Embed Size (px)
Citation preview

Endocrinol. Japon. 1990, 37 (2), 247-254
Tumor Markers and Oncogene Expression in Thyroid Cancer usingBiochemical and Immunohistochemical Studies
TAKUMA HASHIMOTO1, FUJITSUGU MATSUBARA1, YUJI MIZUKAMI2,
ITSUO MIYAZAKI3, TAKATOSHI MICHIGISHI4 AND
NOBORU YANAIHARA5
1Departments of Laboratory Medicine, 2Pathology, 3Surgery and 4Nuclear Medicine,Kanazawa University School of Medicine, Kanazawa 920, Japan,
5Shizuoka College of Pharmacy ,Shizuoka 422, Japan
Abstract
In 111 thyroid cancer patients consisting of 89 papillary carcinomas, 17follicular carcinomas, 2 medullary carcinomas, 1 squamous cell carcinomaand 2 malignant lymphomas, the levels of 12 tumor markers, including thyro-globulin (Tg), were measured in the serum by radioimmunoassay and radio-immunoassay related methods. Serum levels of Tg were elevated in 58.6%,those of CA-M26 in 15.7%, CA 19-9 in 5.3%, CT in 3.6%, NSE in 3.6%,CA 15-3 in 2.6%, CA 125 in 2.6%, CEA in 0.9%, CA-M 29 in 0%, ferritinin 0%, SCC in 0% and AFP in 0% of cases.
Among the patients, there was a case of thyroid carcinoma secretingthyroglobulin and CA 19-9, both of whose titer decreased after surgery.
Immunohistochemical studies were carried out on 57 of the above mentionedpatients plus 6 anaplastic carcinomas, 15 adenomas, 5 adenomatous goiters, 6Hashimoto's thyroiditis, 15 Graves' disease and 15 normal subjects. CA 19-9was positive in 58% of the papillary carcinomas, EGF in 73% of papillarycarcinomas, 67% of anaplastic carcinomas, and 33% of follicular carcinomas,while EGF-R was found in 73% of the papillary carcinomas, and 33% ofthe follicular carcinomas. Enhanced expression of ras p 21 oncogene and (c-myconcogene) was demonstrated in 100% (100%) of anaplastic carcinomas, in 100%(67%) of follicular carcinomas and in 63% (90%) of papillary carcinomas.
Our results indicate that a better tumor marker is required and moreextensive molecular oncology research should be pursued.
In the last 5 years, various tumor markers
have been developed and introduced into
the clinical field. However, little infor-
mation has been published on the valueof these markers in the detection of thyroidcancer. In order to acertain their re-liability or usefulness in the diagnosis ofthyroid cancer, we have evaluated 12 tumormarkers employing 10 commercially availablekits and 2 newly developed kits (CA-M 26,CA-M 29).
Receeived November 22, 1989
Address request for reprints to: TAKUMA
HASHIMOTO, M. D. Kanazawa University
School of Medicine 13-1, Takara-machi, Kana-
zawa, Ishikawa, 920 Japan.

248 HASHIMOTO et al.Endocrinol. Japon.April 1990
So far, thyroglobulin (Tg) measurementby radioimmunoassay (RIA) has been solelyemployed for the detection and post-operative monitoring of patients with thyroidcancer. However, increased concentrationsof Tg have also been seen in many thyroidaldiseases, other than differentiated thyroidcarcinoma (Botsch et al., 1983; Madedduet al., 1985). RIA of Tg has often been
jeopadized by the presence of and-thy-roglobulin antibody in the patient's serum.Thus, serum Tg is not a sufficiently reliableindicator in the diagnosis and follow-up ofdifferentiated thyroid cancer, particularlywhen the patients have anti-thyroglobulinantibodies in their serum as in Graves'disease or chronic thyroiditis (Uller andVan Herle, 1978; Schneider and Pervos,1978). A better tumor marker is urgentlyrequired.
In addition to the detection of tumormarkers in serum, we have examined thetissue expression of those tumor markers,as well as the expression of oncogenes,by immunohistochemical procedures. Ourreasons for this were that overexpressionof several oncogenes has been described invarious cancers (Channing, 1987) and thereare suggestions that oncogenes and their
products may be present in the early stagesof carcinogenesis (Czerniak et al., 1989) butare not detectable in the serum.
Materials and Methods
One hundred eleven patients with variousthyroid cancers were studied: 89 papillarycarcinomas, 17 follicular carcinomas, 2 medul-lary carcinomas, 1 squamous cell carcinomaand 2 malignant lymphomas. None of the
patients had any other malignant or non-malignant diseases, Nor any clinical laboratoryevidence of hepaic, gastrointestinal or pancreaticdiseases.
Serum levels were measured for carci-noembryonic antigen (CEA), a-fetoprotein (AFP)and squamous cell carcinoma antigen (SCC) with
Dainabot kits (Dainabot Co. Japan); thy-
roglobulin (Tg), neuron specific enolase (NSE)
and calcitonin (CT) with EIKEN kits (EIKEN
ICL Japan); carbohydrate antigens (CA 19-9,
CA 15-3, CA 125, with Centocor kits (distributed
by Fujirebio INC. Japan); carcinoma-associated
mucin antigens (CA-M26, CA-M29 [generous
gifts from Dr. P. S. Linsley]): and ferritin using
a LPIA (DIA-IATRON Co. Japan) in patients
with thyroid carcinoma. These tumor markers
were measured by radioimmunoassay or enzyme
immunoassay. The normal ranges of these tumor
markers were described previously (Hashimoto
et al., 1986; Linsley et al., 1988; Hashimoto
et al., 1989). Serum was separated by centri-
fugation at 4°C and stored at-20•Ž until the
assay was undertaken. All the samples were
measured in the same assay run in order to
avoid interassay variations. The significance of
the differences between the mean values was
evaluated by Student t-test.
Immunohistochemical staining was carried
out on tissue obtained from 57 of the patients
previously mentioned: 39 papillary carcinomas,
16 follicular carcinomas, 1 medullary carcinoma
and 1 squamous cell carcinoma. In addition, 6
anaplastic carcinomas, 15 adenomas, 5 ade-
nomatous goiters, 6 Hashimoto's thyroiditis, 15
Graves' disease, and 15 normal thyroids obtained
from lobes opposite to thyroid adenoma, were
also studied. Routinely formalin-fixed and
paraffin-processed material and the avidin-
biotin-peroxidase complex (ABC) technique were
used as previously described (Mizukami et al.,
1988). Antisera to Tg, CT and CEA (Immulok,
Corp. U. S. A.), CA 19-9, and CA 125 Centocor
Co. U. S. A.) were purchased.
The expressions of the ras p21 and c-myc
oncogene were evaluated with the monoclonal
antibody RAP-5 (a generous gift from Dr. H.
Schlom) and the polyclonal antibody produced
by Dr. N. Yanaihara, respectively. The im-
munohistochemical staining of epidermal growth
factor (EGF: Wakunaga Pharmaceutical Co.
Japan) and its receptor (EGF-R: Transformation
Research Inc. Japan) were performed with
commercially available reagents.
Case Report
A 73-year-old female noticed a swelling
on the right side of her neck in Decemcer,

Vol.37, No.2 TUMOR MARKERS AND ONCOGENE EXPRESSION 249
1987. She did not seek medical help until
she came to our outpatient's clinic in
March, 1988, when we diagnosed thyroid
cancer. She was then admitted for surgery.
On examination prior to surgery, there wasno evidence of hepatic, pancreatic or gall
bladder disease. Her serum level of CA
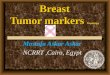
19-9 was as high as 78.1 U/ml. After hertotal thyroidectomy, the subsequent CA 19-9levels dramatically decreased to within thenormal range (Table 1). In the immuno-histochemical study, intense CA 19-9 stain-ing was found in the cytoplasm of the
papillary adenocarcinoma of thyroid (Fig. 2).
Table 1. Changes in serum tumor marker levels in a patient with undifferentiated thyroid
carcinoma with squamous cell metaplasia before and after total thyroidectomy.
Note: the consistency within normal levels in the serum levels of SCC both pre- and post-
operation in the patient with squamous cells carcinoma while Tg levels demonstrated
dramatical changes after total thyroidectomy.
Fig. 1. In follicular cells of papillary carcinoma of the thyroid CA 19-9 is stained intensively.
(•~200)

250 HASHIMOTO et al.Endocrinol. Japon.April 1990
Table 2. Serial analysis of Thyroglobulin (Tg) and CA 19-9 in a patient with CA19-9-producing thyroid cancer
Note: parallel patterns in serum concentrations of Tg and CA 19-9 both pre- and post-
operation
Because there were no other CA 19-9
producing diseases in evidence, weconcluded that this was a very rare
case of CA 19-9 producing thyroid
cancer.
Results
RESULT 1: BiochemicalResults
Serum levels of Tg were elevatedin 58.6%, CA-M26 in 15.7%, CA19-9 in 5.3%, CT in 3.6%, NSEin 3.6%, CA 15-3 in 2.6%, CA 125in 2.6%, CEA in 0.9%, CA-M29 in0%, ferritin in 0%, SCC in 0% andAFP in 0% of cases. One patientwith squamous cell carcinoma showednormal levels of SCC in the bio-chemical studies before and after totalthyroidectomy (Table 1).
RESULT 2: Immunohistochemical Results
In the immunohistochemical stu-dies, CA 19-9 positive staining wasobserved in 58% of papillary carci-nomas (Fig. 1, Table 2). No patientshowed positive CA 125 or CA 15-3staining.
On patient with a minute medul-lary carcinoma of the thyroid gland (0.5 cmin a diameter) showing negative serum CEAand CT levels (serum CEA level was <1.0ng/mg, and CT level was as low as 38pg/ml), demonstrated clear positive staining of
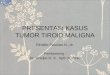
Fig. 2. Staining of EGF (bottom) and EGF-R (upper)
in papillary circinoma of the thyroid.(•~200)
CT and CEA in the immunohistochemicalstudy.
Of the patients studied, strong stainingof EGF in the cytoplasm of thyroid cancerswas found in 73% of paillary cancers

Vol.37, No.2 TUMOR MARKERS AND ONCOGENE EXPRESSION 251
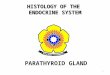
Fig. 3. Intense staining with ras p 21 oncogene is apparent in most tumor cells, characterized
mainly by diffuse cytoplasmic staining and apical luminal surface staining. (•~200)
Fig. 4. Enhanced c-myc expression is observed in the cytoplasm of papillary thyroid
carcinoma. (•~200)

252 HASHIMOTO et al,Endocrinol. Japon.April 1990
(Fig. 2), 67% of anaplastic carcinomas and33% of follicular carcinomas. Intensestaining of EGF-R was found in 73% inthe papillary carcinomas of the thyroid
(Fig. 2), 67% of anaplastic carcinomas and33% of follicular carcinomas, althoughnegative staining was found in the normalthyroid glands or follicular cells of Graves'disease.
As shown in Fig. 3, intense expressionof the ras p21 oncogene was demonstratedin the apical cell surface and cytoplasm of
papillary carcinoma (Fig. 3). Frequency ofthe enhanced expression of ras oncogenewas demonstrated in 100% of follicullarcarcinomas, 100% of anaplastic carcinomasand 63% of palliary carcinomas.
Enhanced c-myc expression was observedin the cytoplasm in 90% of the papillarythyroid carcinomas (Fig. 4), 100% in ana-
plastic carcinomas and 67% in follicularcarcinomas. C-myc gene amplification wasalso observed 100% in Graves' disease.
Discussion
Our present results indicate that thetwelve commercially available RIA kitswhich we studied are not sensitive enoughfor the early detection of thyroid cancer.Only serum levels of Tg and CA-M26were elevated in 58.6% and 15.7% ofcases respectively. Since increased con-centrations of serum Tg have been observedin both thyroid diseases and in thyroidcarcinoma, recent investigations have focusedon exploring a cancer specific Tg structure,in order that an and Tg monoclonal anti-body can be prepared (Kim, Dunn andDunn, 1988; Kohno et al., 1985).
CA-M26 is known to be a reliablemarker for breast cancer (Linsley et al., 1988).We applied it to thyroid cancer and foundthat it is also a fairly good marker for this
purpose. If further studies were directedtowards producing monoclonal antibodies
to recognize different epitopes of mucinsaround CA-M26, successful results might beanticipated. Furtheremore, it is well knownthat about 30% (SD 10%) of all thyroidcancer patients have anti-Tg antibodies
(Bayer and Kriss, 1979) which falsely in-crease or depress Tg values (Schneider andPervos, 1978). Therefore, research into theuse of mucin glycoproteins such as CA-M26as a tumor marker for thyroid cancersshould be pursued.
SCC is reported to be a sensitive tumormarker for squamous cell carcinoma. Weencountered a typical case of squamous cellcarcinoma of the thyroid gland. Contraryto our expectations, we found SCC insensi-tive in our case. The difference betweenthese results may depend on the organdifference or on the stage of the carci-noma.
Although Ohtani et al. (Ohtani et al.,1988) reported NSE was a good tumormarker of medullary thyroid carcinoma,NSE and ferritin estimations have no valuein the diagnosis of thyroid cancer, asreported by Touitou (Touitou and Heshmati,1982).
According to our results then, since sofar as no single one, nor any combinationof the tested tumor markers could con-sistently diagnose thyroid cancer, furtherstudies directed towards producing a specificthyroid tumors marker with monoclonalantibodies should be pursued.
In the course of this study, a case ofCA 19-9-producing papillary carcinoma wasdiscovered (Fig. 1, Table 2). We found ahigh concentration of CA 19-9 in theserum (Table 2). This tumor marker wasalso detected in the cytoplasma membraneof the thyroid cancer by immunoperoxidasestaining (Fig. 1). Thus, we speculatedthat the high serum level of CA 19-9 wasdue to its leakage from the thyroid cancerinto the serum. This possibility was sup-
ported by the finding that the serum levelof CA 19-9 returned to within the normal

Vol.37, No.2 TUMOR MARKERS AND ONCOGENE EXPRESSION 253
range after her total thyroidectomy (Table2). Similar CA 19-9-producing lung cystshave been reported by Okubo et al.(Okuboet al., 1989). Routinely this tumor wouldhave been broadly defined as a follicular or
papillary carcinoma. This case indicatesthat other carbohydrate antigen or cartinomaassociated mucin antigen-producing tumors,could be discovered by combining RIA andimmunohistochemical studies in this way.
During the past decade, there has beena dramatic renewal of interest in growthfactors and oncogenes in the field of cancerresearch (Fusco et al., 1987; Franklyn andSheppard, 1988., Burman et al., 1987). Inour immunohistochemical study, strong stain-ing of EGF and EGF-R in papillary thyroidcancers was demonstrated (Fig. 2). Sincenegative stainings were found in the normalthyroids glands or follicular cells of Graves'disease, these findings support"the autocrinetheory" of thyroid cancer (Schlessinger,1986).
As shown in Fig. 3, intense expressionof the ras p 21 oncogene was demonstratedin the apical cell surface and cytoplasm of
papillary carcinoma (Mizukami et al., 1988).Furtheremore, we observed that ras oncogeneexpression was enhanced in papillary carci-noma and follicular carcinoma. Increasedras p 21 oncogene expression has been ob-served in a variety of human cancers, how-ever, it is postulated that ras p 21 expressioncannot be used as a diagnostic marker inhuman cancer (Czerniak et al., 1989). Inaddition, as shown in Fig. 4, enhanced c-myc expression was observed in the cyto-
plasm of the papillary thyroid carcinomas.C-myc oncogene expression has also beendemonstrated in anaplastic carcinoma andfollicular carcinoma as previously reported
(Burman et al., 1987; Terrier et al., 1985).However, c-myc gene amplification was alsoobserved in Graves' disease. This infersthat c-myc expression might be involved inthe proliferation and development of thyroidcells and is not cancer specific (Nunes et
al., 1987). On the other hand, Burman etal.(Burman et al., 1987) emphasizes that achange in genomic c-myc regulation may
play a role in tumor development in somepatients with thyroid cancer.
In conclusion, to clarify these conflictingreports and to detect early thyroid cancer,more extensive research, including molecularoncology and technology to develop a DNA
probe to aid the diagnosis, is warranted inthis area.
Acknowledgements
We are indebted to Dr. Ellen Ingham for
encouragement, helpful discussions, and com
ments. We also thank Miss Misako Yagi and
Miss Yasuko Kamei for their excellent secretarial
assistance and to Miss Hermione Elliot and
Mr. David Shinya Tano for their help in
English in the preparation of this manuscript.
This work was supported in part by the
Japan Clinical Pathology Foundation for Inter-
national Exchange and Clinical Pathology Foun-
dation of Japan.
References
Bayer, M. F. and J. P. Kriss (1979). Immuno-radiometric assay for serum thyroglobulinSemiquantitative measurement of thyroglobulinin antithyroglobulin positive sera. J. Clin.Endocrinol. Metab. 49, 557-564.
Botsch, H., J. Glatz, E. Schultz, K. W. Wenzel(1983). Long-term follow-up using serial serumthyroglobulin determinations in patients withdifferentiated thyroid carcinoma. Cancer 52,1856-1859.
Burman, K.D., Y. Djuh., R.V. LaRocca, M.E.Nunes, J. C. D'Avis, D. E. Nicholson and L.Wartofsky (1987). C-myc expression in thethyroid I: normal, adenomatous, and cancer-ous thyroid tissue. Horm. Metab. Res. 17(suppl), 63-65.
Channing, J. D.(1987). Cellular oncogenes andhuman carcinogenesis. Clin. Chem. 33, 641-646.
Czerniak, B., F. Herz, W. Gorczyca and L. G.Koss (1989). Expression of ras oncogene p 21

254 HASHIMOTO et al.Endoorinol. Japon.April 1990
protein in early gastric carcinoma and adjacentgastric epithelia. Cancer 64, 1467-1473.
Franklyn, J. A. and M. C. Sheppard (1988).Hormonal control of gene expression. Clin.Endocrinol. 29, 337-348.
Fusco, A., M. Grieco, M. Santoro, M. T.Berlingieri, S. Pilotti, M. A. Pierotti, G. DellaPorta and G. Vecchio (1987). A new oncogenein human thyroid papillary carcinomas andtheir lymph-nodal metastases. Nature 328,170-172.
Hashimoto, T., H. Nakamura, N. Ohba, Y.Mizukami, N. Kawagishi, S. Terahata, F.Matsubara, Y. Watanabe and N. Sawabu(1986). Usefulness of measurement for serumcalcitonin as a tumor marker in thyroid,lung and liver cancer. Clinical Endocrinology(in Japanese) 34, 135-143.
Hashimoto, T., Y. Mizukami, T. Michigishi,F. Matsubara and I. Miyazaki (1989). Tumormarkers and oncogenes of thyroid cancer. Jap.J. Clin. Path.(in Japanese) 37, 122-130.
Kim, P. S., A. D. Dunn and J. T. Dunn (1988).Altered immunoreactivity of thyroglobulin inthyroid disease. J. Clin. Endocrinol. Metab.67, 161-168.
Kohno, Y., O. Tarutani, S. Sakata and H.Nakajima (1985). Monoclonal antibodies tothyroglobulin elucidate differences in proteinstructure of thyroglobulin in healthy indi-viduals and those with papillary adeno-carcinoma. J. Clin. Endocrinol. Metab. 61,343-350.
Linsley, P. S., J. P. Brown, J. L. Magnani andD. Horn (1988). Monoclonal antibodies re-active with mucin glycoproteins found in serafrom breast cancer patients. Cancer Res. 48,2138-2148.
Madeddu, G., A. R. Casu, C. Costanza, G.Maras, M. L. Arras, A. Marrosu and M.Langee (1985). Serum thyroglobulin levels inthe diagnosis and follow-up of subacute'painful' thyr
oiditis. Arch Intern. Med. 145,
243-247.
Mizukami, Y., A. Nonomura, T. Hashimoto ,S. Terahata, F. Matsubara, T. Michigishi and
M. Noguchi (1988). Immunohistochemicaldemonstration of ras p 21 oncogene product innormal, benign, and malignant human thyroidtissues. Cancer 61, 873-880.
Nunes, M. E., Y. Djuh, R. V. LaRocca, D. E.Nicholson, J. R. Baker Jr., L. Wartofsky, J.C. D'Avis and K. D. Burman (1987). C-mycexpression in the thyroid II: thyrocytes andperipheral and intrathyroidal lymphocytesfrom patients with autoimmune thyroiddisease. Horm.Metab. Res. 17, 66-69.
Ohtani, S., K. Iwase, A. Nagasaka, K. Kato,I. Nagatsu, S. Shinoda, M. Inagaki, T.Tsujimura, A, Inagaki, S. Miyakawa, K.Kawase, T. Kawabe, T. Ohyama, R. Masunagaand K. Miura (1988). Tumor marker antigensrelating to thyroid follicular and parafollicularcell in various thyroid disorders. In: NagatakiS. Torizuka K. eds. The thyroid 1988.Amsterdam: Elsevier, 681-684.
Okubo, A., S. Sone, F. Ogushi, T. Ogura, T.Uyama, Y. Monden and and K. II (1989).A case of bronchogenic cyst with high pro-duction of antigen CA 19-9. Cancer 63, 1994-1997.
Schlessinger, J. (1986). Regulation of cell growthby the EGF receptor. In: Kahn P, Graf T,eds. Oncogenes and growth control. Berlin:Spinger-Verlag, 77-84.
Schneider, A. B. and R. Pervos (1978). Radio-immunoassay of human thyroglobulin : effectof antithyroglobulin auto antibodies. J. Clin.EndocKnol. Metab. 47, 126-137.
Terrier, P. H., S. Douc-Rasy and M. Schlumbeger,et al.(1985). Enhanced expression of the c-myc oncogen in a case of anaplastic carcinomaof the thyroid gland. In: Jaffiol C, MilhaudG, eds. Thyroid Cancer. New York: Elsevier,287-288.
Touitou, Y. and H. M. Heshmati (1988). Neuron-specific enolase in medullary thyroid carcinoma.Clin. Chem. 34, 2375-2376.
Uller, R. P. and A. J. Van Herle (1978). Effectof therapy on serum thyroglobulin levels inpatients with Graves' disease. J. Clin. Endo-crinol. Metab. 46, 264-270.