Embed Size (px)
Citation preview
좌심실 수축기능 평가 Cardiac Function
Seonghoon Choi
Cardiology
Hallym university
Basic Echo Review Course

LV systolic function
Systolic function 좌심실 수축 기능 - 심근의 수축으로 심실에서 혈액을 대동맥으로 박출하는
기능 실제 임상에서 LV function의 의미 ①Diagnosis – systolic (and diastolic) dysfunction,
etiology for symptoms ②Assessing response to treatment ③Assessing risk and prognosis – need for intervention
like as defibrillation, valve surgery, medicine, CRT etc. and timing of intervention
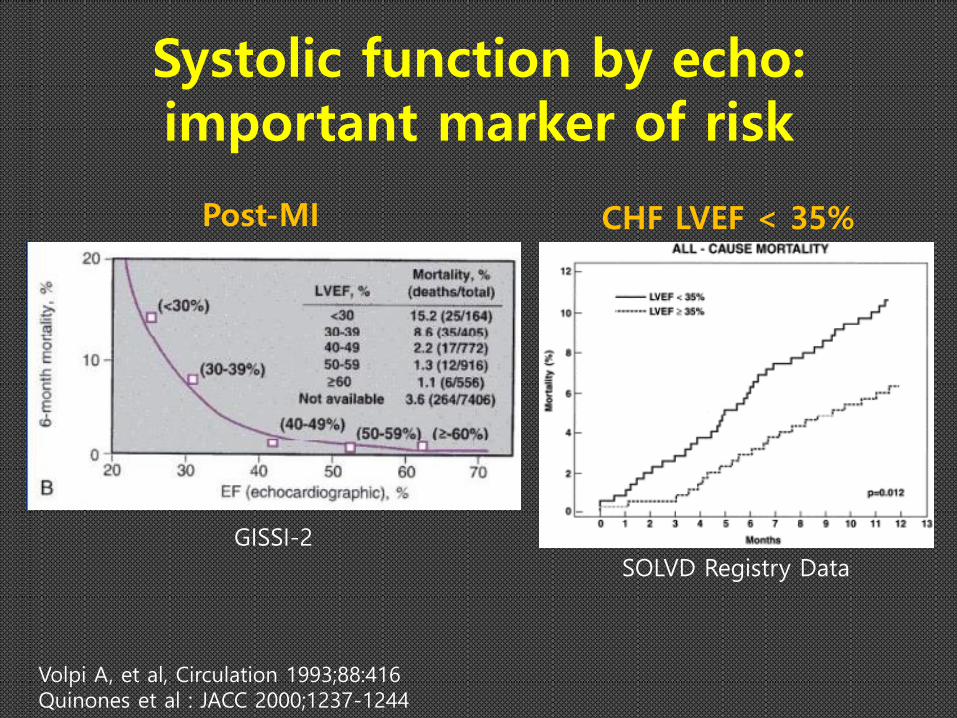
Systolic function by echo: important marker of risk
GISSI-2
Volpi A, et al, Circulation 1993;88:416 Quinones et al : JACC 2000;1237-1244
Post-MI CHF LVEF < 35%
SOLVD Registry Data
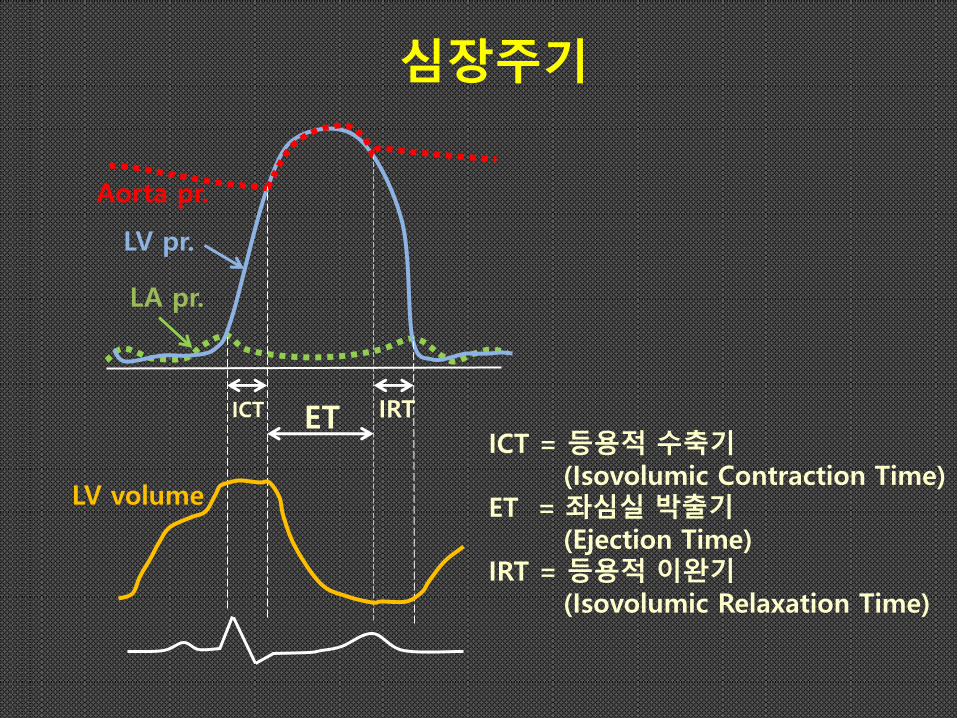
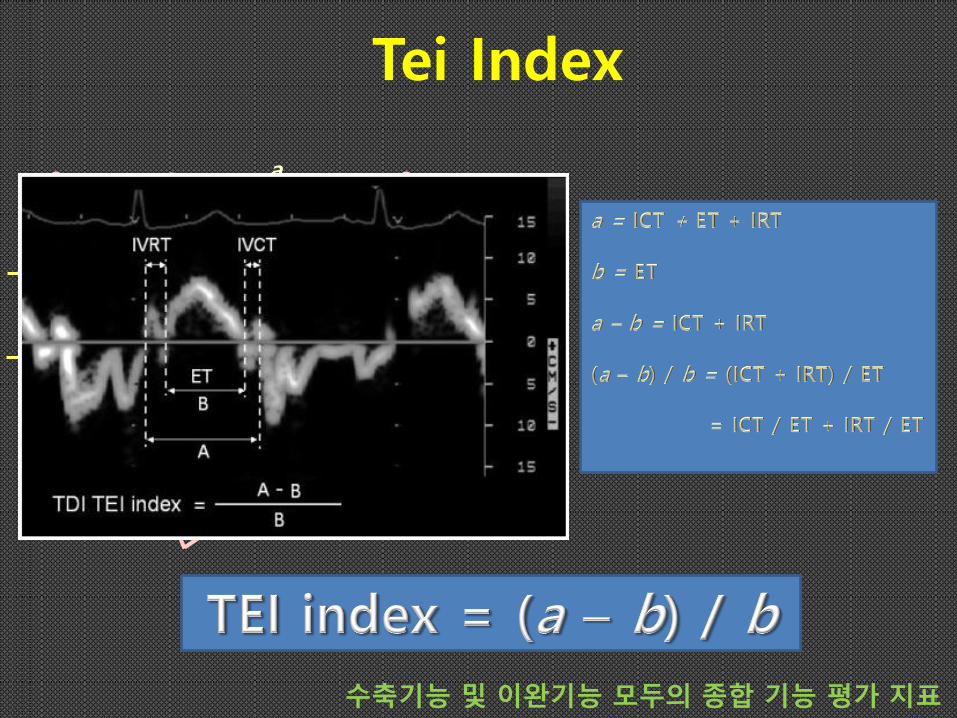
ET ICT IRT
LA pr.
Aorta pr.
LV pr.
LV volume
ICT = 등용적 수축기 (Isovolumic Contraction Time) ET = 좌심실 박출기 (Ejection Time) IRT = 등용적 이완기 (Isovolumic Relaxation Time)
심장주기
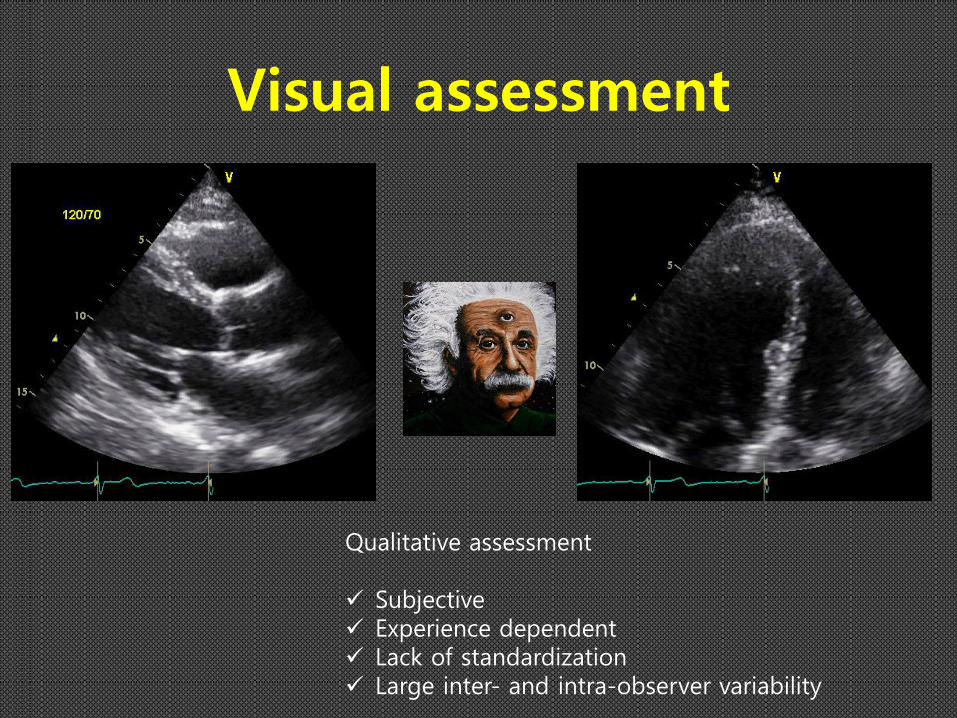
Visual assessment
Qualitative assessment Subjective Experience dependent Lack of standardization Large inter- and intra-observer variability
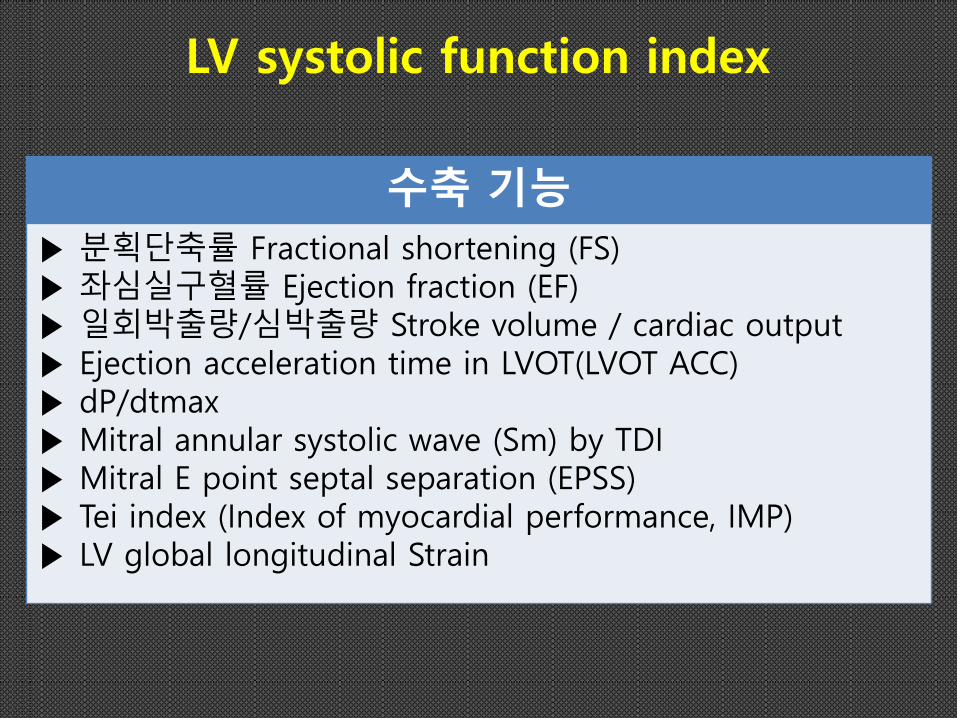
수축 기능
▶ 분획단축률 Fractional shortening (FS) ▶ 좌심실구혈률 Ejection fraction (EF) ▶ 일회박출량/심박출량 Stroke volume / cardiac output ▶ Ejection acceleration time in LVOT(LVOT ACC) ▶ dP/dtmax ▶ Mitral annular systolic wave (Sm) by TDI ▶ Mitral E point septal separation (EPSS) ▶ Tei index (Index of myocardial performance, IMP) ▶ LV global longitudinal Strain
LV systolic function index
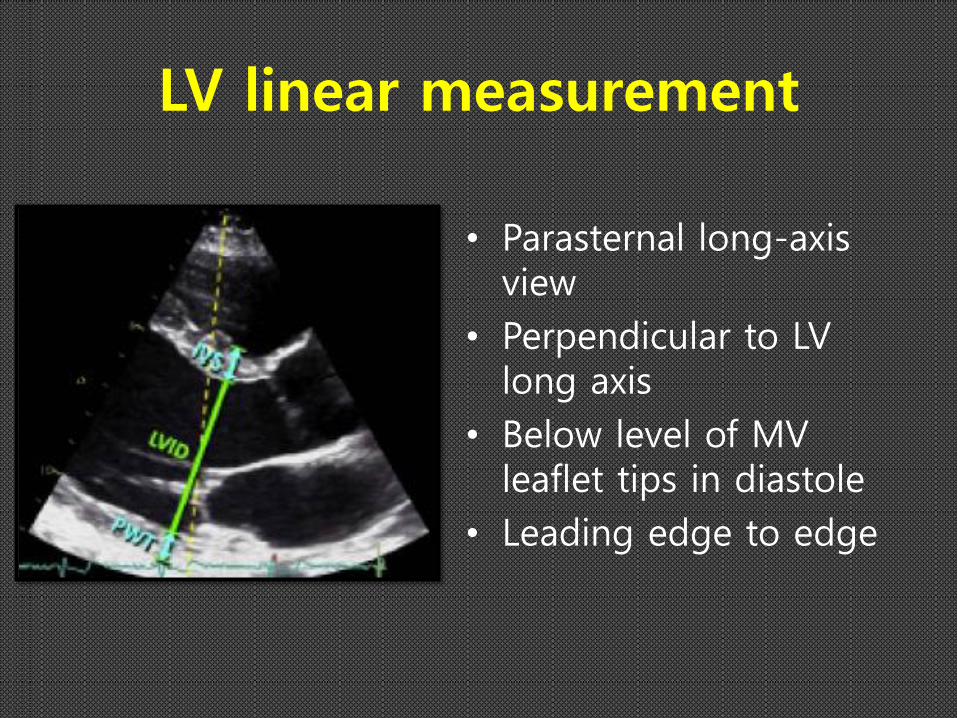
LV linear measurement
• Parasternal long-axis view
• Perpendicular to LV long axis
• Below level of MV leaflet tips in diastole
• Leading edge to edge
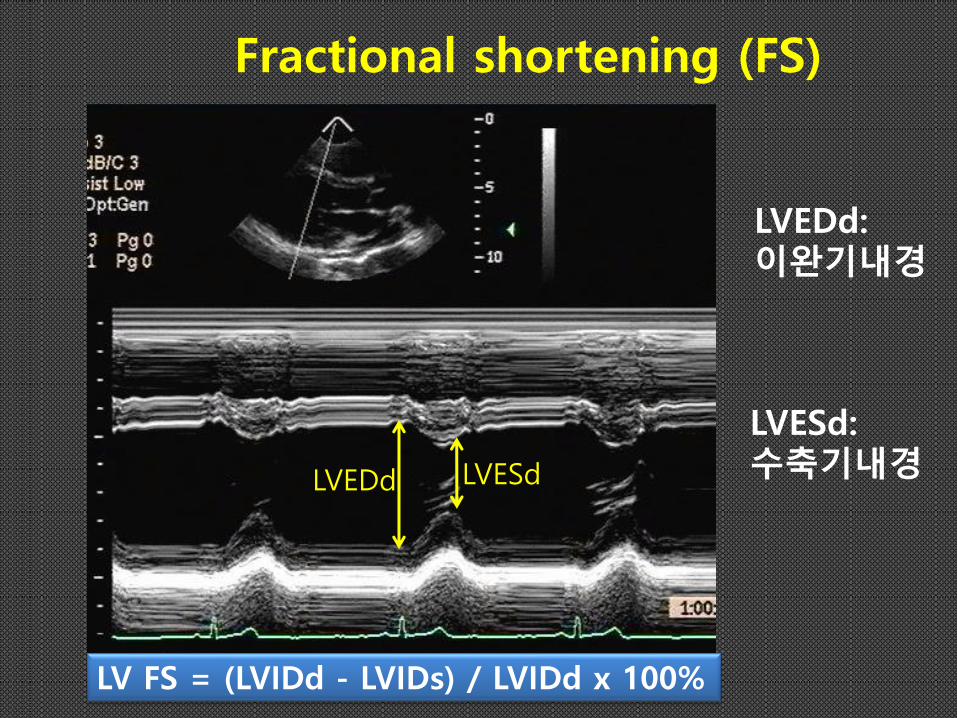
Fractional shortening (FS)
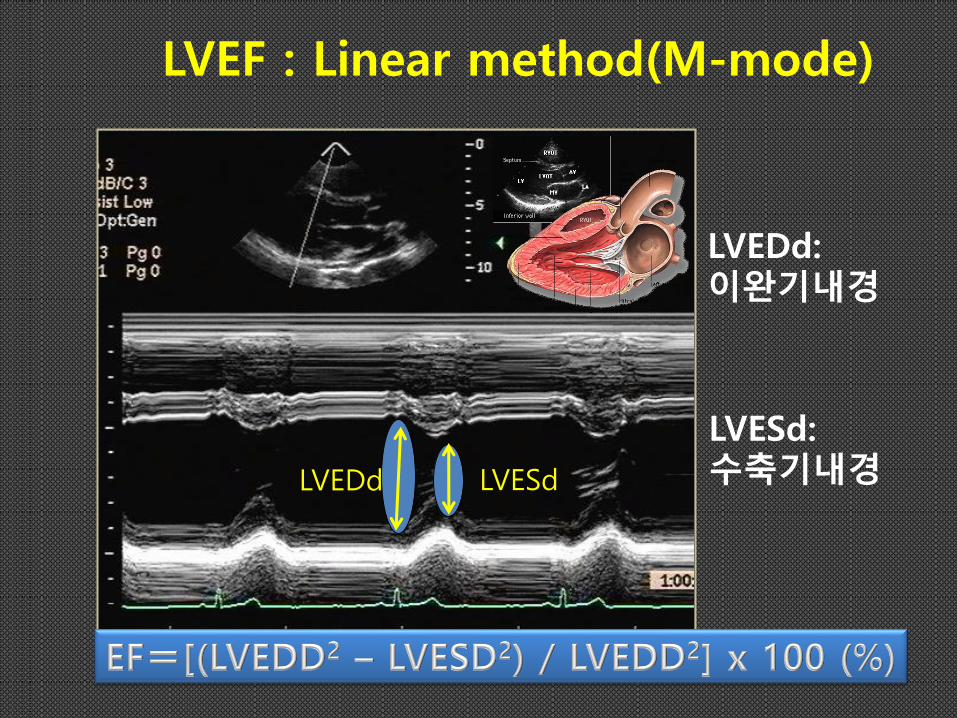
LVEDd: 이완기내경
LVEDd
LVESd: 수축기내경 LVESd
LV FS = (LVIDd - LVIDs) / LVIDd x 100%
Fractional shortening
• Normal >30% (25-45%)
• Severe LV dysfunction <15%
• Limitation
1. measures only transverse myocardial function,
2. describes the contractility of two walls only(infero-lateral and interventricular septum)
3. conclusions about overall LV function are made based on contractility of basal segments, that usually function properly (even in a significant LV systolic dysfunction)
4. completely useless when any regional wall motion abnormalities are present
5. inadequate M-mode cross-section (oblique orientation of the ultrasound beam with respect to the long axis of LV, incorrect cross-section level).
LV ejection fraction
• stroke volume as a percent of end-diastolic volume.
• LVEF = LVSV/LVEDV x 100% = (LVEDV - LVESV)/LVEDV x 100%
LVEDd: 이완기내경
LVEDd
LVESd: 수축기내경 LVESd
LVEF : Linear method(M-mode)
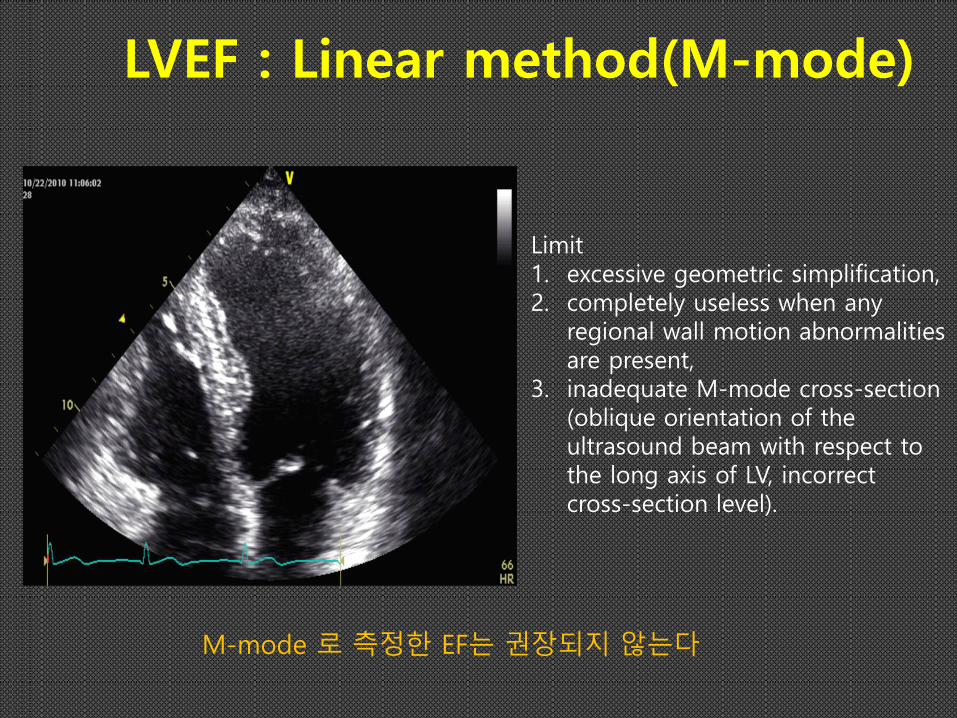
LVEF : Linear method(M-mode)
M-mode 로 측정한 EF는 권장되지 않는다
Limit 1. excessive geometric simplification, 2. completely useless when any
regional wall motion abnormalities are present,
3. inadequate M-mode cross-section (oblique orientation of the ultrasound beam with respect to the long axis of LV, incorrect cross-section level).
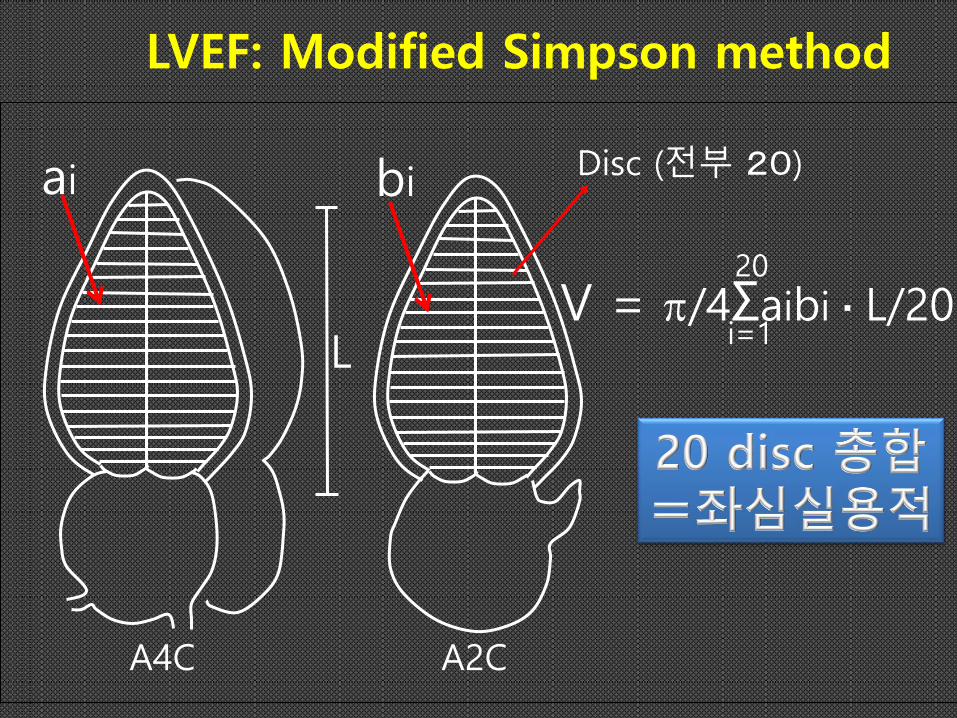
LVEF: Modified Simpson method
A4C A2C
V = /4Σaibi・L/20 20
i=1
Disc (전부 20)
ai
bi
L
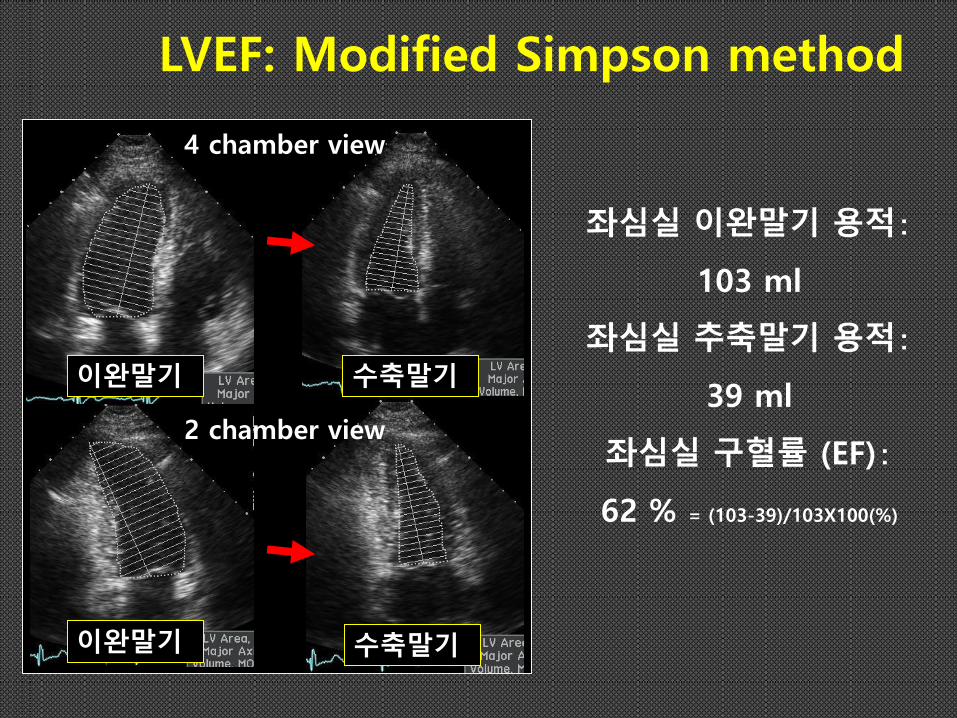
수축말기 이완말기
2 chamber view
좌심실 이완말기 용적:
103 ml
좌심실 추축말기 용적:
39 ml
좌심실 구혈률 (EF):
62 % = (103-39)/103X100(%)
수축말기 이완말기
4 chamber view
LVEF: Modified Simpson method
LVEF: Modified Simpson method
• Limit 1. Inadequate endocardial border definition, even
if optimal image quality (usually anterior and lateral endocardium are inadequately visualized),
2. Suboptimal image quality (especially when significant obesity or COPD are present),
3. Useless when excessive regional wall motion abnormalities or left ventricular geometric alterations are present (e.g. post-infarction aneurysm).
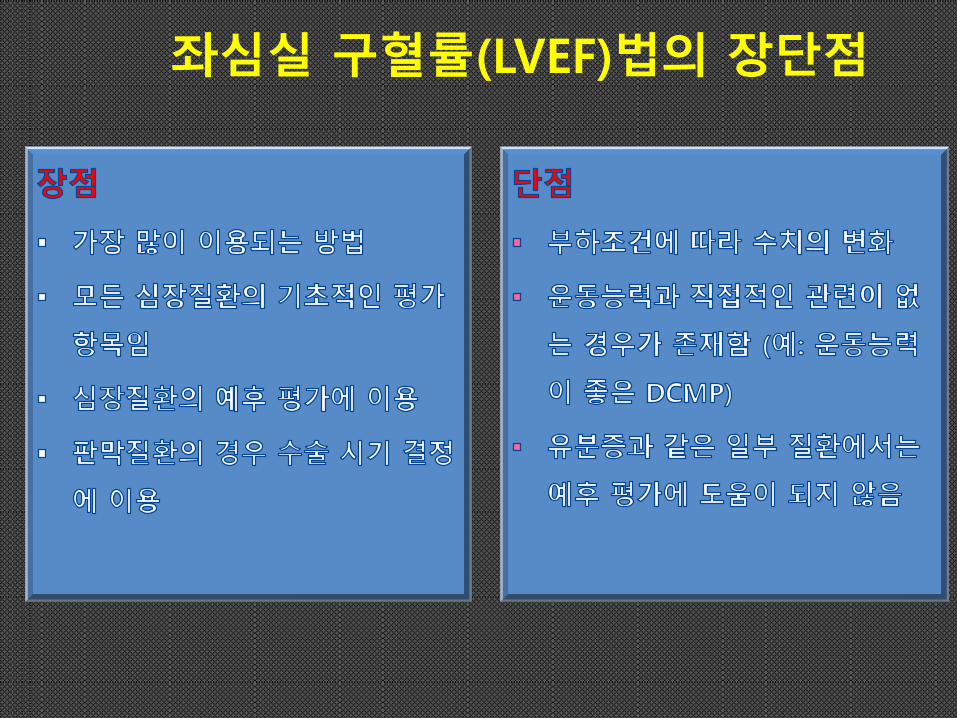
좌심실 구혈률(LVEF)법의 장단점
Potential problems with LVEF
• Load dependency • Measurement issues Measurement issues – Endocardial dropout : overestimation of volume – Foreshortening of the ventricle : underestimation of volume, less effect on EF – Geometric assumptions : influence EF measure when LV distorted – Regional dysfunction Regional dysfunction : over or under- represented with some methods – Paradoxical septal motion, other discoordinations of contraction Underestimation of EF – Heart rate effects Heart rate effects : tachycardia – reproducibility
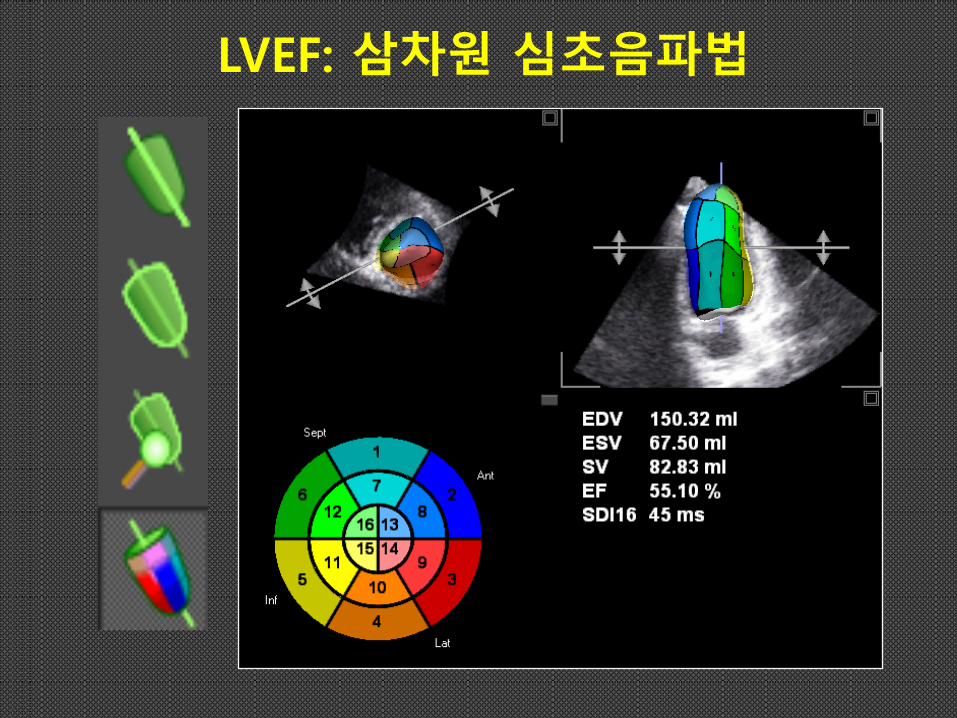
LVEF: 삼차원 심초음파법
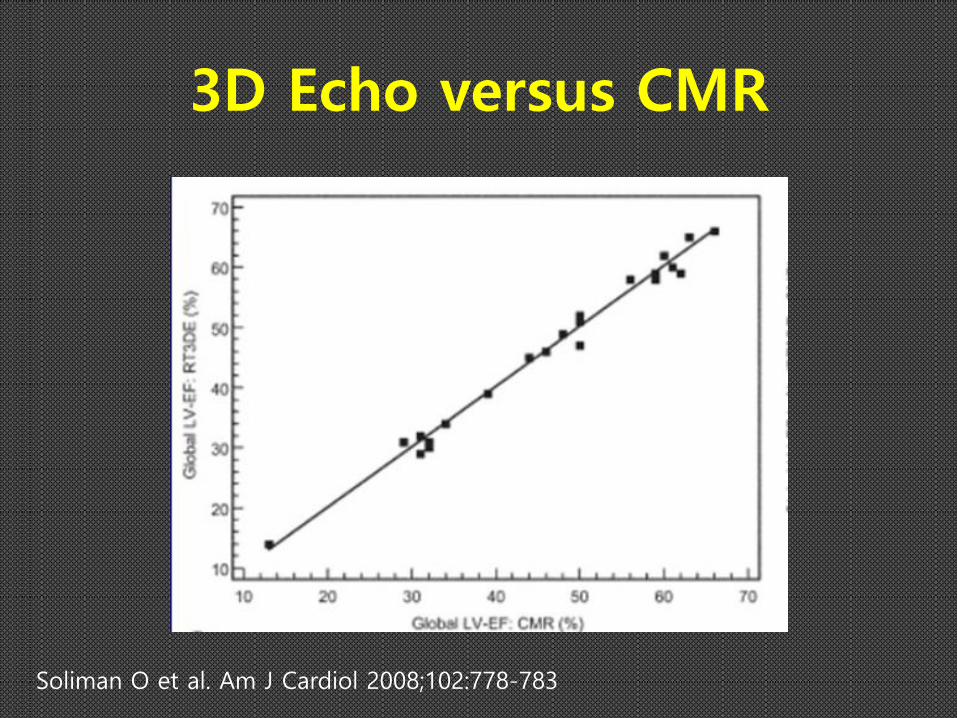
3D Echo versus CMR
Soliman O et al. Am J Cardiol 2008;102:778-783
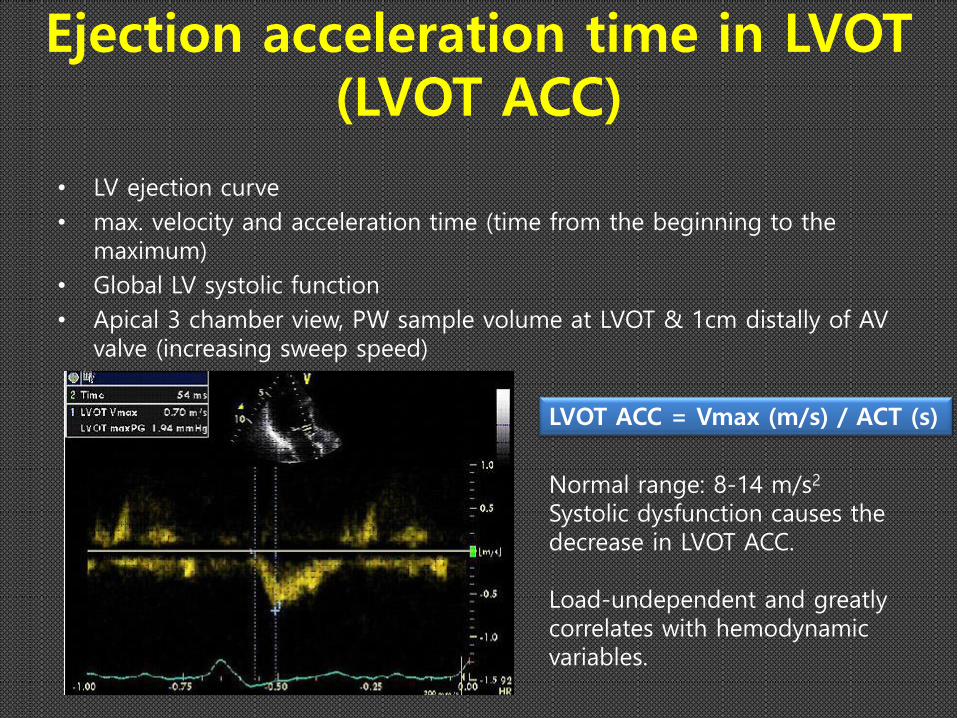
Ejection acceleration time in LVOT (LVOT ACC)
LVOT ACC = Vmax (m/s) / ACT (s)
Normal range: 8-14 m/s2 Systolic dysfunction causes the decrease in LVOT ACC. Load-undependent and greatly correlates with hemodynamic variables.
• LV ejection curve
• max. velocity and acceleration time (time from the beginning to the maximum)
• Global LV systolic function
• Apical 3 chamber view, PW sample volume at LVOT & 1cm distally of AV valve (increasing sweep speed)

Ejection acceleration time in LVOT (LVOT ACC)
Mitral_dP/dt
• Doppler mitral regurgitation (MR) curve
- Instantaneous pressure difference between LV and LA
in systole
• In LV systolic dysfunction,
LV pressure ↓falls / LA pressure ↑
Pressure difference ↓
Rate of increase in velocity of MR jet ↓
• Apical View, MR jet with CW
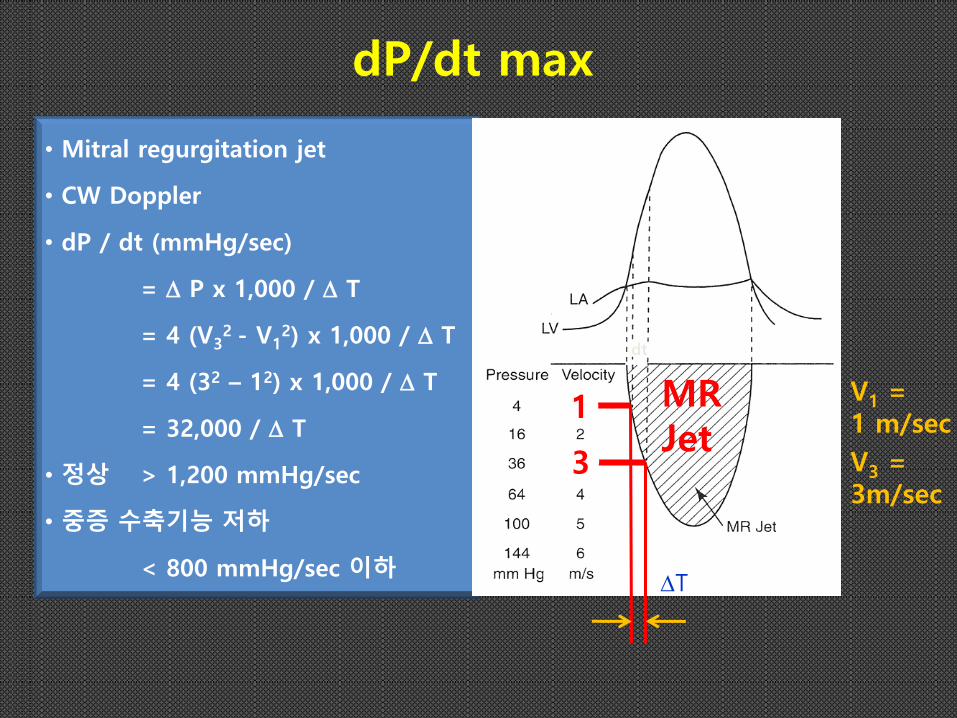
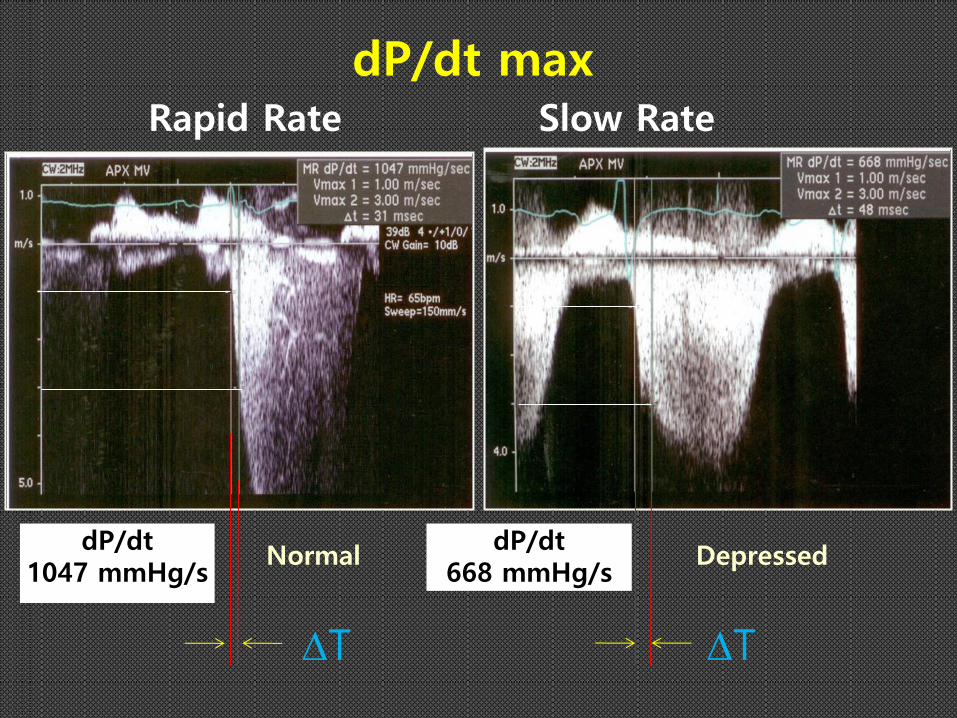
dP/dt max
• Mitral regurgitation jet
• CW Doppler
• dP / dt (mmHg/sec)
= P x 1,000 / T
= 4 (V32 - V1
2) x 1,000 / T
= 4 (32 – 12) x 1,000 / T
= 32,000 / T
• 정상 > 1,200 mmHg/sec
• 중증 수축기능 저하
< 800 mmHg/sec 이하
1
3
dt
T
MR Jet
V1 = 1 m/sec
V3 = 3m/sec
T
Rapid Rate Slow Rate
dP/dt 1047 mmHg/s
Normal Depressed
T
dP/dt 668 mmHg/s
dP/dt max
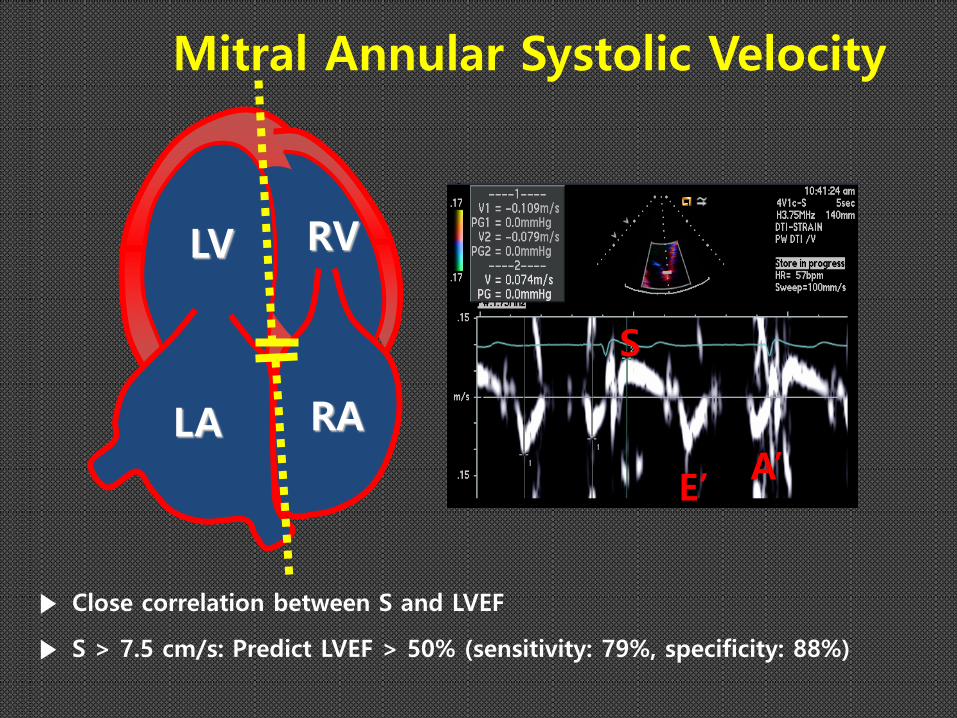
Mitral Annular Systolic Velocity
▶ Close correlation between S and LVEF
▶ S > 7.5 cm/s: Predict LVEF > 50% (sensitivity: 79%, specificity: 88%)
LV
LA RA
RV
S
E’ A’
a
b
등용적 수축기 ICT
등용적 이완기 IRT
수축기 ET
Tei Index
수축기능 및 이완기능 모두의 종합 기능 평가 지표

LV Global Longitudinal Longitudinal Strain
WNL Peak GKS in range of -20% Can be used in low flow AS, cardio-oncology, Valvular regurgitation

LV function in poor echo quality
• Contrast Echo • Non-endocardial border delineation method
- Iso-volumic indices
mitral-dP/dt
- Ejection phase indices
Tei index
FS(M-dode)
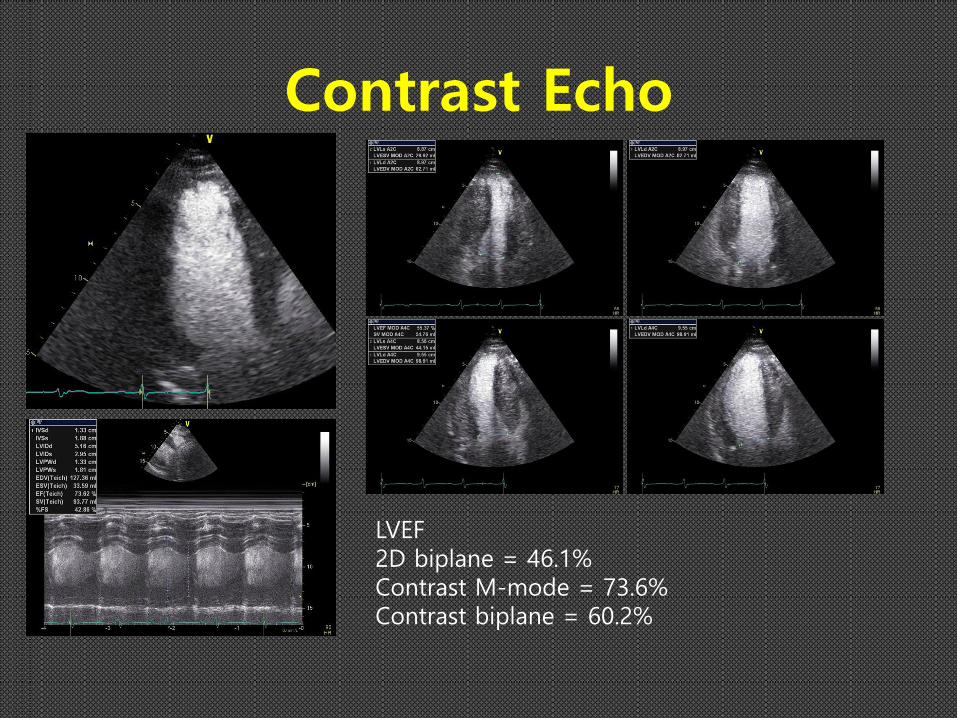
Contrast Echo
LVEF 2D biplane = 46.1% Contrast M-mode = 73.6% Contrast biplane = 60.2%
수축 기능
▶ 분획단축률 Fractional shortening (FS) ▶ 좌심실구혈률 Ejection fraction (EF) ▶ Ejection acceleration time in LVOT(LVOT ACC) ▶ dP/dtmax ▶ Mitral annular systolic wave (Sm) by TDI ▶ Mitral E point septal separation (EPSS) ▶ Tei index (Index of myocardial performance, IMP) ▶ LV global longitudinal Strain
LV systolic function index
Summary
• LV systolic function is single most important cardiac performance measurement.
• Quantitation of LVEF rather than qualitative evaluation like as 2D biplane Simpson method.
• Semi-quantitative global systolic measurement like as LVOT ACC, dP/dtmax, mitral annular systolic wave (Sm), Mitral E point septal separation (EPSS), Tei index, LV global longitudinal Strain.
• Use contrast in poor echo window.