Embed Size (px)
Citation preview

Chang Hoon Yim
Cheil General Hospital
Management of subclinical hypothyroidism in pregnancy

Maternal hypothyroidism
Maternal Fetal
Gestational hypertension Spontaneous abortion
Anemia Small for gestational age
Postpartum hemorrhage Fetal stress during labor
Placental abruption Fetal death
Transient congenital hypothyroidism
Possible impairment in cognitive function
(Best Pract Res Clin Endocrinol Metab, 2004)

Endocrine Society (J Clin Endocrinol Metab, 2007)
American Thyroid Association(Thyroid, 2011)
Endocrine Society (J Clin Endocrinol Metab, 2012)
European Thyroid Association(Eur Thyroid J, 2014)
Guideline for Management of Thyroid Dysfunction During Pregnancy

Adverse maternal and fetal effects
Associated with Overt hypothyroidism Overt hyperthyroidism
Not associated with Subclinical hyperthyroidism
? Subclinical hypothyroidism (SCH)

Free T4 TSHOvert hyperthyroidism ↑ ↓↓
Subclinical hyperthyroidism N ↓Subclinical hypothyroidism N ↑
Overt hypothyroidism ↓ ↑↑

Subclinical hypothyroidism (SCH) in Pregnancy
Diagnosis
Management
Screening

Children of treated women
with hypothyroidism(N=14)
Children of untreated women with hypothy-
roidism(N=48)
Control
(N=124)
IQ score 111 100 107p=0.20 p=0.005
IQ =< 85(%) 0 19 5p=0.90 p=0.007
Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child.
(Haddow JE, N Engl J Med 1999)
25,000 children

numbers TSH IQ p-value*
Gr 1 (control) 124 <98th percentile 107
Gr 2 31 98th – 99.85th 102 NS
Gr 3 31 >99.85th 97 0.003
Relation of severity of maternal hypothyroidism to cognitive development of offspring
(Klein RZ, J Med Screen 2001)
25,000 children
* compared with control

Correlation of IQ and maternal TSH
(Klein RZ, J Med Screen 2001)

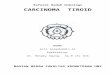
Thyroid function and hCG in pregnancy
Clinical Obstetrics and Gynecology 1997
0 10 20 30 40Gest wks
hCG
total T4
free T4
TSH

Trimester-specific reference ranges for TSH should be applied.
Recommended reference range for TSH 1st trimester : 0.1 ~ 2.5 mIU/L 2nd : 0.2 ~ 3.0 3rd : 0.3 ~ 3.5
(2007)
(Thyroid, 2011)

Prevalence of hypothyroidism in pregnancy
0.2 – 0.5% Overt hypothyroidism (OH) 2 – 2.5% Subclinical hypothyroidism (SCH) (J Med Screen 2000)
Trimester-specific reference ranges (Thyroid, 2011)
15 ~ 20 % SCH (?)

Sample Trimester-Specific Reference Intervals for Serum TSH
Trimester
Reference First Second Third
Haddow † 0.94 (0.08-2.73) 1.29 (0.39-2.70)
Stricker ‡ 1.04 (0.09-2.83) 1.02 (0.20-2.79) 1.14 (0.31-2.90)
Panesar † 0.8 (0.03-2.30) 1.1 (0.03-3.10) 1.3 (0.13-3.50)
Soldin ‡ 0.98 (0.24-2.99) 1.09 (0.46-2.95) 1.2 (0.43-2.78)
Bocos-Terraz ‡ 0.92 (0.03-2.65) 1.12 (0.12-2.64) 1.29 (0.23-3.56)
Marwaha † 2.10 (0.60-5.00) 2.40 (0.43-5.78) 2.10 (0.74-5.70)
(Thyroid 2011)†: 5th and 95th pefcentile, ‡: 2.5 th and 97.5th percentile
1st trimester : 0.1 ~ 2.5 mIU/L
median

제일병원 TSH 정상치 0.30 - 4.5 mU/L
(2011 년 )임신 초기산모
TSH 정상 상한치를 4.5 에서 2.5 mU/L 로 변경
임신 초기산모 1,826 명중 , TSH > 2.5 인 경우가 387 명 (21.0 %)

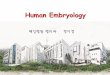
6 7 8 9 10 11 12 13 140
50
100
150
5 6 7 8 9 10 11 12 130.0
1.0
2.0
3.0
4.0
Gestational age (weeks)
TS
H (m
U/L
)
95th
50th
5th
Gestational age (weeks)
Num
bers
Gestational age-specific reference ranges for TSH
2012

4 5 6 7 8 9 10 11 12 130
1
2
3
4
5
6
5 6 7 8 9 10 11 12 130
200
400
600
800
1000
1200
1400
1600
1800
2000
Gestational age (weeks) Gestational age (weeks)
Num
bers
TSH 95th
50th
5th
2010-2015

(J Clin Endocrinol Metab, 2014)

Reporting Thyroid Function Tests in Pregnancy.
(Clin Biochem Rev 2015)
TSH may be affected by many factors including gestational age, analytical method, the antibody status, ethnicity, iodine nutrition and collection time of day.
Numerous papers show that a more realistic figure is between 3.0 and 4.0 mIU/L.
Thyroid Function in Pregnancy: What Is Normal?
(Clin Chem 2015)
Do not rely on fixed universal cutoff concentration, but calculate their own pregnancy-specific reference.

Subclinical Hypothyroidism in Pregnancy: A Systematic Review and Meta-Analysis
(Thyroid 2016)

Subclinical hypothyroidism (SCH)
Many studies association between SCH and adverse preg-nancy outocome (increased risk of placental abruption, preterm delivery, miscarriage, breech presentation)
Some studies no association

Pooled Relative Risk with 95% Confidence Interval Comparing Pregnant Women with SCH to Pregnant Euthyroid Women for All Pregnancy Outcomes
(Thyroid, 2016)

Universal Screening vs Case Finding for Detection and Treatment of Thyroid Hormonal Dysfunction During pregnancy (Negro R, JCEM 2010)
Women assessed 4657 95 excluded for known thy-
roid disease
Randomized4562
Case finding2282
Universal screening2280
Analyzed 2282
High risk454
Euthyroid432
Hypothyroid20
Hyperthyroid2
Low risk1828
Euthyroid1789
Hypothyroid34
Hyperthyroid5
Analyzed 2280
High risk482
Euthyroid461
Hypothyroid19
Hyperthyroid2
Low risk1789
Euthyroid1747
Hypothyroid44
Hyperthyroid7

Number of women experiencing at least one adverse outcome
Case finding (n=2257) Universal screening (n=2259)
High risk Low risk Total High risk Low risk Total
Euthyroid without Ab
166 (41.3%) 659 (39.5%) 824 (39.9%) 179 (41.7%) 637 (39.1%) 816 (39.7%)
Euthyroid with Ab
10 (40%) 49 (47.1%) 59 (45.7%) 13 (48.1%) 45 (42.9%) 58 (43.9%)
Hypothyroid 9 (45%) 31 (91.2%) 40 (74.1%) 6 (31.6%) 15 (34.9%) 21 (33.9%)
Hyperthyroid 2 (100%) 5 (100%) 7 (100%) 1 (50%) 4 (57.1%) 5 (55.5%)
Total 187 (41.7%) 742 (41.1%) 930 (41.2%) 199 (41.7%) 701 (40.5%) 900 (39.8%)
(Negro R, JCEM 2010)

Effects of Levothyroxine Therapy on Pregnancy Outcomes in Women with Subclinical Hypothyroidism
(Maraka S, Thyroid 2016)

Association of maternal thyroid function during early pregnancy with off-spring IQ and brain morphology in childhood: a population-based prospective cohort study
(Korevaar T, Lancet Diabetes Endocrinol. 2016)
3,839 mother-child pairs, serum sample at early pregnancy(<18 weeks)

The association between SCH in pregnancy and impaired neuropsychological development of the offspring is inconsistent.

Controlled Antenatal Thyroid Screening (CATS) (Lazarus JH, N Engl J Med 2012)
21,846 women
10,924 Screening(Assay within 1 wk)
10,922 Control
499 (4.6%) tested positive242 low fT4
232 high TSH25 low fT4 & high TSH
499 LT4 at 13 gwk
390 childrenpsychological test
404 childrenpsychological test
(Assay after delivery)
551 (5.0%) tested positive257 low fT4
264 high TSH30 low fT4 & high TSH

(Lazarus JH, N Engl J Med 2012)
Screening Gr(N=390)
Control Gr(N=404)
G wks median 12.3 12.3 NS interquartile range 11.6 – 13.6 11.6 – 13.5 NS
TSH (median) median 3.8 3.2 NS interquartile range 1.5 – 4.7 1.2 – 4.2 NSIQ mean 99.2 ± 13.3 100.0 ± 13.3 0.40 <85 (% of children) 12.1 14.1 0.39

Effect of treatment of maternal subclinical hypothyroidism or hypothyroxinemia on IQ in offspring
(AJOG supp 2016)2006 ~ 2009, 97,226 pregnant women 3,058 SCH (TSH > 4.0 & normal fT4) -> 677 1,110 Hypothyroxinemia (fT4 < 0.86 & nomal TSH) -> 526Randomized double-masked, placebo-controlled trial mean gest. wks = 17 weeks
Placebo Levothyroxine P valueSCH N=325 N=323 94 [85, 107] 97 [85, 105] 0.76Hypothyroxinemia N=253 N=254
91 [82, 101] 94 [83, 101] 0.30
Data shown as Median IQ Score [25th %tile, 75th %tile]

(ATA 2011)TAb+ & SCH pregnant women should be treated with LT4.
(Endo Society 2012)Recommends LT4 in SCH for obstetrical outcome.
(ETA 2014)SCH during gestation should be treated with LT4.

Endo Society (2012), committee did not reach consensus on the screening.
“Some members recommended screening” “Some members recommended neither for nor against uni-
versal screening. These members strongly support ag-gressive case finding”
TSH screening in pregnant women?

The current recommendations for targeted screening for women at high risk for thyroid dysfunction
Endocrine Society (2012) American Thyroid Association (2011)Aged > 30 years Aged > 30 FHx of autoimmune thyroid disease orHypothyroidism
FHx of thyroid disease
Hx of thyroid surgery Hx of thyroid dysfunction and/or thyroid opGoiter GoiterThyroid antibodies Thyroid antibodiesSx or signs of thyroid hypofunction Sx or signs suggestive of hypothyroidismT1DM or other autoimmune disorders T1DM or other autoimmune disordersHx of miscarriage or preterm delivery Hx of miscarriage or preterm deliveryInfertility InfertilityPrior head or neck irradiation Prior head or neck irradiationCurrent levothyroxine replacement Living in a region with iodine deficiency Morbid obesity Treated with amiodarone or lithium Recent exposure to contrast agents

Screened thyroid function in 1560 pregnant women,
413 women (26.5%), as a high-risk group (PHx or FHx of thyroid disorder)
12 of 40 women with raised TSH (30%) were in the low-risk group.
(Vaidya B, J Clin Endocrinol Metab, 2005)
1600 pregnant women in first trimester,
Of women with thyroid dysfunction, 35.6% were in the low-risk group.
(Nazarpour S, Eur J Endocrinol. 2016 )

10,320 pregnant women in Cheil Hospital
384 pregnant women (TSH > 4.5)
PHx(-) & FHx(-) of thyroid dis: 225 (58.5%)
34 pregnant women (TSH > 10) : Overt hypothyroidism
PHx(-) & FHx(-) of thyroid dis: 17 (50.0%)

(in Cheil Hospital)
10,320 Pregnant women(mean age 33.5 ± 3.9 yrs, median IUP 6.7 wks)
Age > 30 yrs 7,860PHx of thyroid disease 673FHx of thyroid disease 626Age > 30 yrs or PHx or FHx 8,807
Low risk1,513 women
(14.7%)
High risk8,807 women
(85.3%)

- In 2010, Questionnaire survey (605 members of the ETA), 42% responders screened all pregnant women
for thyroid dysfunction.
- Annual Meeting of ATA, 2013Universal screening was recommended by 74%
of the survey respondents.

Screening Pregnant Women for Overt Thyroid Disease
(Alex Stagnaro-Green, JAMA 2015)
Even if the studies demonstrate no benefit of treating SCH, the available evidence supports routine screening of preg-
nant women for overt thyroid disease.

Although there are still no well-controlled studies to justify
universal screening, the majority of the authors
recommend universal screening because of the beneficial
effects of LT4 Tx on unknown overt hypothyroidism, on
obstetric outcome and the fact that the targeted approach
will miss a large percentage of women with SCH.(2014 ETA guideline)




![Management of Thyroid Dysfunction during Pregnancy and … · 2012. 8. 20. · ¢/ID `¨ ¿]]] IUMUTROTK IUS Management of Thyroid Dysfunction during Pregnancy and Postpartum: An](https://img.pdfslide.tips/doc/110x75/5fbd422e6d9f6524ba4d6be2/management-of-thyroid-dysfunction-during-pregnancy-and-2012-8-20-id-.jpg)