Embed Size (px)
Citation preview

Small Molecule Detection in Saliva Facilitates Portable Tests ofMarijuana AbuseJung-Rok Lee,†,§ Joohong Choi,‡,§ Tyler O. Shultz,†,§ and Shan X. Wang*,†,‡
†Department of Materials Science and Engineering, Stanford University, Stanford, California 94305, United States‡Department of Electrical Engineering, Stanford University, Stanford, California 94305, United States
*S Supporting Information
ABSTRACT: As medical and recreational use of cannabis, ormarijuana, becomes more prevalent, law enforcement needs atool to evaluate whether drivers are operating vehicles underthe influence of cannabis, specifically the psychoactivesubstance, tetrahydrocannabinol (THC). However, the cutoffconcentration of THC that causes impairment is stillcontroversial, and current on-site screening tools are notsensitive enough to detect trace amounts of THC in oral fluids.Here we present a novel sensing platform that employs giantmagnetoresistive (GMR) biosensors integrated with a portablereader system and smartphone to detect THC in saliva usingcompetitive assays. With a simple saliva collection scheme, wehave optimized the assay to measure THC in the range from 0to 50 ng/mL, covering most cutoff values proposed in previous studies. This work facilitates on-site screening for THC andshows potential for testing of other small molecule drugs and analytes in point-of-care (POC) settings.
Since 1970, cannabis has been classified as a Schedule Isubstance under the Controlled Substances Act, indicating
a high potential for abuse and a lack of medical value.1
However, in light of evidence about its therapeutic effect,2,3 23states and the District of Columbia in the United States haverecently legalized the medical use of cannabis. Four states(Alaska, Colorado, Oregon, and Washington) have evenlegalized its recreational use. These legislation changes haveraised concerns about individuals driving under the influence(DUI) of marijuana. In fact, the states that have legalized thedrug have reported a substantial increase in cases of DUI ofcannabis.4−6 To regulate DUI drivers, on-site tests for one ofthe most potent psychoactive agents in cannabis, Δ9-tetrahydrocannabinol (Δ9-THC, or THC), similar to abreathalyzer for estimating blood alcohol content (BAC), areurgently needed. Although the gold standard for forensicanalysis of THC is chromatography combined with massspectroscopy using blood samples, the bulky equipmentrequired for this is not suitable for road tests, and collectionof blood would require testers to have training in taking bloodsamples. Moreover, urine tests, which are the most widely usedmethod in drug testing, can detect only THC metabolites,which only become detectable in urine at least several hoursafter intake of cannabis, far past the window of intoxication andimpairment.7,8 Furthermore, there is preliminary evidence thatthe concentration of THC in saliva can be correlated withimpairment.7,9 Thus, for road tests, oral fluids (saliva) arepreferred because they enable noninvasive and rapid measure-ments of THC. However, two significant problems with on-site
screening of THC in oral fluids exist. The first is that no solidscientific consensus exists on the cutoff concentration of THCat which drivers’ performance is clearly impaired,8−10 eventhough it is clear that THC impairs its users’ cognitive andpsychomotor abilities.11 A possible reason on the unestablishedcutoff is that pharmacokinetics of THC and its effect arecomplicated because THC accumulates in fatty tissues due toits high solubility in lipids.12 Therefore, the concentration ofTHC at the time of measurement could be different from thatwhen a driver is behind the wheel or under the influence.12−14
Another reason could be that different studies have useddifferent techniques to detect THC in oral fluids, and this mayfurther generate discrepancies between the results. The secondproblem with on-site screening is that current rapid test toolsare not sensitive enough to detect THC within the variousproposed ranges of cut-offs.7,15 To overcome these problems,many research groups have developed various techniques todetect THC in saliva.16−18
Here, we report a mobile technology that facilitates rapid andprecise measurement of THC in oral fluids using magneticbiosensors. The technology is based on GMR biosensors, whichhave been demonstrated to measure cancer,19 radiation,20 andcardiovascular biomarkers,21 in conjunction with magneticnanoparticles (MNPs),22−27 after the advent of the initialconcepts.28 The miniaturized platform with disposable chip
Received: April 28, 2016Accepted: July 19, 2016Published: July 19, 2016
Letter
pubs.acs.org/ac
© 2016 American Chemical Society 7457 DOI: 10.1021/acs.analchem.6b01688Anal. Chem. 2016, 88, 7457−7461

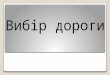
cartridges incorporates Bluetooth communication protocols,which enable POC measurement and compatibility with anytypes of smartphones or laptops equipped with Bluetooth ports(Figure 1A). The GMR biosensor chip consists of 80 sensors
that can be individually functionalized for multiplex assays(Figure 1B). A new concept of toroidal core coil for applying anexternal magnetic field and a compact design of circuit boardreduced power consumption significantly and improved theportability of the device (Figure S1).To measure small molecules such as THC (molecular
weight, 314.5 Da), we employed competitive assays instead oftraditional sandwich assays, as demonstrated previously,16
because the small molecules usually lack two binding sites(i.e., epitopes) required for the sandwich assays.29,30 Even
though these molecules have sufficient epitopes for binding totwo antibodies, the sandwich cannot be formed due to sterichindrance. Our competitive assay requires only one type ofantibody that can recognize THC and link MNPs to the boundTHC on the surface of the biosensor via biotin−streptavidininteraction (Figure 1C). The biotinylated antibodies wereadded to the sample of interest that contained THC andincubated for 15 min to bind to THC in the sample aspreincubation (details in Supporting Information). Then, 50 μLof the mixture were added to the chip where bovine serumalbumin (BSA) and THC conjugated with BSA (THC-BSA)were immobilized on different sensors to allow unoccupiedantibodies to bind to THC-BSA on the sensors for anadditional 15 min. After washing the chip, the chip cartridgewas inserted into the measurement reader, and 40 μL ofstreptavidin-coated MNPs were introduced. The stray fieldfrom the bound MNPs disturbs the magnetization of biosensorsunderneath, which changes the resistance of the biosensor. Thechanges in resistance, monitored as GMR biosensor signals(ΔMR/MR0), are proportional to the number of boundMNPs31 and have an inverse relationship with the concen-tration of THC in the sample due to the nature of competitiveassays. Figure 1D shows the measurement signals for THC at 5ng/mL spiked in saliva using the smartphone and customizedapp shown in Figure 1A. To the best of our knowledge, this isthe first demonstration that GMR biosensors are capable ofdetecting small molecules.To collect saliva samples from drivers, we have developed a
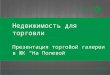
simple sample collection strategy using a cotton swab, syringe,and filter unit, which can be easily performed without anytrained medical professional (Figure 2). First, oral fluid is
collected with a cotton swab. The swab is then inserted into asyringe and squeezed to release the fluid. This step replaces acentrifuging process, which is not manageable on the road. Thefilter unit attached to the syringe further removes viscousmucus, food particles, and extra debris in the sample. Thisapproach could also address the contamination issue, previouslyreported,32 that causes high concentrations of THC at theinitial measurement. In our testing, we collected saliva samplesfrom a donor in our research group who claimed to be drug-free and used them to dilute THC.Although there is no solid scientific consensus on the cutoff
concentration of THC, most previous studies have suggestedthe values ranging from 2 to 25 ng/mL.9,15,33 To achieve bettersensitivity around this range, we optimized the concentration ofanti-THC biotinylated antibodies and incubation time. First,
Figure 1. GMR biosensor platform and competitive assays. (A) Left: ameasurement reader includes a toroid core coil, electrical circuits, andBluetooth module. The dimension of the reader is 105 mm × 90 mm.Middle: a disposable cartridge is based on a customized design ofprinted circuit board (PCB) integrated with a GMR biosensor chipand reaction well. Right: a smartphone with customized app. (B)Disposable cartridge. GMR biosensor chip was wire-bonded to thecustomized PCB, and the reaction well was glued on top of the chip.The GMR biosensor chip consists of 80 sensors, and the last row (8sensors at the bottom) are used as electrical reference sensors. As anexample, capture probes (BSA or THC-BSA) were spotted on foursensors in the middle. The scale bar is 500 μm. (C) Schematic ofcompetitive assay. Step 1: anti-THC biotinylated antibodies weremixed with a THC-containing sample and preincubated to bind toTHC. Yellow circles represent THC. Step 2: the mixture was added tothe chip where BSA and THC-BSA were immobilized on differentsensors and incubated for unoccupied antibodies to bind THC-BSA.Step 3: Unbound antibodies were washed, and MNPs were added tothe chip to read out the signals. (D) Real-time measurement signals.The chip was added to the reader, and MNPs were then added to thechip at ∼1.5 min. THC-BSA, BSA, and biotinylated BSA (Biotin-BSA)were immobilized on different sensors, and signals from these sensorswere monitored. The signals are the average of 8 identical sensorsignals and referenced to the averaged signal from reference sensors.The error bars represent standard deviations of 8 identical sensorsignals.
Figure 2. Saliva collection scheme. Step 1: A cotton swab, filter unit,and syringe are prepared. Plunger of the syringe is completely pulledout. The cotton swab is placed for 1 or 2 min in the mouth of anindividual who is being tested to fully absorb oral fluids. Step 2: Thefilter unit is attached to the syringe, and the saturated cotton swab isloaded into the syringe. Step 3: The cotton swab is squeezed using theplunger, and the released fluid is collected in a test tube.
Analytical Chemistry Letter
DOI: 10.1021/acs.analchem.6b01688Anal. Chem. 2016, 88, 7457−7461
7458

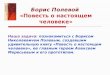
three different concentrations of antibodies (5, 1, and 0.5 μg/mL) were tested with zero analyte and THC at 5 and 20 ng/mL, respectively (Figure 3A). The antibodies at 5 μg/mL
showed less reduction in signals as the concentration of THCincreases compared to other antibody concentrations, whichresults in a wider dynamic range. The concentration of 1 μg/mL produced a fairly linear titration curve within the range,while 0.5 μg/mL showed a steeper drop at 5 ng/mL of THCbut almost the same signal as 1 μg/mL of antibodies at 20 ng/mL of THC. In addition, the mass concentrations of antibodies(1 μg/mL) and THC (5 ng/mL) correspond to 7 nM and 16nM in molar concentration, respectively. Considering thebivalency of the antibody, the binding capacity is well-matched.Thus, the depletion of antibodies by THC was effectivelymonitored in the competitive assays, and we therefore usedantibodies at 1 μg/mL for subsequent experiments. Todetermine an optimal time frame for incubation of a samplemixture with the chip, three different incubation times (5, 10,and 15 min) for the chip incubation were tested with 15 min ofpreincubation (Figure 3B). The signals were saturated foraround 15 min, and the difference between signals of 0 and 5ng/mL of THC was maximized in the case of 15 min of chipincubation. Using these conditions (1 μg/mL of antibodies and15 min/15 min incubation), we obtained a titration curve witha dynamic range from 0 to 50 ng/mL of THC in saliva (Figure
3C). Furthermore, preincubation and chip-incubation timeswere reduced to 5 and 10 min, respectively, and the GMRsensor signals were taken at 5 min after adding MNPs insteadof 10 min to carry out the entire measurement within 20 min(Figure S2). The result showed no significant loss inperformance. This was because the signal levels of 10 minchip-incubation was fairly close to those of 15 min incubationas shown in Figure 3B, and the sensor signals typically reachedtheir plateaus within less than 5 min after addition of MNPs asshown in Figure 1D. Moreover, the result revealed thatpreincubation time was still not a limiting factor when it was setto 5 min. Since the preincubation is three-dimensional mixingand binding between THC and antibodies, which is much fasterthan binding of antibodies to THC on planar surfaces duringthe chip-incubation, the preincubation could be furtherreduced, compared to the chip-incubation. Without anypreincubation, THC in a wider dynamic range (0 to 200 ng/mL) was detected with 5 μg/mL of antibodies within 3 min oftotal assay time (Figure 3D), which showed promise forroadside testing. In this case, a higher concentration ofantibodies warranted less chip-incubation time to obtain asubstantial signal of antibody binding to THC on the surface.In a similar manner, the assay can be further tailored to adjustthe sensitivity and dynamic range by changing antibodyconcentration and incubation time if the cutoff concentrationof THC is beyond the current range.Since the binding of the antibodies to THC is a
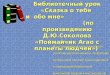
thermodynamic process, the temperature affects the assayresults and there are day-to-day variations in measurementsignals due to temperature fluctuations, chip-to-chip variations,or incubation time variations. Thus, to increase accuracy of theassay and minimize the measurement variation, we havedesigned a two-compartment cartridge where two reactionwells are installed on a GMR biosensor chip to measure boththe sample of interest and a reference sample simultaneouslywith the same chip (Figure 4A), which ensures that bothsamples experience the same experimental condition includingtemperature, incubation time, and biochip fabrication. Sincetwo samples are measured with the same chip at the same time,all measurement variation such as chip-to-chip variation,
Figure 3. Optimization of the assay and titration curves. (A)Sensitivity and dynamic range tuning with antibody concentration.Three antibody concentrations (5, 1, and 0.5 μg/mL) were tested with3 different sample concentrations (0, 5, and 20 ng/mL), respectively.The signals at 5 and 20 ng/mL were normalized by the signal at 0 ng/mL for each antibody concentration for comparison. (B) Optimizationof chip incubation time. The antibodies at 1 μg/mL were used todetect both THC at 0 and 5 ng/mL with 3 different chip incubationdurations. A 15 min preincubation was performed to mix the samplewith antibodies. The data point is denoted with an asterisk if Welch’s t-test shows p < 0.01. (C) Titration curve of the assay with salivasamples. The concentration of THC in the sample varied from 0 to100 ng/mL. The biotinylated antibodies at 1 μg/mL and 15 minpreincubation/15 min chip incubation were used. (D) 3 min assaysusing single step incubation without preincubation. The mixture of thesample and antibody was immediately added to the chip and incubatedfor 2 min. The concentration of the antibodies was 5 μg/mL, and thesignals were obtained 1 min after adding MNPs. The signals are theaverage of 4 identical sensors, and the error bars represent thestandard deviations.
Figure 4. Two-compartment cartridge. (A) Customized design of two-compartment cartridge. A GMR biosensor chip was wire-bonded tothe PCB, and a two-compartment reaction well with a gasket made ofpolydimethylsiloxane (PDMS) was assembled on the chip. Eachcompartment includes 20 biosensors. (B) Simultaneous THCmeasurement of two samples. Saliva samples containing THC at 0and 5 ng/mL, respectively, were measured with the same chip usingthe two-compartment cartridge. The average and standard deviation ofsignals from 4 THC-BSA coated sensors in each compartment (blueand red) are shown. The p-value was determined using Welch’s t-test.
Analytical Chemistry Letter
DOI: 10.1021/acs.analchem.6b01688Anal. Chem. 2016, 88, 7457−7461
7459

temperature fluctuation, and reagent variation can be reducedor even eliminated. For demonstration, saliva samplescontaining 0 and 5 ng/mL of THC, respectively, weremeasured with the two-compartment cartridge (Figure 4B).With the measurement using the two-compartment cartridge,the tester can easily determine whether the test result is positiveor negative by the difference between the signals of twosamples. For example, if it is assumed that the cutoffconcentration is 5 ng/mL (reference sample) and the samplewithout THC (0 ng/mL) is collected from a driver, the testresult is negative, i.e., a higher signal than the reference samplemeans negative, and a signal lower than or equal to thereference is positive.To investigate whether the competitive assay could be
applicable to other small molecules, we performed measure-ment of morphine (285.3 Da) by replacing THC withmorphine. The sensors were coated with morphine-BSA inlieu of THC-BSA, and antimorphine antibodies at 0.1 μg/mLwere used. The signals from zero analyte, morphine at 10 and100 ng/mL showed statistically significant differences (FigureS3).In summary, we have demonstrated that the miniaturized
GMR biosensor platform enables rapid and precise detection ofTHC in saliva. This platform validated the technical feasibilityfor on-site screening on drivers under the influence, and ourresults showed that the technique could be used to establish thecutoff concentration of THC, performing the tests without anydelays involved with transferring samples to the clinicallaboratories. In addition, the platform is capable of detectingTHC in blood (Figure S4), because GMR biosensors arematrix-insensitive.19 Thus, the correlation between concen-trations of THC in blood and saliva, which is currentlycontroversial,7,9,33,34 could be addressed with a more accuratecomparison using the same measurement modality. With themultiplexing capability of the GMR biosensor chip, the nextgeneration of the platform could include metabolites of THCon the sensors to simultaneously detect THC and itsmetabolites in blood and urine. This multiplex measurementwould allow researchers to study the pharmacokinetics of thedrug more rigorously. Furthermore, because it has beenrecently reported that 11-nor-9-Carboxy-THC (THC-COOH) in saliva could be a better biomarker to detectcannabis use,35 it would be interesting to measure THC-COOH and THC together to increase the accuracy of the testand develop a new criterion of cutoff. In addition, if there is abetter biomarker that can reveal THC’s pharmacodynamics inthe brain and the relationship with its concentration in blood orsaliva, it could be a more precise indicator for the level ofimpairment. However, there is a potential limitation of testingTHC in saliva. THC in saliva is thought to originate from oralmucosal depots, not from blood.32 Thus, if cannabis isconsumed through edibles it would be difficult to detectTHC in saliva. Lastly, since the competitive assays areapplicable to detection of any type of small molecules, theplatform could be used to detect different drugs such as heroinand cocaine in addition to THC and morphine as well as todetect therapeutic small molecule inhibitors in cancer treat-ments.36,37
■ ASSOCIATED CONTENT*S Supporting InformationThe Supporting Information is available free of charge on theACS Publications website at DOI: 10.1021/acs.anal-chem.6b01688.
Full experimental details, electronics, 20 min assays,morphine measurement, and measurement of THC inblood (Figures S1−S4) (PDF)
■ AUTHOR INFORMATIONCorresponding Author*E-mail: [email protected]. Fax: +1 (650) 736-1984.Author Contributions§J.-R.L., J.C., and T.O.S. contributed equally.NotesThe authors declare the following competing financialinterest(s): J.-R.L., T.O.S., and S.X.W. have related patents orpatent applications assigned to Stanford University and out-licensed for potential commercialization. S.X.W. has stock orstock options in MagArray, Inc., which has licensed relevantpatents from Stanford University for commercialization ofGMR biosensor chips.
■ ACKNOWLEDGMENTSThis work was supported in part by Stanford Center forMagnetic Nanotechnology and Skippy Frank TranslationalFund. J.C. acknowledges the STX Foundation fellowship. Wewould like to acknowledge the XPRIZE Foundation and NokiaSensing XCHALLENGE competition for motivating the designof the platform.
■ REFERENCES(1) Bostwick, J. M. Mayo Clin. Proc. 2012, 87, 172−186.(2) Hoffmann, D. E.; Weber, E. N. Engl. J. Med. 2010, 362, 1453−1457.(3) Hill, K. P. JAMA 2015, 313, 2474−2483.(4) Pollini, R. A.; Romano, E.; Johnson, M. B.; Lacey, J. H. DrugAlcohol Depend. 2015, 150, 135−140.(5) Maxwell, J. C.; Mendelson, B. J. Addict. Med. 2016, 10, 3−12.(6) Wilkinson, S. T.; Yarnell, S.; Radhakrishnan, R.; Ball, S. A.;D’Souza, D. C. Annu. Rev. Med. 2016, 67, 453−466.(7) Kintz, P.; Cirimele, V.; Ludes, B. J. Anal. Toxicol. 2000, 24, 557−561.(8) Allen, K. R. Ann. Clin. Biochem. 2011, 48, 531−541.(9) Ramaekers, J. G.; Moeller, M. R.; van Ruitenbeek, P.; Theunissen,E. L.; Schneider, E.; Kauert, G. Drug Alcohol Depend. 2006, 85, 114−122.(10) Kadehjian, L. Forensic Sci. Int. 2005, 150, 151−160.(11) Ramaekers, J. G.; Robbe, H. W.; O’Hanlon, J. F. Hum.Psychopharmacol. 2000, 15, 551−558.(12) Ashton, C. H. Br. J. Psychiatry 2001, 178, 101−106.(13) Hartman, R. L.; Brown, T. L.; Milavetz, G.; Spurgin, A.;Gorelick, D. A.; Gaffney, G.; Huestis, M. A. Clin. Chem. 2015, 61,850−869.(14) Wood, E.; Brooks-Russell, A.; Drum, P. Traffic Inj Prev 2016, 17,105−108.(15) Verstraete, A. G. Forensic Sci. Int. 2005, 150, 143−150.(16) Bruls, D. M.; Evers, T. H.; Kahlman, J. A.; van Lankvelt, P. J.;Ovsyanko, M.; Pelssers, E. G.; Schleipen, J. J.; de Theije, F. K.;Verschuren, C. A.; van der Wijk, T.; van Zon, J. B.; Dittmer, W. U.;Immink, A. H.; Nieuwenhuis, J. H.; Prins, M. W. Lab Chip 2009, 9,3504−3510.(17) Shao, J.; Li, Z. Y.; Jiang, H.; Wang, W. L.; Wu, Y. X. Proc. SPIE2014, 9297, 92971K.
Analytical Chemistry Letter
DOI: 10.1021/acs.analchem.6b01688Anal. Chem. 2016, 88, 7457−7461
7460

(18) Molnar, A.; Lewis, J.; Doble, P.; Hansen, G.; Prolov, T.; Fu, S.Forensic Sci. Int. 2012, 215, 92−96.(19) Gaster, R. S.; Hall, D. A.; Nielsen, C. H.; Osterfeld, S. J.; Yu, H.;Mach, K. E.; Wilson, R. J.; Murmann, B.; Liao, J. C.; Gambhir, S. S.;Wang, S. X. Nat. Med. 2009, 15, 1327−1332.(20) Kim, D.; Marchetti, F.; Chen, Z.; Zaric, S.; Wilson, R. J.; Hall, D.A.; Gaster, R. S.; Lee, J. R.; Wang, J.; Osterfeld, S. J.; Yu, H.; White, R.M.; Blakely, W. F.; Peterson, L. E.; Bhatnagar, S.; Mannion, B.; Tseng,S.; Roth, K.; Coleman, M.; Snijders, A. M.; Wyrobek, A. J.; Wang, S. X.Sci. Rep. 2013, 3, 2234.(21) Wang, Y.; Wang, W.; Yu, L.; Tu, L.; Feng, Y.; Klein, T.; Wang, J.P. Biosens. Bioelectron. 2015, 70, 61−68.(22) Lee, N.; Yoo, D.; Ling, D.; Cho, M. H.; Hyeon, T.; Cheon, J.Chem. Rev. 2015, 115, 10637−10689.(23) Chapman, S.; Dobrovolskaia, M.; Farahani, K.; Goodwin, A.;Joshi, A.; Lee, H.; Meade, T.; Pomper, M.; Ptak, K.; Rao, J.; Singh, R.;Sridhar, S.; Stern, S.; Wang, A.; Weaver, J. B.; Woloschak, G.; Yang, L.Nano Today 2013, 8, 454−460.(24) Sun, S.; Zeng, H.; Robinson, D. B.; Raoux, S.; Rice, P. M.;Wang, S. X.; Li, G. J. Am. Chem. Soc. 2004, 126, 273−279.(25) Wang, W.; Wang, Y.; Tu, L.; Feng, Y.; Klein, T.; Wang, J. P. Sci.Rep. 2014, 4, 5716.(26) Lee, J. R.; Sato, N.; Bechstein, D. J.; Osterfeld, S. J.; Wang, J.;Gani, A. W.; Hall, D. A.; Wang, S. X. Sci. Rep. 2016, 6, 18692.(27) Park, J.; Joo, J.; Kwon, S. G.; Jang, Y.; Hyeon, T. Angew. Chem.,Int. Ed. 2007, 46, 4630−4660.(28) Baselt, D. R.; Lee, G. U.; Natesan, M.; Metzger, S. W.; Sheehan,P. E.; Colton, R. J. Biosens. Bioelectron. 1998, 13, 731−739.(29) Zuo, X.; Xiao, Y.; Plaxco, K. W. J. Am. Chem. Soc. 2009, 131,6944−6945.(30) Yakes, B. J.; Etheridge, S. M.; Mulvaney, S. P.; Tamanaha, C. R.Mar. Drugs 2010, 8, 565−576.(31) Wang, S. X.; Li, G. IEEE Trans. Magn. 2008, 44, 1687−1702.(32) Huestis, M. A.; Cone, E. J. J. Anal. Toxicol. 2004, 28, 394−399.(33) Van der Linden, T.; Wille, S. M.; Ramirez-Fernandez, M.;Verstraete, A. G.; Samyn, N. Forensic Sci. Int. 2015, 249, 148−155.(34) Laloup, M.; Del Mar Ramirez Fernandez, M.; Wood, M.; DeBoeck, G.; Maes, V.; Samyn, N. Forensic Sci. Int. 2006, 161, 175−179.(35) Milman, G.; Barnes, A. J.; Schwope, D. M.; Schwilke, E. W.;Darwin, W. D.; Goodwin, R. S.; Kelly, D. L.; Gorelick, D. A.; Huestis,M. A. Clin. Chem. 2010, 56, 1261−1269.(36) Baker, B. R.; Lai, R. Y.; Wood, M. S.; Doctor, E. H.; Heeger, A.J.; Plaxco, K. W. J. Am. Chem. Soc. 2006, 128, 3138−3139.(37) Wang, W. U.; Chen, C.; Lin, K. H.; Fang, Y.; Lieber, C. M. Proc.Natl. Acad. Sci. U. S. A. 2005, 102, 3208−3212.
Analytical Chemistry Letter
DOI: 10.1021/acs.analchem.6b01688Anal. Chem. 2016, 88, 7457−7461
7461