Ultrasound Obstet Gynecol 2013; 42: 329–334Published online 4 August 2013 in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.12486
Does 17-α-hydroxyprogesterone caproate affect fetalbiometry and birth weight in twin pregnancy?E. J. H. MULDER*, E. M. J. VERSTEEGH†, K. W. M. BLOEMENKAMP†, A. C. LIM‡,B. W. J. MOL‡, D. J. BEKEDAM§, A. KWEE*, H. W. BRUINSE* and G. C. M. L. CHRISTIAENS**Department of Obstetrics, University Medical Center Utrecht (UMCU), Utrecht, The Netherlands; †Department of Obstetrics, LeidenUniversity Medical Center (LUMC), Leiden, The Netherlands; ‡Department of Obstetrics, Academic Medical Center (AMC), Amsterdam,The Netherlands; §Department of Obstetrics, Onze Lieve Vrouwe Gasthuis, Amsterdam, The Netherlands
KEYWORDS: 17-α-hydroxyprogesterone caproate; fetal growth; preterm birth; twins
ABSTRACT
Objective Increasingly, maternal administration of 17-α-hydroxyprogesterone caproate (17-OHPC) is utilized toprevent preterm birth, but the fetal safety of 17-OHPCis still a matter of concern. This study aimed to assesswhether exposure to 17-OHPC during the second andthird trimesters of pregnancy affects fetal biometry intwin gestations.
Methods This study included a subset of women witha twin pregnancy who had been previously included ina randomized clinical trial comparing the effectivenessof 17-OHPC and placebo on neonatal outcomes andpreterm birth rates in multiple pregnancy. In the presentstudy, the individual growth patterns of femur length,head circumference and abdominal circumference werecompared between fetuses of women who had beenrandomized to receive weekly injections of either 17-OHPC (n = 52) or placebo (n = 58) at between 16–20and 36 weeks’ gestation.
Results The three biometric variables assessed developedsimilarly in fetuses in both the group exposed to 17-OHPC and the placebo group during the second half ofpregnancy. Birth weight adjusted for parity and fetal sexwas also comparable between groups.
Conclusion The use of 17-OHPC has no adverse effectson fetal biometry and birth weight in twins. Copyright 2013 ISUOG. Published by John Wiley & Sons Ltd.
INTRODUCTION
Preterm birth, defined by the World Health Organizationas birth before 37 weeks’ gestation1, is the leadingcause of neonatal mortality and morbidity. Prophylacticadministration of 17-α-hydroxyprogesterone caproate(17-OHPC) to women with a singleton pregnancy anda history of spontaneous preterm delivery can reduce the
Correspondence to: Dr E. J. H. Mulder, Department of Obstetrics, Wilhelmina Children’s Hospital, University Medical Center, KE.04.123.1,Lundlaan 6, 3584 EA Utrecht, The Netherlands (e-mail: [email protected])
Accepted: 18 March 2013
recurrence of preterm birth2–4. Progesterone is believed toexert an inhibitory effect on prostaglandins and oxytocinand to decrease the number of oxytocin receptors and gapjunctions in the myometrium, which are crucial elementsin the activation of (preterm) delivery5. However, the fetalsafety of 17-OHPC is still a matter for concern6–9.
Our study was prompted by the case of a pregnantwoman at increased risk of recurrent preterm birth. At20 weeks’ gestation, after 4 weeks of 17-OHPC treatment,ultrasonography showed extremely shortened fetal longbones (far below the third percentile). At this time,treatment was discontinued on the mother’s initiativeand fetal catch-up growth was observed, such that allbones had a length at or above the third percentile by32 weeks, except for femur length, which remained belowthe third percentile until delivery at term. Birth weightwas below the fifth percentile and was much lower thanthat of a previous unexposed sibling.
In light of this case, we decided to assess whetherantenatal exposure to 17-OHPC affects the growthtrajectory of individual fetuses. For this purpose, we useddata from a large Dutch randomized controlled trial onthe prevention of preterm birth in multiple pregnancies(AMPHIA trial)10. This trial compared neonatal out-comes of pregnancies randomized for maternal use of17-OHPC vs placebo, and showed no beneficial effect of17-OHPC administration on the rates of preterm birthand neonatal morbidity in multiple pregnancies.
METHODS
The present study was a secondary analysis of data fromthe AMPHIA trial (ISRCTN Register, www.isrctn.org,ISRCTN40512715). This trial was a multicenter, double-blind, placebo-controlled, randomized trial comparing theeffect on neonatal outcome of weekly intramuscular injec-tions of either 17-OHPC or placebo10. The original trialincluded a total of 671 pregnant women with multiple
Copyright 2013 ISUOG. Published by John Wiley & Sons Ltd. ORIGINAL PAPER

330 Mulder et al.
pregnancies treated at 55 obstetric clinics in The Nether-lands randomized between August 2006 and August2009. The study was approved by the research ethicscommittee of the Academic Medical Center in Amsterdam(Ref MEC 05/102), and written informed consent wasobtained from each participant. Patients received their firstinjection of 17-OHPC (250 mg in 1 mL of castor oil) orplacebo (1 mL of castor oil) at between 16 and 20 weeks’gestation, and their last injection at 36 weeks except incases in which delivery occurred before 36 weeks.
The present sample used for modeling fetal growthtrajectories consisted of all 126 AMPHIA participantsfrom four clinics, distributed as follows: UniversityMedical Center Utrecht, Utrecht (n = 43); AcademicMedical Center, Amsterdam (n = 35); Onze Lieve VrouweGasthuis, Amsterdam (n = 27); and Leiden UniversityMedical Center, Leiden (n = 21). Data on maternal andpregnancy characteristics, including dates of injection,chorionicity, gestational age (GA) at delivery and birthweight, were collected from the AMPHIA Trial database.Serial ultrasonographic measurements of femur length,head circumference and abdominal circumference, maderegularly on individual fetuses between 15 and 40 weeks’gestation, were retrospectively collected from electronicpatient records kept by each of the four clinics.
The fetal ultrasound examinations were carried outby trained and accredited ultrasonographers under thesupervision of an obstetrician in each center. Fetalbiometry on twins was performed biweekly as part ofroutine care using standard methods11 and accordingto nationally accepted guidelines for fetal ultrasoundbiometry of the Dutch Society of Obstetrics andGynecology (‘Fetal Biometry’ protocol, NVOG, version1.0, released 2008). We distinguished between the twofetuses to allow for assessment of the individual twinsduring repeat scans. We referred to the one that is lowerin the pelvis (and therefore the one due to be born first)as Fetus 1 or Twin A. Additional intrauterine ‘mapping’included assessment of fetal sex, location in the placenta,intrapair growth discordance (if present) and fetal positionon the right side vs the left side of the uterus. Fetalposition is generally stable from 24 weeks onwards, butswapping of positions can sometimes occur. To check forthis, the longitudinal biometric measurements of each pairwere scrutinized for unexpected, illogical, or unrealisticdiscrepancies in biometry during data preparation. Suchdeviations occurred infrequently and were correctedbefore statistical analysis was carried out.
For inclusion in our analysis, participants were requiredto have a twin pregnancy with delivery at or after27 weeks’ gestation, and to have had at least three serialultrasound measurements, the final measurement beingmade after 26 weeks. These inclusion criteria were met by110 out of the 126 women (Figure 1).
Statistical analysis
To demonstrate a difference of 2 mm in femur lengthbetween the two randomization groups at 23 weeks’
gestation, the study required 200 fetuses (100 pertreatment arm) to have 80% power and a 5% type-1error probability. The randomization code was notdisclosed to the investigators until all biometric data hadbeen collected.
Data management and statistical analysis were per-formed with SPSS for Windows (version 18, IBM/SPSSInc., Chicago, IL, USA). Results were summarized withthe use of standard descriptive statistics: n (%) for cate-gorical variables and mean (SD) for continuous variables.Groups were evaluated for equivalence using the chi-square or Fisher’s exact test for categorical measures,as appropriate, and t-tests for continuous variables. Vari-ables that were not normally distributed were transformed(log or square root). Fetal biometry and birth weight wereanalyzed at the individual twin level.
The serial measurements available for each fetus wereanalyzed with multilevel (mixed-effects) modeling toproduce individual growth trajectories. The first levelcomprises the repeated measurements on an individualfetus, the second level the twin number (1 or 2) and thethird level the individual mother. Mixed-effects modelsallow for intrafetal correlation of repeated measurements,make use of the exact age at measurement and accountfor a dissimilar number of measurements on each fetus.Such models also allow for individual variation ingrowth trajectories, as random effects permit variabilityin intercept, slope and curvature between subjects. Weexplored quadratic and cubic functions of GA for eachfetal biometric variable. The GA terms (linear, quadraticand cubic) were included as both fixed and random effects.Treatment (17-OHPC vs placebo) was included as a maineffect and also as an interaction with the GA terms.
The potential effect of 17-OHPC treatment on birthweight was studied in a multivariable regression analysis(SPSS option: General Linear Models, GLM).
RESULTS
Maternal characteristics and outcome of pregnancy arepresented in Table 1. Most variables were similar betweenthe 17-OHPC and placebo groups. However, there was anunbalanced distribution regarding chorionicity and modeof conception, with larger proportions of monochorionicand spontaneously conceived pregnancies in the placebogroup than in the 17-OHPC group. All 220 fetuses wereborn alive and none died in the neonatal period.
In total, there were 1325, 1211 and 1367 measurementsof fetal femur length, head circumference and abdominalcircumference, respectively, with an average of 6 (range,3–11) per fetus for each biometric variable; these numbersdid not differ statistically between groups (P = 0.74, 0.63and 0.33, respectively). The time interval between thefinal biometric measurement and birth was 1.9 (range,0.1–7.3) weeks in the 17-OHPC group and 1.7 (range,0–5.7) weeks in the placebo group (P = 0.60).
Mixed-effects models were applied to the serial datafor femur length, head circumference and abdominalcircumference. A quadratic function of GA (centered at
Copyright 2013 ISUOG. Published by John Wiley & Sons Ltd. Ultrasound Obstet Gynecol 2013; 42: 329–334.

Fetal growth and 17-OHPC 331
Excluded:Triplet pregnancy (n = 7) Delivery < 27 weeks or last fetal measurement < 26 weeks (n = 7)
Fewer than three fetal measurements (n = 2)
Women who met inclusion criteria(n = 110)
Women who participated inAMPHIA trial at four centers
(n = 126)
Women randomized to17-OHPC(n = 52)
Women randomized toplacebo(n = 58)
Neonatal outcomeavailable(n = 104)
Neonatal outcomeavailable(n = 116)
Figure 1 Flow-chart of study population. 17-OHPC, 17-α-hydroxyprogesterone caproate.
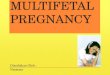
15 weeks) with random effects for the intercept (constant)and the linear (GA) and quadratic (GA2) terms fit thedata best. The models also included the main effectof treatment (17-OHPC vs placebo) and treatment-by-GA and treatment-by-GA2 interactions as fixed effects.Chorionicity and mode of conception, considered ascovariables, were handled similarly. The results forthe final models are shown in Table 2. The threebiometric variables showed a non-linear increase in sizebetween 15 and 40 weeks’ gestation, demonstrated bythe highly significant growth curve parameters (intercept,GA and GA2). There was a significant main effectof chorionicity on all biometric variables. The threeparameters measured were smaller in monochorionicthan in dichorionic twins at 15 weeks’ gestation, andthe differences remained throughout pregnancy forfemur length and abdominal circumference. For headcircumference, the initial difference in size decreasedwith increasing gestation (significant chorionicity-by-GAinteraction). Twin number (1 or 2), mode of conception,and treatment with 17-OHPC did not influence the shapeof the three growth curves. Treatment-by-chorionicityinteractions were not significant. Figure 2 shows thegrowth curves of femur length for the placebo and 17-OHPC groups separately, illustrating the absence of effectof intrauterine exposure to 17-OHPC on fetal growth.
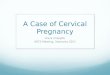
In the total sample of 220 fetuses, mean GA at birthwas 36.0 (range, 27.4–40.3) weeks and mean birthweight was 2408 (range, 650–4450) g (Figure 3). GA atbirth and birth weight were similar between the placeboand 17-OHPC groups in univariate analysis (Table 1).To ascertain whether exposure to 17-OHPC has an inde-pendent effect on birth weight, we analyzed with GLM
the birth-weight data for all infants using age at birth(centered at 36 weeks) and treatment as predictors. Parity,chorionicity, ethnicity and fetal gender were included ascovariables. A linear model fitted the data best. The meanpredicted birth weight at 36 weeks’ gestation was 2412 g(SE 52 g) and was 170 g (SE 8 g) lower or higher foreach week that birth occurred before or after 36 weeks,respectively (P < 0.0001 for both model estimates). Therewere significant main effects on birth weight for parityand fetal gender, with fetuses of nulliparous womenweighing 118 g (SE 46 g) less than those of parous women(P = 0.01) and males weighing 130 g (SE 44 g) morethan females (P = 0.003). Chorionicity and ethnicitydid not influence birth weight (P = 0.32 and P = 0.12,respectively). Fetuses exposed in utero to 17-OHPCweighed 35 g (SE 46 g) less than fetuses in the placebogroup, but this difference was not significant (P = 0.44).
DISCUSSION
Treatment with natural or synthetic progestin (17-OHPC) is widely used in the prevention of (recurrent)preterm birth. Several randomized controlled studieshave demonstrated a considerable reduction in pretermdelivery rates when progesterone was administered towomen carrying singletons2,3,12,13, but not in cases ofmultiple pregnancy4,10,14–16. The latter phenomenon iscorroborated by our subsample analysis of the AMPHIATrial (Table 1). The present findings on fetal twinsdemonstrate that maternal administration of 17-OHPCat weekly intervals between 16 and 36 weeks’ gestationhas no adverse effects on the intrauterine growth patternsof femur length and head and abdominal circumference,
Copyright 2013 ISUOG. Published by John Wiley & Sons Ltd. Ultrasound Obstet Gynecol 2013; 42: 329–334.

332 Mulder et al.
Table 1 Baseline characteristics and outcome data of twin pregnancies included in this study according to exposure to17-α-hydroxyprogesterone caproate (17-OHPC) or placebo
Parameter17-OHPC
group (n = 52)Placebo
group (n = 58) P
Maternal characteristicsAge (years) 34.2 ± 4.3 33.4 ± 5.2 0.40Body mass index (kg/m2) 24.4 ± 5.1 23.8 ± 4.3 0.48Race 0.44
Caucasian 39 (75.0) 48 (82.8)Other 13 (25.0) 10 (17.2)
Higher education 22 (42.3) 30 (51.7) 0.43Smoker 8 (15.4) 12 (20.7) 0.62Alcohol consumption 1 (1.9) 2 (3.4) 1.00
Pregnancy characteristicsNulliparous 27 (51.9) 37 (63.8) 0.21Mode of conception 0.009
Spontaneous 26 (50.0) 44 (75.9)Assisted reproduction treatment* 26 (50.0) 14 (24.1)
Chorionicity 0.022Monochorionic 4 (7.7) 14 (24.1)Dichorionic 48 (92.3) 44 (75.9)
Outcome of pregnancyGestational age at birth (weeks) 36.5 ± 2.5 35.7 ± 3.0 0.11Delivery before 32 weeks’ gestation 3 (5.8) 7 (12.1) 0.33Gender 0.27
Male 46/104 (44.2) 60/116 (51.7)Female 58/104 (55.8) 56/116 (48.3)
Birth weight (g) 2461 ± 519 2359 ± 627 0.19Birth weight < 10th percentile 28/104 (26.9) 26/116 (22.4) 0.54Intrapair growth discrepancy (%)† 12.4 ± 11.7 10.3 ± 7.9 0.27Intrapair growth discrepancy > 20% 8 (15.4) 5 (8.6) 0.38
Data shown as mean ± SD or n (%). *Ovarian hyperstimulation, in-vitro fertilization or intracytoplasmic sperm injection. †((Larger birthweight – smaller birth weight)/larger birth weight) × 100%.
Table 2 Statistical results of linear mixed modeling for fetal biometric measurements
Variable Femur length Head circumference† Abdominal circumference
Intercept‡ 16.7 (0.3)*** 10.7 (0.04)*** 92.1 (1.5)***Time effects
GA‡ 3.3 (0.05)*** 0.557 (0.006)*** 12.6 (0.2)***GA2‡ −0.041 (0.002)*** −0.011 (0.0002)*** −0.108 (0.008)***
Group effectsFetus 2 vs Fetus 1 −0.08 (0.22) 0.04 (0.03) 0.6 (0.9)Monochorionic vs dichorionic −0.69 (0.29)* −0.11 (0.05)* −5.1 (1.5)**ART vs spontaneous conception −0.50 (0.46) 0.05 (0.07) −0.19 (1.4)17-OHPC treatment vs placebo 0.071 (0.40) −0.04 (0.03) −1.5 (1.3)
Time-by-group effectsGA; monochorionic vs dichorionic −0.0074 (0.081) 0.009 (0.004)* 0.094 (0.20)GA2; monochorionic vs dichorionic 0.0017 (0.0037) −0.0002 (0.0006) −0.0014 (0.02)GA; ART vs spontaneous conception 0.051 (0.08) −0.017 (0.013) −0.16 (0.16)GA2; ART vs spontaneous conception −0.0032 (0.0033) 0.0007 (0.0005) 0.004 (0.02)GA; 17-OHPC treatment vs placebo 0.017 (0.07) 0.004 (0.003) 0.094 (0.15)GA2; 17-OHPC treatment vs placebo −0.00024 (0.003) −0.00032 (0.0005) −0.0022 (0.016)
Data are presented as estimates (β) and standard error (in parentheses) of models. ***P < 0.0001. **P < 0.001. *P < 0.05. †Model estimatesafter square root transformation. ‡Gestational age centered at 15 weeks’ gestation. 17-OHPC, 17-α-hydroxyprogesterone caproate; ART,assisted reproduction treatment (ovarian hyperstimulation, in-vitro fertilization or intracytoplasmic sperm injection); GA, gestational age.
and does not influence birth weight. Northen et al.17
in a follow-up study found no differences in height,weight and head circumference between children exposedin utero to 17-OHPC and randomly allocated controlswhen examined at 4 years of age.
Others have expressed concerns about the fetal safety ofprogestogens, 17-OHPC in particular6–9. These concernsrelate to a statistically non-significant increase in fetalloss (miscarriage, perinatal death/stillbirth) in the originalNational Institutes of Health (NIH) study2, and to
reported observations on embryo viability (increasedresorption i.e. miscarriage) and malformations fromreproductive toxicology studies in animals8. However,a recent large study found no evidence of an increasedrate of (early) fetal loss in women treated with 17-OHPCduring pregnancy18. In addition, the existing literatureon animal developmental toxicity regarding 17-OHPCgenerally appears to bear little relevance to the humansituation, mainly owing to methodological flaws and theuse of suprapharmacologic doses7–9. Nevertheless, of
Copyright 2013 ISUOG. Published by John Wiley & Sons Ltd. Ultrasound Obstet Gynecol 2013; 42: 329–334.

Fetal growth and 17-OHPC 333
80
70
60
50
40
Fem
ur le
ngth
(m
m)
30
20
10
015 20 25 30 35 40
Gestational age (weeks)
Figure 2 Femur length in fetuses exposed to17-α-hydroxyprogesterone caproate ( ) and placebo ( ),together with overall 95% prediction intervals ( ).
interest to the present investigation are findings in theoffspring of pregnant mice implanted with 17-OHPCpellets between gestational days 7 and 20 (term)19. Fetalbone development and growth, assessed by diaphysealand epiphyseal lengths of humerus and femur, and birthweight were unaffected in the pups exposed to 17-OHPCat a dose 70 times higher than the human therapeutic dose.Collectively, the results of the abovementioned studiesare reassuring with regard to the safety of antenatal17-OHPC treatment. Future follow-up studies shouldinvestigate whether long-term physical development andneurodevelopment are affected.
In retrospect, we believe that the observation of short-ened bones in a fetus exposed to 17-OHPC that gave theimpetus for the present study (see Introduction), must beconsidered unrelated to 17-OHPC. Not only did the infantpresent with a ventricular septal defect that was surgicallycorrected at 31/2 months after birth, but he also had tem-porary hypercalcemia and hypervitaminosis D during thefirst year of life. At the time of writing, at the age of 2years, the infant was developing normally. The continu-ing maternal hypervitaminosis D remains hitherto unex-plained; a chromosomal array examination was normal.
Twins are born earlier and have lower birth weightthan singletons, with monochorionic twins weighing lessat birth than dichorionic twins20,21. We found differentialintrauterine growth patterns between monochorionicand dichorionic twins for femur length and head andabdominal circumference, but mode of conception had no
5000
4000
3000
Bir
th w
eigh
t (g
)
2000
1000
025 30 35 40
Gestational age (weeks)
Figure 3 Scatter plot of birth weights of individual twins in groupsexposed to 17-α-hydroxyprogesterone caproate ( ) (n = 104) orplacebo ( ) (n = 116).
effect on the physical development of fetal twins. Gielenet al.20 in a study of over 8000 twins found a linearrelationship between birth weight and GA at birth, witha mean increase in weight of about 160 g per week. Theauthors examined a variety of maternal, twin-specific andplacental factors for a potential effect on birth weight,but only a few were found to be independent variables.These included parity, fetal sex and site of umbilical cordinsertion, but not, among others, mode of conception,chorionicity, zygosity or placental fusion. Although westudied a limited number of covariables, the results of ourtwin birth-weight analysis are fully in line with those ofthis large twin study20. We also found an increase in meanbirth weight of 170 g per week and independent effects onbirth weight of parity and fetal sex, but not of chorionicity.Importantly, antenatal exposure to 17-OHPC had nosignificant effect on fetal biometric variables and on birthweight whether adjusted for covariables or not.
The unbalanced distribution of monochorionic andspontaneously conceived cases between the 17-OHPCand placebo groups is a limitation of the study. However,we believe that our main finding, i.e. absence of effect ofexposure to 17-OHPC on fetal physical development, isunbiased. Neither chorionicity nor mode of conceptionappeared to play an important independent role duringfetal development for reasons mentioned above. Inaddition, a systematic review did not report differencesin outcomes of twin pregnancies between assisted andnatural conception, in terms of (very) low birth weightand (very) preterm birth22. Another limitation relates tothe retrospective design of the present study, absence of
Copyright 2013 ISUOG. Published by John Wiley & Sons Ltd. Ultrasound Obstet Gynecol 2013; 42: 329–334.

334 Mulder et al.
controls for assessing intra- and interobserver agreementand variation among the four centers. However, illogicaldiscrepancies in intertwin biometry were encountered veryrarely during data collection and scrutiny. The qualityof the data is high because nationwide protocols werefollowed and the centers each had the use of good-qualityequipment and dedicated, qualified sonographers.
We conclude that this study does not indicate an adverseeffect of weekly intramuscular injections of 17-OHPC onfetal growth trajectories during the second and thirdtrimesters and on birth weight in twins.
ACKNOWLEDGMENT
The AMPHIA trial was funded by ZonMw, The Nether-lands organization for health research and development(grant number of the original trial 62200019).
REFERENCES
1. World Health Organization. International classification ofdiseases and related health problems (10th revision). WorldHealth Organization: Geneva, 1992.
2. Meis PJ, Klebanoff M, Thom E, Dombrovski MP, Sibai B,Moawad AH, Spong CY, Hauth JC, Miodovnik M, VarnerMW, Leveno KJ, Caritis SN, Iams JD, Wapner RJ, Conway D,O’Sullivan MJ, Carpenter M, Mercer B, Ramin SM, ThorpJM, Peaceman AM, Gabbe S; National Institute of ChildHealth and Human Development Maternal–Fetal MedicineUnits Network. Prevention of recurrent preterm delivery by17-alpha-hydroxyprogesterone caproate. N Engl J Med 2003;348: 2379–2385.
3. Da Fonseca EB, Bittar RE, Carvalho MH, Zugaib M. Prophy-lactic administration of progesterone by vaginal suppository toreduce the incidence of spontaneous preterm birth in women atincreased risk: a randomized placebo-controlled double blindstudy. Am J Obstet Gynecol 2003; 188: 419–424.
4. Likis FE, Velez Edwards DR, Andrews JC, Woodworth AL,Jerome RN, Fonnesbeck CJ, McKoy JN, Hartmann KE.Progestogens for preterm birth prevention: a systematic reviewand meta-analysis. Obstet Gynecol 2012; 120: 897–907.
5. Zakar T, Mesiano S. How does progesterone relax the uterusin pregnancy? N Engl J Med 2011; 364: 972–973.
6. O’Brien JM. The safety of progesterone and 17-hydroxyprogesterone caproate administration for theprevention of preterm birth: an evidence-based assessment. AmJ Perinatol 2012; 29: 665–672.
7. Behrman RE, Butler AS (eds). Preterm birth: Causes,Consequences, and Prevention. The National Academies Press:Washington, DC, 2006.
8. Christian MS, Brent RL, Calda P. Embryo–fetal toxicitysignals for 17alpha-hydroxyprogesterone caproate in high-risk pregnancies: a review of the non-clinical literature forembryo–fetal toxicity with progestins. J Matern Fetal NeonatalMed 2007; 20: 89–112.
9. Calda P. Safety signals of 17-OHP-C use in pregnancy andefficacy in prevention of preterm birth. J Matern Fetal NeonatalMed 2009; 22: 540–542.
10. Lim AC, Schuit E, Bloemenkamp K, Bernardus RE, Duvekot JJ,Erwich JJHM, van Eyck J, Groenewold RHH, Hasaart THM,Hummel P, Kars MM, Kwee A, van Oirschot CM, van PampusMG, Papatsonis D, Porath MM, Spaanderman ME, Willekes C,Wilpshaar J, Mol BWJ, Bruinse HW. 17α-hydroxyprogesteronecaproate for the prevention of adverse neonatal outcome inmultiple pregnancies. Obstet Gynecol 2011; 118: 513–520.
11. Verburg BO, Steegers EAP, de Ridder M, Snijders RJM, SmithE, Hofman A, Moll HA, Jaddoe VW, Witteman JC. Newcharts for ultrasound dating of pregnancy and assessment offetal growth: longitudinal data from a population-based cohortstudy. Ultrasound Obstet Gynecol 2008; 31: 388–396.
12. Romero R, Nicolaides K, Conde-Agudelo A, Tabor A, O’BrienJM, Cetingoz E, Da Fonseca E, Creasy GW, Klein K, Rode L,Soma-Pillay P, Fusey S, Cam C, Alfirevic Z, Hassan SS. Vaginalprogesterone in women with an asymptomatic sonographicshort cervix in the midtrimester decreases preterm deliveryand neonatal morbidity: a systematic review and metaanalysisof individual patient data. Am J Obstet Gynecol 2012; 206:124.e1–19.
13. Hassan SS, Romero R, Vidyadhari D, Fusey S, Baxter JK,Khandelwal M, Vijayaraghavan J, Trivedi Y, Soma-Pillay P,Sambarey P, Dayal A, Potapov V, O’Brien J, Astakhov V, YuzkoO, Kinzler W, Dattel B, Sehdev H, Mazheika L, ManchulenkoD, Gervasi MT, Sullivan L, Conde-Agudelo A, Phillips JA,Creasy GW. Vaginal progesterone reduces the rate of pretermbirth in women with a sonographic short cervix: a multicenter,randomized, double-blind, placebo-controlled trial. UltrasoundObstet Gynecol 2011; 38: 18–31.
14. Norman JE, Mackenzie F, Owen P, Mactier H, HanrettyK, Cooper S, Calder A, Mires G, Danielian P, Sturgiss S,MacLennan G, Tydeman G, Thornton S, Martin B, ThorntonJG, Neilson JP, Norrie J. Progesterone for the prevention ofpreterm birth in twin pregnancy (STOPPIT): a randomised,double-blind, placebo-controlled study and meta-analysis.Lancet 2009; 373: 2034–2040.
15. Rouse DJ, Caritis SN, Peaceman AM, Sciscione A, Thom EA,Spong CY, Varner M, Malone F, Iams JD, Mercer BM, ThorpJ, Sorokin Y, Carpenter M, Lo J, Ramin S, Harper M, AndersonG; National Institute of Child Health and Human DevelopmentMaternal–Fetal Medicine Units Network. A trial of 17 alpha-hydroxyprogesterone caproate to prevent prematurity in twins.N Engl J Med 2007; 357: 454–461.
16. Rode L, Klein K, Nicolaides KH, Krampl-Bettelheim E, TaborA; PREDICT Group. Prevention of preterm delivery in twingestations (PREDICT): a multicenter, randomized, placebo-controlled trial on the effect of vaginal micronized progesterone.Ultrasound Obstet Gynecol 2011; 38: 272–280.
17. Northen AT, Norman GS, Anderson K, Moseley L, Divito M,Cotroneo M, Swain M, Bousleiman S, Johnson F, DormanK, Milluzzi C, Tillinghast JA, Kerr M, Mallett G, Thom E,Pagliaro S, Anderson GD; National Institute of Child Healthand Human Development (NICHD) Maternal–Fetal MedicineUnits (MFMU) Network. Follow-up of children exposed inutero to 17 alpha-hydroxyprogesterone caproate comparedwith placebo. Obstet Gynecol 2007; 110: 865–872.
18. Sibai BM, Istwan NB, Palmer B, Stanziano GJ. Preg-nancy outcome of women receiving compounded 17α-hydroxyprogesterone caproate for prophylactic prevention ofpreterm birth 2004 to 2011. Am J Perinatol 2012; 29: 635–642.
19. Carbone JP, Brent RL. Genital and nongenital teratogenesisof prenatal progestogen therapy: the effects of 17 alpha-hydroxyprogesterone caproate on embryonic and fetal devel-opment and endochondral ossification in the C57B1/6 J mouse.Am J Obstet Gynecol 1993; 169: 1292–1298.
20. Gielen M, Lindsey PJ, Derom C, Loos RJF, Derom R, NijhuisJG, Vlietinck R. Twin birth weight standards. Neonatology2007; 92: 164–173.
21. Hack K, Derks J, Elias S, Franx A, Roos EJ, Voerman SK, BodeCL, Koopman-Esseboom C, Visser GH. Increased perinatalmortality and morbidity in monochorionic versus dichorionictwin pregnancies: clinical implications of a large Dutch cohortstudy. BJOG 2008; 115: 58–67.
22. Helmerhorst FM, Perquin DA, Donker D, Keirse MJ. Perinataloutcome of singletons and twins after assisted conception: asystematic review of controlled studies. BMJ 2004; 328: 261.
Copyright 2013 ISUOG. Published by John Wiley & Sons Ltd. Ultrasound Obstet Gynecol 2013; 42: 329–334.
Recommended