Embed Size (px)
DESCRIPTION
Predict of coronary artery lesions (CAL) in Kawasaki disease (KD)
Citation preview
Heidelberg, Germany
Predict CAL formation in Kawasaki disease
郭和昌 醫師
高雄長庚醫院 兒童過敏免疫風濕科長庚大學臨研所
June 30, 2010
郭和昌 醫師
• 國立陽明大學醫學士• 長庚大學臨床醫學研究所博士班進修• 中華民國小兒科專科醫師• 中華民國免疫過敏專科醫師• 台灣兒童過敏氣喘暨免疫學會專科醫師
• 美國過敏氣喘免疫學會 (AAAAI) 會員• 歐洲過敏氣喘及臨床免疫學會 (EAACI) 會員• 亞洲兒科醫學研究學會 (ASPR) 會員
• 高雄長庚助理教授級主治醫師 (2010~)• 長庚大學兼任講師 (2009~)• 教育部審訂講師 (2009~)
• 川崎症專屬部落格• http://tw.myblog.yahoo.com/erickuo48
Rotenberg, Germany
9th IKDS, April 10-12, 2008 Taipei, Taiwan.
十大棘手兒少疾病 川崎病排第一• 該 會經近五百名兒科專科醫師會員,票選出
十大連兒科醫師都不免感到棘手的兒少疾病,依序為
• 川崎病、• 心肌炎、• 腸病毒重症、• 腸套疊、• 噬血症候群、• 闌尾炎、• 幼年型糖尿病、• 幼年型類風濕關節炎、• 腦膜炎及過敏性紫斑症。
2010/05/06 02:55 黃 天如/台北報導 中國時報【黃天如/台北報導】

『虛空有盡,我願無窮,我今生做不完的事,願在未來的無量生中繼續推動, 我個人無法完成的事,勸請大家共同推動』 --聖嚴法師
做儍事!


• Introduction
• Diagnosis
• Treatment
• Prognosis – CAL formation
– IVIG resistance
Content
西子灣
何謂川崎病 (Kawasaki disease) ?•是一種多系統血管發炎症候群•目前造成的原因仍不清楚•主要發生在嬰兒以及小於五歲的幼童•於 1974 年川崎富作 (Tomisaku Kawasaki) 醫師首先用英文發表五十位川崎氏症病患
• 到目前為止,川崎氏症的標準診斷仍完全依靠臨床症狀,還沒有任何一個具體的實驗室檢驗數據可用於確認及診斷川崎氏症。
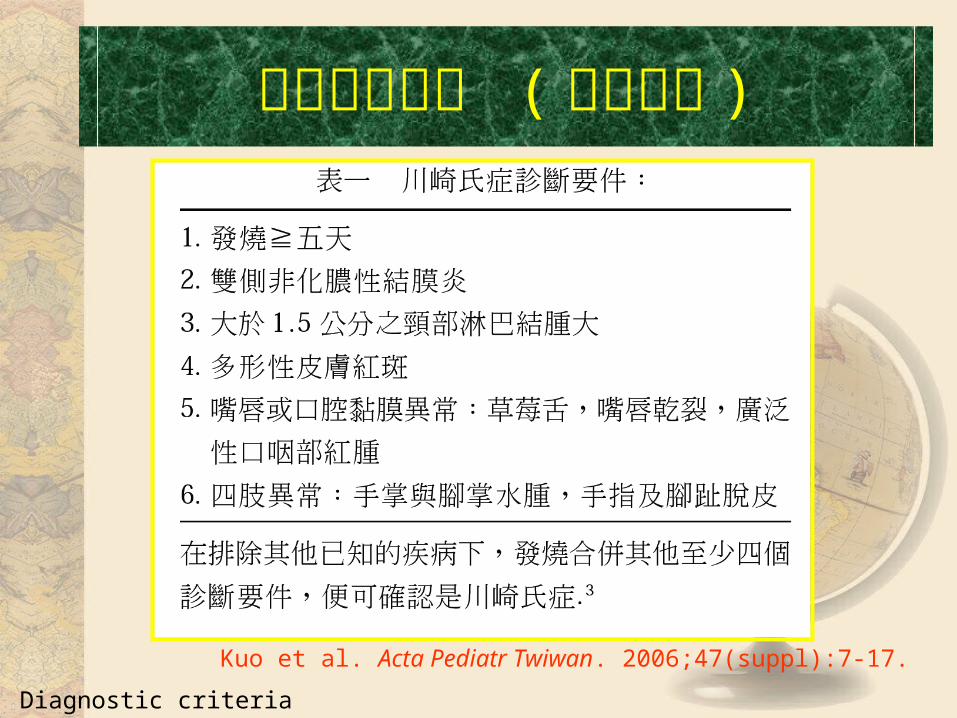
臨床表現特點 ( 診斷要件 )
Q1: Diagnostic criteria
Kuo et al. Acta Pediatr Twiwan. 2006;47(suppl):7-17.

Kawasaki Disease- 後天性心臟病之主因Kawasaki Disease- 後天性心臟病之主因
Involved small and medial size vessel Coronary artery aneurysm
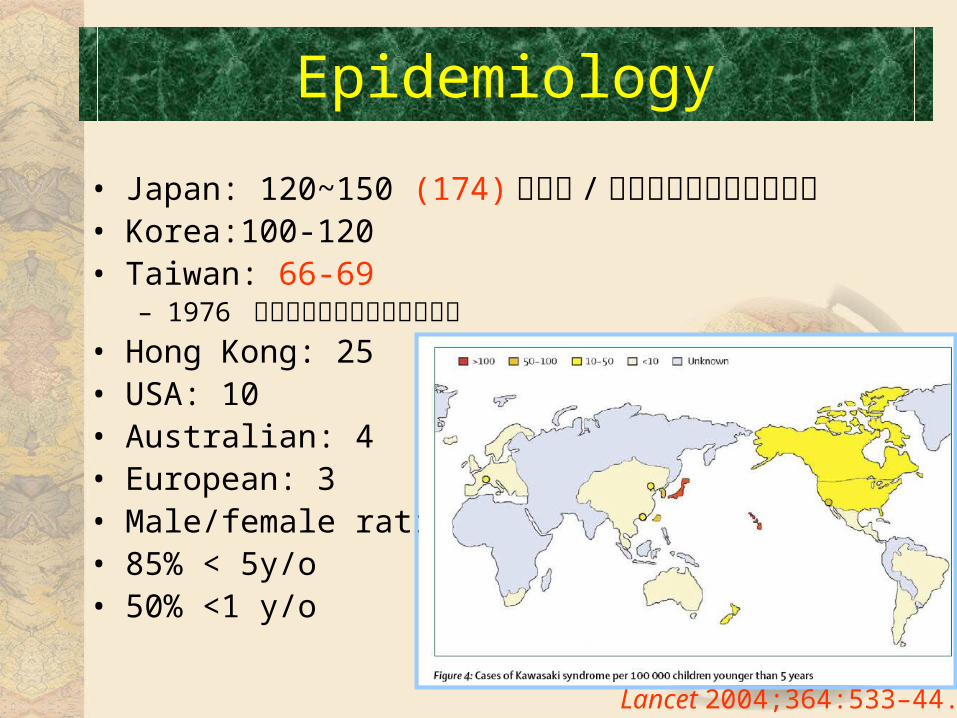
• Japan: 120~150 (174) 個案例 /每十萬名小於五歲的幼童• Korea:100-120• Taiwan: 66-69
– 1976 年首先有川崎氏症的案例報告• Hong Kong: 25• USA: 10• Australian: 4• European: 3• Male/female ratio: 1.4• 85% < 5y/o• 50% <1 y/o
Epidemiology
Lancet 2004;364:533–44.
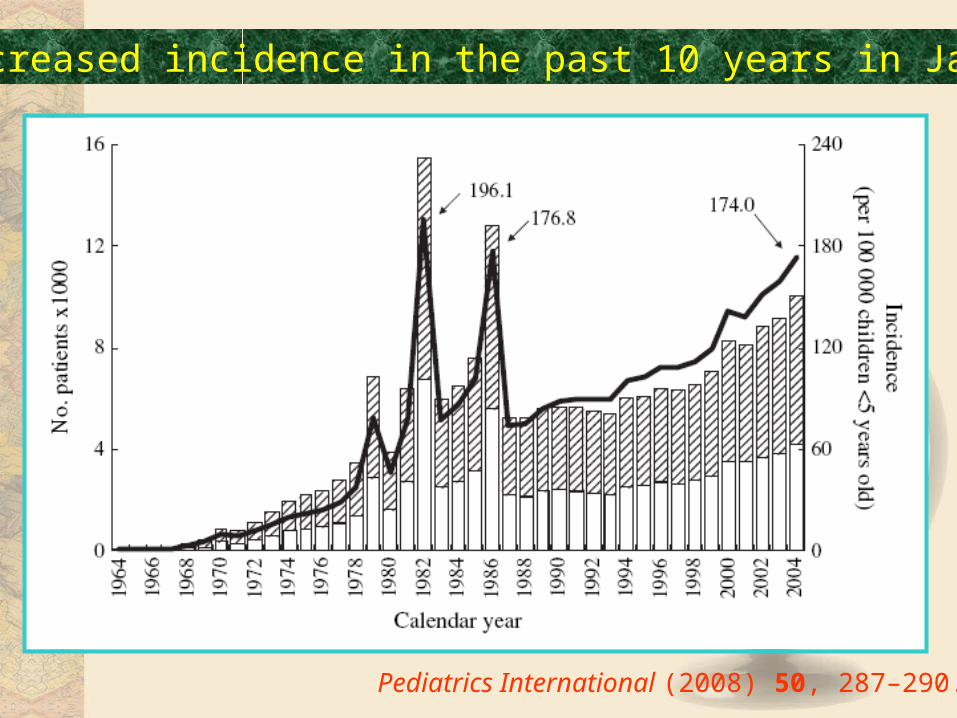
Pediatrics International (2008) 50, 287–290.
Increased incidence in the past 10 years in Japan
Pediatrics International (2008) 50, 287–290.
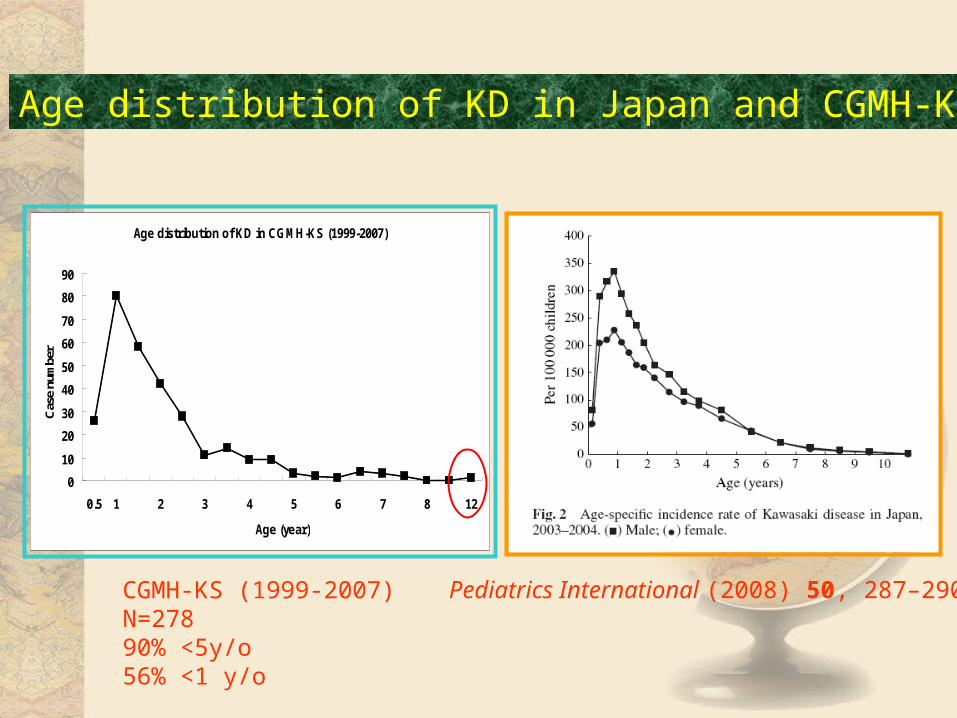
Age distribution of KD in Japan and CGMH-KS
Age distribution of KD in CGMH-KS (1999-2007)
0
10
20
30
40
50
60
70
80
90
0.5 1 2 3 4 5 6 7 8 12
Age (year)
Cas
e nu
mbe
r
CGMH-KS (1999-2007)N=27890% <5y/o56% <1 y/o
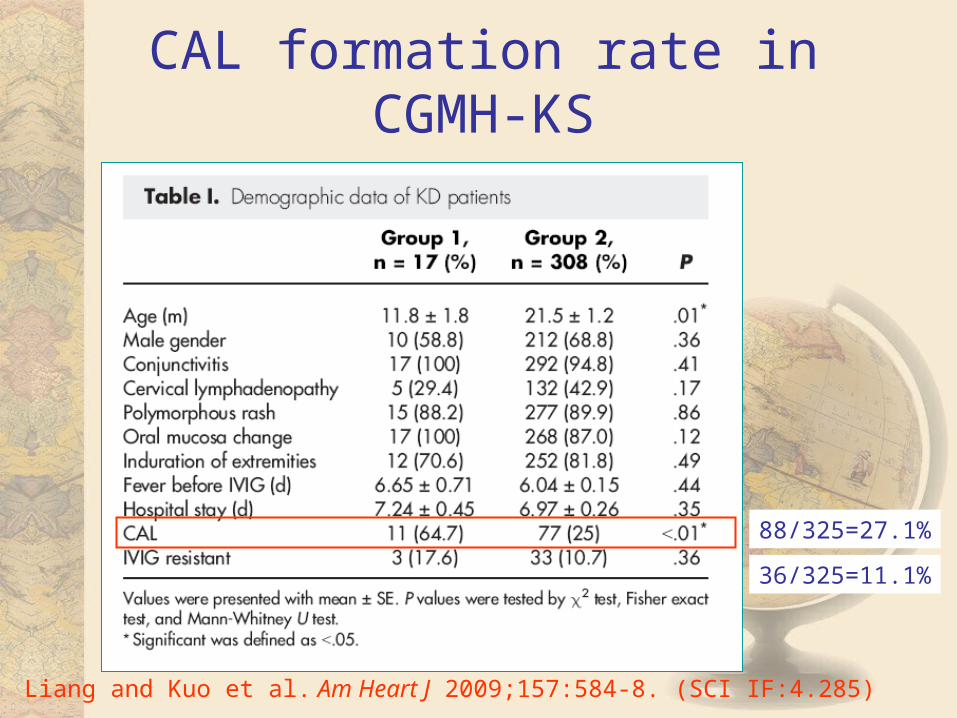
CAL formation rate in CGMH-KS
Liang and Kuo et al. Am Heart J 2009;157:584-8. (SCI IF:4.285)
88/325=27.1%
36/325=11.1%
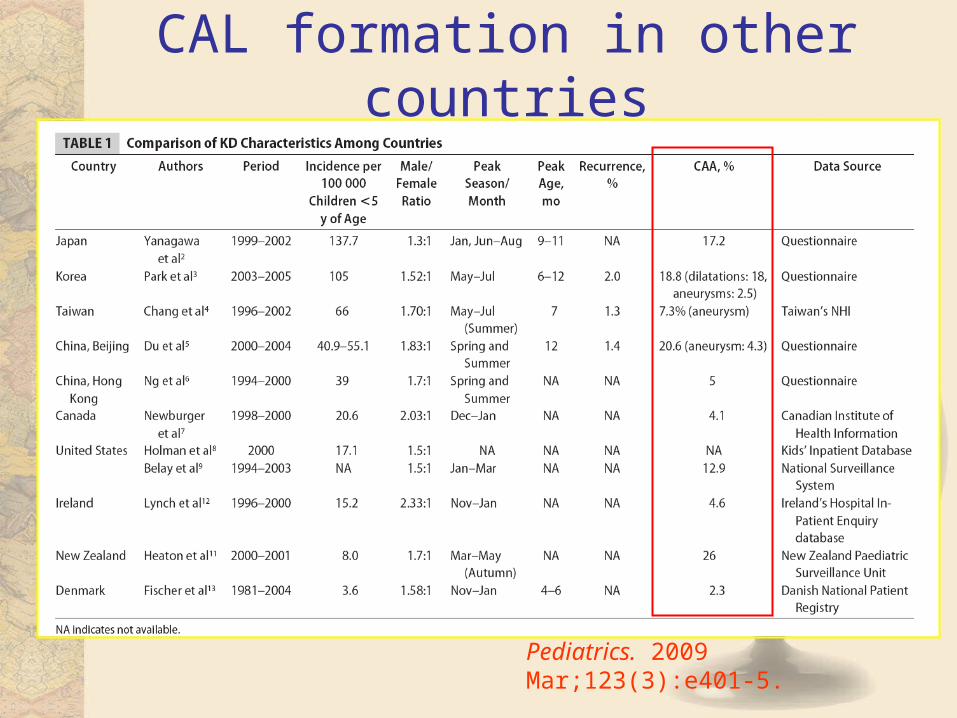
CAL formation in other countries
Pediatrics. 2009 Mar;123(3):e401-5.
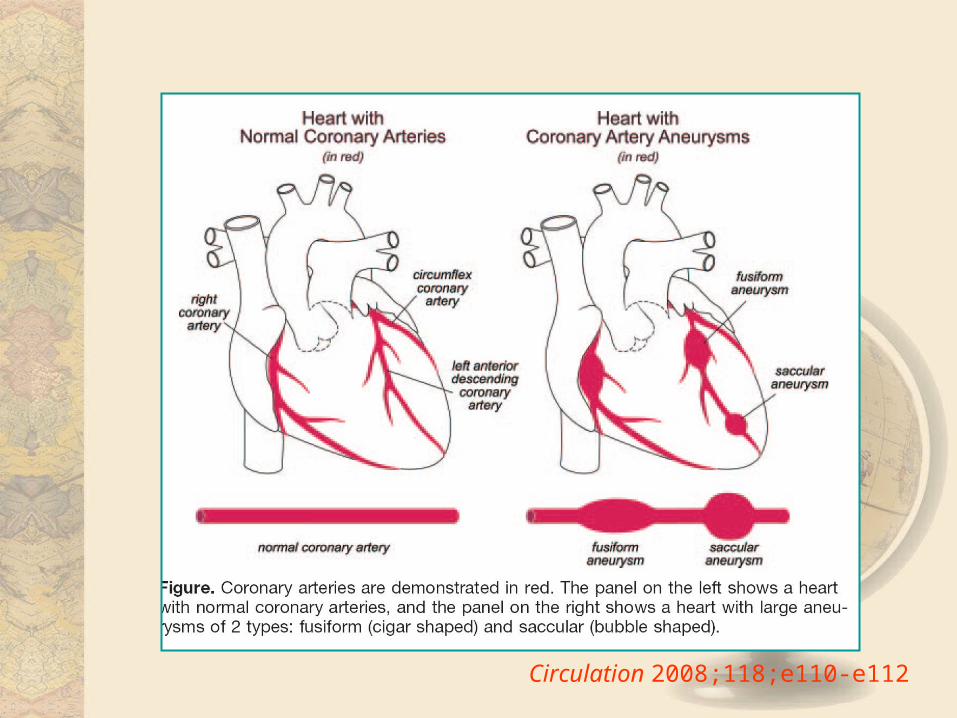
Circulation 2008;118;e110-e112

南靖土樓
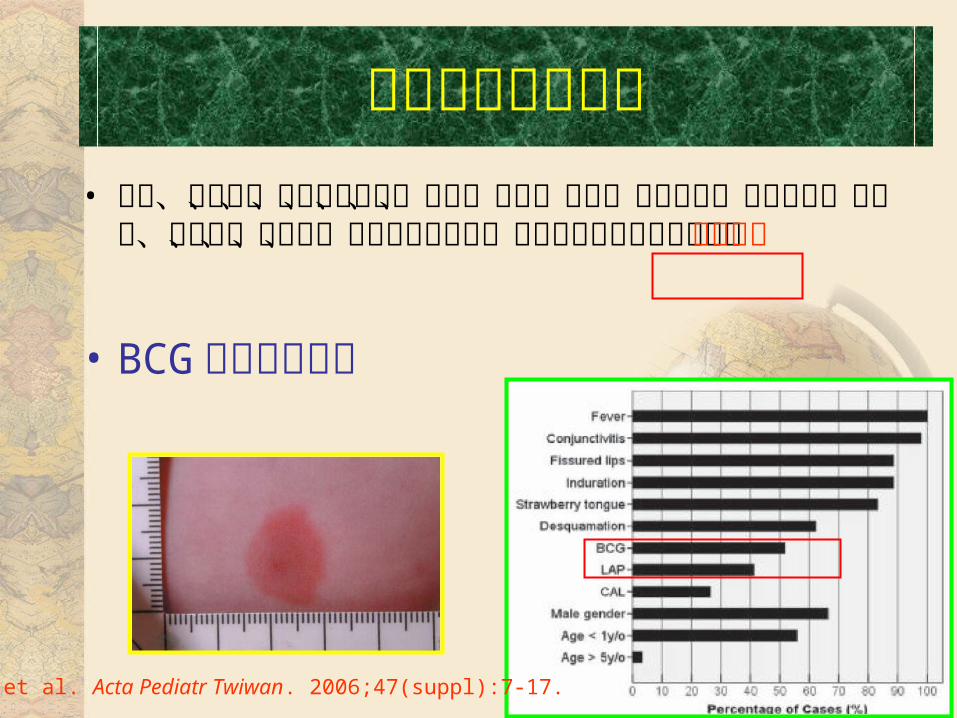
• 躁動、虹彩炎、無菌性腦膜炎、咳嗽、嘔吐、腹瀉、腹部疼痛、膽囊水腫、尿道炎、關節痛、關節炎、白蛋白指數低下、肝功能上升以及心臟衰竭、步態不穩
• BCG 接種部位反應
Kuo et al. Acta Pediatr Twiwan. 2006;47(suppl):7-17.
非特異性臨床特徵
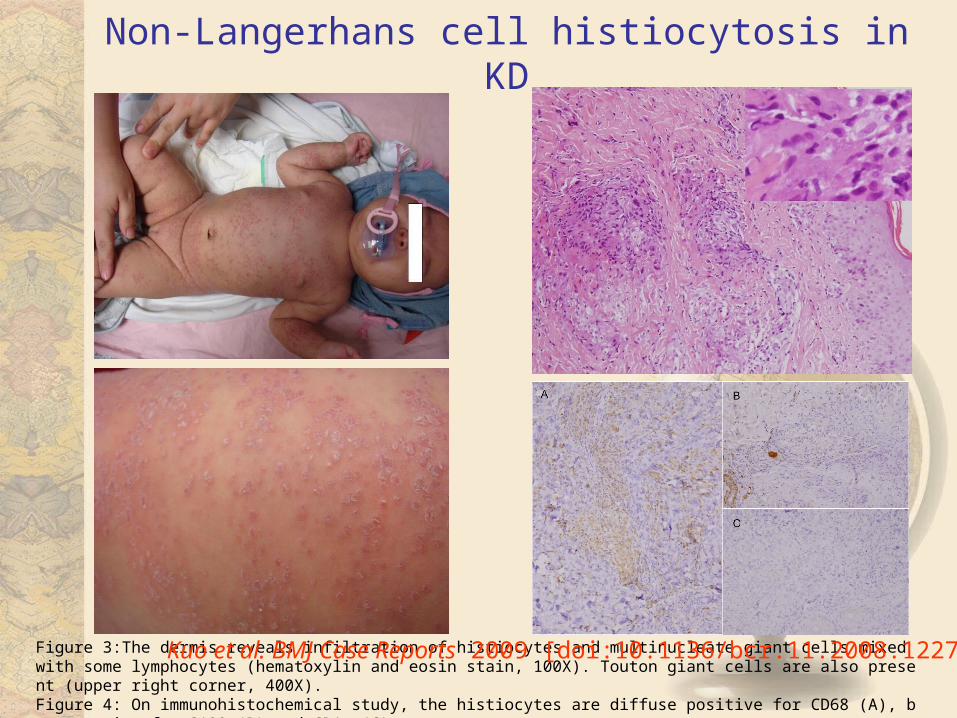
Non-Langerhans cell histiocytosis in KD
Figure 3:The dermis reveals infiltration of histiocytes and multinucleate giant cells mixed with some lymphocytes (hematoxylin and eosin stain, 100X). Touton giant cells are also present (upper right corner, 400X). Figure 4: On immunohistochemical study, the histiocytes are diffuse positive for CD68 (A), but negative for S100 (B) and CD1a (C).
Kuo et al. BMJ Case Reports 2009 [doi:10.1136/bcr.11.2008.1227]
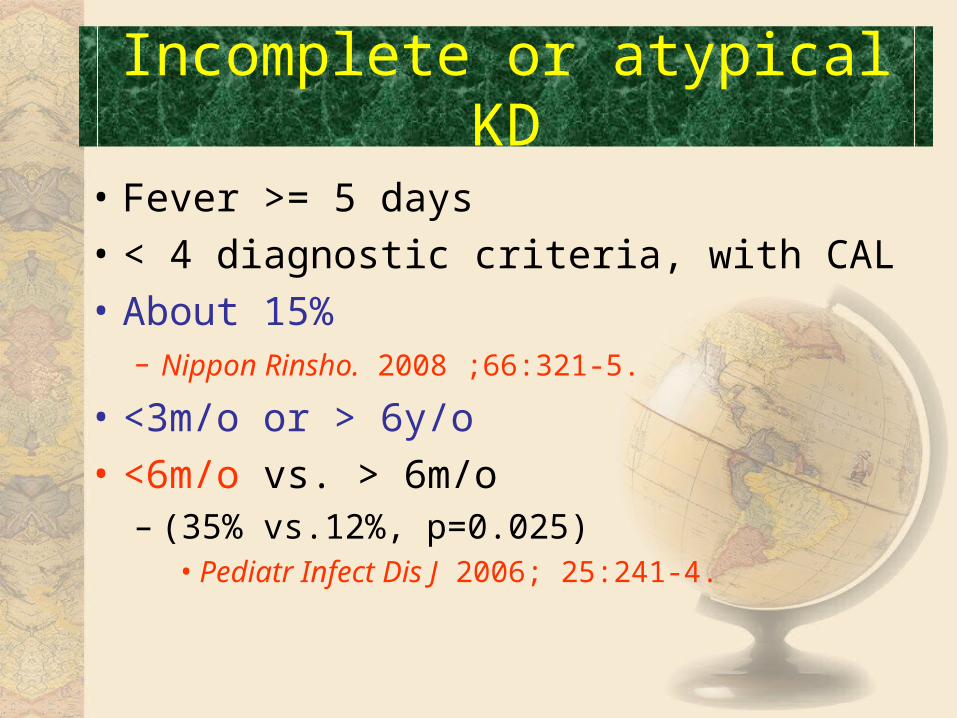
• Fever >= 5 days
• < 4 diagnostic criteria, with CAL
• About 15%– Nippon Rinsho. 2008 ;66:321-5.
• <3m/o or > 6y/o
• <6m/o vs. > 6m/o – (35% vs.12%, p=0.025)
• Pediatr Infect Dis J 2006; 25:241-4.
Incomplete or atypical KD
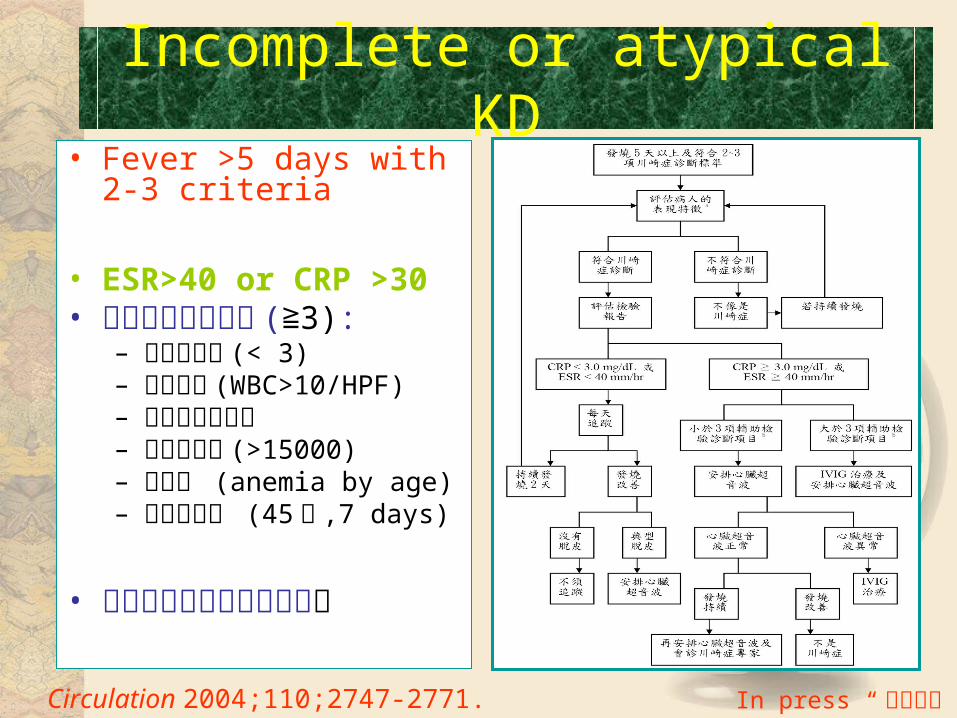
• Fever >5 days with 2-3 criteria
• ESR>40 or CRP >30• 輔助性的診斷指標 ( 3)≧ :
– 白蛋白指數 (< 3)– 尿液檢查 (WBC>10/HPF)– 肝功能指數異常– 白血球數量 (>15000)– 血色素 (anemia by age)– 血小板數目 (45萬 ,7 days)
• 排除其他類似之臨床疾患。
Circulation 2004;110;2747-2771.
Incomplete or atypical KD
In press “護理雜誌”
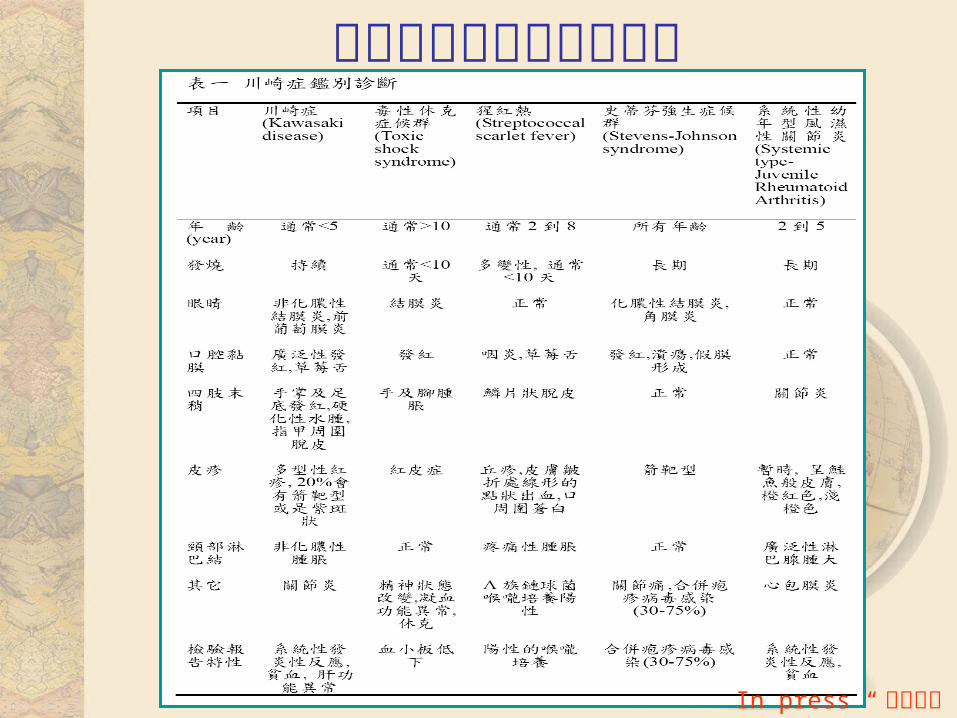
排除其他類似之臨床疾患
In press “護理雜誌”
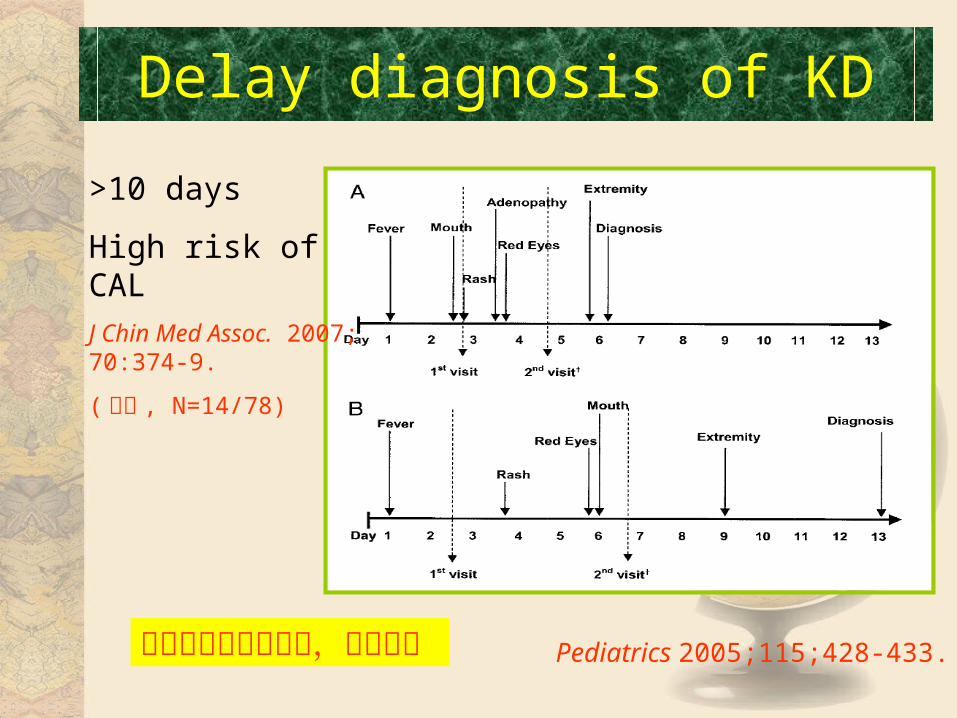
Delay diagnosis of KD
Pediatrics 2005;115;428-433.
>10 days
High risk of CAL
J Chin Med Assoc. 2007;70:374-9.
( 北榮 , N=14/78)
醫師心中要有川崎病,才能確診

廈門環島路夜景
Treatment
• High dose IVIG (2gm/kg) in 12 hours• Aspirin (80-100 mg/kg) in acute stage• Aspirin (3-5 mg/kg) after fever subside
– Normal ESR, Plt and 2D echo • Aspirin: (should receive an annual influenza vaccine)
– 北美地區 (80~100mg/kg/day) Nelson textbook• Circulation 1993; 87:1776-80.
– 日本地區中等劑量 (30~50mg/kg/day)• Prog Clin Biol Res 1987; 250:401-13.
– Hsieh KS et al. 於 1993~2003 統計 162 位 KD• Pediatrics 2004; 114;689-93.
Treatment
History of IVIG in KD
• 1981: Imback: IVIG in ITP (Lancet)
• 1983: Furusho: IVIG in 40 Japanese patients with KD (Lancet)
• 1986: US Multicenter KD Study Group: 168 KD patients, 400mg/kg x 4 d reduces CAA from 20% to 3-5 % (NEJM)
• 1991: US Multicenter KD Study Group: 549 US patients, single infusion of 2 g/kg superiors to 400mg/kg x 4d in reducing fever and inflammatory markers (NEJM)
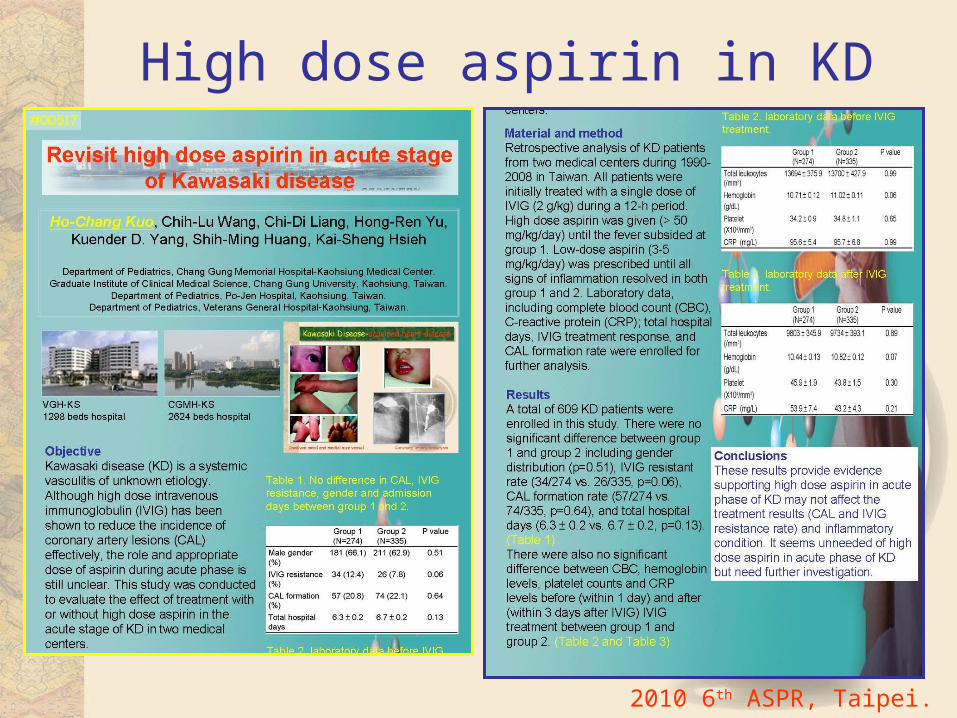
High dose aspirin in KD
2010 6th ASPR, Taipei.
• Day 4– Early IVIG treatment for KD: the nationwide
surveys in Japan. • J Pediatr 2005;146:149-50.
• Day 5– 15,940 KD patients in Japan
• Pediatr Infect Dis J. 2008;27:155-160.
Treatment- IVIG timing
Definition of IVIG resistance
• Persistent or recrudescent fever BT>38.0 C or 100.4 F) 36 hrs following end of IVIG infusion
• Workshop of KD investigators held in Chicago 2006: resistance preferred over “failure” or “non-response”
• 約 7.8%~38%– Pediatr Cardiol. 2003;Pediatr Infect Dis J. 1998– J Pediatr. 2008 Jul;153(1):117-21.
• Our hospital: 10.8% (30/278)• 3-4% non-response to 2nd dose IVIG
– 4/278 (1.4 % in our hospital)
• 20% in Japan– Nippon Rinsho. 2008;66:332-7.
• Recurrent KD: 6.89 per 1000/years– Acta Paediatr. 2001;90:40-4.
• 2/278 (0.72% in our hospital)
Initial IVIG-resistance
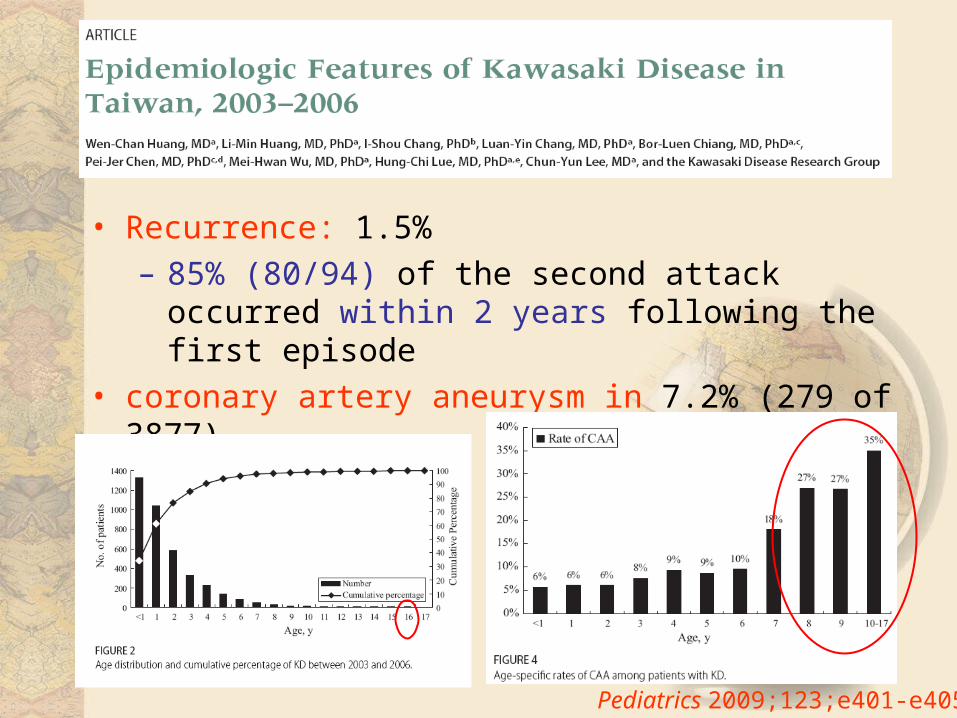
• Recurrence: 1.5% – 85% (80/94) of the second attack occurred within 2
years following the first episode • coronary artery aneurysm in 7.2% (279 of 3877)
Pediatrics 2009;123;e401-e405
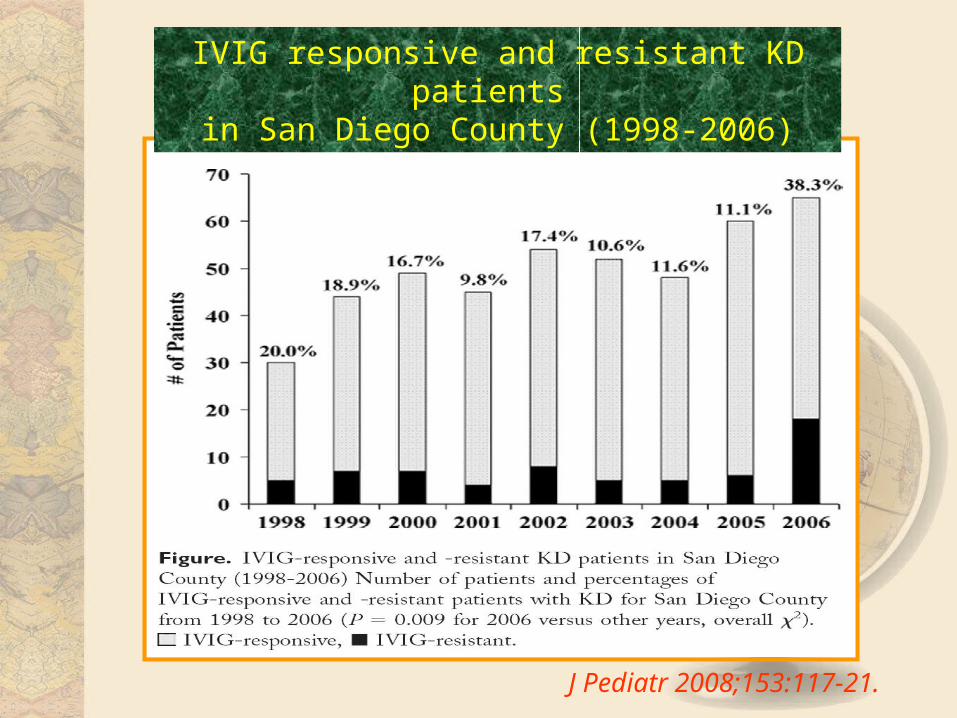
J Pediatr 2008;153:117-21.
IVIG responsive and resistant KD patients in San Diego County (1998-2006)
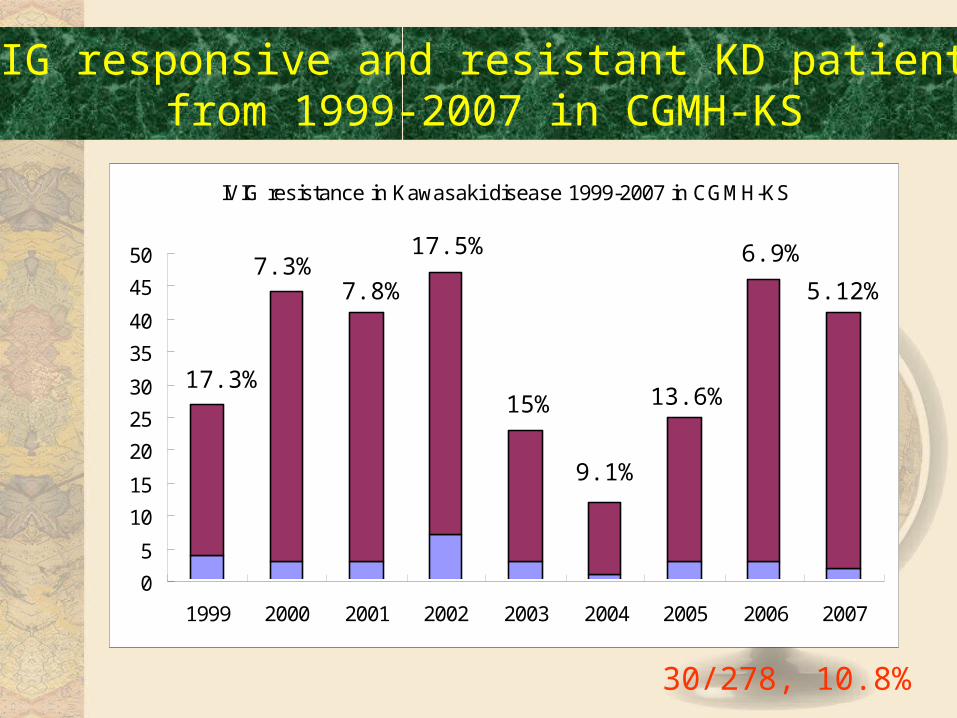
IVIG resistance in Kawasaki disease 1999-2007 in CGMH-KS
0
5
10
15
20
25
30
35
40
45
50
1999 2000 2001 2002 2003 2004 2005 2006 2007
30/278, 10.8%
IVIG responsive and resistant KD patients from 1999-2007 in CGMH-KS
17.3%
7.3%7.8%
17.5%
15%
9.1%
13.6%
6.9%
5.12%
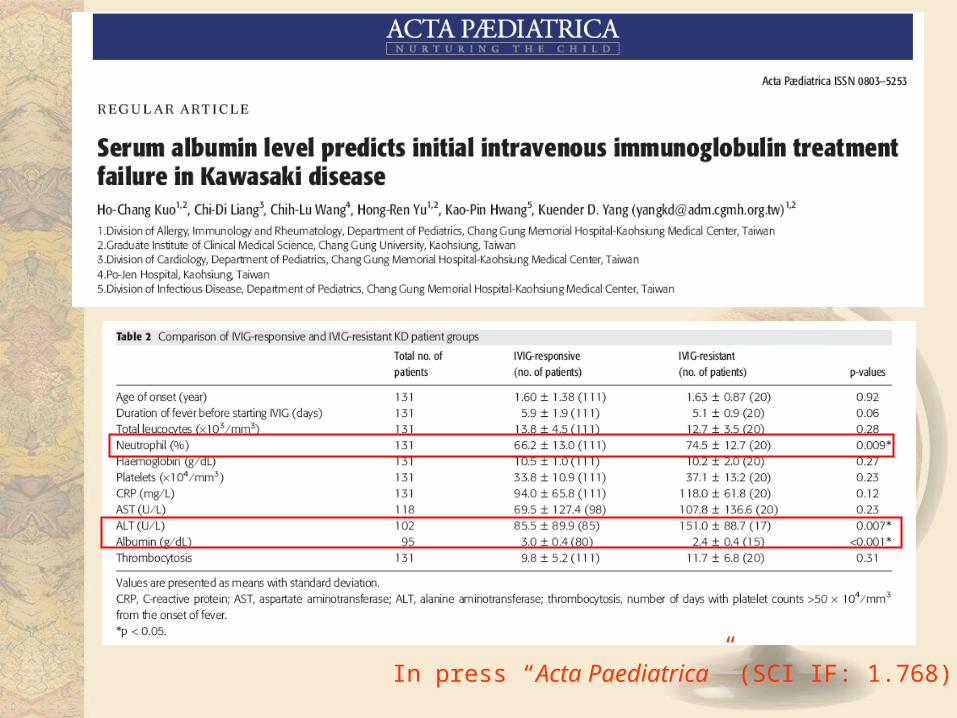
In press “Acta Paediatrica” (SCI IF: 1.768)
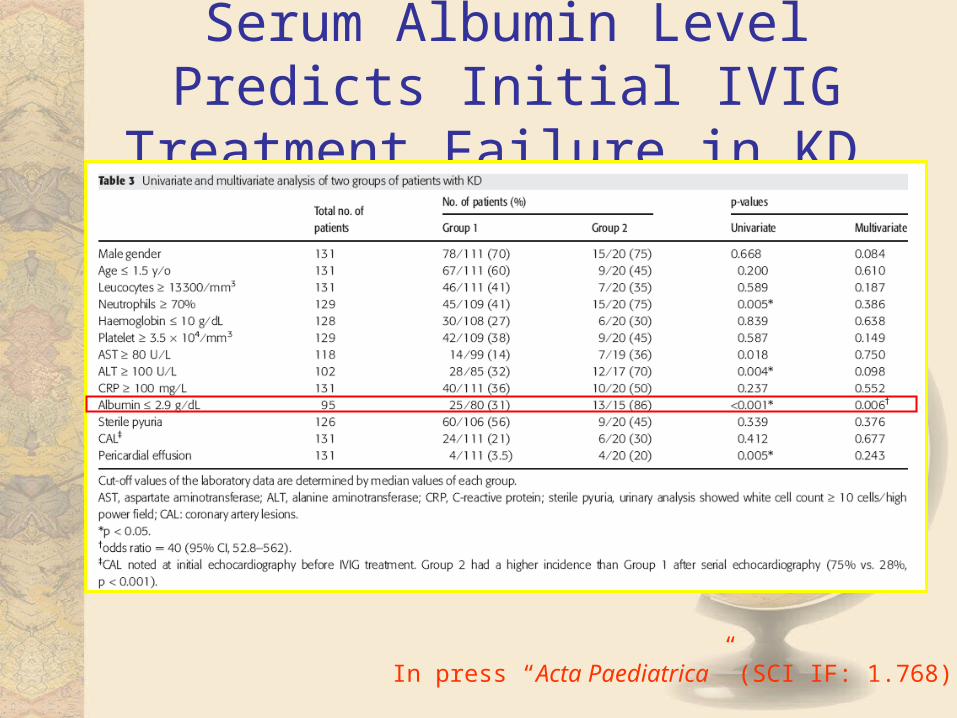
Serum Albumin Level Predicts Initial IVIG Treatment Failure in KD
In press “Acta Paediatrica” (SCI IF: 1.768)
• Repeat IVIG• Methylpredinsolone pulse• Cyclosporin• Cyclophosphamide• Methotrexate
– Scand J Rheumatol 2005;34:136-9.• Plasma exchange
– Eur J Pediatr. 2004;163:263–264.• Pentoxifylline (inhibit TNF mRNA)
– Eur J Pediatr. 1994;153:663–667.• Abciximab• Enbrel • Ulinastatin
– trypsin inhibitor
Other Treatment
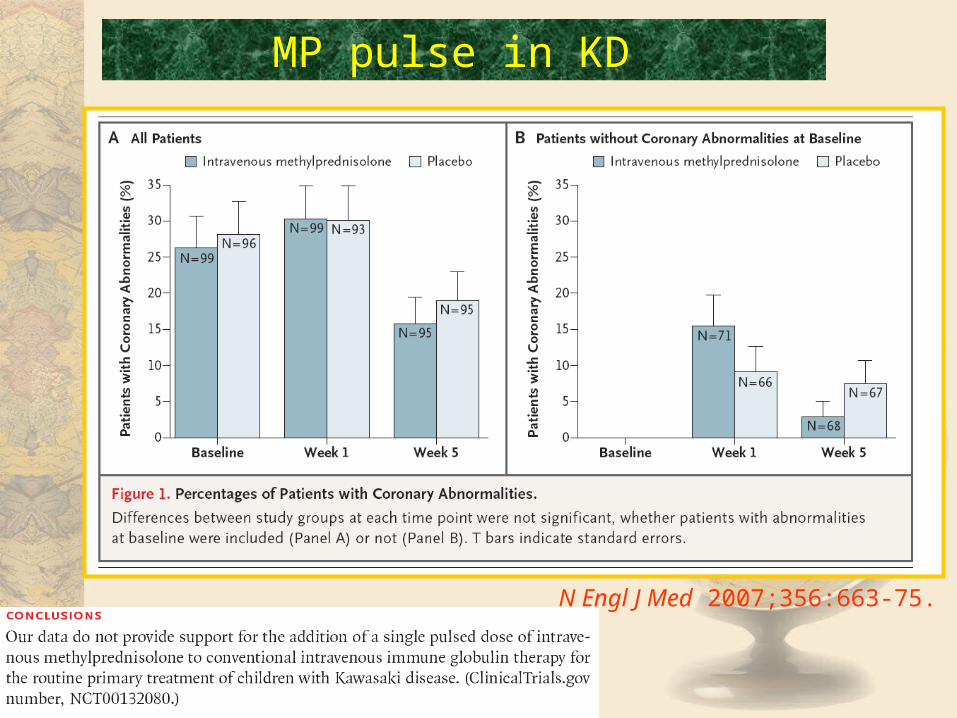
N Engl J Med 2007;356:663-75.
MP pulse in KD
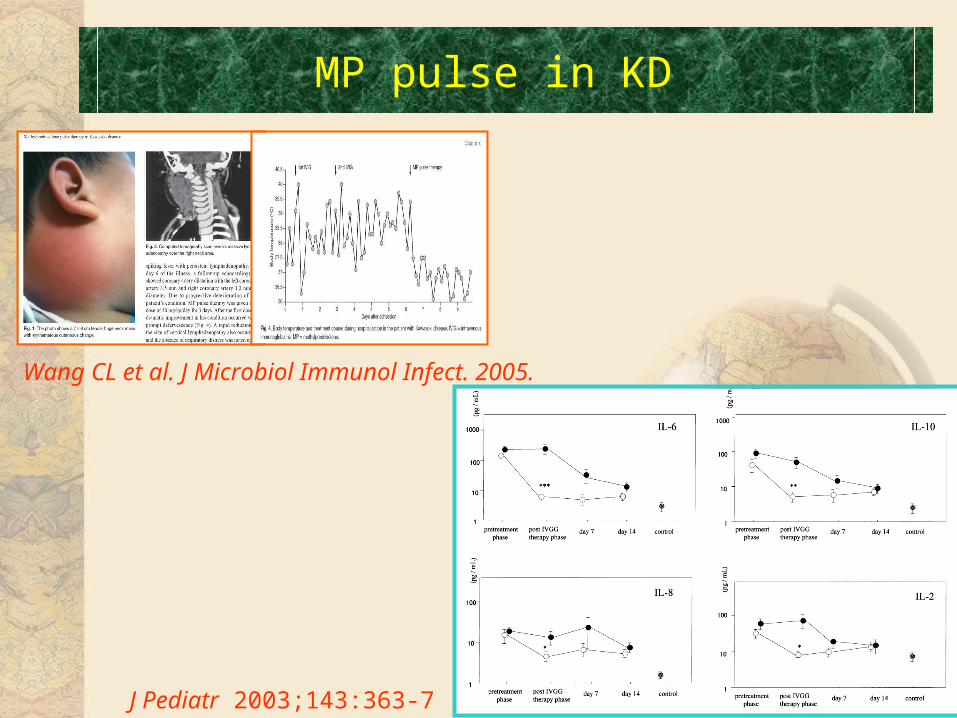
MP pulse in KD
Wang CL et al. J Microbiol Immunol Infect. 2005.
J Pediatr 2003;143:363-7
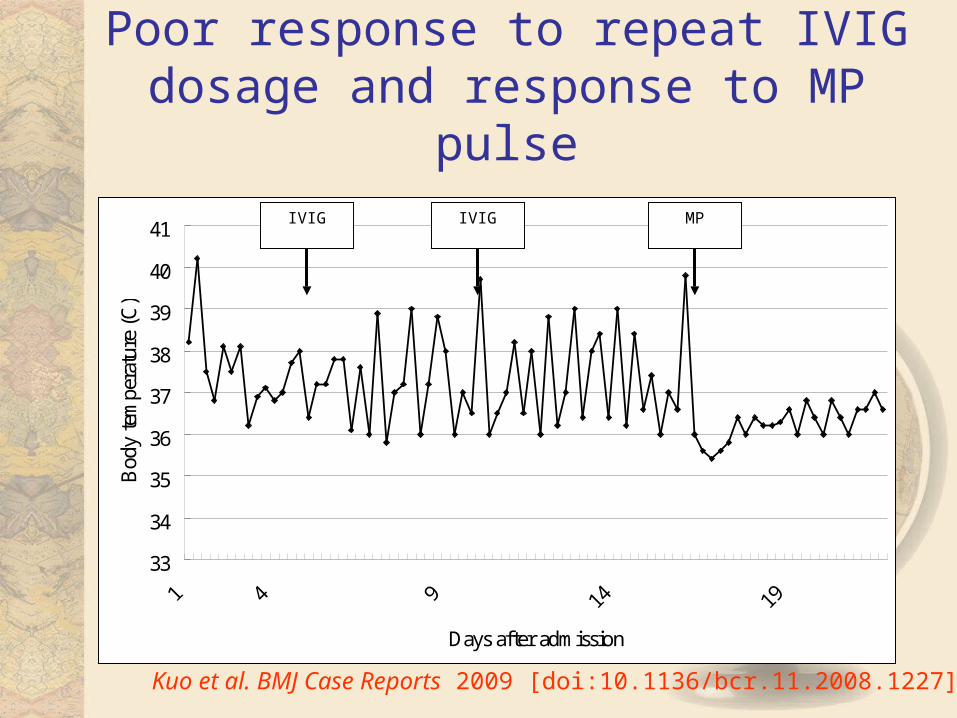
Poor response to repeat IVIG dosage and response to MP pulse
33
34
35
36
37
38
39
40
41
Days after admission
Bod
y te
mpe
ratu
re (
C)
IVIG IVIG MP
Kuo et al. BMJ Case Reports 2009 [doi:10.1136/bcr.11.2008.1227]
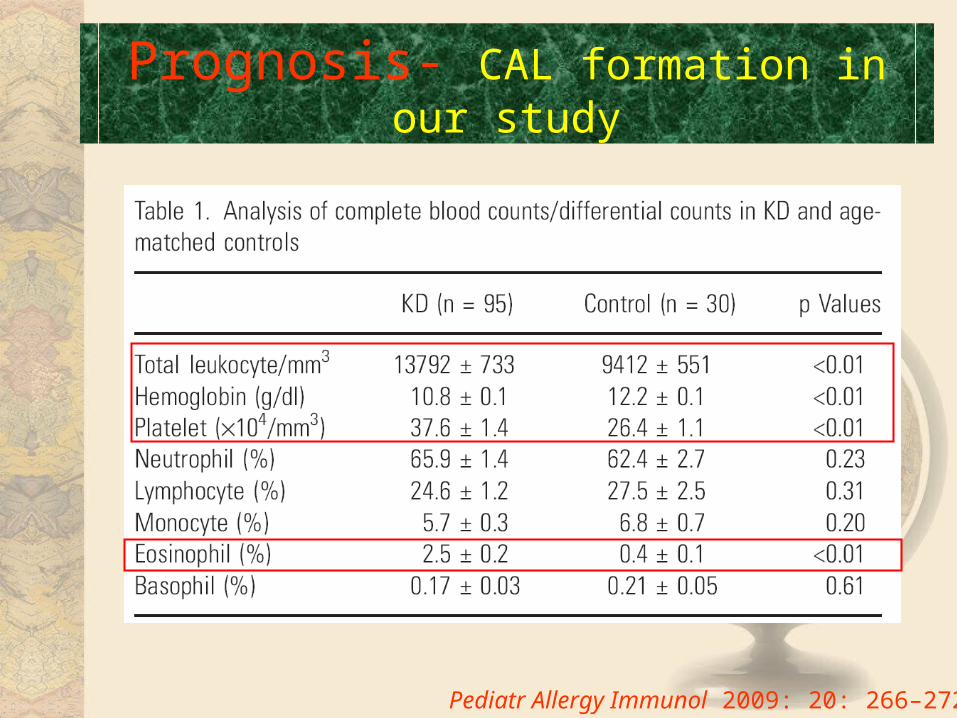
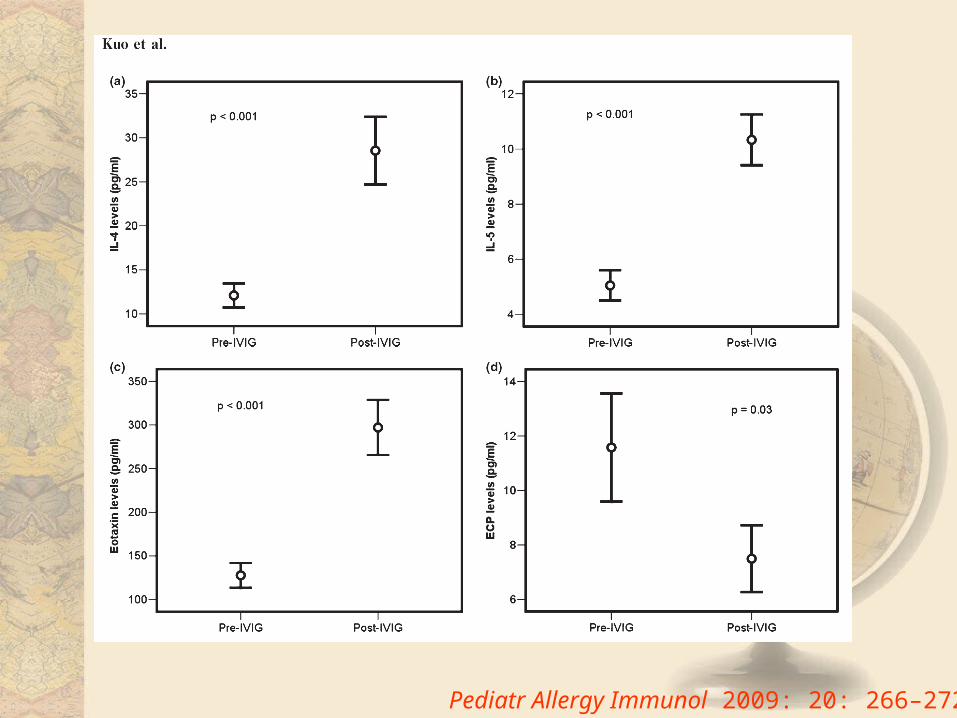
Prognosis- CAL formation in our study
Pediatr Allergy Immunol 2009: 20: 266–272.
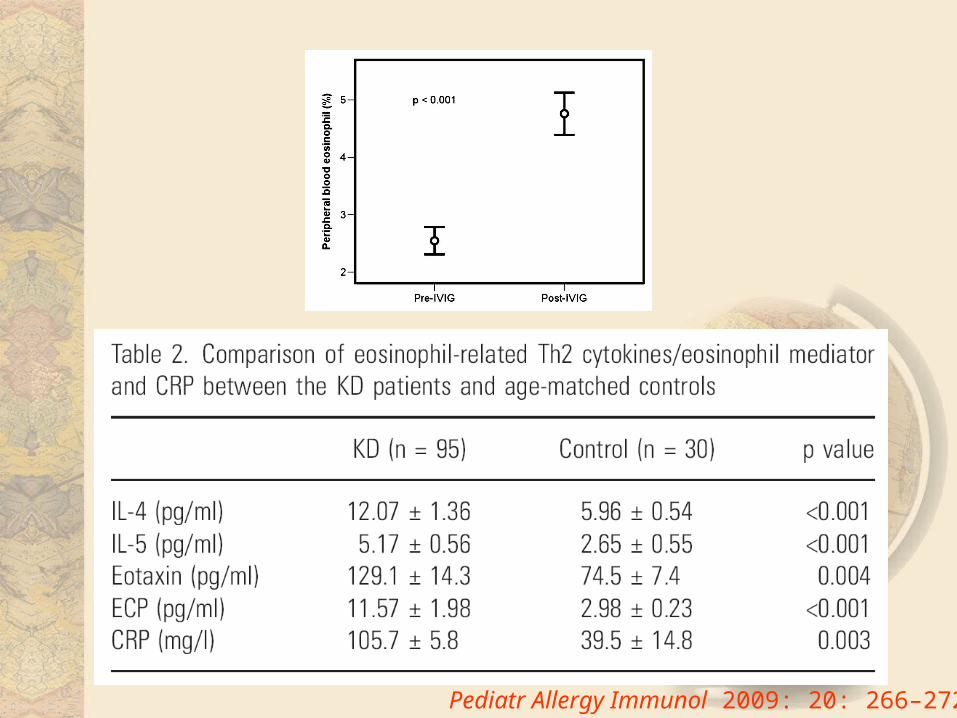
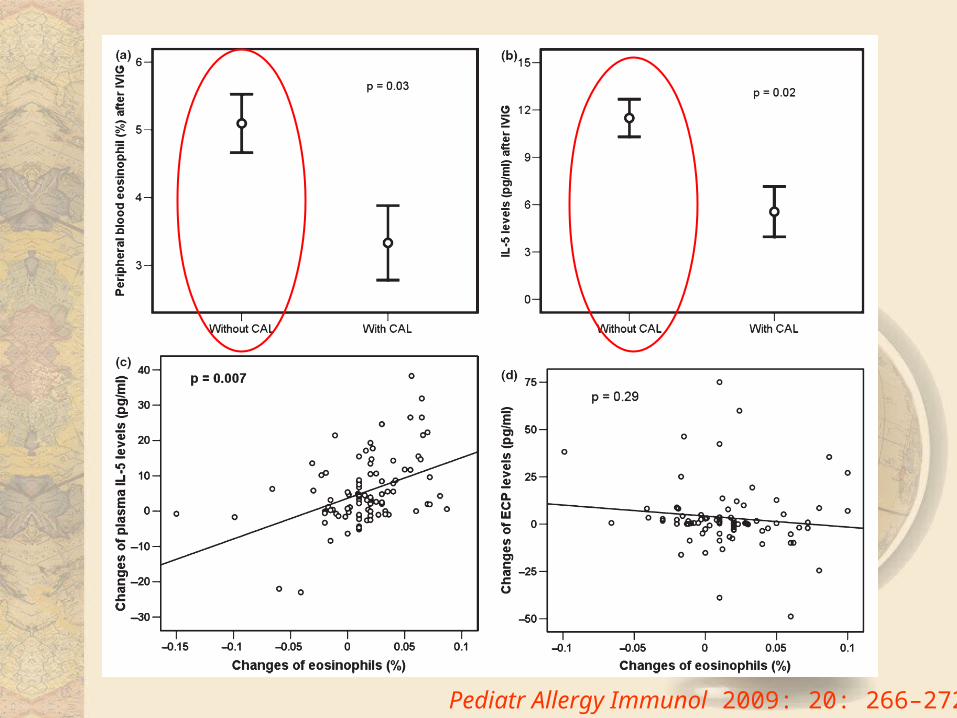
Pediatr Allergy Immunol 2009: 20: 266–272.
Pediatr Allergy Immunol 2009: 20: 266–272.
Pediatr Allergy Immunol 2009: 20: 266–272.
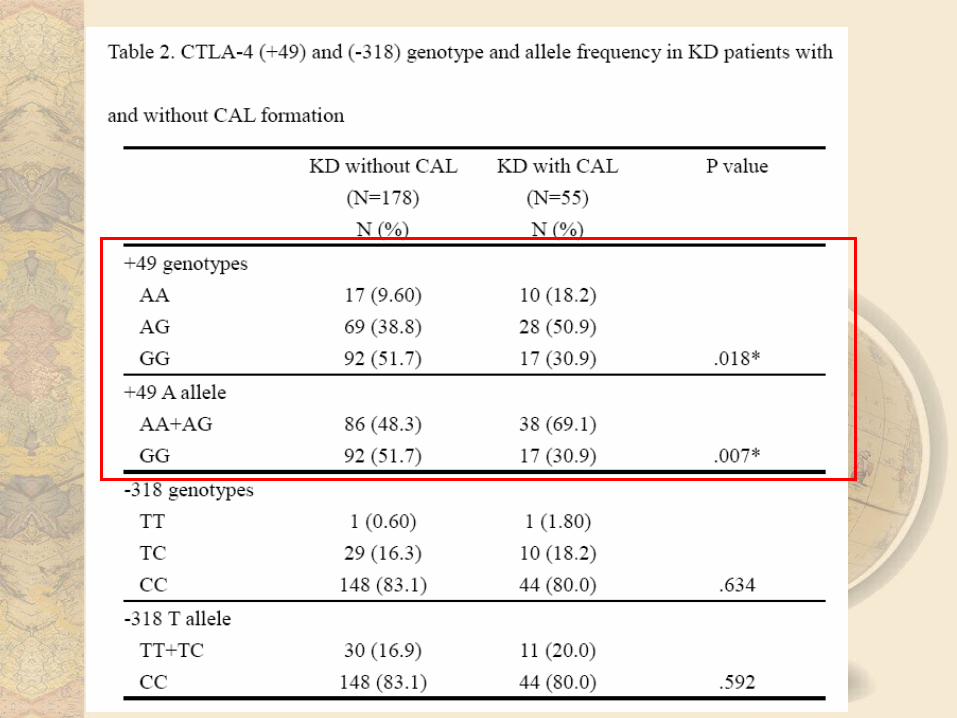
Genetic study in CAL formation of KD
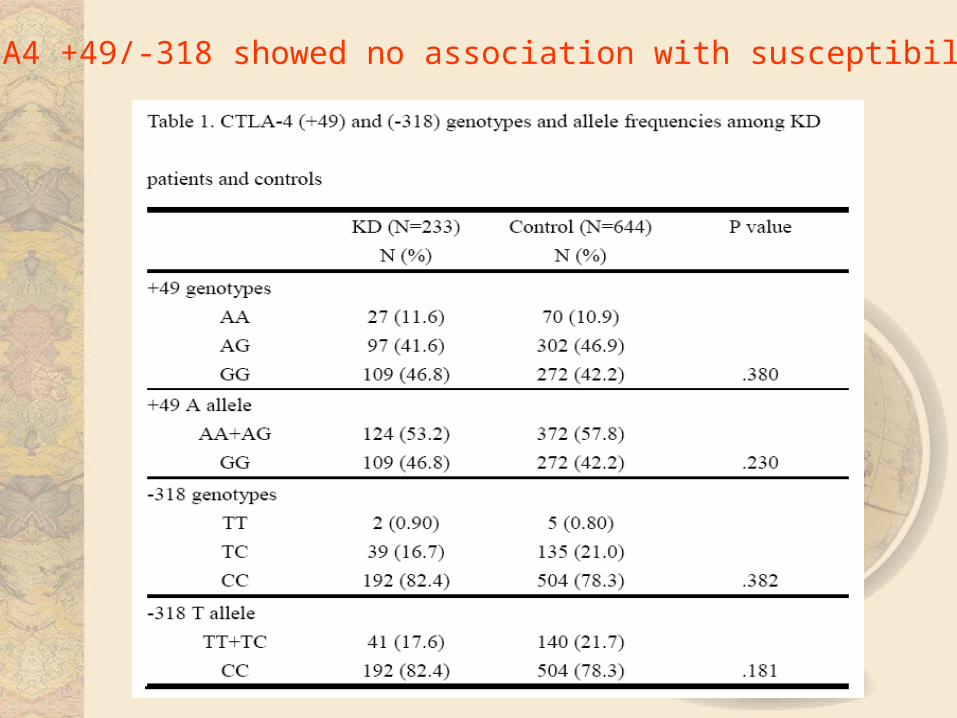
CTLA4 +49/-318 showed no association with susceptibility

Materials and methods
• A total of 801 case were enrolled– 226 KD – 575 control (without history of KD)– IIIumina array chip (customized 384 SNPs)
• Genetic association was initially assessed by univariate (UVA) and multivariate (MVA) analysis
• Multifactor dimensionality reduction (MDR)– identify gene-gene interaction
• Immune related cytokine levels in plasma:– Th1: IFNγ, IL-2– Th2: IL-4, IL-5– Innate: IL-6, IL-10 (Luminex100)– Treg: TGFβ (ELISA)
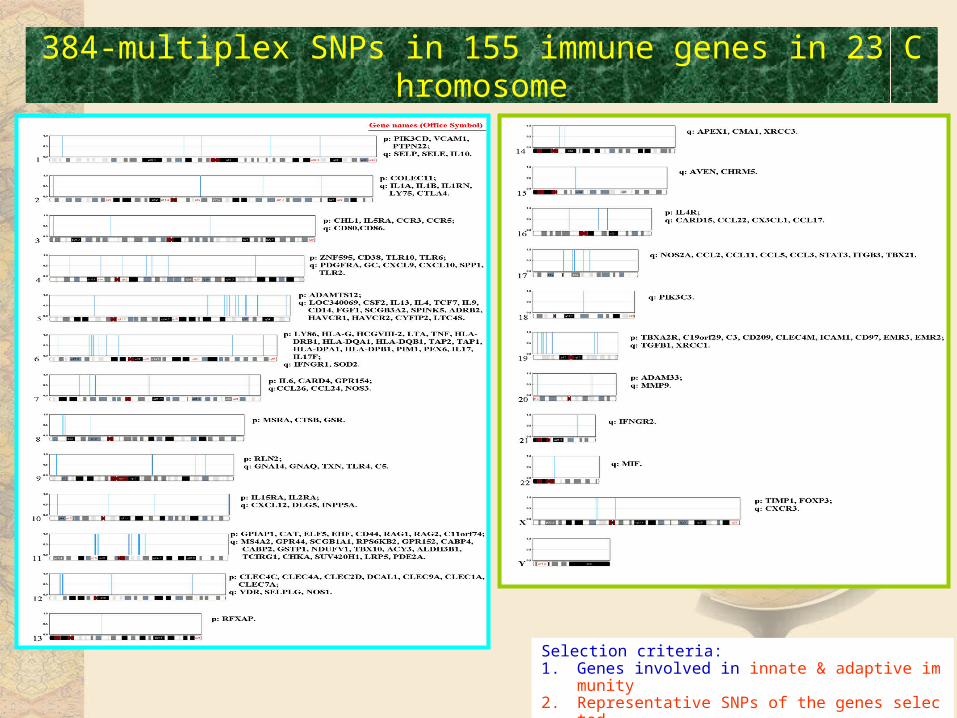
384-multiplex SNPs in 155 immune genes in 23 Chromosome
Selection criteria: 1. Genes involved in innate & adaptive immunity2. Representative SNPs of the genes selected3. Allele frequency >3% based on power calculation
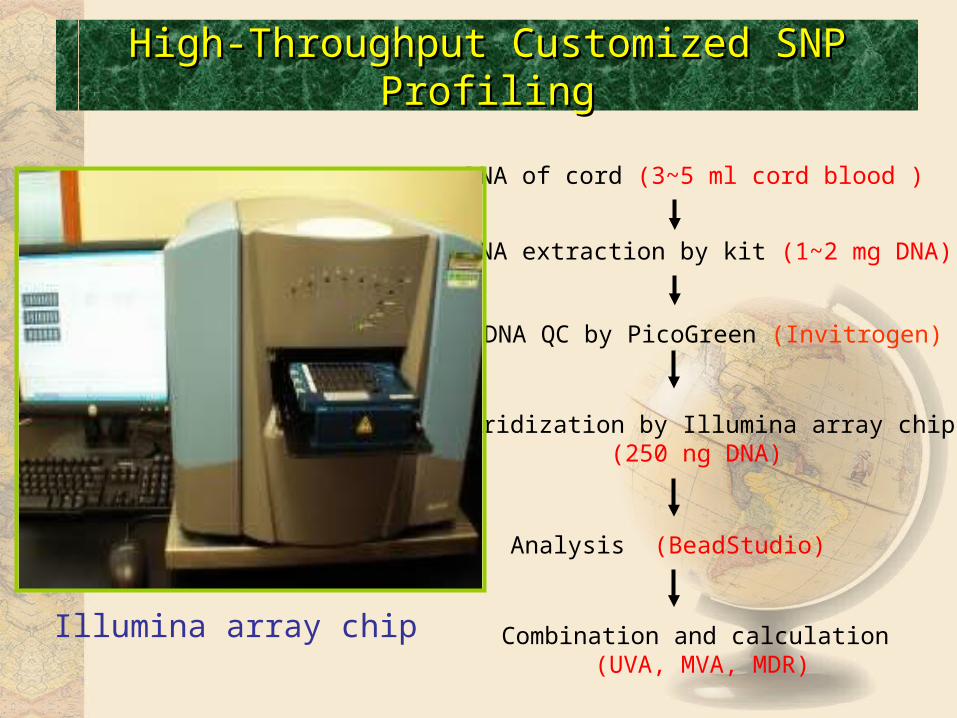
High-Throughput Customized SNP ProfilingHigh-Throughput Customized SNP Profiling
DNA extraction by kit (1~2 mg DNA)
DNA of cord (3~5 ml cord blood )
Hybridization by Illumina array chip(250 ng DNA)
DNA QC by PicoGreen (Invitrogen)
Analysis (BeadStudio)
Combination and calculation (UVA, MVA, MDR)
Illumina array chip
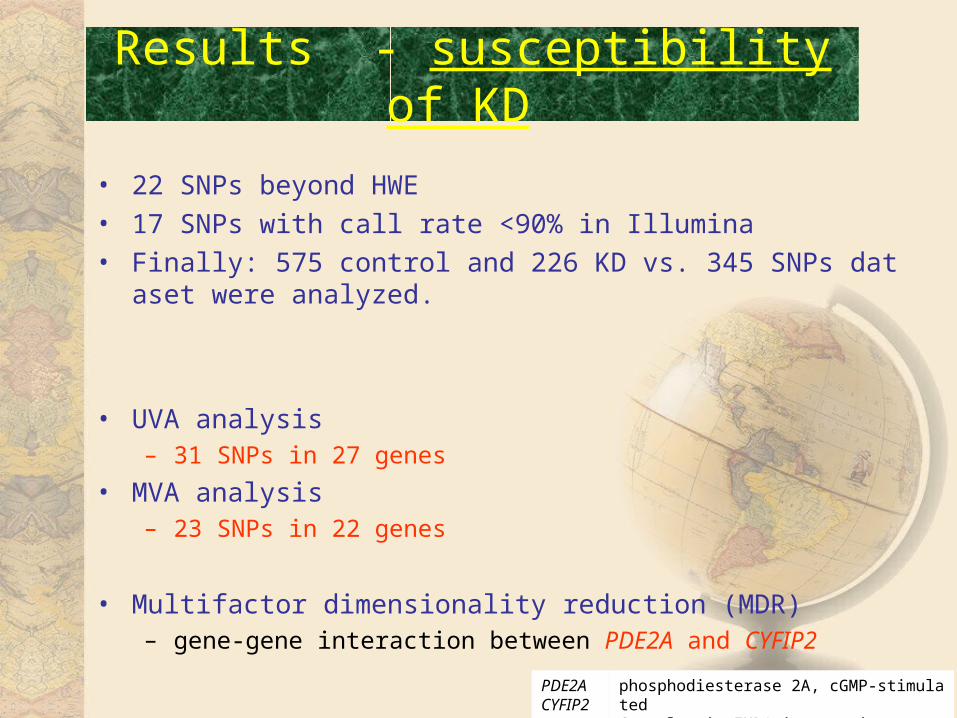
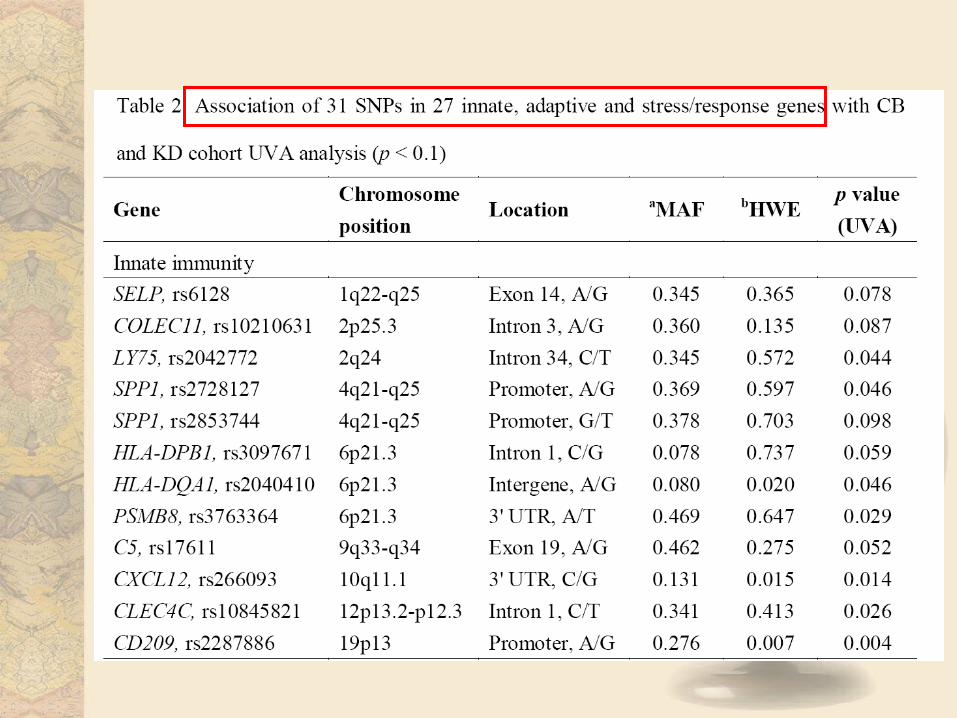
Results - susceptibility of KD
• 22 SNPs beyond HWE• 17 SNPs with call rate <90% in Illumina• Finally: 575 control and 226 KD vs. 345 SNPs dataset were analy
zed.
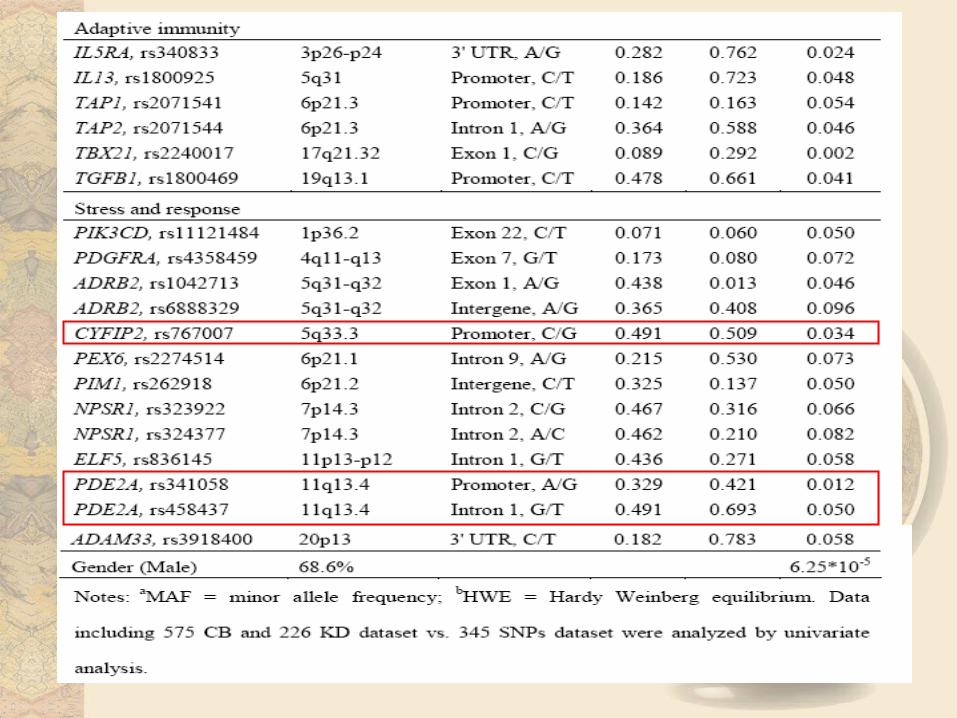
• UVA analysis– 31 SNPs in 27 genes
• MVA analysis– 23 SNPs in 22 genes
• Multifactor dimensionality reduction (MDR) – gene-gene interaction between PDE2A and CYFIP2
PDE2A CYFIP2
phosphodiesterase 2A, cGMP-stimulated Cytoplasmic FMR1-interacting protein 2
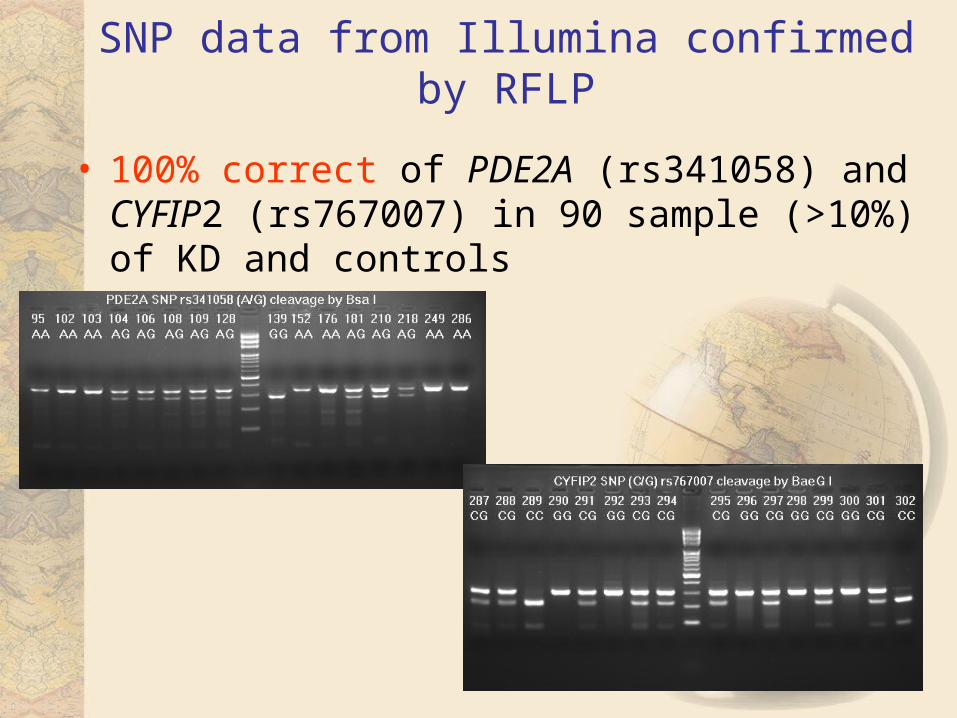
SNP data from Illumina confirmed by RFLP
• 100% correct of PDE2A (rs341058) and CYFIP2 (rs767007) in 90 sample (>10%) of KD and controls
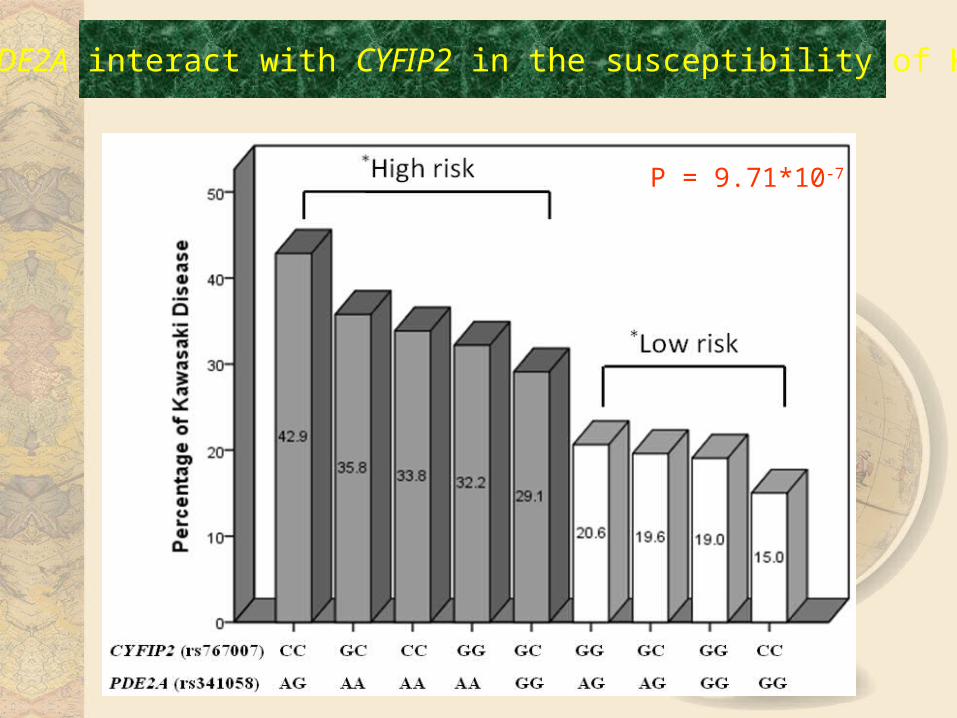
P = 9.71*10-7
PDE2A interact with CYFIP2 in the susceptibility of KD
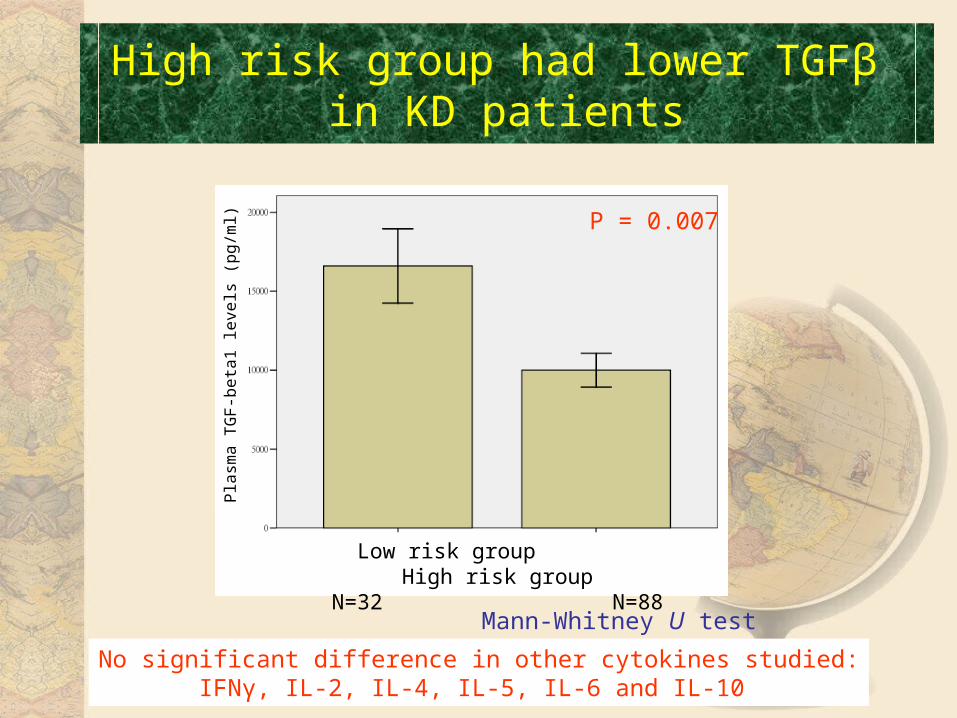
High risk group had lower TGFβ in KD patients
P = 0.007
No significant difference in other cytokines studied:IFNγ, IL-2, IL-4, IL-5, IL-6 and IL-10
Pla
sma
TG
F-b
eta
1 le
vels
(p
g/m
l)
Low risk group High risk groupN=32 N=88
Mann-Whitney U test
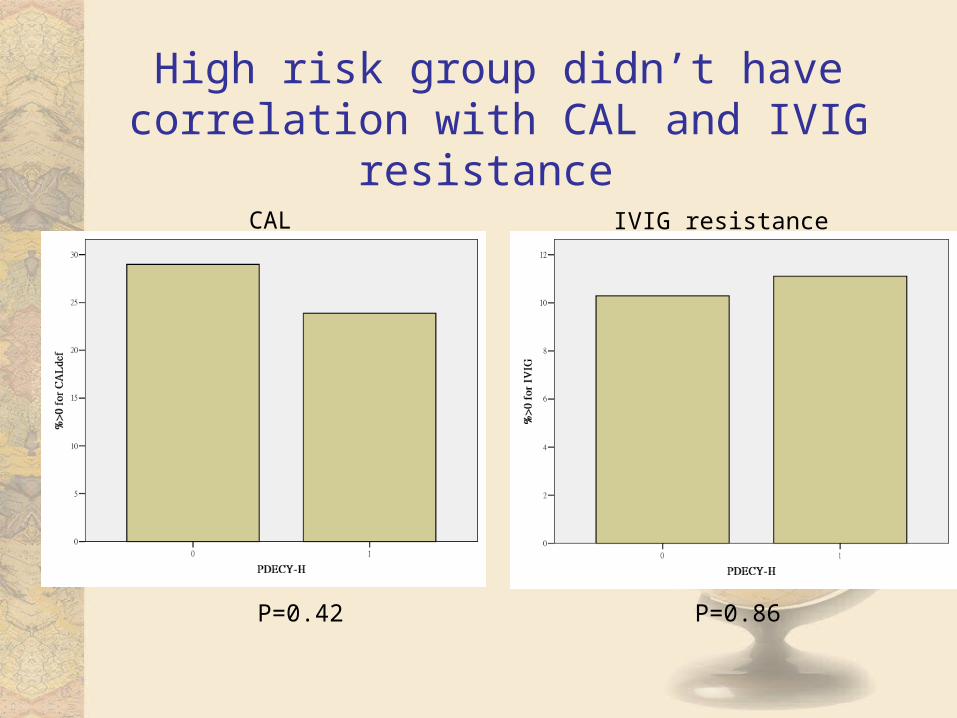
High risk group didn’t have correlation with CAL and IVIG resistance
P=0.42 P=0.86
CAL IVIG resistance
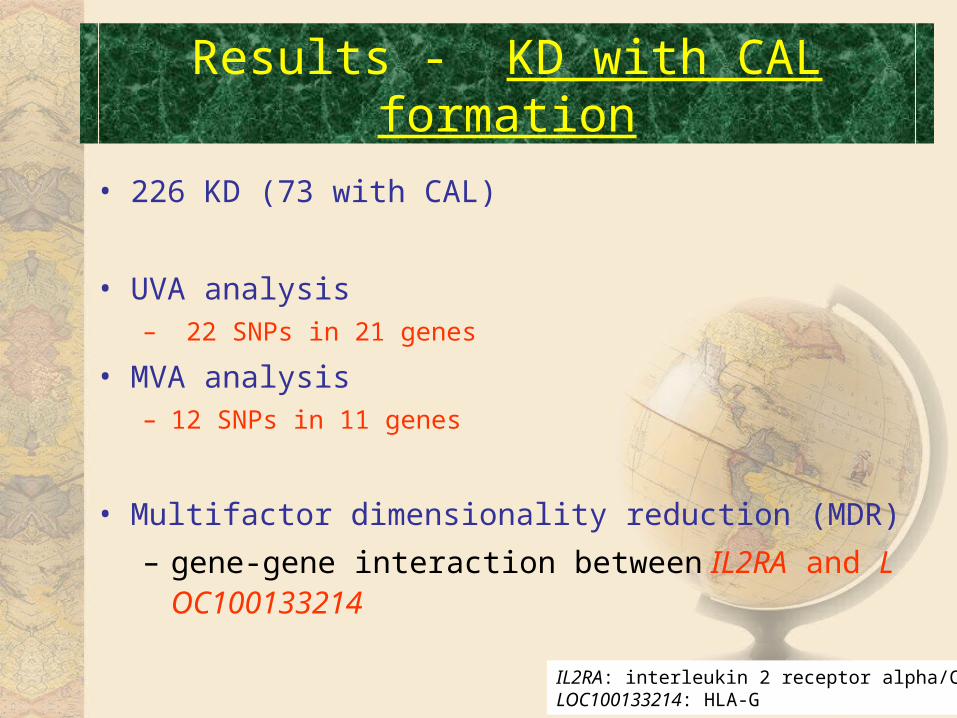
Results - KD with CAL formation
• 226 KD (73 with CAL)
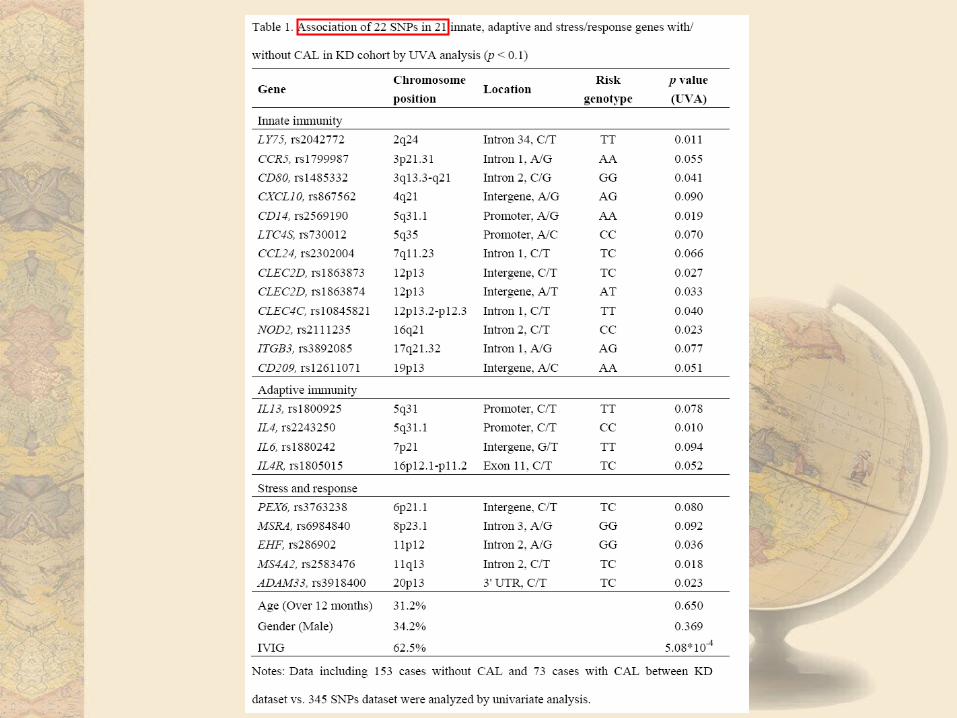
• UVA analysis– 22 SNPs in 21 genes
• MVA analysis– 12 SNPs in 11 genes
• Multifactor dimensionality reduction (MDR)
– gene-gene interaction between IL2RA and LOC100133214
IL2RA: interleukin 2 receptor alpha/CD25LOC100133214: HLA-G
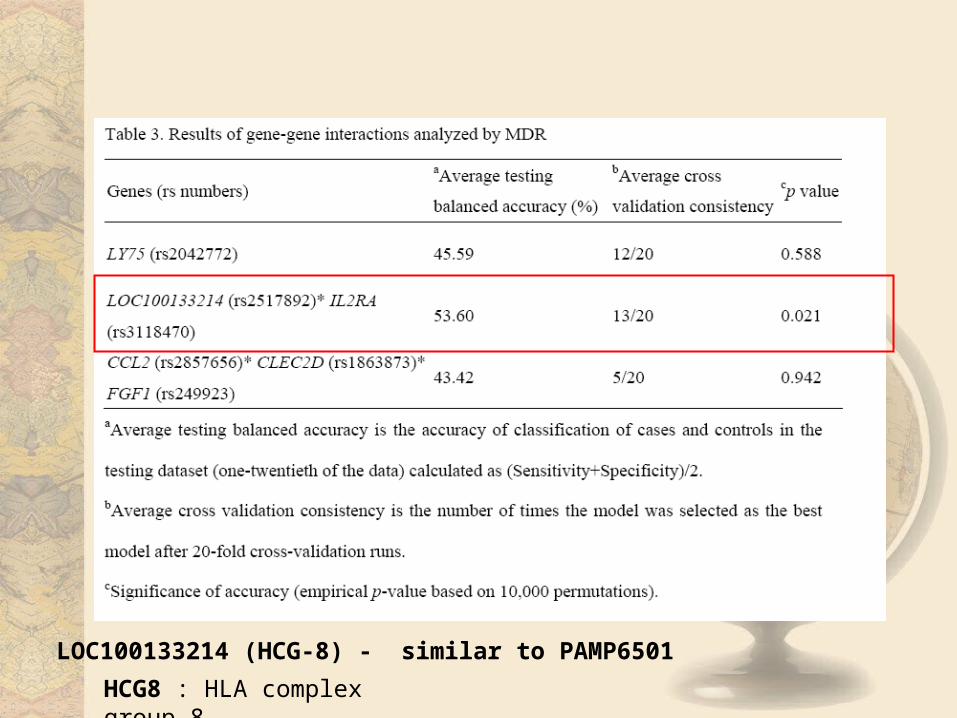
LOC100133214 (HCG-8) - similar to PAMP6501
HCG8 : HLA complex group 8
• 100% correct of IL2RA (rs3118470) and LOC (rs2517892) in 90 sample (>10%) of KD and controls
• Pyrosequencing assay: Without restriction enzyme (mini-sequencing)
SNP data from Illumina confirmed by RFLP and Pyrosequencing Assay
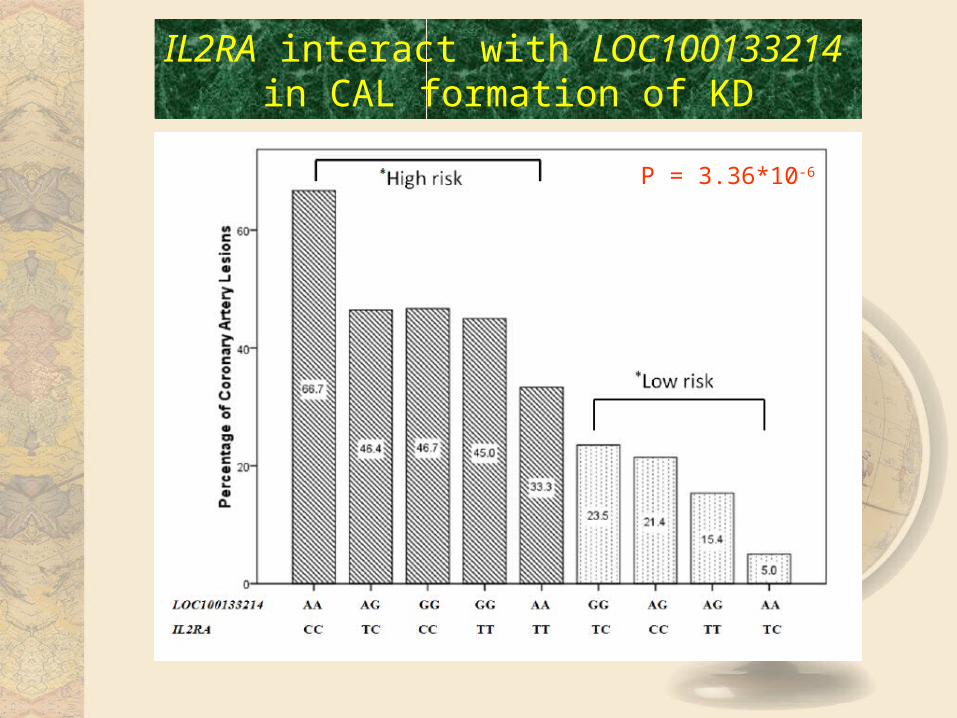
P = 3.36*10-6
IL2RA interact with LOC100133214 in CAL formation of KD
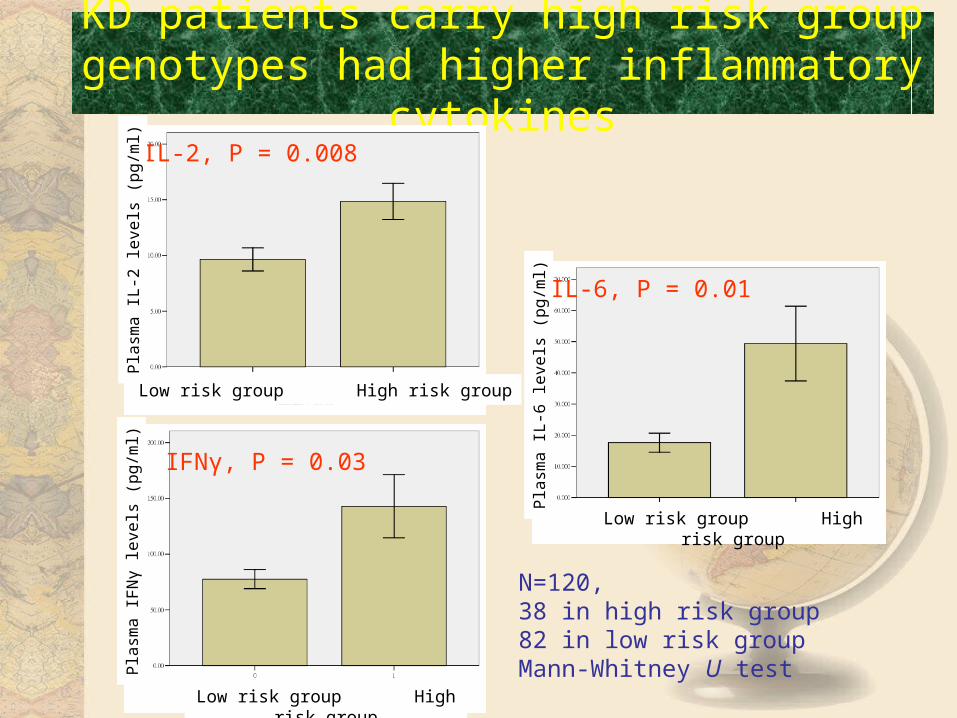
KD patients carry high risk group genotypes had higher inflammatory cytokines
IL-2, P = 0.008
IFNγ, P = 0.03
IL-6, P = 0.01
Low risk group High risk group
Low risk group High risk group
Low risk group High risk group
Pla
sma
IL
-2 le
vels
(p
g/m
l)P
lasm
a I
FN
γ le
vels
(p
g/m
l)
Pla
sma
IL
-6 le
vels
(p
g/m
l)
N=120, 38 in high risk group82 in low risk groupMann-Whitney U test
Conclusions
• Total 226 KD and 575 controls with 345 SNPs were analyzed
• Susceptibility of KD– UVA: 31 SNPs in 27 genes
– MVA: 23 SNPs in 22 genes
– MDR analyses:• Gene-gene interaction between PDE2A and CYFIP2
– Patients carry high risk group genotypes had lower TGFβ levels
• High risk group of susceptibility didn’t associated with CAL formation (p=0.42) or IVIG resistance
Conclusions • Genetic association in KD patients with CAL formation
– 226 KD (73 with CAL)
– UVA: 22 SNPs in 21 genes
– MVA: 12 SNPs in 11 genes
– MDR: • Gene-gene interaction between IL2RA and LOC100133214
– Patients carry high risk group genotypes had higher inflammatory cytokines
• IL-2, IFNγ and IL-6
• susceptibility and CAL formation may associated with different genes or gene-gene interaction
• Gene-gene interaction had role on the susceptibility and CAL formation of KD
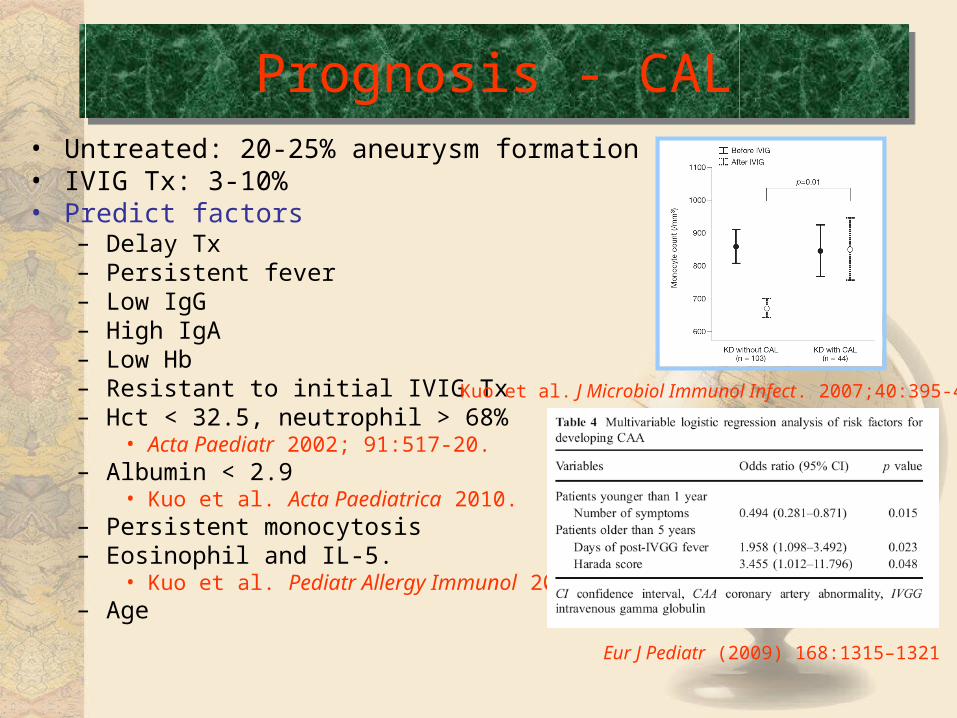
• Untreated: 20-25% aneurysm formation• IVIG Tx: 3-10% • Predict factors
– Delay Tx– Persistent fever – Low IgG– High IgA– Low Hb– Resistant to initial IVIG Tx– Hct < 32.5, neutrophil > 68%
• Acta Paediatr 2002; 91:517-20.– Albumin < 2.9
• Kuo et al. Acta Paediatrica 2010.– Persistent monocytosis – Eosinophil and IL-5.
• Kuo et al. Pediatr Allergy Immunol 2008.– Age
Prognosis - CALPrognosis - CAL
Kuo et al. J Microbiol Immunol Infect. 2007;40:395-400
Eur J Pediatr (2009) 168:1315–1321
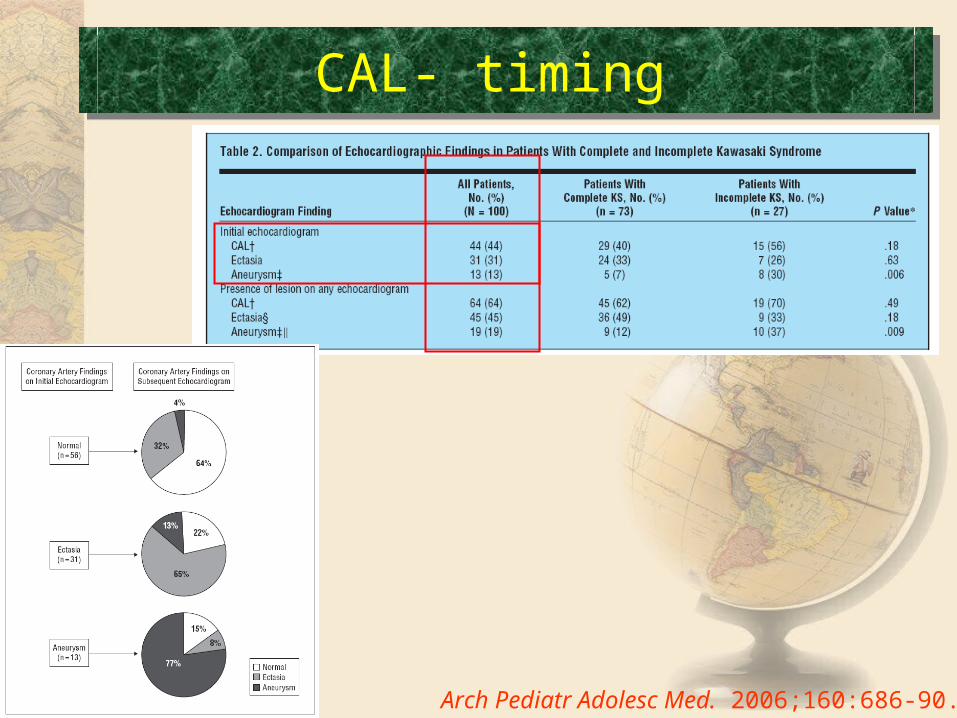
CAL- timing CAL- timing
Arch Pediatr Adolesc Med. 2006;160:686-90.
How to follow up after KD
• diagnosis and then 1 to 2 weeks and 4 to 6 weeks
• Children with persistent fever or coronary aneurysms may have additional testing.
• All children who have had KD should adopt a heart-healthy lifestyle (that is, no smoking, regular exercise, heart-healthy diet)
Circulation 2008;118;e110-e112
問題• 郭醫師您好:這幾天在網路上拼命蒐集有關川崎氏症的資料,偶爾看到您
的部落格很高興,想請教您一些問題。
• 我的女兒因為川崎氏症目前還在台南的新樓醫院住院當中,• 在上週二確診為此症時已經在上週二晚間六點多開始打免疫球蛋白連續十二小時共 4瓶﹝各 50 c.c﹞,
• 第二天身上的紅疹已經退去百分之八九十左右了,• 週三晚間再打一次同前一天的劑量跟時間• 週四中午過後已經看不到身上的疹子。• 但是,一直到現在還是有發燒的情形。• 一天大概二 ~三次,每次都燒到 39度左右開始給塞劑才能退燒。• 這其中,有抽血的報告是發炎指數上升,但剛開始來時的肝指數過高的情形有下降。
• 也因為有發炎所以有加入抗生素的療程進天是第三天,• 另外也有驗大便驗 血都排除腺病毒、 EB病毒 ...的感染。• 阿斯匹靈從昨天中午開始加到兩顆的劑量。• 今天從凌晨開始到晚上為止還是發燒了三次,目前用了兩次塞劑,第三次就是 現在還在躺冰枕觀察。
• 請問您,我們該怎麼辦呢 ?
我們在川崎症的研究報告
感恩所有同仁的幫忙 !
希望我們我們可以給川崎症病童更好的照護!
Thanks a lot!
雅典學院 :Academy, 8000pc puzzle
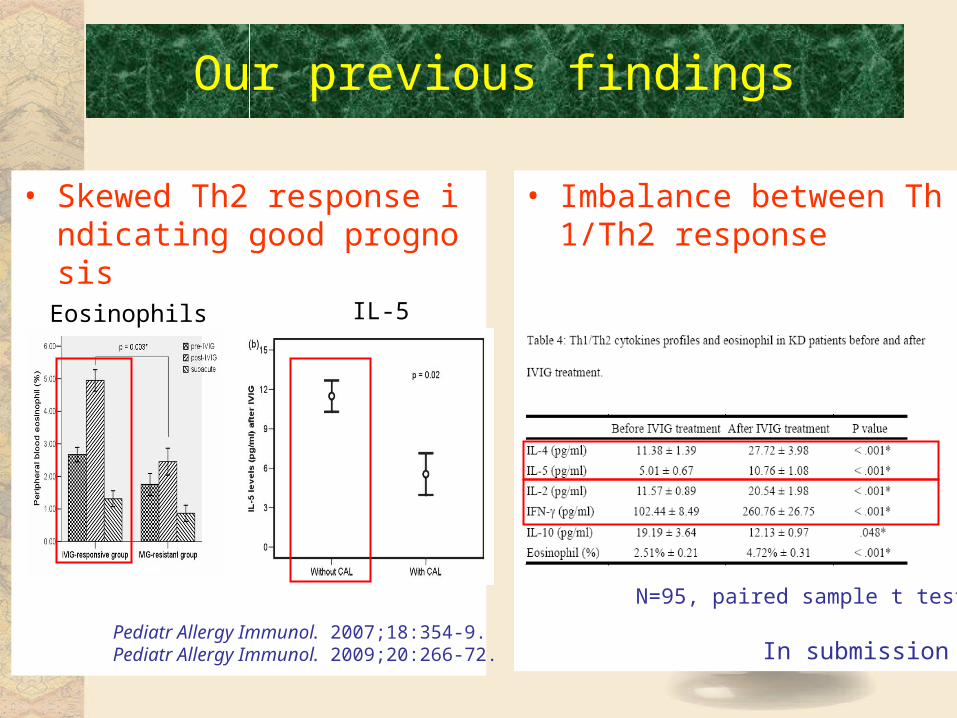
Our previous findings
• Skewed Th2 response indicating good prognosis
• Imbalance between Th1/Th2 response
Pediatr Allergy Immunol. 2007;18:354-9.Pediatr Allergy Immunol. 2009;20:266-72.
IL-5Eosinophils
N=95, paired sample t test
In submission