Embed Size (px)
Citation preview
Carcinoma de Próstata
Nuevas Alternativas de Tratamiento Medico
Dr. Luis Miguel Zetina ToacheCancer Consultants GT
JMR. TX .CABAZITAXEL. JUN. 2011
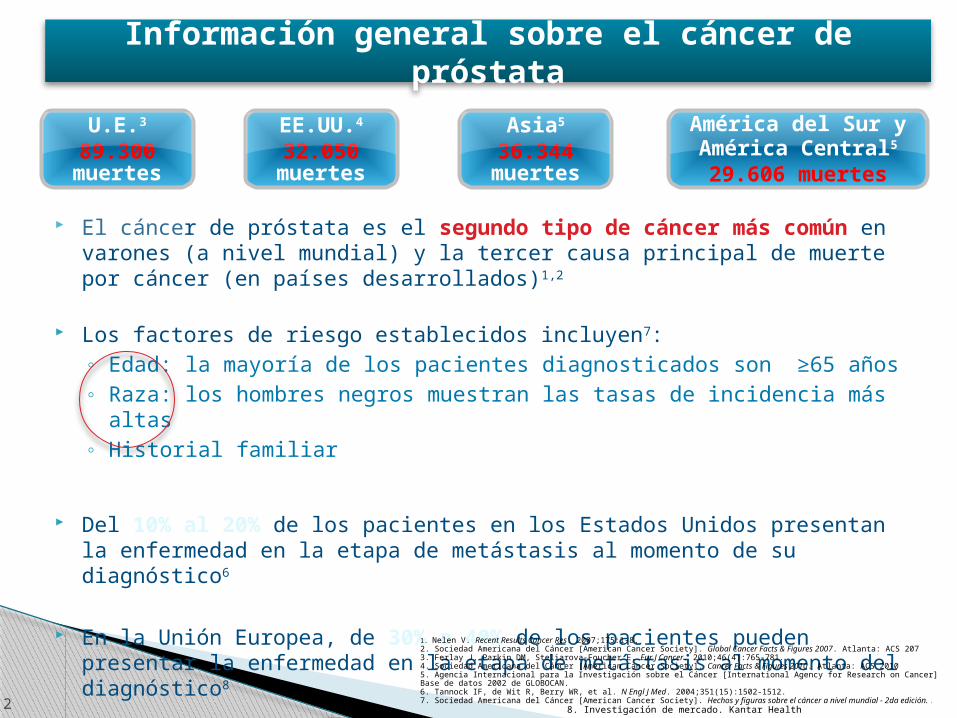
Información general sobre el cáncer de próstata
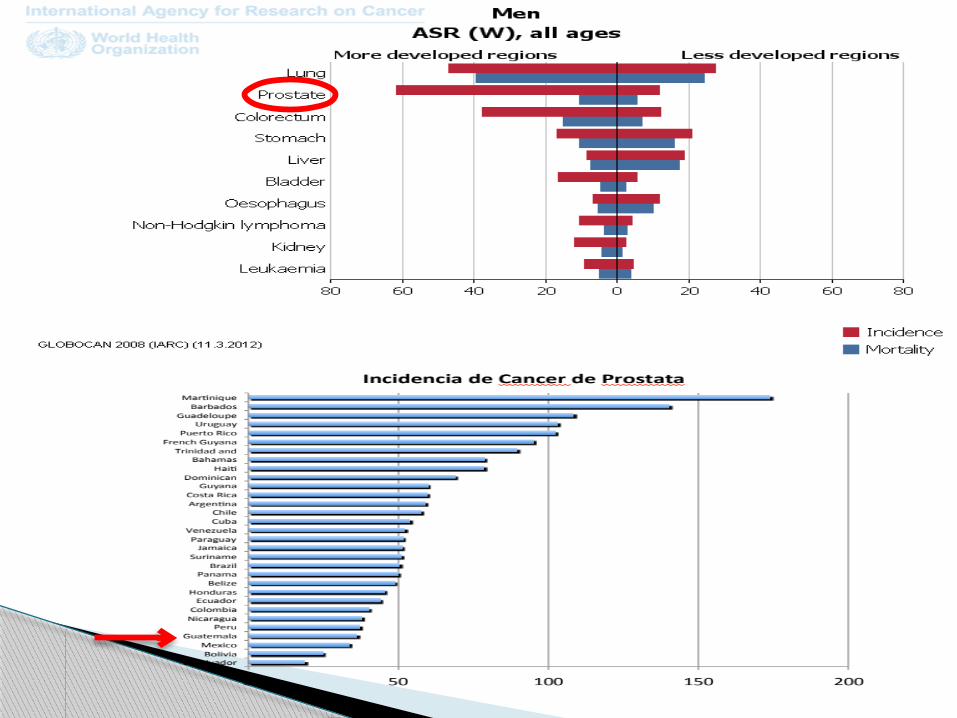
El cáncer de próstata es el segundo tipo de cáncer más común en varones (a nivel mundial) y la tercer causa principal de muerte por cáncer (en países desarrollados)1,2
Los factores de riesgo establecidos incluyen7:◦ Edad: la mayoría de los pacientes diagnosticados son ≥65 años ◦ Raza: los hombres negros muestran las tasas de incidencia más altas◦ Historial familiar
Del 10% al 20% de los pacientes en los Estados Unidos presentan la enfermedad en la etapa de metástasis al momento de su diagnóstico6
En la Unión Europea, de 30% a 40% de los pacientes pueden presentar la enfermedad en la etapa de metástasis al momento del diagnóstico8
2
EE.UU.4
32.050 muertes
U.E.3
89.300 muertes
Asia5
36.344 muertes
América del Sur y América Central5
29.606 muertes
1. Nelen V. Recent Results Cancer Res. 2007;175:1-8.2. Sociedad Americana del Cáncer [American Cancer Society]. Global Cancer Facts & Figures 2007. Atlanta: ACS 2073. Ferlay J, Parkin DM, Steliarova-Foucher E. Eur J Cancer. 2010;46(4):765-781.4. Sociedad Americana del Cáncer [American Cancer Society]. Cancer Facts & Figures 2010. Atlanta: ACS 20105. Agencia Internacional para la Investigación sobre el Cáncer [International Agency for Research on Cancer] Base de datos 2002 de GLOBOCAN. 6. Tannock IF, de Wit R, Berry WR, et al. N Engl J Med. 2004;351(15):1502-1512.7. Sociedad Americana del Cáncer [American Cancer Society]. Hechos y figuras sobre el cáncer a nivel mundial - 2da edición. . 8. Investigación de mercado. Kantar Health

La Cargade Metástasis óseas
DOLOR
CompresiónMedularAnemia
Hipercalcemia
Fracturas
Discapacidad

optimismo
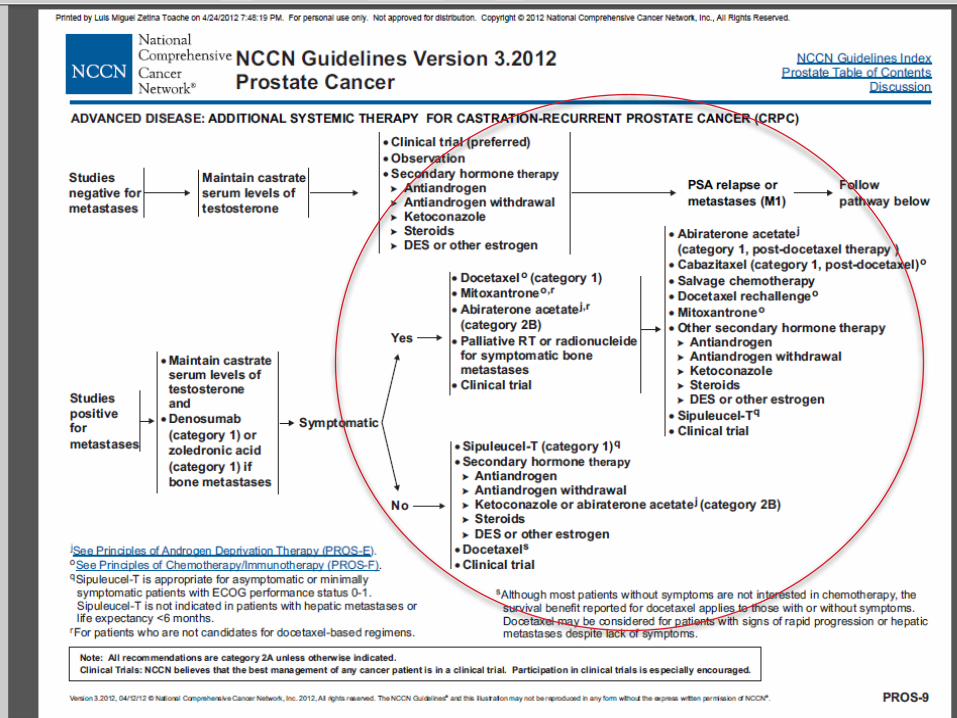
Carcinoma Prostata HR
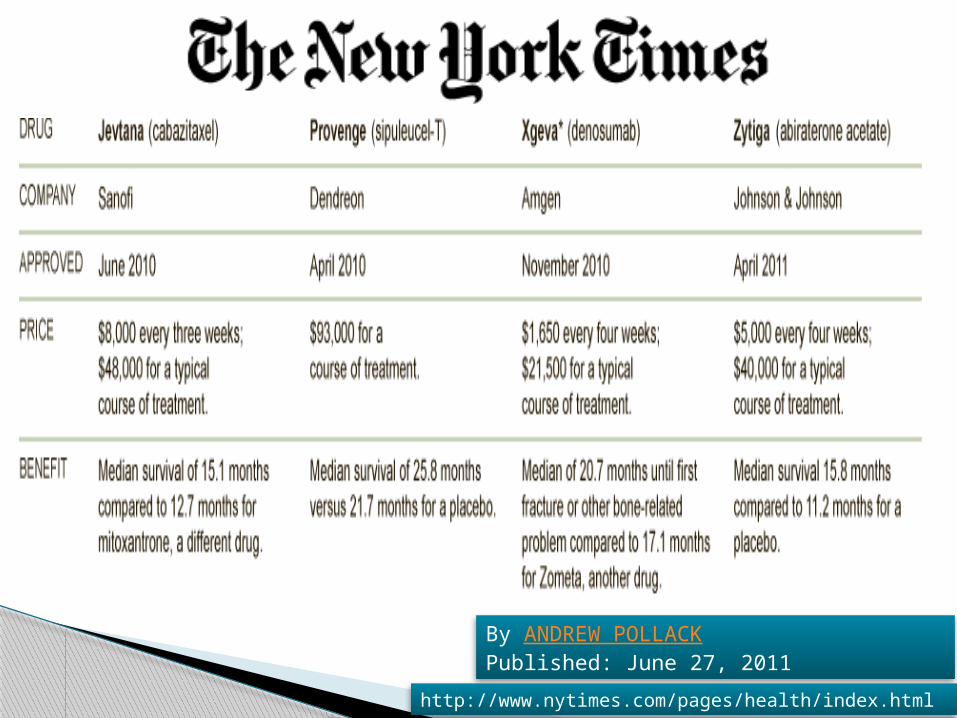
By ANDREW POLLACKPublished: June 27, 2011
http://www.nytimes.com/pages/health/index.html
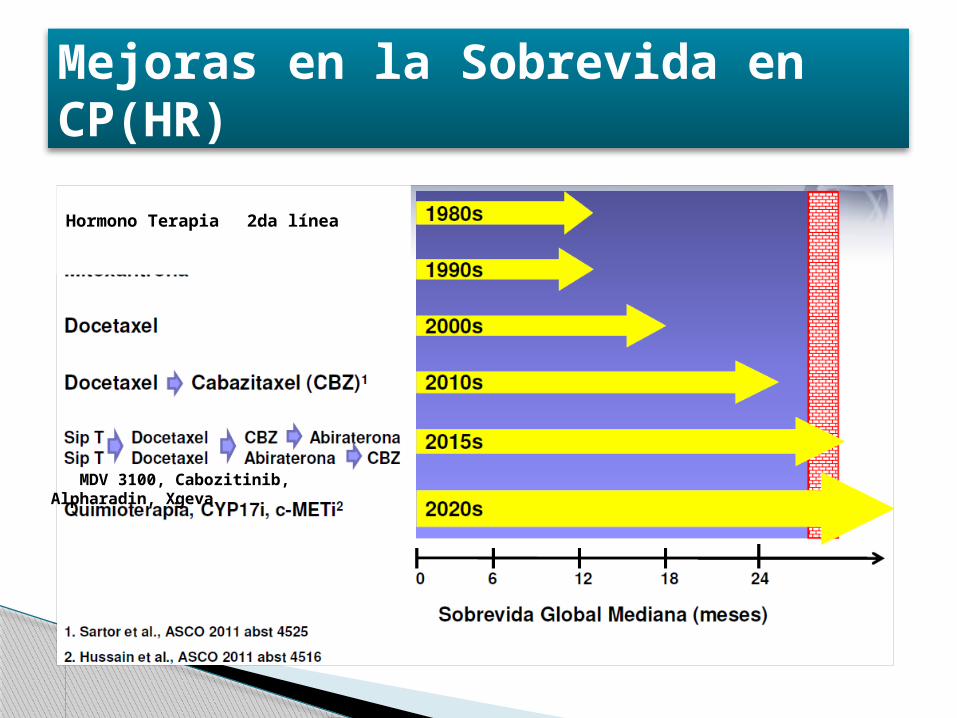
Mejoras en la Sobrevida en CP(HR)
Hormono Terapia 2da línea
MDV 3100, Cabozitinib, Alpharadin, Xgeva
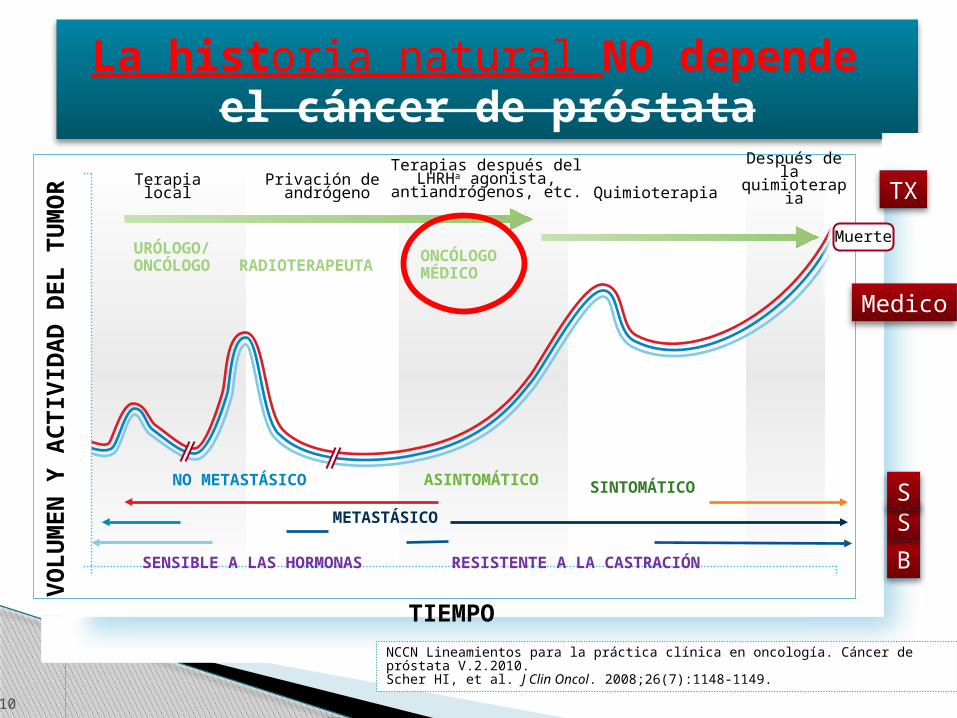
La historia natural NO depende el cáncer de próstata
10
medoi
TIEMPOVO
LU
MEN
Y A
CTIV
IDA
D D
EL T
UM
OR
Privación de andrógeno Quimioterapia Después de la
quimioterapiaTerapia
local
Terapias después delLHRHa agonista,
antiandrógenos, etc.
ASINTOMÁTICO SINTOMÁTICONO METASTÁSICO
METASTÁSICO
SENSIBLE A LAS HORMONAS RESISTENTE A LA CASTRACIÓN
Muerte
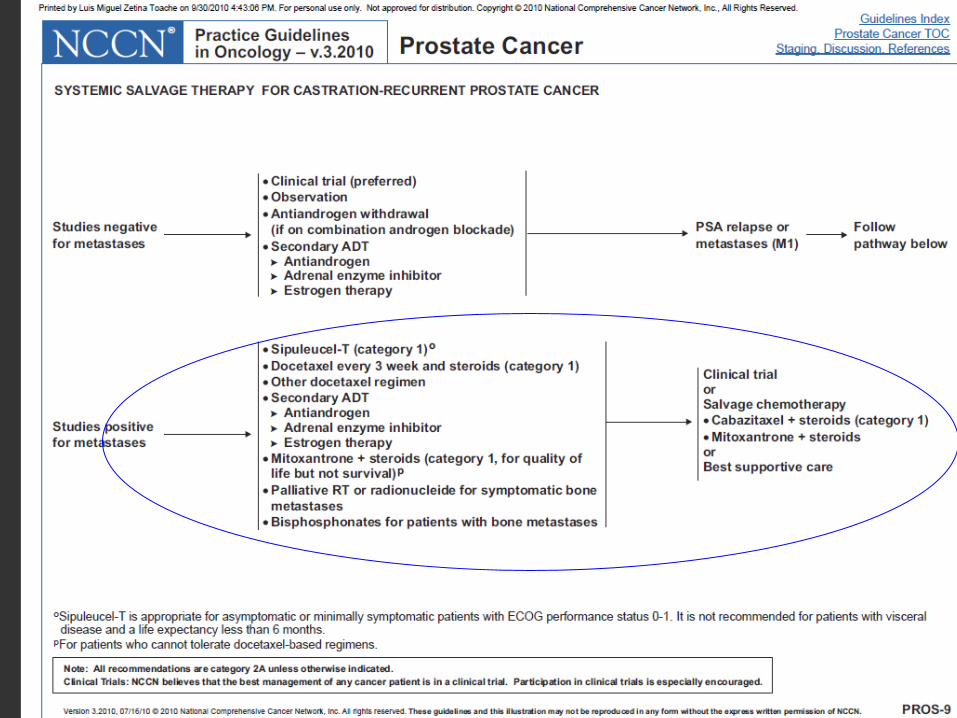
NCCN Lineamientos para la práctica clínica en oncología. Cáncer de próstata V.2.2010.Scher HI, et al. J Clin Oncol. 2008;26(7):1148-1149.
URÓLOGO/ONCÓLOGO RADIOTERAPEUTA
ONCÓLOGOMÉDICO
B
S
TX
S
Medico
GLB.CAB.11.08.09 9/11
Los beneficios de un enfoque multidisciplinario en el tratamiento del mHRPC
•El enfoque multidisciplinario puede servir al cuidado del paciente– Identificación de oportunidades para una terapia apropiada en los primeros estadios de
la enfermedad metástasica.– Asegurar la derivación oportuna y exitosa– Alineación de expectativas mutuas y objetivos de tratamiento
11
En pacientes con un alto riesgo de progreso de la enfermedada
“El comienzo temprano de un tratamiento de quimioterapia [de primera línea] en pacientes [con mHRPC] resulta en una mejora significativa de la sobrevida a diferencia de aquellos pacientes en los que se retrasa el inicio del tratamiento sistémico citotóxico”.
- Asociación Europea de UrologíaAbril 2011
1. Sternberg CN, Krainer M, Oh WK, et al. BJU Int. 2007;99(1):22-27.2. 2. Gomella LG, Lin J, Hoffman-Censits J, et al. J Oncol Pract. 2010;6(6): e5-e10. 3. Mottet N, Bellmunt J,
Bolla M, et al. Eur Urol. 2011;59(4):572-583.
Enfermera oncológica
Urólogo
Oncólogo médico
Oncólogo Radio
Terapeuta
PACIENTE
GLB.CAB.11.08.09 9/11
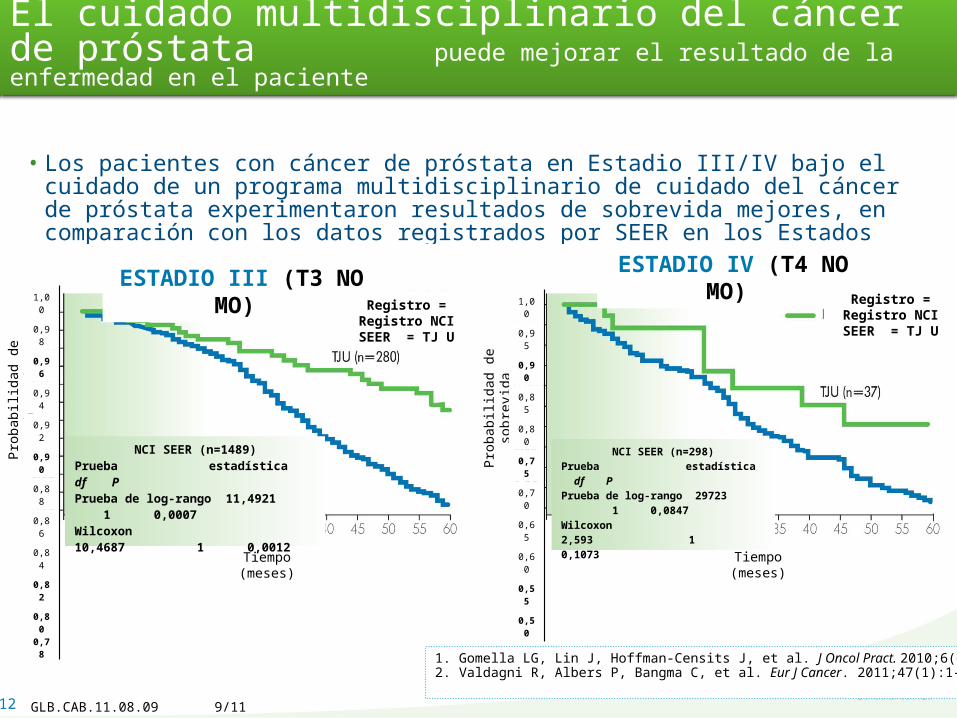
El cuidado multidisciplinario del cáncer de próstata puede mejorar el resultado de la enfermedad en el paciente
• Los pacientes con cáncer de próstata en Estadio III/IV bajo el cuidado de un programa multidisciplinario de cuidado del cáncer de próstata experimentaron resultados de sobrevida mejores, en comparación con los datos registrados por SEER en los Estados Unidos.
12
1. Gomella LG, Lin J, Hoffman-Censits J, et al. J Oncol Pract. 2010;6(6): e5-e10.2. Valdagni R, Albers P, Bangma C, et al. Eur J Cancer. 2011;47(1):1-7.
Tiempo (meses) Tiempo (meses)
ESTADIO III (T3 NO MO) ESTADIO IV (T4 NO MO)
Registro = Registro NCI SEER = TJ U
Registro = Registro NCI SEER = TJ U
Prob
abili
dad
de
sobr
evid
a
Prob
abili
dad
de s
obre
vida
NCI SEER (n=1489)Prueba estadística df PPrueba de log-rango 11,4921 1 0,0007Wilcoxon 10,4687 1 0,0012
NCI SEER (n=298)Prueba estadística df PPrueba de log-rango 29723 1 0,0847Wilcoxon 2,593 1 0,1073
1,00
0,95
0,90
0,85
0,80
0,75
0,70
0,65
0,60
0,55
0,50
1,00
0,98
0,96
0,94
0,92
0,90
0,88
0,86
0,84
0,82
0,800,78
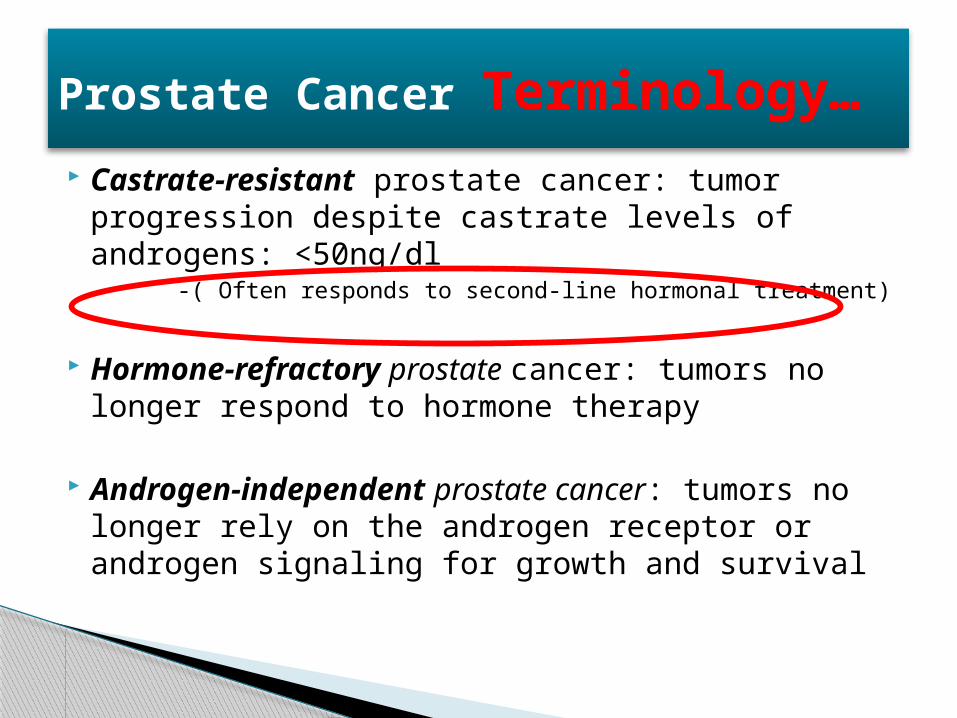
Prostate Cancer Terminology…
Castrate-resistant prostate cancer: tumor progression despite castrate levels of androgens: <50ng/dl
-( Often responds to second-line hormonal treatment)
Hormone-refractory prostate cancer: tumors no longer respond to hormone therapy
Androgen-independent prostate cancer: tumors no longer rely on the androgen receptor or androgen signaling for growth and survival
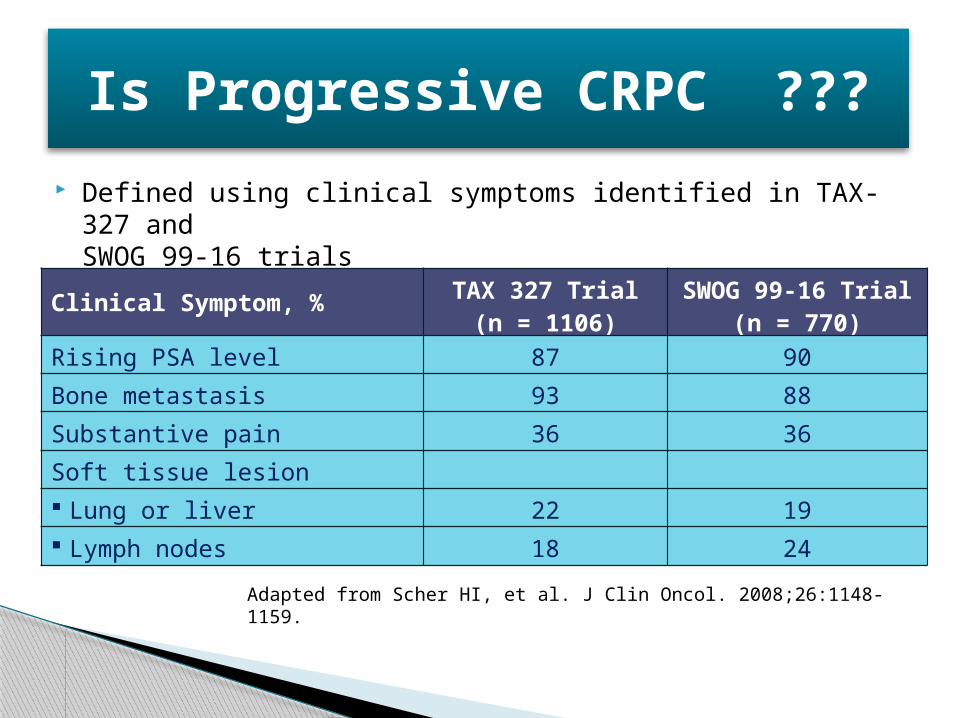
Is Progressive CRPC ???
Defined using clinical symptoms identified in TAX-327 and SWOG 99-16 trials
Adapted from Scher HI, et al. J Clin Oncol. 2008;26:1148-1159.
Clinical Symptom, % TAX 327 Trial(n = 1106)
SWOG 99-16 Trial(n = 770)
Rising PSA level 87 90
Bone metastasis 93 88
Substantive pain 36 36
Soft tissue lesion
Lung or liver 22 19
Lymph nodes 18 24
When Is Chemotherapy Appropriate in the CRPC Patient?
Yes, this patient should receive chemotherapy◦ Nodal spread with no evidence of bone or visceral
(liver, lung) disease◦ Bone disease without nodal disease or visceral spread◦ Visceral metastases with or without other metastatic sites
No, this patient should not receive chemotherapy◦ Locally progressing tumor without metastatic disease◦ Rising PSA and no detectable metastatic disease (rising
PSA-castrate)
Factors Affecting Treatment Initiating Chemotherapy: PSA Doubling Time
Patients with a slow PSA doubling time and symptomatic bone-only disease should receive secondary hormonal therapy plus palliative radiotherapy and zoledronic acid[1] ◦ Asymptomatic patients with slow PSA doubling time usually
placed on observation only
Symptomatic patients with a rapid PSA doubling time should receive docetaxel-based chemotherapy◦ Investigational strategies also appropriate for patients with rapid
PSA doubling time[2]
◦ Docetaxel appropriate for patients with symptomatic disease or visceral metastases
1. Calabro F, et al. Eur Urol. 2007;51:17-26.2. Mendiratta P, et al. Ref Urol. 2007;9(suppl 1):S9-S19.
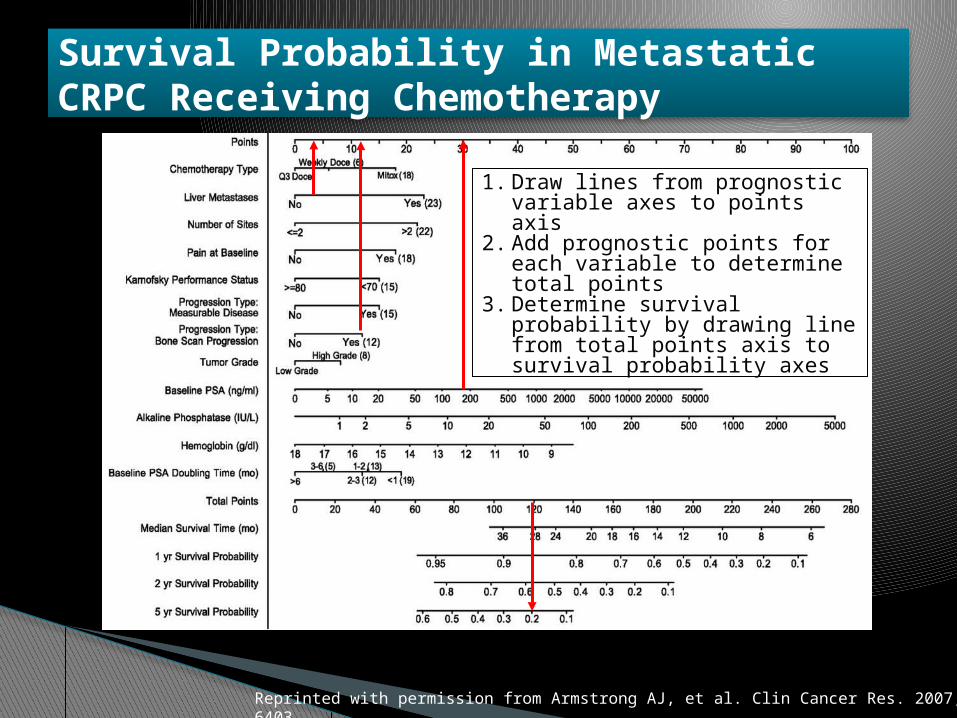
Survival Probability in Metastatic CRPC Receiving Chemotherapy
Reprinted with permission from Armstrong AJ, et al. Clin Cancer Res. 2007;13:6396-6403.
1. Draw lines from prognostic variable axes to points axis
2. Add prognostic points for each variable to determine total points
3. Determine survival probability by drawing line from total points axis to survival probability axes
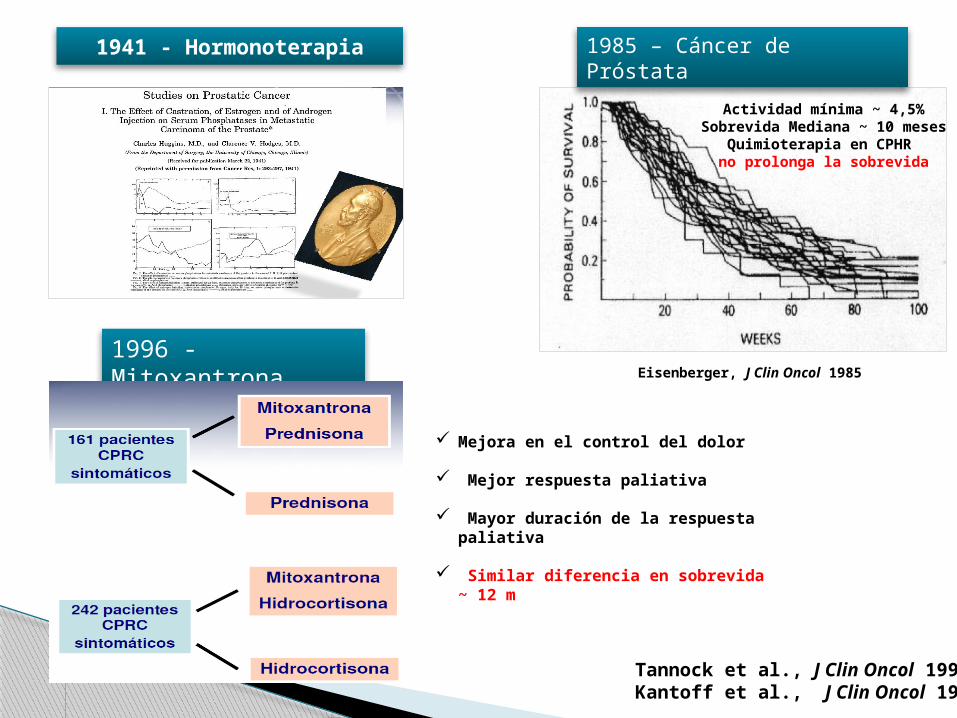
1941 - Hormonoterapia 1985 – Cáncer de Próstata
Eisenberger, J Clin Oncol 1985
Actividad mínima ~ 4,5%Sobrevida Mediana ~ 10 meses
Quimioterapia en CPHR no prolonga la sobrevida
1996 - Mitoxantrona
Mejora en el control del dolor
Mejor respuesta paliativa
Mayor duración de la respuesta paliativa
Similar diferencia en sobrevida ~ 12 m
Tannock et al., J Clin Oncol 1996 Kantoff et al., J Clin Oncol 1999
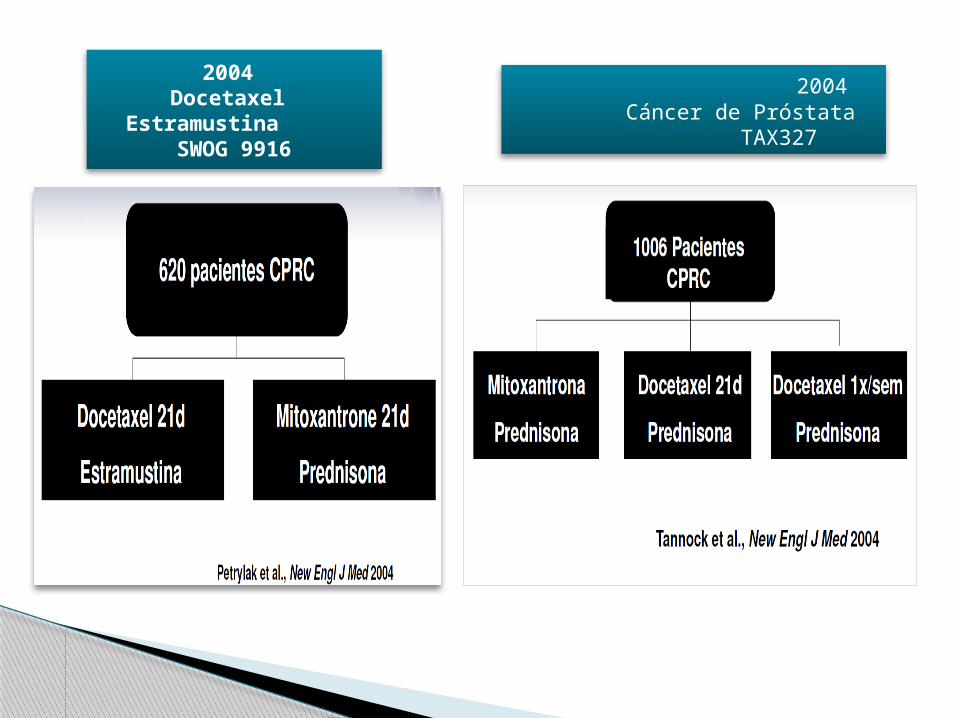
2004 Docetaxel Estramustina
SWOG 9916
2004 Cáncer de Próstata TAX327
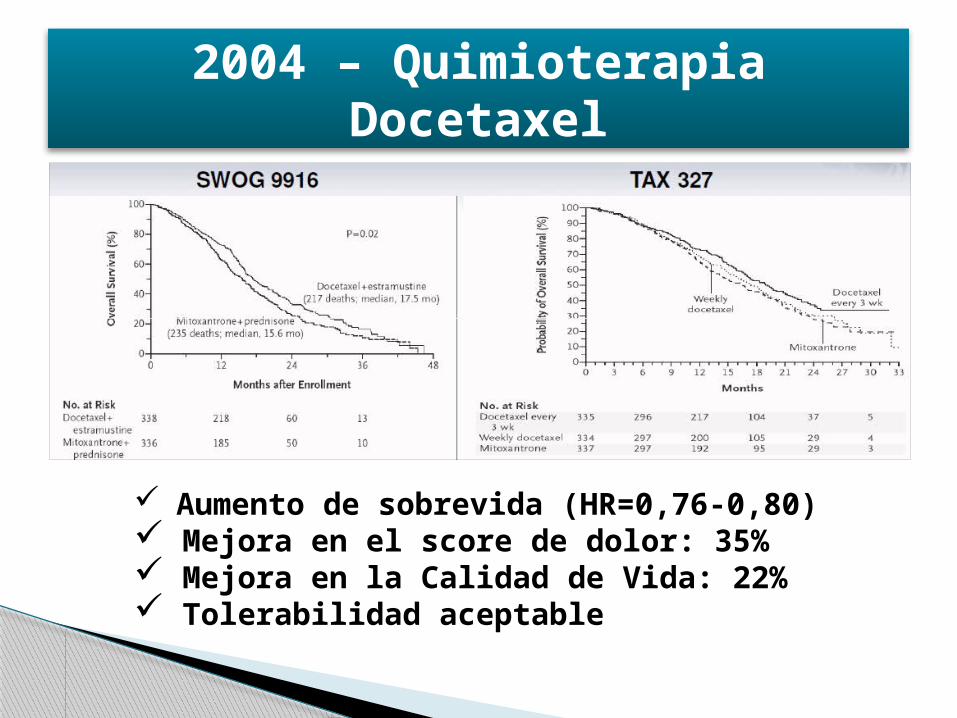
2004 – Quimioterapia Docetaxel
Aumento de sobrevida (HR=0,76-0,80) Mejora en el score de dolor: 35% Mejora en la Calidad de Vida: 22% Tolerabilidad aceptable
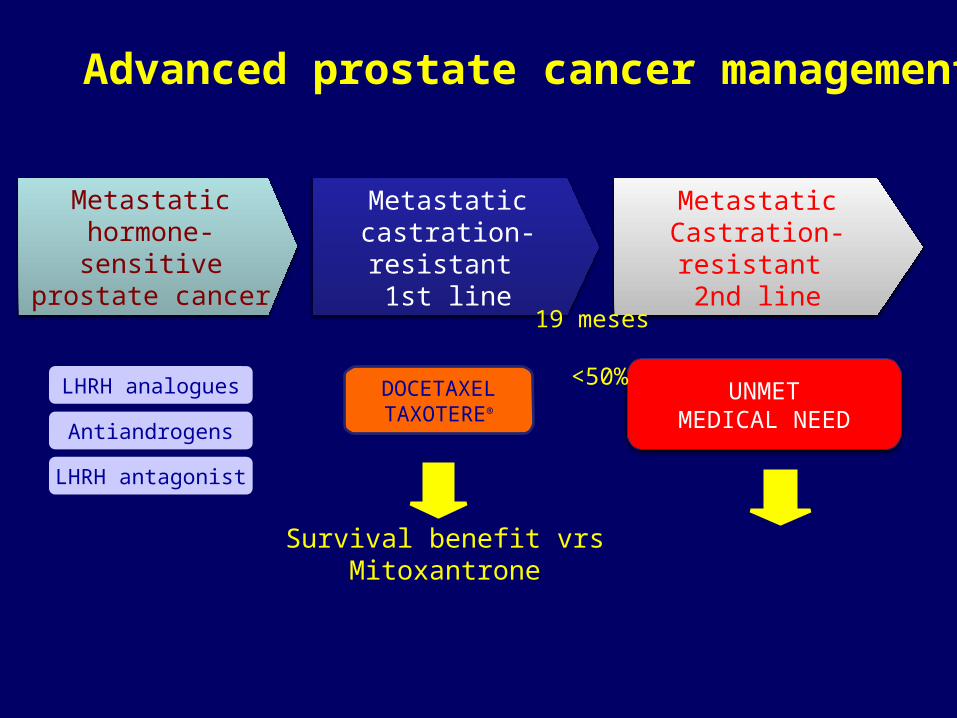
Metastatichormone-sensitive
prostate cancer
MetastaticCastration-resistant
2nd line
Metastaticcastration-resistant
1st line
Advanced prostate cancer management
DOCETAXELTAXOTERE®
Survival benefit vrs Mitoxantrone
UNMETMEDICAL NEED
LHRH analogues
Antiandrogens
LHRH antagonist
19 meses <50%
Resistencia a taxanos - Un problema recurrenteMecanismos de resistencia al taxano•No existe mecanismo único de resistencia al docetaxel identificado en pacientes1-3
•En las células no sensibles al taxano, los dos mecanismos más comúnmente asociados con la resistencia al taxano son1-3:– Sobreexpresión de los miembros de la familia del casete de transportadores ATP
(p.ej. P glicoproteína)– Alteraciones de la tubulina: el objetivo celular de los taxanos
•Otros mecanismos de resistencia pueden estar relacionados con la reglamentación disfuncional de señalamiento apoptótico, como la sobreexpresión HER24
Repercusiones clínicas•No respondedores1
•Los respondedores iniciales progresarán de modo eventual1
23
1. Fojo AT, Menefee M. Semin Oncol. 2005;32(6 supl. 7):S3-S8. 2. McGrogan BT, et al. Biochim Biophys Acta. 2008;1785(2):96-132.3. Jordan MA, Wilson L. Nat Rev Cancer 2004, 4:253-265.4. Modi S, et al. Cancer Invest 2005;23:483−487.
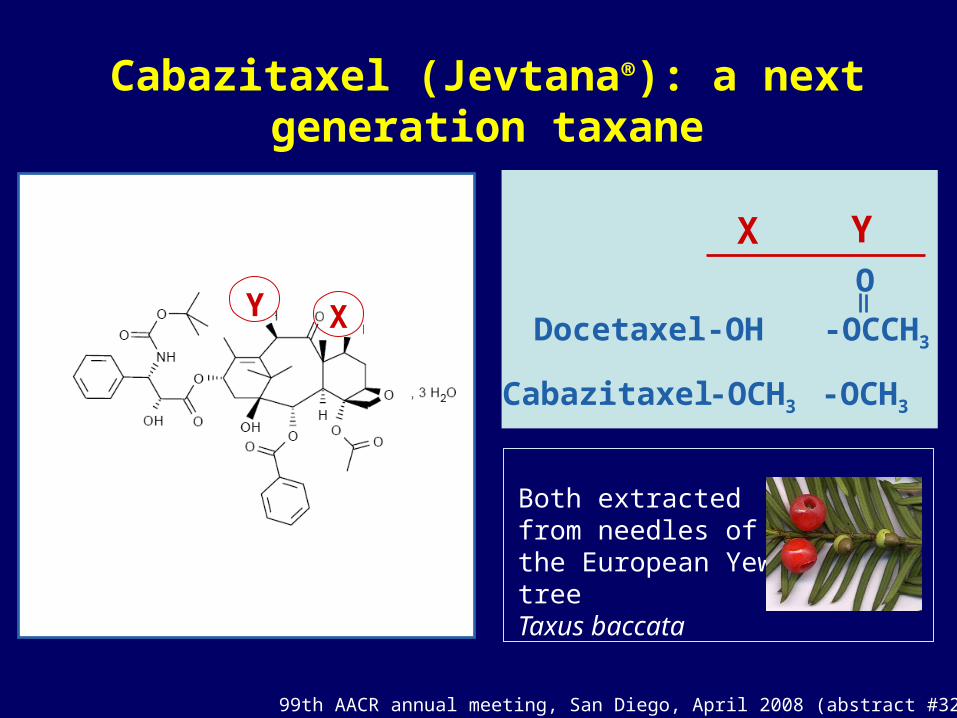
Cabazitaxel (Jevtana®): a next generation taxane
Both extracted from needles of the European Yew treeTaxus baccata
XY
X Y
Docetaxel
Cabazitaxel
-OH
-OCH3 -OCH3
-OCCH3
O
99th AACR annual meeting, San Diego, April 2008 (abstract #3227)
Cabazitaxel: A Major Advance in mHRPC Treatment
• Selected over 450 docetaxel analogues for it’s ability to overcome taxane resistance
• Cabazitaxel– As potent as docetaxel
against sensitive cell lines and tumor models
– Active in vitro and in vivo against tumor models resistant to currently available taxanes
Cabazitaxel1
Galsky MD et al. Nat Rev Drug Discov. 2010;9:677-8 Mita AC et al. Clin Cancer Res. 2009;15(2):723-730.
Cabazitaxel Prescribing Information. Bridgewater, NJ: sanofi-aventis U.S. LLC; June 2010.
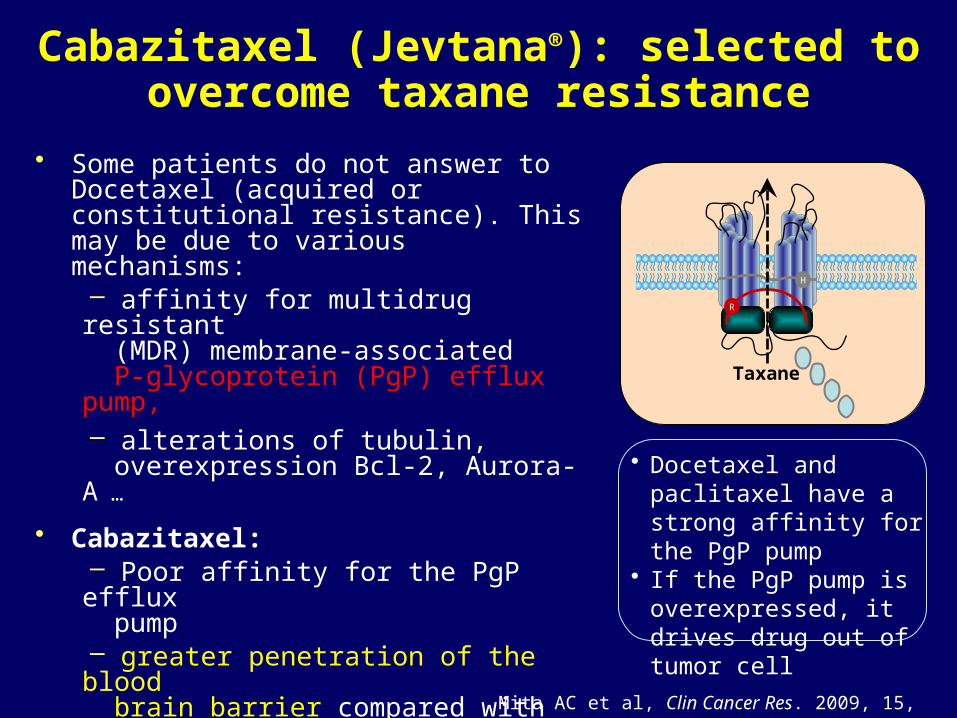
Cabazitaxel (Jevtana®): selected to overcome taxane resistance
• Some patients do not answer to Docetaxel (acquired or constitutional resistance). This may be due to various mechanisms:– affinity for multidrug resistant
(MDR) membrane-associated P-glycoprotein (PgP) efflux pump,– alterations of tubulin,
overexpression Bcl-2, Aurora-A …
• Cabazitaxel:– Poor affinity for the PgP efflux
pump– greater penetration of the blood
brain barrier compared with docetaxel and paclitaxel– Active in vitro and in vivo on
tumors resistant to Docetaxel
Mita AC et al, Clin Cancer Res. 2009, 15, 723-730
Taxane
H
R
• Docetaxel and paclitaxel have a strong affinity for the PgP pump
• If the PgP pump is overexpressed, it drives drug out of tumor cell

De Bono J et al. Lancet, 2010, 376:1147-54
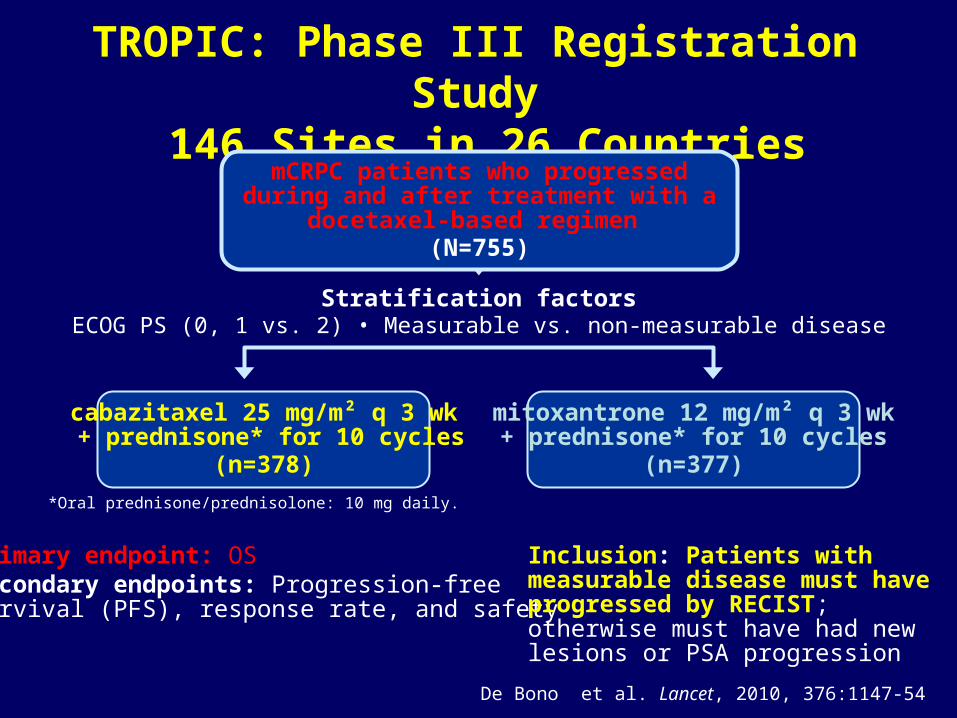
TROPIC: Phase III Registration Study 146 Sites in 26 Countries
Primary endpoint: OSSecondary endpoints: Progression-freesurvival (PFS), response rate, and safety
Inclusion: Patients with measurable disease must have progressed by RECIST; otherwise must have had new lesions or PSA progression
cabazitaxel 25 mg/m² q 3 wk + prednisone* for 10 cycles
(n=378)
mitoxantrone 12 mg/m² q 3 wk+ prednisone* for 10 cycles
(n=377)*Oral prednisone/prednisolone: 10 mg daily.
Stratification factorsECOG PS (0, 1 vs. 2) • Measurable vs. non-measurable disease
mCRPC patients who progressed during and after treatment with a docetaxel-based regimen
(N=755)
De Bono et al. Lancet, 2010, 376:1147-54
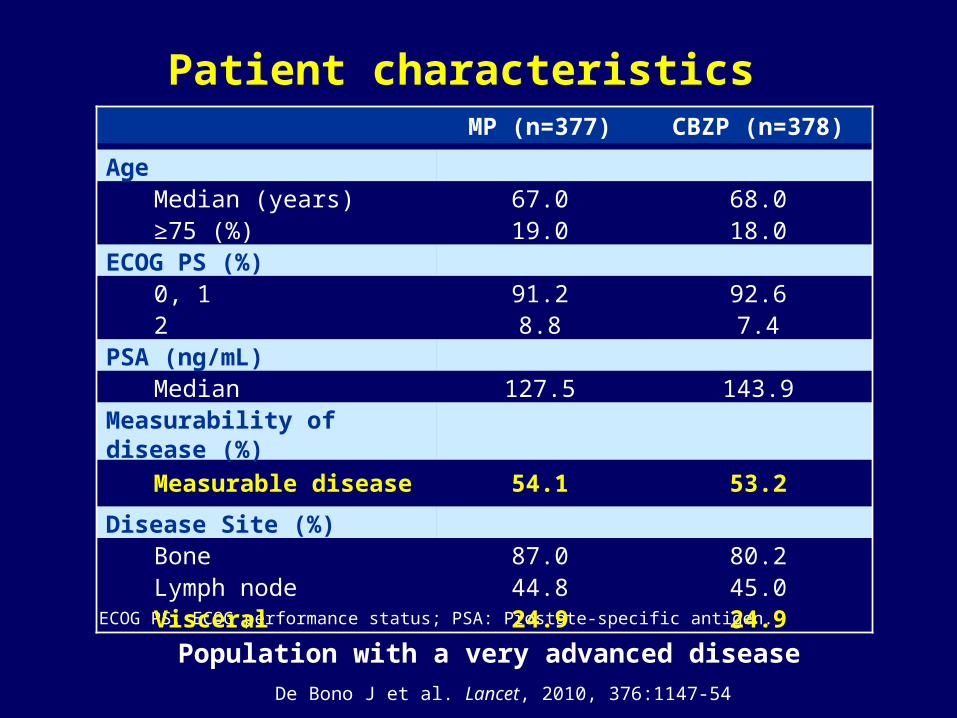
Patient characteristics
ECOG PS: ECOG performance status; PSA: Prostate-specific antigen.
MP (n=377) CBZP (n=378)
Age
Median (years) 67.0 68.0≥75 (%) 19.0 18.0
ECOG PS (%)
0, 1 91.2 92.62 8.8 7.4
PSA (ng/mL)
Median 127.5 143.9Measurability of disease (%)
Measurable disease 54.1 53.2
Disease Site (%)
Bone 87.0 80.2Lymph node 44.8 45.0Visceral 24.9 24.9
De Bono J et al. Lancet, 2010, 376:1147-54
Population with a very advanced disease
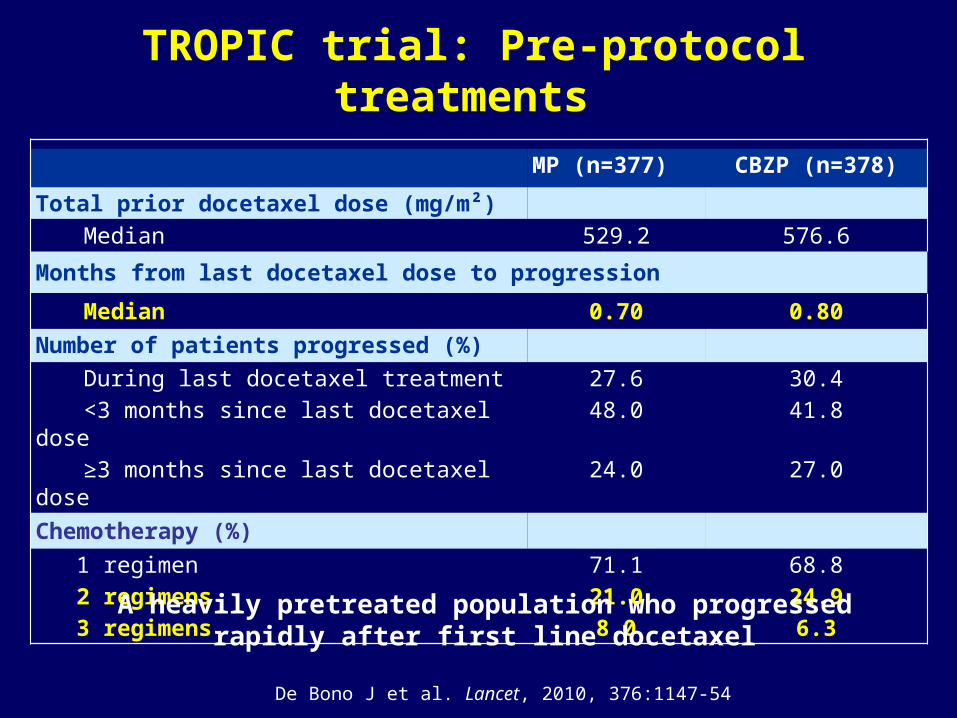
TROPIC trial: Pre-protocol treatments
MP (n=377) CBZP (n=378)
Total prior docetaxel dose (mg/m²)Median 529.2 576.6
Months from last docetaxel dose to progression
Median 0.70 0.80Number of patients progressed (%)
During last docetaxel treatment 27.6 30.4<3 months since last docetaxel dose 48.0 41.8≥3 months since last docetaxel dose 24.0 27.0
Chemotherapy (%) 1 regimen 71.1 68.8 2 regimens 21.0 24.9 3 regimens 8.0 6.3
De Bono J et al. Lancet, 2010, 376:1147-54
A heavily pretreated population who progressedrapidly after first line docetaxel
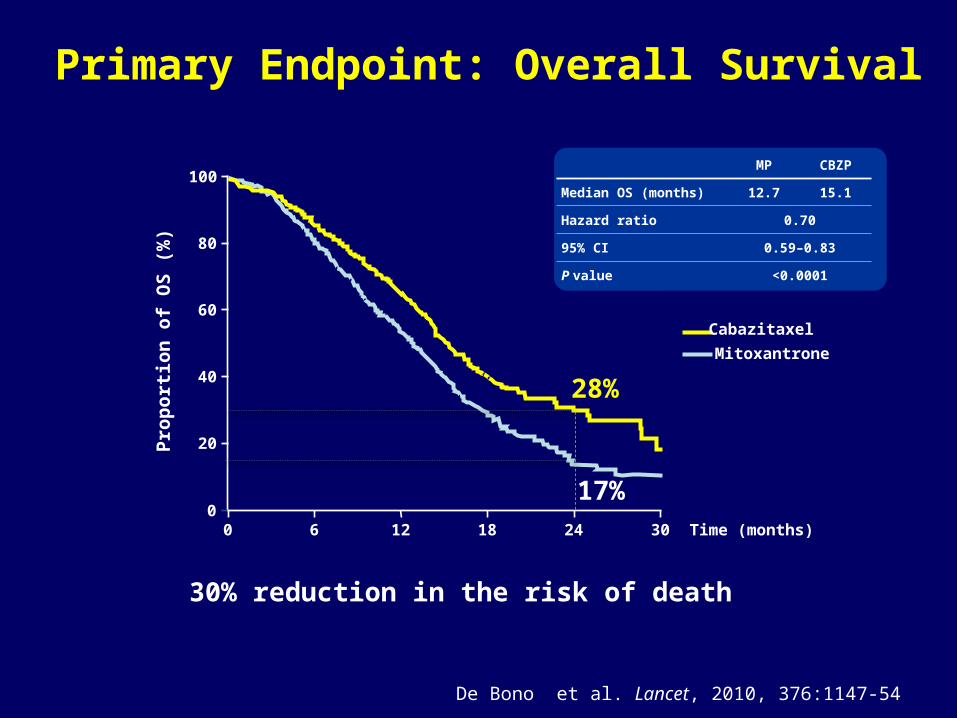
Primary Endpoint: Overall Survival
De Bono et al. Lancet, 2010, 376:1147-54
30% reduction in the risk of death
MP CBZP
Median OS (months) 12.7 15.1
Hazard ratio 0.70
95% CI 0.59–0.83
P value <0.0001
Pro
po
rtio
n o
f O
S (
%)
100
80
60
40
20
0
Mitoxantrone
Cabazitaxel
0 6 12 18 24 30
28%
17%Time (months)
32
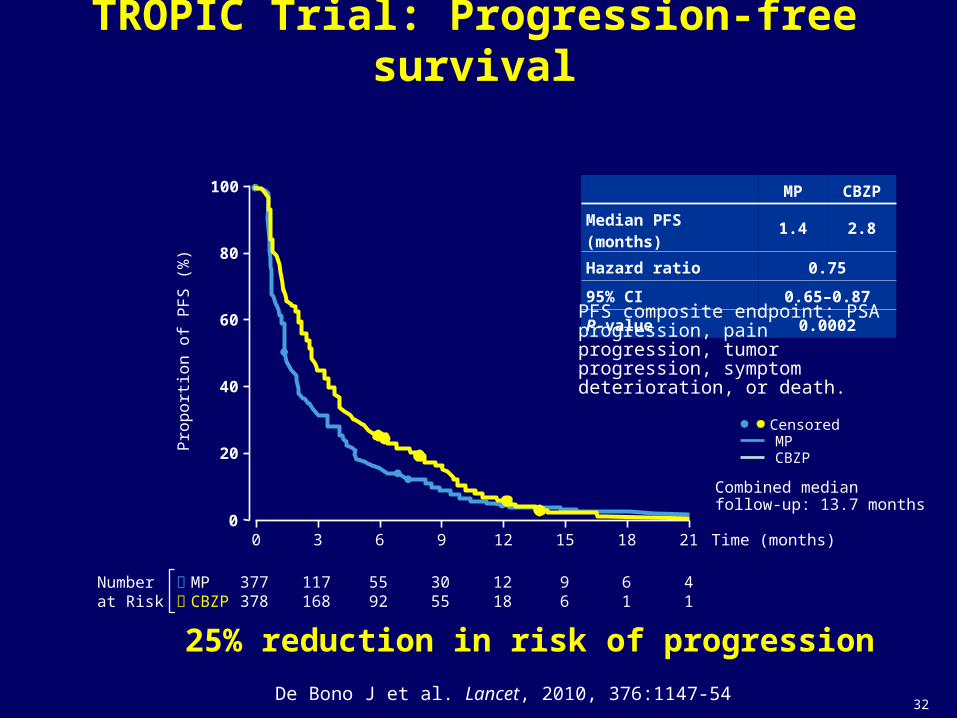
TROPIC Trial: Progression-free survival
Pro
po
rtio
n o
f P
FS
(%
)
377378
5592
1218
61
41
100
80
60
40
20
0Time (months)0 6 12 18 213 9 15
117168
3055
96
MP CBZP
Median PFS (months) 1.4 2.8
Hazard ratio 0.75
95% CI 0.65–0.87
P-value 0.0002
Numberat Risk
MP CBZP
CensoredMPCBZP
Combined medianfollow-up: 13.7 months
PFS composite endpoint: PSA progression, pain progression, tumor progression, symptom deterioration, or death.
De Bono J et al. Lancet, 2010, 376:1147-54
25% reduction in risk of progression
33
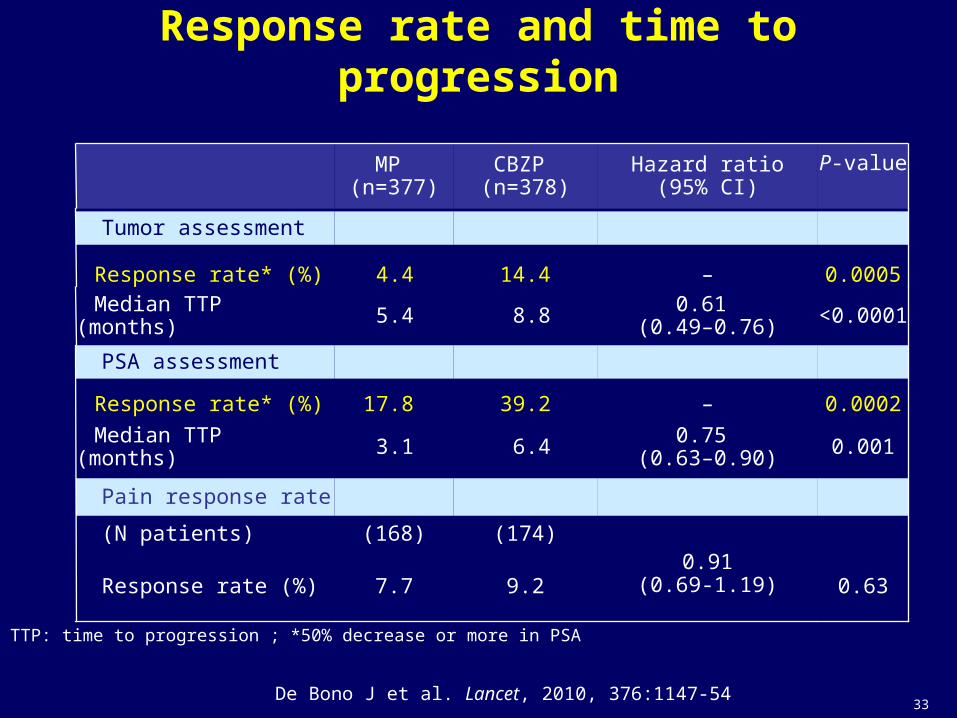
TROPIC Trial: Response rate and time to progression
(174)(168) (N patients)
Pain response rate
0.0010.75 (0.63–0.90)6.43.1Median TTP (months)
0.630.91
(0.69-1.19)9.27.7 Response rate (%)
MP (n=377)
CBZP (n=378)
Hazard ratio(95% CI)
P-value
Tumor assessment
Response rate* (%) 4.4 14.4 – 0.0005
Median TTP (months) 5.4 8.8 0.61 (0.49–0.76) <0.0001
PSA assessment
Response rate* (%) 17.8 39.2 – 0.0002
TTP: time to progression ; *50% decrease or more in PSA
De Bono J et al. Lancet, 2010, 376:1147-54
34
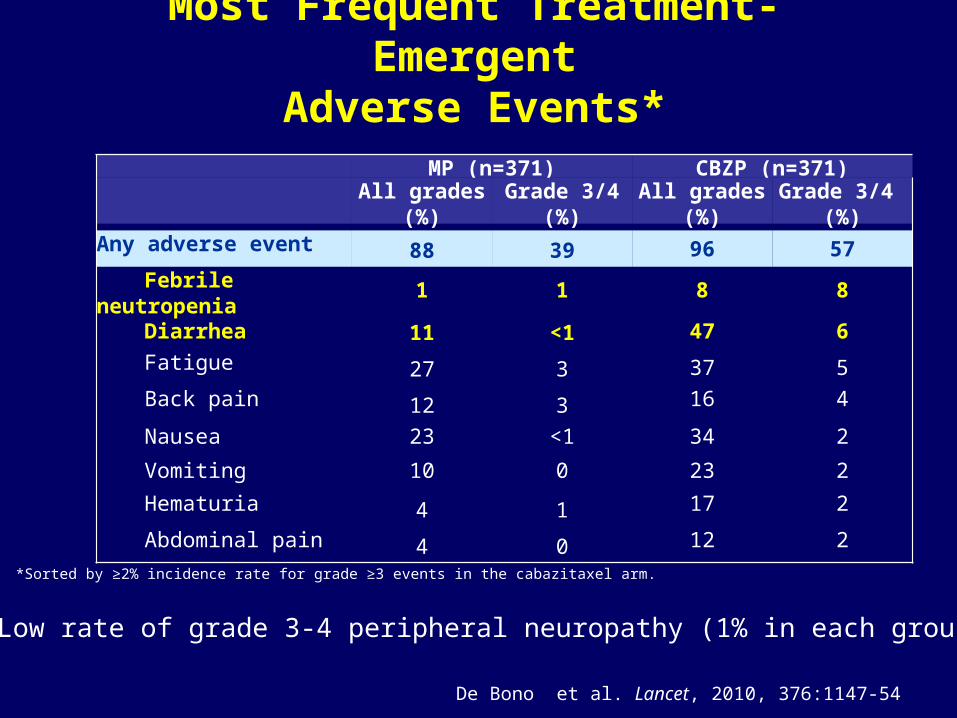
MP (n=371) CBZP (n=371)All grades
(%)Grade 3/4
(%)All grades
(%)Grade 3/4
(%)Any adverse event 88 39 96 57
Febrile neutropenia 1 1 8 8
Diarrhea 11 <1 47 6Fatigue 27 3 37 5Back pain 12 3 16 4
Nausea 23 <1 34 2
Vomiting 10 0 23 2
Hematuria 4 1 17 2
Abdominal pain 4 0 12 2
Most Frequent Treatment-EmergentAdverse Events*
*Sorted by ≥2% incidence rate for grade ≥3 events in the cabazitaxel arm.
Low rate of grade 3-4 peripheral neuropathy (1% in each group)
De Bono et al. Lancet, 2010, 376:1147-54
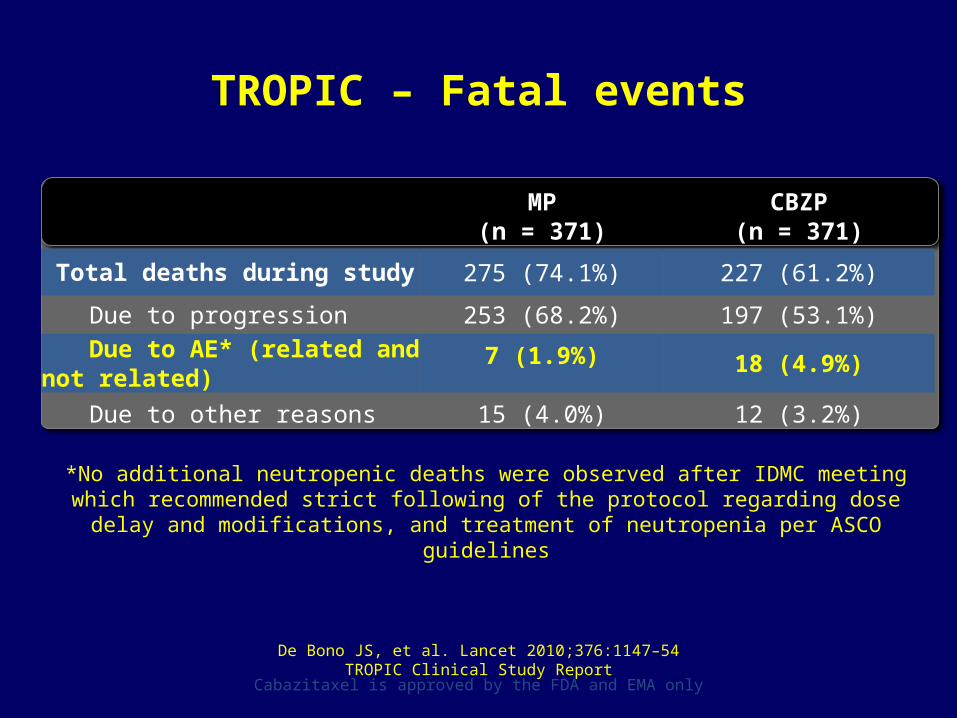
TROPIC – Fatal events
MP(n = 371)
CBZP(n = 371)
Total deaths during study 275 (74.1%) 227 (61.2%)
Due to progression 253 (68.2%) 197 (53.1%)Due to AE* (related and not
related)7 (1.9%) 18 (4.9%)
Due to other reasons 15 (4.0%) 12 (3.2%)
*No additional neutropenic deaths were observed after IDMC meeting which recommended strict following of the protocol regarding dose delay and modifications, and treatment of
neutropenia per ASCO guidelines
De Bono JS, et al. Lancet 2010;376:1147–54TROPIC Clinical Study Report
Cabazitaxel is approved by the FDA and EMA only
Management of AEs
• Patient selection is critical• Patient education is critical• Chemotherapy to be given in experienced
centres• G-CSF as per ASCO guidelines
EAU guidelines
• EAU guidelines: – Cabazitaxel should be considered as an effective
second-line treatment following docetaxel(Level of evidence A)
Mottet N, et al. Eur Urol 2011;59:572–83
38
Conclusion on Cabazitaxel study
• Cabazitaxel demonstrated a statistically and clinically significant survival improvement compared with mitoxantrone in study population– 15.1 months vs 12.7 months– 28% reduced risk of death (HR=0.72, P <.0001)– Survival benefit consistent across subgroups
• Secondary endpoints of PFS, RR, and TTP also significantly improved
• Safety profile was manageable– Proactive management of side effects recommended
(neutropenia/diarrhea)Cabazitaxel is the first treatment to show a survival benefit in patients with mCRPC after failure of docetaxel-based therapy
39
Cabazitaxel: Further development
• Which dose of cabazitaxel to use 25 or 20 mg/m2?• Is cabazitaxel as effective as docetaxel in first-line setting?
• Is cabazitaxel more or less hematotoxic than docetaxel?
• Will cabazitaxel be evaluated in early stages?
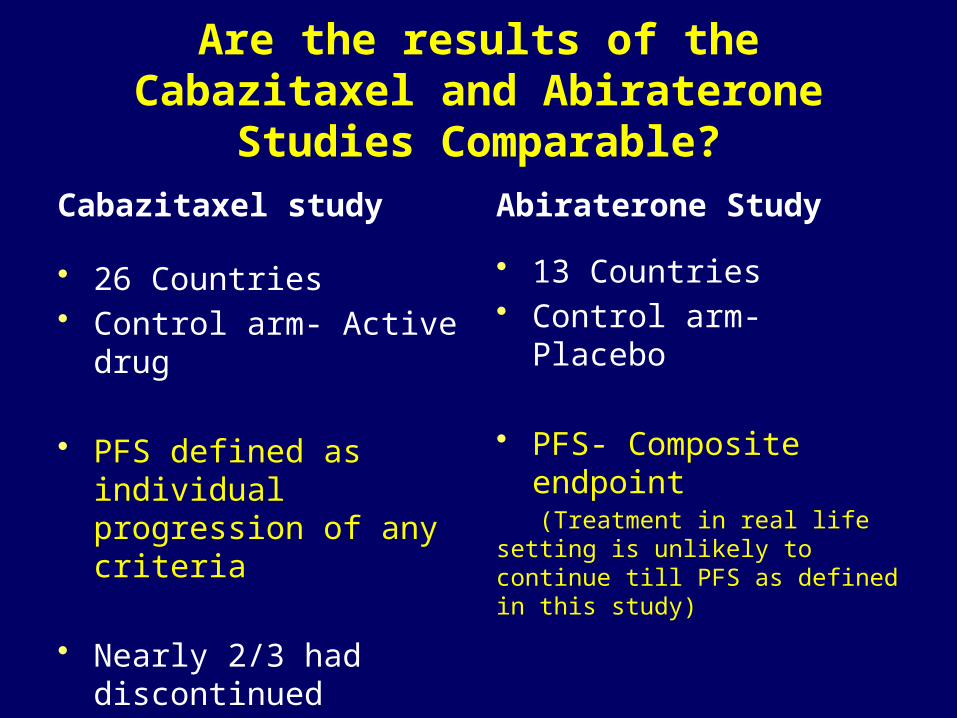
Are the results of the Cabazitaxel and Abiraterone Studies Comparable?
Cabazitaxel study
• 26 Countries• Control arm- Active drug
• PFS defined as individual progression of any criteria
• Nearly 2/3 had discontinued previous Docetaxel therapy due to disease progression
Abiraterone Study
• 13 Countries• Control arm- Placebo
• PFS- Composite endpoint (Treatment in real life setting is unlikely to continue till PFS as defined in this study)
• Not specified
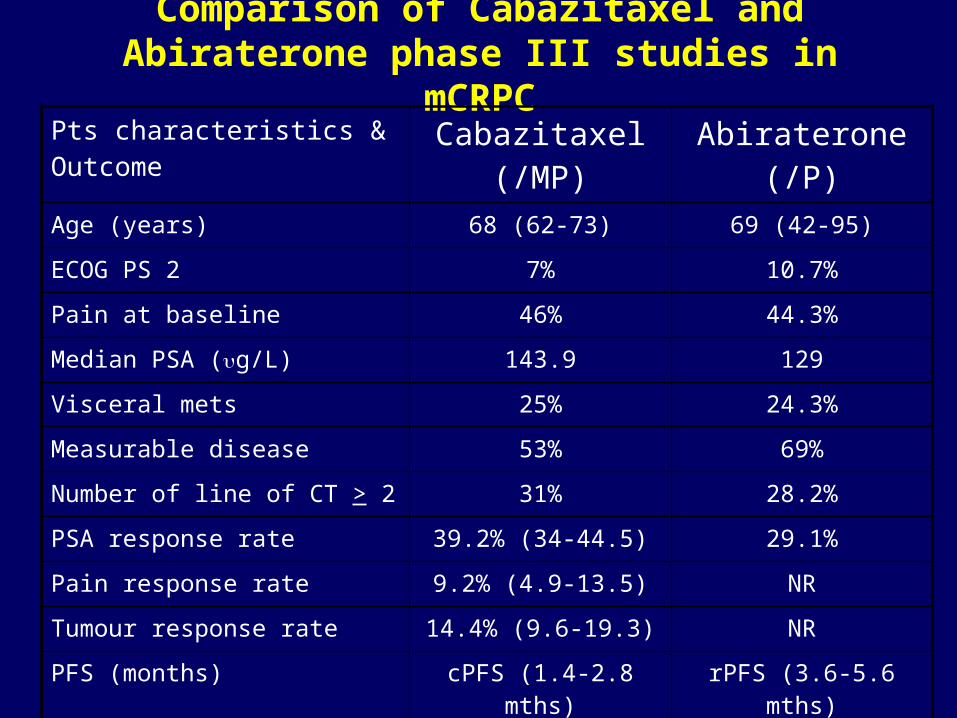
Comparison of Cabazitaxel and Abiraterone phase III studies in mCRPC
Pts characteristics & Outcome Cabazitaxel (/MP) Abiraterone (/P)Age (years) 68 (62-73) 69 (42-95)
ECOG PS 2 7% 10.7%
Pain at baseline 46% 44.3%
Median PSA (ug/L) 143.9 129
Visceral mets 25% 24.3%
Measurable disease 53% 69%
Number of line of CT > 2 31% 28.2%
PSA response rate 39.2% (34-44.5) 29.1%
Pain response rate 9.2% (4.9-13.5) NR
Tumour response rate 14.4% (9.6-19.3) NR
PFS (months) cPFS (1.4-2.8 mths) rPFS (3.6-5.6 mths)
Overall Survival (months) 12.7 —› 15.1 10.9 —› 14.8
My reasons for giving Cabazitaxel first
• TROPIC had about 70% patients who were ‘early’ progressors
• Ensures patients have the option of having both treatments (Cabazitaxel and then Abiraterone)
• Tolerance in ‘real life’ setting is better than in TROPIC study with QOL benefits
• Option of entering patients into further hormone therapy trials post-cabazitaxel
• Paramount to have a full and fair discussion with the patient and their carers
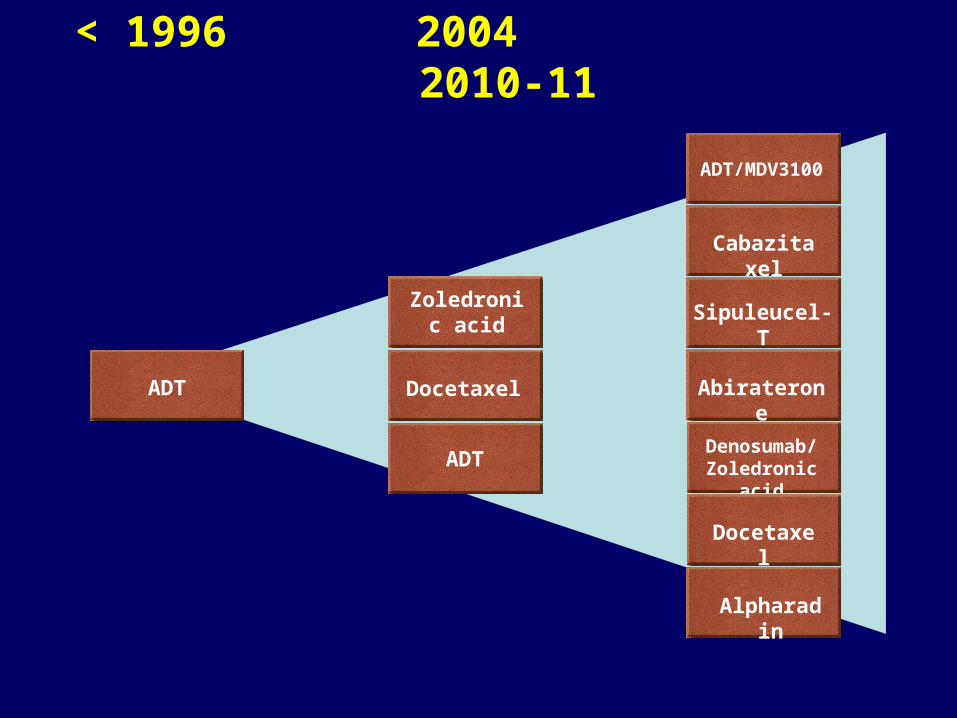
< 1996 2004 2010-11
Zoledronic acid
Docetaxel
ADTDenosumab/
Zoledronic acid
Sipuleucel-T
Alpharadin
Docetaxel
Cabazitaxel
ADT/MDV3100
AbirateroneADT
Patient management: a patient-centred partnership
Partnership
Urologists Oncologists
Nurses/Pharmacists
Support Support
Patient





























