics
Relative Size of Plasma
Lipoproteins According to Their Hydrated Density
Braunwald: Heart Disease: A Textbook of Cardiovascular Medicine,
6th ed.,
-
Clinical event data Clinical
event data
Statin trialsStatin trials
The Evolution of Clinical Event Data
Non-Statin trialsNon-Statin
trialsCholesterolhypothesisCholesterolhypothesis
EpidemiologyEpidemiology
-
Very high cholesterol with CHD or MI
Moderate high cholesterol in high risk CHD or MI
Normal cholesterol with CHD or MI
High cholesterol with NO CHD or MI
No history of CHD or MI, average TC and LDL-C, but below average
HDL-C
4S
LIPID, PLAC I / II, KAPS, REGRESS
CARE
WOSCOPS
AFCAPS/TexCAPS
The Pyramid of Statin TrialsRelative Size of the Various
Segments
of the PopulationMIRACL, Risk-HIAAcute Coronary Syndrome
Low to moderate cholesterol without CHD or MI
ASCOT-LLT, CARDS
HPS
-
Trial WOSCOPS AFCAPS/ TexCAPS
HPS ASPEN 4S LIPID CARE TNTTotal
TNTMet S
TNTDiabetes
N 6.595 6.505 20.536 2.410 4.444 9.014 4.159 10.001 5.584
1.501
LDL-C -26% -27% -29% -29% -36% -25% -28% -21% -24% -20%
82%72%
80%75%75%
62%73%73%
62%69%
Results from statin outcome trials show the existence of
significant residual CV risk
Adapted from Libby P, J Am Coll Cardiol 2005;46:1225-1228
Res
idua
l Maj
or C
oron
ary
Eve
nts
(%)
-
Low HDL-C
High TG
Theatherogenic
triad
Atherogenic dyslipidemia - The atherogenic triad
Expert Panel on Detection, Evaluation,and Treatment of High
Blood Cholesterol in Adults JAMA 2001;285:2486-2497
High LDL-C
High sd LDL-C
-
0
1
2
3
4
Copenhagen Male StudyRelative risk for ischemic heart disease
(IHD) during8 years according to level of fasting TG
Rel
ativ
e R
isk
of IH
D
From: J. Jeppesen et. al. Circulation 97:1029-1036, 1998
1.01.5
2.2
TG Level (Thirds)
0.88(0.44-1.09)
78
1.33(1.10-1.59)
117
2.45(1.60-22.4)
217
(mmol/L)
(mg/dl)
P < .05
P < .001
Adjusted for:AgeLDL-CHDL-CAlcohol useTobaccoPhysical
activityBMISBP/DBPHTNNIDDMGlycosuriaLow social class
-
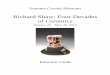
Prospective Cardiovascular Münster Study (PROCAM)
CHD Risk According to Triglycerides and LDL/HDL Cholesterol
Ratio
Inci
denc
e (p
er 1
,000
in 6
yea
rs)
Taken from Lipid Metabolism Disorders and Coronary Heart
Disease, G. Assmann, Editor, MMV Medizin Verlag, Munich 1993
Triglycerides< 200 mg/dl
LDL Cholesterol / HDL Cholesterol
0
50
100
150
200
250*
116
24 31
245
* This bar represents 5% of the subjects in which 25% of the CHD
events occurred.
Triglycerides
200 mg/dl
2.3 mmol/L)
5.0 > 5.0
-
Interrelation Between Atherosclerosis and Insulin Resistance
HypertensionHypertension
ObesityObesity
HyperinsulinemiaHyperinsulinemia
DiabetesDiabetes
HypertriglyceridemiaHypertriglyceridemia
Small, dense LDLSmall, dense LDL
Low HDLLow HDL
HypercoagulabilityHypercoagulability
Insulin Resistance
InsulinInsulin ResistanceResistance
AtherosclerosisAtherosclerosis
Atherosclerosis
-
(hepatic(hepatic lipase)lipase)
Mechanisms Relating Insulin Resistance and Dyslipidemia
Fat CellsFat Cells LiverLiver
KidneyKidneyInsulinInsulin
IRIR XX
(CETP)(CETP)
CECE
TGTG
Apo BApo B
VLDLVLDL
(CETP)(CETP)
VLDLVLDL HDLHDL
(lipoprotein or hepatic lipase)(lipoprotein or hepatic
lipase)
SDSD LDLLDLLDLLDL
TGTGApo AApo A--11
TGTGCECE
FFAFFA
-
Accumulation of chylomicron remnants
Accumulation of VLDL remnants
Generation of small, dense LDL-C
Association with low HDL-C
Increased coagulability
- plasminogen activator inhibitor (PAI-1)
- factor VIIc
- Activation of prothrombin to thrombin
Hypertriglyceridemia and CHD Risk: Associated Abnormalities
-
FirstFirst--line agentsline agents
HMG CoA HMG CoA reductasereductase inhibitorinhibitor
FibricFibric acid derivativeacid derivative
SecondSecond--line agentsline agents
Bile acid binding resinsBile acid binding resins
Nicotinic acidNicotinic acid
Pharmacologic Agents for Treatment of Dyslipidemia
American Diabetes Association. Diabetes Care 2000;23(suppl
1):S57-S60.
In diabetic patients, nicotinic acid should be restricted to
-
Action of Fibrate --- Activate PPARαto improve Lipid Profile1.
Activate LPL gene, LPL↑ , TG↓
2. Apo AI/AII↑, Hepatic secretion of HDL↑
3. Inhibit Apo CIII, VLDL → large LDL↑
-
Fenofibrate
Increased degradation of triglyceride-rich lipoproteins
PPAR
Increase of LPL gene expression
Triglycerides
Increased production
of LPL
Fenofibrate increases LPL gene expression
Decrease TG-rich lipoproteins
-
Lowering TG Effect
-60%
-50%
-40%
-30%
-20%
-10%
0%
S20 vs Feno M P20 vs Feno M A10 vs Feno M
% c
hang
e
StatinFenofibrate
Type IIB patients1 Type IIB patients2 Type IIB patients3
N = 45 N = 152 N = 84
1) Steinmetz A et al,J Cardiovasc Pharmacol 1996;27:563-570 2)
Ducobu J et al, J Cardiovasc Pharmacol, 2003; 41:60-67
3) Ooi TC et al, Arterioscler Thromb 1997; 17:1793-1799
P < 0.05P < 0.001 P < 0.0001
-
Fenofibrate to increase HDL
20
30
40
50
-
Qualitative effect of fenofibrate and atorvastatin on lipid
profile
Exp Clin Endocrinol Diabetes 2004, 112:241-247
Small dense LDL
P=0.028*
P=0.028*P=0.173 P=0. 753
-
Fibrate mechanisms of actionFibrate
PPAR
Reverse
cholesterol transport
LDL particle size
HDL synthesis
Inflammation
Triglycerides
-
Established role of fibratesRaising HDL & lowering TG
1. Rubins HB et al. N Engl J Med 1999;341:410–82. Frick MH et
al. N Engl J Med 1987; 317: 1237–453. Diabetes Atherosclerosis
Intervention Study Investigators. Lancet 2001; 357: 905–104. The
BIP Study Group. Circulation 2000; 102–21
VA-HIT1
-41% CHD Deathp = 0.02
BIP4
-29% MIp = 0.02
DAIS3
-23% CV EventsNS
HHS2
-78% CHDp = 0.002
HDL
TG
Sd-LDL
-
VA-HIT StudyLipid entrance criteria:Lipid entrance criteria:
HDL 40 mg/dl
LDL 140 mg/dl
TG 300 mg/dl
Endpoints:Endpoints:Primary endpoint: nonfatal MI or CHD
deathnonfatal MI or CHD deathSecondary endpoint: death, stroke and
other CV death, stroke and other CV
events / proceduresevents / proceduresRubins HB, et al. N Engl J
Med 1999 Aug 5;341(6):410-8
-
VA-HIT Study% change in lipid at 1 year% change in lipid at 1
year
Gemfibrozil Group Placebo GroupPlacebo Group
TC TC 2.8 %2.8 % 2.1 %2.1 %
HDL HDL 7.5 % 7.5 % 1.8 %1.8 %
TG TG 24.5 %24.5 % 9.6 %9.6 %Rubins HB, et al. N Engl J Med 1999
Aug 5;341(6):410-8
-
VA-HIT - Mean On-treatment Lipid Levels
171
116
32.5
176170
115
34.5
122
0
20
40
60
80
100
120
140
160
180
200
TC LDL-C HDL-C TG
Mea
n Pl
asm
a Le
vel (
mg/
dL) Placebo
Gemfibrozil
*P< 0.001, difference betweentreatment and placebo groups
*
*
*
-
VA-HIT StudyPrimary Endpoints by Treatment GroupPrimary
Endpoints by Treatment Group
PlaceboPlacebo Gemfibrozil RRR%RRR% 95%CI95%CI P valueP
valuen=1267 n=1267 n=1264
CHD death/Nonfatal MI 274 (21.6%) 219 (17.3%) 22 7~35 0.005
CHD death CHD death 118 (9.3%) 93 (7.4%) 118 (9.3%) 93 (7.4%) 22
--2~41 0.0732~41 0.073
Nonfatal MI 183 (14.4%) 145 (11.6%) 183 (14.4%) 145 (11.6%) 22
3~37 3~37 0.024
Rubins HB, et al. N Engl J Med 1999 Aug 5;341(6):410-8
-
Downs et al: JAMA 1998;279:1615–1622
Risk Reduction in a Population With Low HDL-C:
AFCAPS/ TexCAPS—Study Design
6605 men and women without CHD
Cholesterol 4.7–6.8 mmol/L (182–263 mg/dL)
HDL-C
-
–32% –33%
–0
–10
–20
–30
–40
–50
Downs et al: JAMA 1998;279:1615–1622
Risk Reduction in a Population With Low HDL-C: AFCAPS/TexCAPS
—
Results Summary
All risk reductions are P
-
Effect of Treatment on Lipids and Fibrinogen in BIP Study
(The BIP Study Group, Circulation. 2000;102:21.)
http://circ.ahajournals.org/content/vol102/issue1/images/large/hc2604227001.jpeg
-
Cumulative probability of the primary end point in BIP Study
(The BIP Study Group, Circulation. 2000;102:21.)
http://circ.ahajournals.org/content/vol102/issue1/images/large/hc2604227003.jpeg
-
Trial VA-HIT BIP AFCAPS/TexCAPS
Drug Gemfibrozil Bezafibrate LovastatinIndication 2nd prevention
2nd prevention 1st preventionDuration (years) 5.2 6.2 5.2Primary
endpoint Non-fatal MI/CAD deathMI/sudden death 1st major
coronaryPatient characteristicsAge (years) 64 60 58No. (men/women)
2531/0 2825/265 5608/99Diabetes (%) 25 10 3Hypertension 57 32
22Current smokers (%) 20 12 12Total cholesterol (mmol/1) 4.5 5.6
5.7Triglyceride (mmol/1) 1.8 1.6 1.8LDL cholesterol (mmol/1) 2.9
3.9 3.9HDL cholesterol (mmol/1) 0.8 0.9 0.9Outcome variablesTotal
cholesterol -6 -4 - 18TriglyceHde (%) -31 - 21 - 15LDL cholesterol
-4 -6 - 25HDL cholesterol +6 +18 +6RR red. in 1st endpoint (%) - 22
-9 - 37AR red. in 1st endpoint (%) -4.4 -1.4 -4.1NNT to prevent
event 23 a 24
Comparison of recent clinical endpoint trials employing a
fibrate in patients with low plasma HDL cholesterol levels
-
Comparison of Baseline Lipids in Secondary Prevention Trial
LDL-C (mg/dl) HDL-C (mg/dl)
190 4S 4745
170 4341
150 LIPID CARE 39LIPID 37
130 CARE BIP 3533
110 VA-HIT VA-HIT 31
4S
Rubins HB, et al. N Engl J Med 1999 Aug 5;341(6):410-8
AFCAPS/TexCAPS
-
Kaplan-Meier curves for the
primary end point in subgroups of
patients with baseline TG < 200 and > 200 mg/dL.
(The BIP Study Group, Circulation. 2000;102:21.)
http://circ.ahajournals.org/content/vol102/issue1/images/large/hc2604227005.jpeg
-
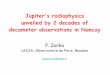
Helsinki Heart Study – baseline triglycerides and HDL-C
HDL-C
42 mg/dlHDL-C
42 mg/dl
CH
D in
cide
nce
per 1
000
pers
on –
year
s
Triglycerides (mg/dL)Manninen et al. Circulation 1992;85:37
20
16
12
8
4
0
200 > 200
200 > 200
GemfibrozilPlacebo
-
Minimum lumendiameter
0.00
-0.02
-0.04
-0.06
-0.08
-0.10
mm
-40%
Prog
ress
ion
of C
AD
Prog
ress
ion
of C
AD
Lancet 2001; 357: 905-910
% Change
Percent stenosis
4.00
2.00
0.00
-42%
Mean Segment Diameter
0.00
-0.02
-0.04
-0.06
-0.08
-0.10mm
-25%
p = 0.029p = 0.029 p = 0.020p = 0.020 p = 0.171p = 0.171
PlaceboFenofibrate
Fenofibrate treatment decreases theprogression of
atherosclerosis in type 2
diabetic patients
-
Trial nMajor CVD event rate (%)
RRR (%) p-Valuecontrol drug
Primary prevention
HHS1Overall: 4,081 41.4 27.3 34
-
FIELD: Fenofibrate Intervention and Event Lowering in
Diabetes
Randomized, double-blind, international studyPatients with Type
2 diabetesage: 50 – 75 yearshigh risk of CHD (n = 8500)primary and
secondary prevention
Comparison of treatment with fenofibrate or placebo (average 5
years treatment)Principal study outcome: the effect of lipid
modification, by micronized fenofibrate,
on CHD mortality among all randomized patients
-
9,795 Patients
Fenofibrate 200 mg/day, n = 4,895
Placebo, n = 4,900
Average Follow-up:
5 Yearsand 500
CHD Events
FIELD Study Investigators. Lancet 2005, e-publication November
14
Study Design5-year double blind, placebo controlled study
against a background of usual care, including the option to add
other lipid-modifying therapies
-
Results: compliance and statin use
Drop-outsHR = 1.01
95% CI = (0.93 –1.11)p=0.76
Drop-insHR = 0.47
95% CI = (0.44 – 0.51)P
-
-6.9% -5.8%
-21.9%
1.2%
-30
-25
-20
-15
-10
-5
0
5
10
TC LDL-C HDL-C TG
Per
cent
age
Cha
nge
From
Bas
elin
e at
clo
se o
ut(c
orre
cted
for p
lace
bo e
ffect
)
Lipid Effects of Fenofibrate at Study Close (full cohort)
-
Primary End Point : CHD Events (Non fatal MI + CHD Death)
Years from randomisation
Cum
ulat
ive
risk
(%)
0 1 2 3 4 5 6
0
2
4
6
8
10
Placebo 4900 4835 4741 4646 4547 2541 837Fenofibrate 4895 4837
4745 4664 4555 2553 850
PlaceboFenofibrate
HR = 0.8995% CI = (0.75 – 1.05)
p=0.16
-
Outcomes adjusted for statin useFenofibrate Treatment Effect
Relative Risk Reduction (95% CI)
P
CHD EventsUnadjusted 11% (-5 to 25) 0.16Adjusted for statin use*
19% (4 to 32) 0.01
Total CVD EventsUnadjusted 11% (1 to 20) 0.035Adjusted for
statin use* 15% (5 to 24) 0.004* Non-randomised comparison
adjusting for on-study statin use
-
Scott R et al Circulation 2007;116:II-838 Abstract 3691*HDL-c:
200 mg/dL
17.8
13.5
0.74(0.59-0.92)
P=0.01
Highest therapeutical benefit of fenofibrate in patients with
elevated TG and low HDL cholesterol
(FIELD study)
-
PControl
-
Risk Reduction (%)0 5 10 15 20 25 30 35
Albuminuria
Retinopathy
Fenofibrate: Effective on Microvascular and Peripheral Vascular
Disease
Effects independent of the degree of glycemic control
(HbA1c),concomitant medications or reduction in blood pressure!
15%P =0.002
30%P
-
1,450 1,450
1,450 1,450
ACCORD: NIH/NHLBI Trial Action to Control CardiOvascular Risk in
Diabetes
Simvastatin 20 mg
Intensive glycemic control
Standard glycemic control
Does a therapeutic strategy that targets HbA1c < 6% reduce
the rate of CVD compared with a target of < 7.5%?
Does combination therapy with a fibrate plus a statin reduce CVD
more than statin therapy alone?
http://www.clinicaltrials.gov/ct/gui/show
Simvastatin 20 mg + Fenofibrate 160 mg
-
140
150
160
170
180
190
200
0 1 2 3 4 5 6 7
mg/
dl
Years Post-Randomization
Mean Total Cholesterol
FenoPlacebo
N = 5483 5180 4988 4783 5250 3377 1668 491
60
70
80
90
100
110
120
0 1 2 3 4 5 6 7
mg/
dl
Years Post-Randomization
Mean LDL-C
FenoPlacebo
N = 5483 5180 4988 4783 5250 3377 1668 491 N = 5483 5180 4988
4783 5250 3377 1668 491 N = 5483 5180 4988 4783 5250 3377 1668
491
37
38
39
40
41
42
0 1 2 3 4 5 6 7
mg/
dl
Years Post-Randomization
Mean HDL-C
FenoPlacebo
N = 5483 5180 4988 4783 5250 3377 1668 491 N = 5483 5180 4988
4783 5250 3377 1668 491
110
120
130
140
150
160
170
0 1 2 3 4 5 6 7
mg/
dl
Years Post-Randomization
Median Triglycerides
FenoPlacebo
N = 5432 5180 4988 4783 5250 3377 1668 491
ACCORD Lipid Profile
-
ACCORD Study
-
Primary Outcome By Treatment Group and Baseline Subgroups
-
Primary Outcome By Treatment Group and Baseline Subgroups
-
Trial(Drug)
Primary Endpoint: Entire Cohort (P-value)
Lipid Subgroup Criterion
Primary Endpoint: Subgroup
HHS (Gemfibrozil) -34% (0.02)
TG > 200 mg/dlLDL-C/HDL-C > 5.0 -71%
BIP (Bezafibrate) -7.3% (0.24)
TG > 200 mg/dl-39.5%
FIELD(Fenofibrate) -11% (0.16)
TG > 204 mg/dlHDL-C < 42 mg/dl -27%
ACCORD(Fenofibrate) -8% (0.32)
TG > 204 mg/dlHDL-C < 34 mg/dl -31%
-
Niacin (Nicotinic Acid)
83
-
The Nicotinic Acid Receptor GPR109A (PUMA-G or HM74A)
86
-
87
-
Combination Niacin Extended-Release/ Lovastatin vs Monotherapy
with Atorvastatin or
SimvastatinPercent Change from Baseline
Week 8 Week 12Niacin ER/L 1000/40 mg A 10 mg
Niacin ER/L 1000/40 mg S 20 mg
LDL-C –39%* –38% –42%* –35%HDL-C +20%** +3% +19%**
+8%Triglyceride –30%** –20% –36%** –15%Lipoprotein(a) –16%** +5%
–20%** –1%
Bays H et al. Am J Cardiol 2003;91:667-672.
**P
-
P
-
ARBITER 6–HALTS TrialThe patients who had CAD or equivalent, who
were receiving long-term statin therapy, and in whom an LDL- C
-
Mean Percent Changes in Cholesterol and Triglyceride Levels over
the 14-month Study Period among the 208
Patients Who Completed the Study
Taylor, et al. N Engl J Med 2009;361.
-
Changes in the Mean Carotid Intima–Media Thickness over the
14-Month Study Period
Taylor, et al. N Engl J Med 2009;361.
-
Conventional WisdomTreatment Assumptions in CAD Mx:1. Patients
with symptomatic CAD and
chronic angina who have significant coronary stenoses “need”
revascularization
2. Revascularization is required to improve prognosis
3. PCI is less invasive than CABG surgery (i.e., is safer) and,
therefore, should be selected.
-
Stable CAD: PCI vs Conservative Medical ManagementMeta-analysis
of 11 randomized trials; N = 2,950
DeathCardiac death or MI
Nonfatal MICABG
PCI
Katritsis DG et al. Circulation. 2005;111:2906-12.
0 1 2
P
0.680.280.120.820.34
Risk ratio(95% Cl)
Favors PCI Favors Medical Management
-
PCI + Optimal Medical Therapy
will be Superior to
Optimal Medical Therapy Alone
Hypothesis of COURAGE Study
-
Survival Free of Death from Any Cause and Myocardial Infarction
(COURAGE)
Number at RiskMedical Therapy 1138 1017 959 834 638 408 192
30PCI 1149 1013 952 833 637 417 200 35
Years0 1 2 3 4 5 6
0.0
0.5
0.6
0.7
0.8
0.9
1.0
PCI + OMT
Optimal Medical Therapy (OMT)
Hazard ratio: 1.0595% CI (0.87-1.27)P = 0.62
7
-
Optimal Medical Therapy in COURAGEPharmacologic
Anti-platelet: aspirin; clopidogrel in accordance with
established practice standardsLipid-lowering agents: simvastatin
±
ezetimibe or ER niacin ±
fenofibrateACE Inhibitor or ARB: lisinopril or
losartanBeta-blocker: long-acting metoprololCalcium channel
blocker: amlodipineNitrate: isosorbide 5-mononitrate
Applied to Both Arms by Protocol and Case-Managed
-
Published NEJM 11/15/2011 (online)Published NEJM 11/15/2011
(online)
-
AIMAIM--HIGH TrialHIGH TrialAAtherothrombosistherothrombosis
IIntervention in ntervention in MMetabolic Syndrome with Low
etabolic Syndrome with Low
HHDL/High Triglycerides and DL/High Triglycerides and IImpact
onmpact on GGlobal lobal HHealth Outcomesealth Outcomes
-
Adjust simva to LDL 40 – 80
mg/dL
Adjust simva to LDL 40 – 80
mg/dL
Study DesignStudy Design
Months Relative to RandomizationMonths Relative to
Randomization--22 --11 00 11 22 33 66 1212
Open-Label Run- In: Up-Titrate Niacin from 500mg to
2,000mg/day
4-8 weeks
Open-Label Run- In: Up-Titrate Niacin from 500mg to
2,000mg/day
4-8 weeksFollow to end
of study
Follow to end
of study
ER Niacin ER Niacin + 40+ 40--80 mg/day 80 mg/day
simvastatinsimvastatin
PlaceboPlacebo + 40+ 40--80 mg/day 80 mg/day
simvastatinsimvastatin
R
-
HDLHDL--C at Baseline & FollowC at Baseline &
Follow--upup
*
-
Triglycerides at Baseline and FollowTriglycerides at Baseline
and Follow--upup
-
LDLLDL--C at Baseline & FollowC at Baseline &
Follow--upup
P < 0.001 *
-
Time (years)Time (years)
Cum
ulat
ive
% w
ith P
rimar
y O
utco
me
Cum
ulat
ive
% w
ith P
rimar
y O
utco
me
00
1010
2020
3030
4040
5050
00 11 22 33 44
MonotherapyMonotherapyCombination TherapyCombination Therapy
HR 1.02, 95% CI 0.87, 1,21HR 1.02, 95% CI 0.87, 1,21LogLog--rank
P value= 0.79rank P value= 0.79
N at riskN at riskMonotherapyMonotherapy
Combination TherapyCombination Therapy
1696169617181718
1581158116061606
1381138113661366
910910903903
436436428428
Primary OutcomePrimary Outcome
16.2%
16.4%
-
Wei‐Hsian Yin, Chau‐Chung Wu, Jaw‐Wen Chen, on behalf of
the T‐SPARCLE Registry Investigators
Taiwanese Secondary Prevention for
patients with AtheRosCLErotic
disease (T‐
SPARCLE) Registry (2009‐2011)
-
AIM of The Study
The study attempts to register and follow up a large
population of patients receiving
secondary prevention therapy for the CVD
to define the current status of lipid lowering therapy in
Taiwan
the effects of lipid‐lowering therapy on CVD morbidity
and mortality during a follow up of 5 years.
Outcome study in relation to lipid control in Taiwan
insufficient !!
-
Inclusion criteriaMale or female patients with stable symptomatic atherosclerotic
diseases aged > 18 years. The definition of coronary atherosclerosis: (1) the presence of
significant coronary artery occlusion of >50% in diameter by cardiac
catheterization examination, (2) having history of myocardial
infarction (MI) as evidenced by ECG or hospitalization, or (3) angina
patient showing ischemic ECG changes or positive response to stress
test.
Cerebral vascular disease, defined as: cerebral infarction, intra‐
cerebral hemorrhage (excluding intra‐cerebral hemorrhage associated
with trauma or other diseases), and transient ischemic attack whose
carotid artery ultrasound confirms atheromatous
change with more
than 70% blockage. Peripheral atherosclerosis with symptoms of ischemia and confirmed
by Doppler ultrasound or angiography.
-
T‐SPARCLE 參加研究中心分布圖
新北市
北榮(603)
振興(602)
台大(507)
馬偕(474)
北市醫 ‐
仁愛(110)
北市醫 –
和平(106) 林長(110)
中榮(300)中山(115)
成大(665)
市南(317)
高醫(300)
義大(221)
亞東(131)
14 Centers4,561 patients
3,486 eligible for
analysis
-
Patient characteristics and biochemistry
124
Factors Mean
Mean systolic BP (N=3,264) 133 mmHg
Mean diastolic BP (N=3,240) 76 mmHg
Mean pulse rate (N=2,607) 75 bpm
Mean waist (N=3,110) 94 cm
Mean hip (N=3,034) 101 cm
Mean WHR (N=3,038) 0.93
Mean height (N=3,329) 163 cm
Mean weight (N=3,357) 70 kg
Factors Mean
Total choleterol (N=3,486) 175 mg/dL
HDL cholesterol (N=3,486) 46 mg/dL
LDL cholesterol (N=3,486) 101 mg/dL
Triglycerides (N=3,486) 140 mg/dL
AC sugar (N=3,080) 118 m/dL
HbA1c (N=1,750) 7.3%
Creatinine (N=3,057) 1.13 mg/dL
GPT (N=2,695) 29 mg/dL
CPK (N=1,450) 132 mg/dL
-
Proportion of patients
attaining their lipid goals
%
-
126
Treatment to the Target by Drugs (I)
-
127
Multivariate Analysis of Factors Associated with LDL Target
Achievement
-
128
Multivariate Analysis of Factors Associated with TG Target
Achievement
-
Management of High TGPrimary Management
Control underlying conditions (ex. Hypothyroidism, DM, Nephrotic
syndrome, Chronic liver disease, Cushing’s syndrome, etc.)
Control body weightInstitute diet (increase the ratio of
MUFA/SFA and complex CH2 O)Institute regular exerciseRestrict
alcohol in selected patientsAvoid concurrent agents that increase
TG (b-blocker, estrogen,
steroids, and diurectics)Drug Therapy
Fibrate: Helsinki, VA-HIT, BIP, DAIS, FIELD, UKLDS
StatinNicotinic acidn-3 free fatty acid (fish oil)Combination
therapyThe indications for the proper use of these drugs have not
been
satisfactorily defined.
-
謝謝聆聽謝謝聆聽敬請賜教敬請賜教
chauchungwu@[email protected]
高三酸甘油脂血症之臨床意義與治療 Lipoproteins in Human PlasmaThe Evolution
of Clinical Event Data投影片編號 7Benefits of lowering LDL投影片編號
9Atherogenic dyslipidemia �- The atherogenic triadCopenhagen Male
StudyProspective Cardiovascular �Münster Study
(PROCAM)Interrelation Between Atherosclerosis and Insulin
ResistanceMechanisms Relating Insulin Resistance and
DyslipidemiaHypertriglyceridemia and CHD Risk: Associated
AbnormalitiesPharmacologic Agents for Treatment of
DyslipidemiaAction of Fibrate --- Activate PPARαto improve Lipid
ProfileFenofibrate increases LPL gene expressionLowering TG
EffectFenofibrate to increase HDLQualitative effect of fenofibrate
and �atorvastatin on lipid profileFibrate mechanisms of action投影片編號
48VA-HIT StudyVA-HIT Study投影片編號 51VA-HIT StudyRisk Reduction in a
Population �With Low HDL-C: �AFCAPS/ TexCAPS—Study DesignRisk
Reduction in a Population With �Low HDL-C: AFCAPS/ TexCAPS
—�Results Summary投影片編號 55投影片編號 56投影片編號 57投影片編號 58投影片編號 59Helsinki
Heart Study –�baseline triglycerides and HDL-C投影片編號 61投影片編號
62FIELD: Fenofibrate Intervention and Event Lowering in
DiabetesStudy DesignResults: compliance and statin use投影片編號
66Primary End Point : CHD Events �(Non fatal MI + CHD Death)
Outcomes adjusted for statin use投影片編號 71投影片編號 72Fenofibrate:
Effective on Microvascular and Peripheral Vascular DiseaseACCORD:
NIH/NHLBI Trial Action to Control CardiOvascular Risk in
Diabetes投影片編號 77投影片編號 79投影片編號 80投影片編號 81投影片編號 82Niacin (Nicotinic
Acid)The Nicotinic Acid Receptor GPR109A (PUMA-G or HM74A)投影片編號
87Combination Niacin Extended-Release/ Lovastatin vs Monotherapy
with Atorvastatin or SimvastatinCombination Niacin
Extended-Release/Lovastatin Compared with Statin AloneARBITER
6–HALTS TrialMean Percent Changes in Cholesterol and Triglyceride
Levels over the 14-month Study Period among the 208 Patients Who
Completed the StudyChanges in the Mean Carotid Intima–Media
Thickness over the 14-Month Study PeriodConventional WisdomStable
CAD: PCI vs Conservative�Medical Management投影片編號 97Survival Free of
Death from Any Cause and Myocardial Infarction (COURAGE)投影片編號
101Published NEJM 11/15/2011 (online)AIM-HIGH TrialStudy
DesignHDL-C at Baseline & Follow-upTriglycerides at Baseline
and Follow-upLDL-C at Baseline & Follow-up投影片編號 114投影片編號 120AIM
of The StudyInclusion criteriaT-SPARCLE 參加研究中心分布圖Patient
characteristics and biochemistryProportion of patients �attaining
their lipid goals投影片編號 126投影片編號 127投影片編號 128Management of High
TG投影片編號 130