Embed Size (px)
Citation preview

荆志成 , M.D; FCCP.上海市肺科医院同济大学医学院
肺动脉高压:肺动脉高压: 20102010 --
Pulmonary Arterial HypertensionPulmonary Arterial Hypertension

Patho-Anatomy of AMI

In 1891, the German pathologist Romberg observed that the heart of an individual,
suffering from a stricture of the pulmonary arteries due to severe sclerosis, was double
the size of a man´s fist.He again named this disease sclerosis of the
pulmonary arteries.


危险因素(芬氟拉明… )
遗传易感性(BMPR2, ALK-1, endoglin,
5-HTT...)
血管损伤
内皮细胞功能紊乱(NO, PgI2, ET-1, vWF…)
平滑肌细胞功能紊乱(Kv1.5 …)
炎症因子(IL-1, IL-6,
MIP-1, RANTES, fractalkine)
肺动脉高压
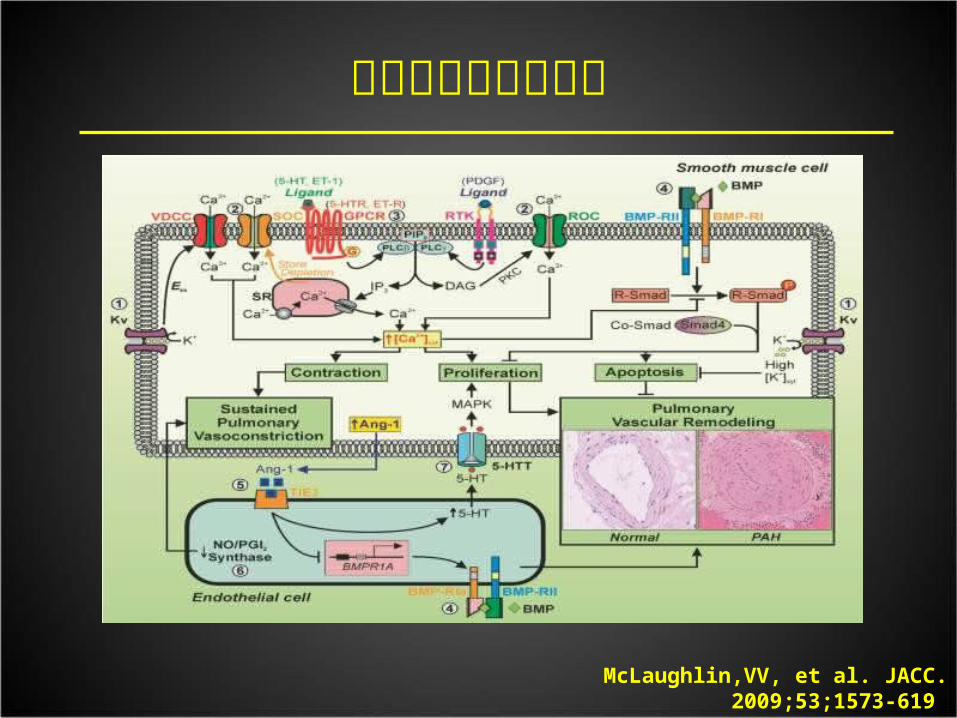
肺动脉高压发病机理
McLaughlin,VV, et al. JACC. 2009;53;1573-619

1. 肺动脉高压
特发性肺动脉高压 遗传性 BMPR2 ALK1, endoglin 未知突变 药物或毒物 相关性 结缔组织病 心脏或大血管左向右分流 门脉高压 HIV 感染 血吸虫病 慢性溶血性贫血1′肺静脉闭塞病,肺毛细血管瘤样病
2. 左心疾病相关肺高血压 收缩功能障碍 舒张功能障碍 瓣膜病
COPD 间质性肺病 其他混合性通气功能或限制性通气功能障碍 呼吸睡眠暂停 慢性高原病 发育异常
4. 慢性血栓栓塞性肺高血压
5. 原因不明的或多因素肺高血压
肺高血压临床分类 (updated 4rd WHO-Danapoint 2008)
血液学异常 :骨髓异常增生,脾切除 系统性异常 : 血管炎 , 结节病 , 肺朗格罕氏细胞 增多症 , 多发性神经纤维瘤病 代谢异常 : 糖原累积病 , 高雪氏病 , 甲状腺异常 其他 : 肿瘤阻塞 , 纤维纵隔炎 , 肾衰或透析 ,
3. 慢性肺病或缺氧性疾病相关肺高血压
What we have done? - Concepts of PH
• PH - pulmonary hypertension 肺高血压症• PAH - pulmonary arterial hypertension 肺动脉高压• IPAH - Idiopathic PAH 特发性肺动脉高压• PVH - pulmonary venous hypertension 肺静脉高压• In China : most patients with PH were
still wrongly called PAH

Could not diagnosis early
Poor Prognosis
Expensive cost
Current Status of PAH in China
No standardized treatments

What we have done?- Prevalence
• The lowest estimates of the prevalence of PAH and IPAH are 15 cases and 5.9 cases/million adult population.
• The lowest estimate of PAH incidence is 2.4 cases/million
adult population/year.
• Still no prevalence data in China• The awareness is poor in public, in
physicians and in government• No support from Government can be
available to the patients

The 1st registry study of PAH in China
Z-C JING et al. Chest.2007;132:373-379

What we have done?- registry study
country Number of
patients enrolled
Etiology Medial Survival(years)
Survival
1 year
2 year
3 year
5 year
NIH-1989 187 PPH 2.8 68% 48% 34%
USA-2006
576 WHO IPAH
3.6 84% 67% 58%
France 674 WHO IPAH
89%
Japan 223 PPH 2.8
Mexico 66 IPAH 4.0
Indian 61 PPH 1.8 48% 32%
China 76 IPAH 2.4 68% 57% 39% 21%

What we have done? - acute vasoreactivity test
• Long-term response to CCBs in IPAH should be identified by acute vasoreactivity test
• But, in fact…
IPAH
CHD-PAH
CTD-PAH
FPAH
anorexigen PAH
others
PoPAH
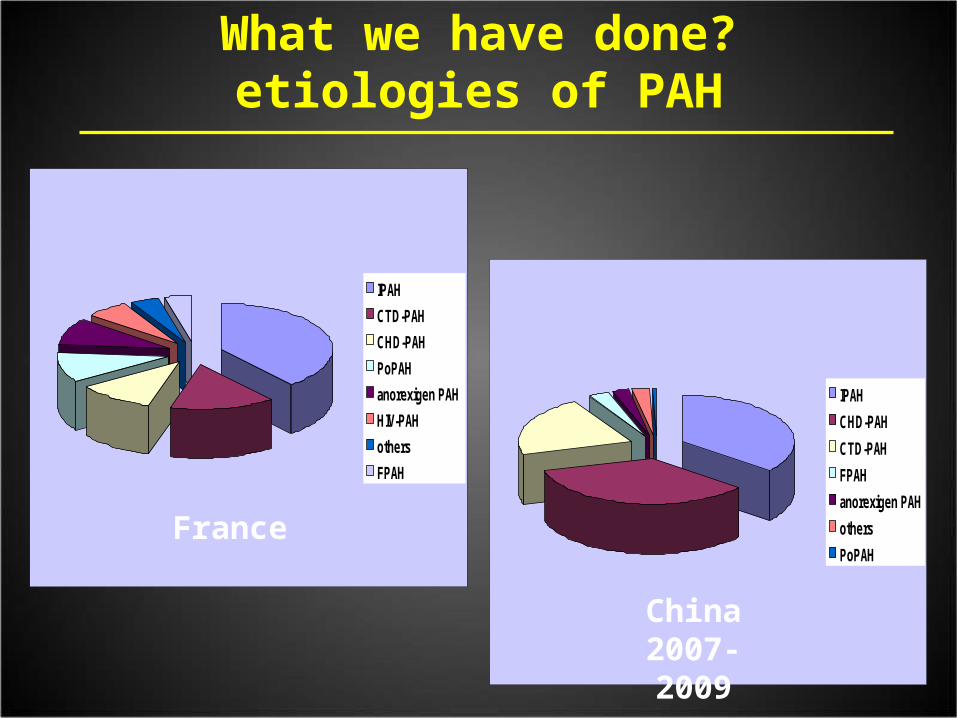
What we have done?etiologies of PAH
China 2007-2009
IPAH
CTD-PAH
CHD-PAH
PoPAH
anorexigen PAH
HIV-PAH
others
FPAH
France

IPAH
(n=173)
CHD-PAH
(n=165)
CTD-PAH
(n=103)
Age (years) 33 ± 15 27 ± 13 41 ± 14
Female (n%) 121 (69.9) 102 (61.8) 88 (85.4)
Time of symptom onset to diagnosis (years)
3.4 ± 4.3 7.9 ± 9.2 3.0 ± 3.2
WHO functional classification
Class andⅠ Ⅱ 83 (48.0) 100 (60.6) 41 (39.8)
Class and Ⅲ Ⅳ 90 (52.0) 65 (39.4) 62 (60.2)
6MWD (m) 394 ± 114 433 ± 105 384 ±107
Demographic characteristics in our center from 2007-2009
Unpublished data of Shanghai Pulmonary hospital

Adult congenital heart disease and idiopathic pulmonary artery hypertension like physiology
• Small defect with PAH• Virus infection during pregnancy• Pulmonary vascular pathology was onset to
intervene with the outcome of cardiovascular development
Dana point meeting, THE NEW DIAGNOSIS: IPAH LIKE PHYSIOLOGY

What we have done? - Definition for PAH
mPAP ≥ 25 mm Hg
PCWP ≤15 mm Hg assessed by RHC
PVR > 3 Wood U
However, only few centers like to use RHC as diagnostic
measure for PAH
Echo was still the most popular way to confirm PAH in
China up to now
But more and more centers initiated standard RHC
procedure and pulmonary vasoreactivity testing after 2006

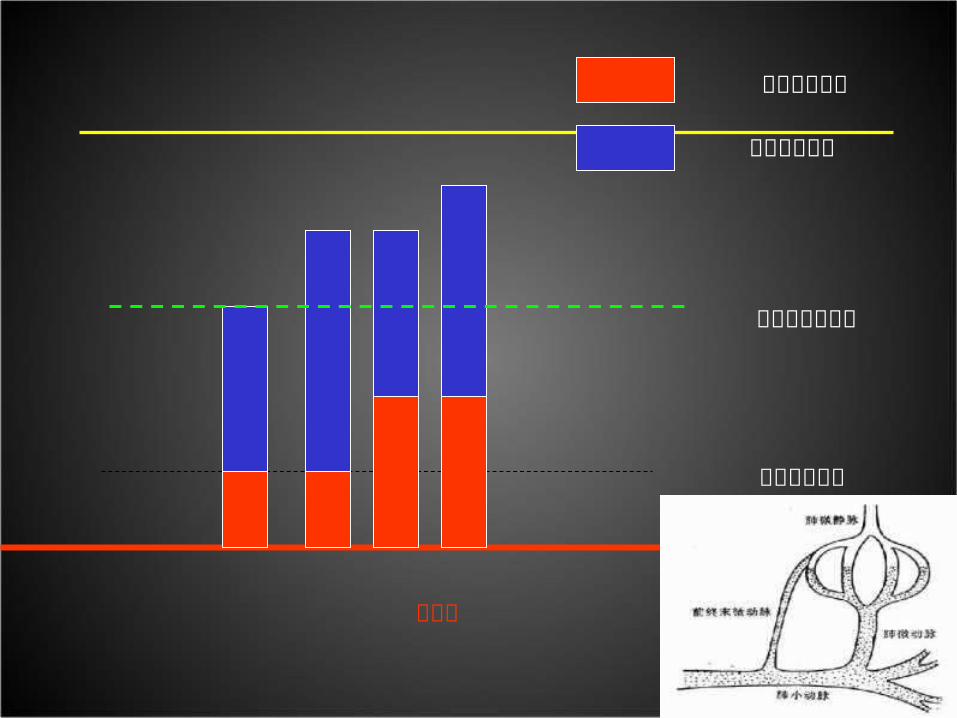
左心房
毛细血管后压
毛细血管前压
毛细血管水平
正常肺动脉压力

肺高压的血流动力学定义肺高压的血流动力学定义
定义定义 特征特征 临床分组临床分组
肺高压肺高压 平均肺动脉压≥ 25mmHg
所有
毛细血管毛细血管前肺高压前肺高压
1. 平均肺动脉压≥ 25mmHg
2. 肺毛细血管楔压≤ 15mmHg
1 、肺动脉高压3 、肺病相关性肺高压4 、慢性血栓栓塞性肺高压5 、不明原因肺高压
毛细血管毛细血管后肺高压后肺高压
被动型被动型
反应型反应型
1. 平均肺动脉压≥ 25mmHg
2. 肺毛细血管楔压> 15mmHg ,心排量下降,或正常
2 左心疾病相关性肺高压
跨肺压≤ 12mmHg
跨肺压 > 12 mmHg

ECHO SCREEN


What we have done? - RHC
Firstly perform RHC through antebranchial vein in China
Data from the Cathé Lab of Shanghai Pulmonary Hospital

Edwards Swan-Ganz Cath

Rubin LJ and Badesch DB: Ann Intern Med 2005; 143: 282-92.
Durg testing must be done in the 1st evaluation
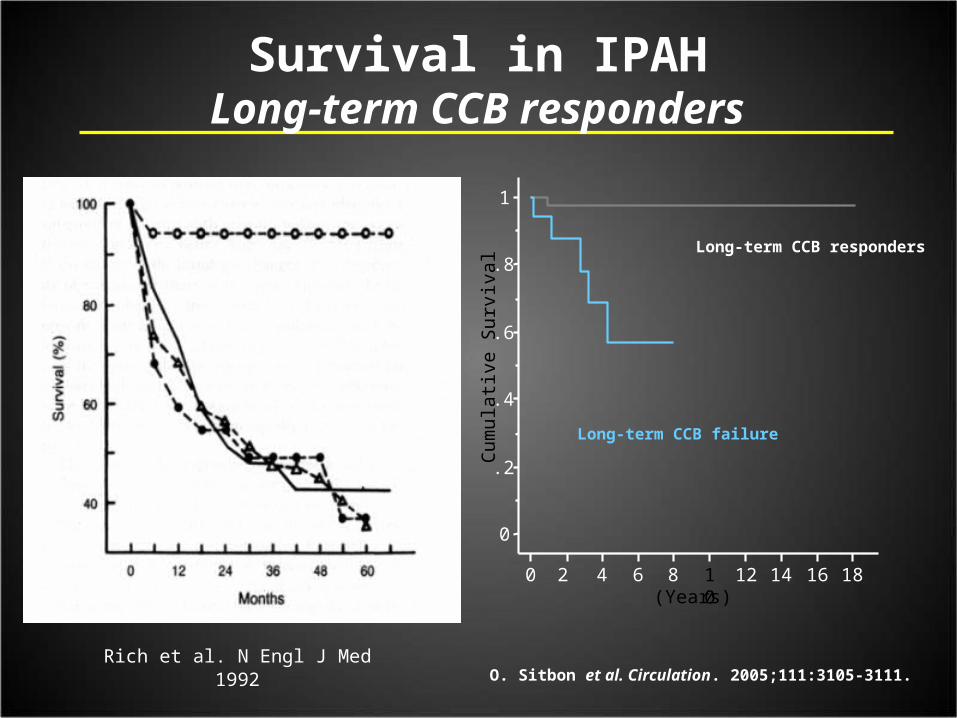
(Years)
Long-term CCB responders
Long-term CCB failureCum
ula
tive
Su
rviv
al
0
.2
.4
.6
.8
1
0 2 4 6 8 10
12 14 16 18
Survival in IPAHLong-term CCB responders
Rich et al. N Engl J Med 1992O. Sitbon et al. Circulation. 2005;111:3105-3111.

• Responders to CCBs versus Prinzmental’s Variant Angina: Spasm of artery, younger, better survival, calcium antagonists are useful
• Non-responder to CCBs versus angina secondary to Coronary atherosclerosis: more complex artery remodeling
Different vascular disease, attacked the same target organ: pulmonary artery and right ventricular
Should we classify IPAH into 2 subgroups?
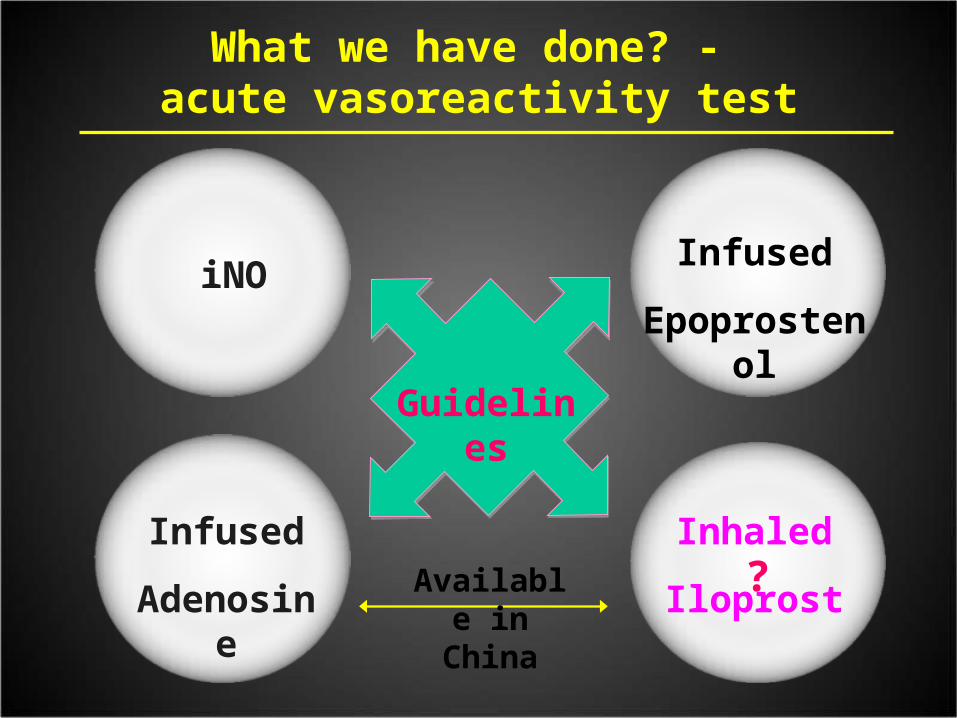
What we have done? - acute vasoreactivity test
Infused
Epoprostenol
Guidelines
iNO
Infused
Adenosine
Inhaled
Iloprost?Available
in China
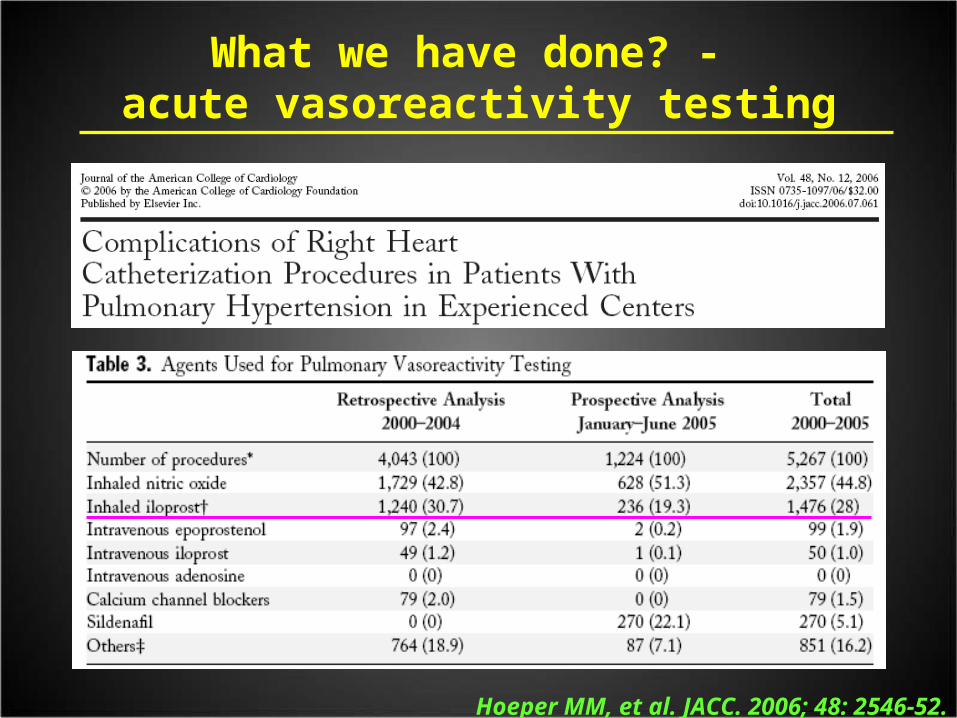
What we have done? - acute vasoreactivity testing
Hoeper MM, et al. JACC. 2006; 48: 2546-52.

What we have done? - acute vasoreactivity test
Opitz CF, et al. Eur Respir J. 2009; 33: 1247–9.
What we have done? - acute vasoreactivity test
The first study to prospectively address this question in a sizable group of IPAH patients is published by JING et al. in this issue of the ERJ.
Z-C JING, et al. Eur Respir J. 2009; 33: 1354–60.

Acute responder to Iloprost
PAP 92/34/59 mm HgPAP 36/11/20 mm Hg
CO 3.53 L/minCO 2.94 L/min
data of Shanghai Pulmonary hospital

What we have done? - acute vasoreactivity test
What we have done ? – pulmonary angiography
• Pulmonary angiography is very important to diagnostic use in PH, especially for CTEPH
• But, doctors in China seldom underwent this procedure just because the severely elevated pulmonary arterial pressure

What we have done ? – pulmonary angiography
Hemodynamic changes after pulmonary angiography in PAH (N=157)
Before After Changes P
HR, bpm 85 ± 15 86 ± 15 1.3 0.002
mSBP, mm Hg 87 ± 14 86 ± 13 -0.9 0.114
sPAP, mm Hg 90 ± 30 97 ± 31 7.3 <0.001
mPAP, mm Hg 53 ± 20 58 ± 21 4.5 <0.001
dPAP, mm Hg 33 ± 18 36 ± 18 2.5 <0.001
Unpublished data of Shanghai Pulmonary hospital
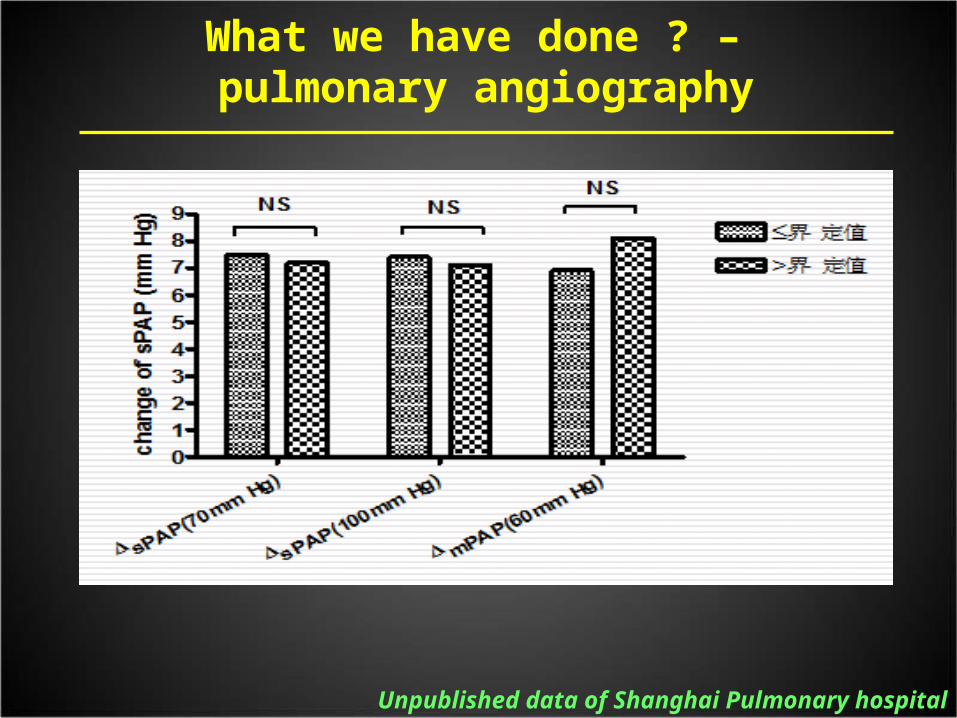
What we have done ? – pulmonary angiography
Unpublished data of Shanghai Pulmonary hospital

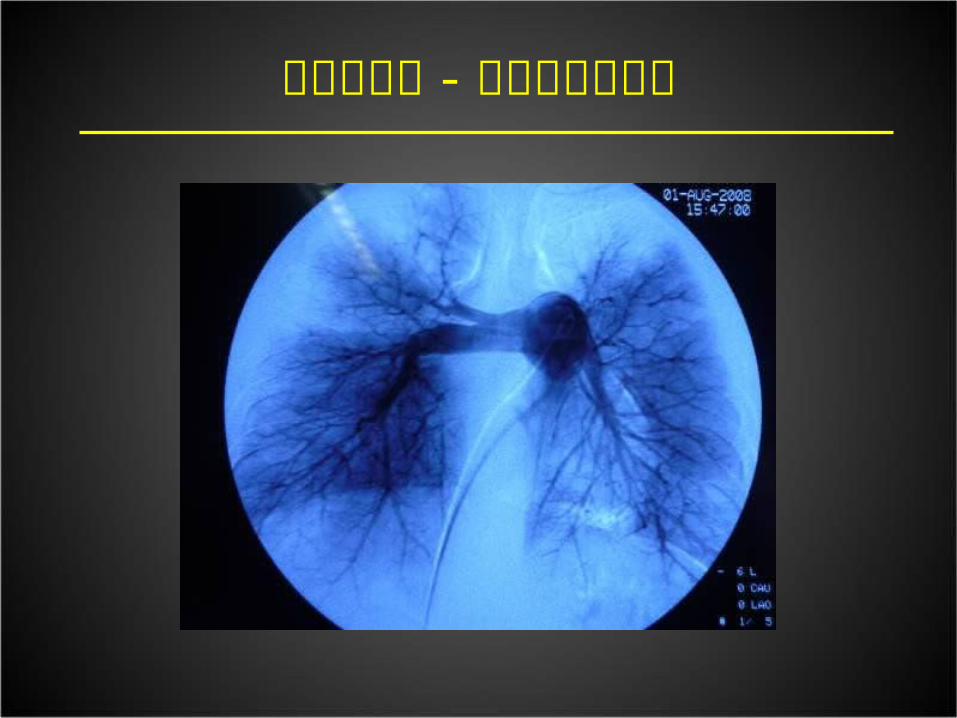
What we have done ? – pulmonary angiography

肺动脉造影 -CTEPH

肺动脉造影 - 肺血管炎
肺动脉造影 - 肺动脉发育不良

PE OR TUMOR : CATHETERIZE BIOPSY
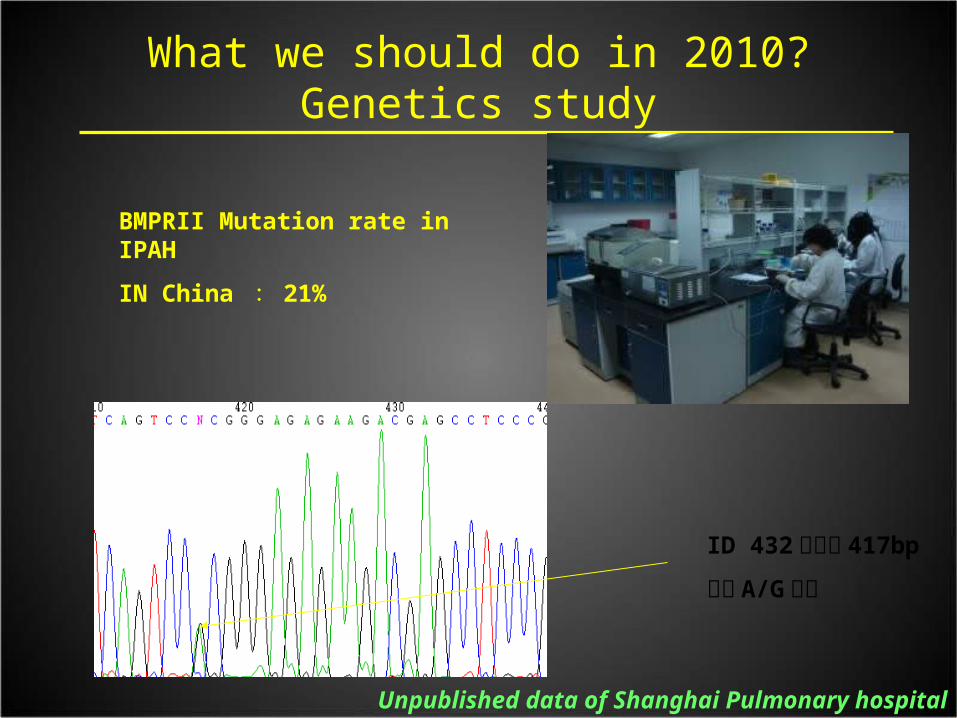
ID 432号患者 417bp
位置 A/G杂合
What we should do in 2010?Genetics study
Unpublished data of Shanghai Pulmonary hospital
BMPRII Mutation rate in IPAH
IN China : 21%


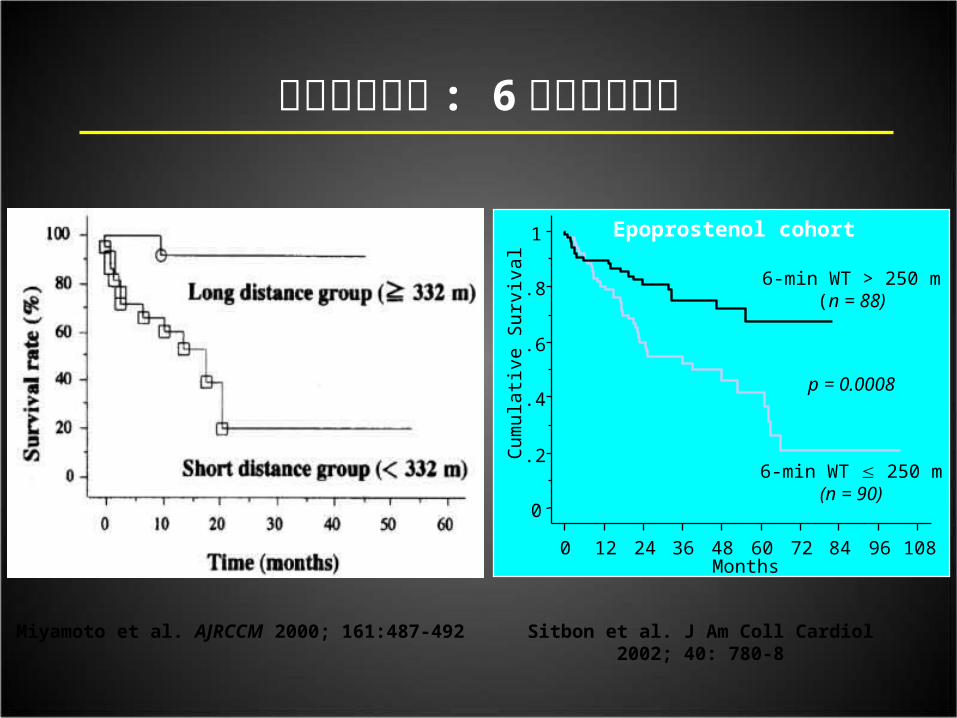
运动能力评估 : 6分钟步行距离
Miyamoto et al. AJRCCM 2000; 161:487-492
Cum
ula
tive
Su
rviv
al
Months
p = 0.0008
6-min WT > 250 m(n = 88)
6-min WT 250 m(n = 90)
0
.2
.4
.6
.8
1
0 12 24 36 48 60 72 84 96 108
Sitbon et al. J Am Coll Cardiol 2002; 40: 780-8
Epoprostenol cohort

Nagaya N, et al. Am J Respir Crit Care Med 1999; 160:478-92
Control(n = 30)
NYHA II(n = 5)
NYHA III(n = 72)
NYHA IV(n = 13)
Ser
um
uri
c ac
id le
vels
(m
g/d
l)
*
0
2
4
6
8
10
12
Ser
um
uri
c ac
id l
evel
s (m
g/d
l)
+
*
0
2
4
6
8
10
12
ASSESSMENT OF PAH SEVERITYURIC ACID
Su
rviv
al (
%)
Time (years)
6.49 mg/dl
< 6.4 mg/dl(median)

Nagaya N, et al. Circulation 2000; 102:865-70.
Baseline BNP Follow-up BNP
100
80
60
40
20
0
0 12 24 36 48
BNP < 150 pg/ml
BNP 150 pg/ml
Time (months)
Su
rviv
al r
ate
(%) 100
80
60
40
20
0
0 12 24 36 48
BNP < 180 pg/ml
BNP 180 pg/ml
Time (months)
ASSESSMENT OF PAH SEVERITYNATRIURETIC PEPTIDES

Torbicki A, et al. Circulation 2003
ASSESSMENT OF PAH SEVERITYTROPONIN T
What we have done? – treatments
• Up to now, only two PAH-specific drugs have been marketed in China
Bosentan Iloprost
• Other off-label PAH-specific drugs PDE-5: Sildenafil, Vardenafil Prostanoids: Beraprost
Both more than 10,000 € annually
1,500-2,000 € annually


Z-C Jing, et al. J Heart Lung Transplant. 2010; 29:150-6

P=0.03
X-Q XU, Z-C JING, et al. Hypertension Research. 2009;32:911-5

No patients dead during obversational period
Z-C JING, et al. HEART.2009;95:1531-6
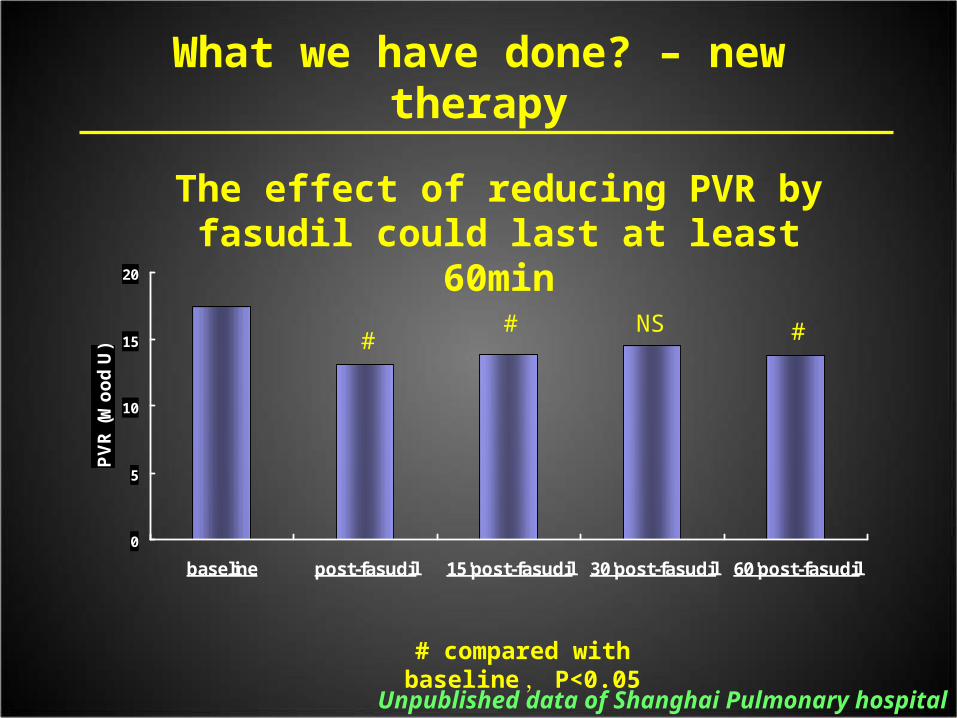
What we have done? – new therapy
0
5
10
15
20
baseline post-fasudil 15'post-fasudil 30'post-fasudil 60'post-fasudil
PV
R (
Wo
od
U) #
# #
The effect of reducing PVR by fasudil could last at least 60min
NS
# compared with baseline , P<0.05
Unpublished data of Shanghai Pulmonary hospital

What we have done? – treatments
IPAH
(n=235)
CHD-PAH
(n=195)
CTD-PAH
(n=123)
Target therapy, n
Bosentan 30 37 31
Iloprost 6 18 1
Sidenafil 52 55 43
Vardenafil 58 55 32 Combined 91 25 16
Traditional therapy, n
Digoxin 75 51 39
Diuretic 99 93 60
Statin 64 65 37
Anticoagulant 50 40 35
Unpublished data of Shanghai Pulmonary hospital
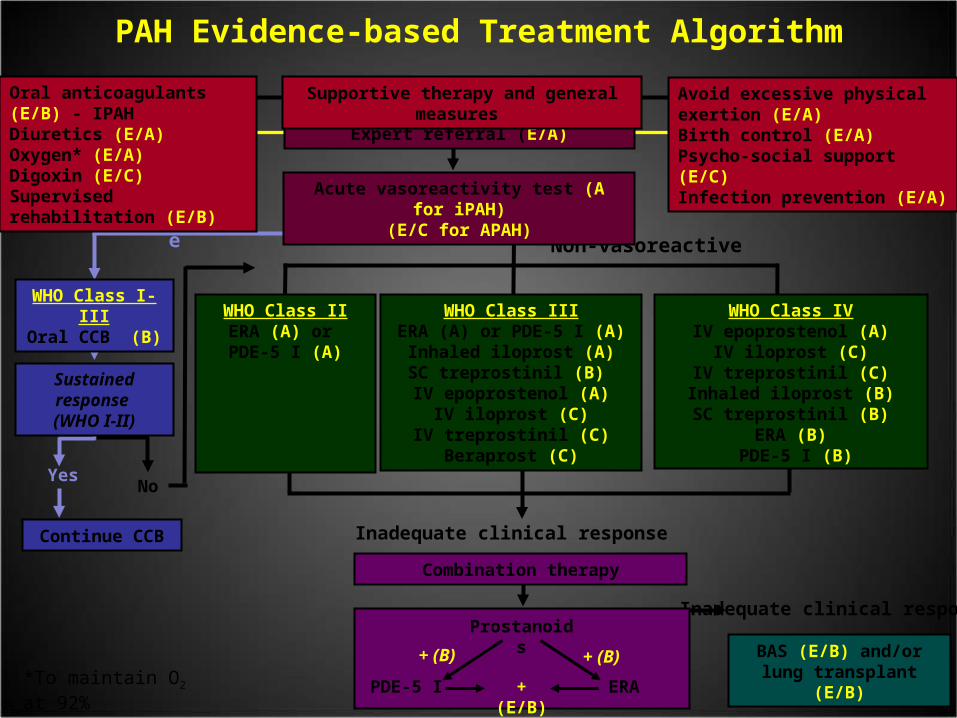
BAS (E/B) and/orlung transplant (E/B)
Inadequate clinical response
Combination therapy
PDE-5 I
Prostanoids
ERA + (E/B)
+ (B)+ (B)
Inadequate clinical responseContinue CCB
Yes
Vasoreactive
WHO Class I-IIIOral CCB (B)
Sustained response (WHO I-II)
WHO Class IIIERA (A) or PDE-5 I (A)
Inhaled iloprost (A)SC treprostinil (B) IV epoprostenol (A)
IV iloprost (C)IV treprostinil (C)
Beraprost (C)
WHO Class IVIV epoprostenol (A)
IV iloprost (C)IV treprostinil (C)
Inhaled iloprost (B)SC treprostinil (B)
ERA (B) PDE-5 I (B)
WHO Class IIERA (A) or PDE-5 I (A)
Non-vasoreactive
No
PAH Evidence-based Treatment Algorithm
Acute vasoreactivity test (A for iPAH)(E/C for APAH)
Expert referral (E/A)
Supportive therapy and general measures Avoid excessive physical exertion (E/A)Birth control (E/A)Psycho-social support (E/C)Infection prevention (E/A)
Oral anticoagulants (E/B) - IPAHDiuretics (E/A)Oxygen* (E/A)Digoxin (E/C)Supervised rehabilitation (E/B)
*To maintain O2 at 92%

Survival data for PAH patients in China-from 2006-2009
The data was from Shanghai Pulmonary Hospital, Tongji University
--- CDHPAH--- IPAH--- CTDPAH

Survival data for IPAH in China
Survival data in different
ears for IPAH1 year 2 year 3 year
Without PAH-targeted therapies - before 2006
68% 57% 39%
With adequate bosentan therapies - USA
96% 89% 86%
With adequate targeted therapies - China after 2007
92% 81% 75%
Zhi-Cheng JING, et al. CHEST 2007; 132: 373-9.Mc Laughlin, et al. Eur Resp J 2005; 25: 244-9.

< 30% (4.3%)
> 100% (40.9%)
50~100 % (40.5%)
30~50 % (14.3%)
Proportion of treatment cost and family income / per year of PAH patients in China
What have we done? – economic burden
Unpublished data of Shanghai Pulmonary hospital
More Clinical Trials will be available for our patients
• Sildenafil: 1mg, 5mg or 10mg• Vardenafil: EVALUATION• Seraphin: Macitentan• Sitaxsentan• Bosentan Phase IV• Iptakalim Phase II-III• CHEST• PATENT• Greephin• …
• Not only apply a opportunity to patients who could receive therapies freely, but also a really good chance to learn evaluated and diagnostic strategy from those trials to Chinese doctors.

WHO FC ⅠⅡ
WHO FC ⅢⅣ
WHO FC and Ⅰ ⅡWHO FC and Ⅲ
Ⅳ
1 year 99.1% 86.3%
2 year 97.2% 70.7%
3 year 94.8% 67.3%
What we should do in 2010?Earlier detection should be important
Unpublished data of Shanghai Pulmonary hospital

What we should do in 2010?Thrombolysis therapy can move out the risk of chronic pulmonary hypertension
Unpublished data of Shanghai Pulmonary hospital

What we should do in 2010?Interventional therapy for CTEPH cases
术前 PAP
95/23/52 mm Hg
术后 PAP
73/19/39 mm Hg
2010年 4月 23日完成于上海市肺科医院导管室

What we should do in 2010?New drug therapy for Eisenmenger Physiology
• Sildenafil• Beroprost• Bosentan• Iloprost• Fasudil• Ambrisentan• Combination therapy
This is challenge condition in developing countries, although We need more evidence on the drug therapy for Eisenmenger physiology, maybe we can take a choice to screen some cases that could be cured!

全国肺动脉高压筛查诊断治疗专家共识2007 年 7 月 28 日 ( 中华心血管病杂志, 2007 年 11月)
What we should do in 2010?Update our expert consensus on Pulmonary hypertension

Right heart remodeling and ischemia
• Right coronary artery flow will be decreased or stopped during the systol-period
• PA-RV-LV interaction
NF. Voelkel, et al. Circulation, 2006; 114: 1883.HC. Champion, et al. Circulation, 2009; 120:992.

What we should do in 2010?The Burden of Pulmonary Hypertension
The Burden of Pulmonary Hypertensionin China-The Qinghai-Tibet plateau

What we should do in 2010?The patients’ education and club

What we should do in 2010?Pulmonary hypertension Journal in China

What we should do in 2010? To update our therapeutic strategies
• Exciting progresses have achieved, but not enough
• To push more doctors to know bosentan: not only vasodilator, but also reversing vascular remodeling and decrease RV hypertrophy
• New agents development : Macitentan …
• Combinational therapies
• Update our therapeutic goal
-6MWD? -Keep WHO functional class I-II ?
-Hemodynamics? -Right ventricular anatomy and function ?

Clinical factors associated with prognosis
Clinical features Survival
N=487
Non-Survival
N=53
P
Age, years 32 ± 15 30 ± 15 NS
6MWD, meters 407 ±106 409 ±158 NS
mRAP, mm Hg 7 ±5 7 ±6 NS
mPAP, mm Hg 65 ±21 67 ±20 NS
PVR, Woods U 16 ±11 16 ±9 NS
CI, L/min/m2 2.8 ±1.1 2.7 ±0.9 NS
SvO2, % 65 ±12 65 ±11 NS
UA, umol/L 369 ±129 361 ±110 NS
BNP 1003 ±918 1342 ±1404 NS
Diameters of RV, mm 32 ±11 36 ±11 0.026
Unpublished data

PAH is all about the RV
Time
PAP
PVR
CO
Pre-symptomatic/ Compensated
Symptomatic/ Decompensating
Symptom ThresholdRV FailureRV Failure
Declining/ Decompensated
New Direction: combination therapy maybe the better way to control RHF
• RV mass and size are strong predictors of survival
• May focus to Right Ventricle–Pulmonary Circulation Unit : Ischemia +over-pressure load
• How to improve the myocardium tissue ischemia? How can we gradually reverse of RV remodeling and normalize the RV size and function with medicine?
Voelkel NF et al.Circulation.2006;114:1883–1891. Champion HC et al.Circualtion.2009;120;992-1007.

Future: what we should do?
• To set up the truly therapy goal : pulmonary artery remodeling—occlusion---hemodynamic worse—heart remodeling—heart failure ( not only right heart failure, the wholely cardivascular system collapse )
• To reverse the right heart pathological remodeling : stronger combination therapy to 1) control the pulmonary arerial spasm and contraction ;2 ) stop and reverse the pulmonary vascular remodeling; 3 ) resolve the ischemia of myocardium
• To investigate who is the murderer to initiate the pulmonary arterial disease : not BMPRII mutation, maybe Virus infection on the pulmonary vascular bed?

西地那非联合贝前列素治疗
Unpublished data from Shanghai Pulmonary Hospital

右心衰竭
增加右室收缩功能
降低右室容量负荷 降低右室压力负荷Lang IM, et al. European Heart Journal .2007;9 (Supplement H):
H61–H67

联合治疗重症右心衰竭和肺高压危象
• 静脉泵入伊洛前列素(万他维)• 联合吸入万他维• 联合静脉泵入法舒地尔(天津红日药业:川威)• 联合高浓度氧疗• 联合多巴胺静脉滴注• 联合口服西地那非+波生坦• 控制肺部感染• 血流动力学监测• 氧动力学监测:混合静脉氧饱和度

Research will open the cure
大鼠肺动脉压力波形图

Acknowledgment1996-2008, our team only based in Beijing
From April 2008, our team actived in Beijing and
Shanghai
From April 2008, our lab research team was founded in Shanghai

![haigan renkeipath 1.ppt [互換モード] - Aichi Prefecture · 乳がん 大腸がん 肝臓がん 肺がん 胃がん 地域がん拠点病院 14病院 地域医療 かかりつけ医](https://img.pdfslide.tips/doc/110x75/5e32e7fa1cef6268437d1169/haigan-renkeipath-1ppt-fff-aichi-prefecture-oe-eoe.jpg)