Embed Size (px)
Citation preview

Korean Society of Interventional Radiology ■
7/25
Sp
ec
ial Le
ctu
re III
111 ▌
10:40-11:00 Special Lecture III. Vascular Malformation and Budd-Chiari Syndrome Saturday 25, July
Moderators: 윤현기 (울산의대), 김만득 (연세의대)
Treatment of complex vascular malformation
김 경 래
(UNC, USA)
Introduction
The International Society for the Study of Vascular Anomalies (ISSVA) classification scheme divides vas-cular anomalies into two broad categories: vascular tumors and vascular malformations (www.issva.org ). Among the many subsets within each category, lesions can be isolated or occur in multiple parts of the body and can be features of syndromes some of which are characterized by phenotypic overgrowth (vascular anomaly-overgrowth syndromes). Although hemangiomas and other vascular tumors can be seen, vascular anomaly-overgrowth syndromes almost always feature vascular malformations. It is recommended to use of the terms “segmental overgrowth” or “lateralized overgrowth” instead of “hemihypertrophy”. Segmental overgrowth is defined as “significant increase in length and/or girth of most or all of one side of the body compared to its contralateral side”. It is often but not necessarily restricted to one side of the body or one extremity. It can involve bone, soft tissue, or blood vessels alone or in combination. Identification of genetic abnormalities in vascular anomalies in general and particularly in overgrowth syndrome has led to reclassification of these disorders. Gene mutations are helpful diagnostic tools but are not entirely specific and can be associated with multiple overlapping or even distinct phenotypes. Low level mosaicism has been observed in vascular anomaly-overgrowth syndromes, such that suggestive phenotypes, even when genetic testing is negative, should be considered provisionally diagnostic.
PROS (PIK3CA-Related Overgrowth Spectrum): A few excellent reviews detail the clinical and genetic as-pects of this clinically overlapping group of syndromes. In brief, major manifestations of PROS are combina-tions of segmental body (adipose, muscle, nerve, bone) or brain and cranial overgrowth, often but not al-ways with vascular malformations and epidermal nevi. Heterozygous (usually somatic mosaic but sometimes constitutional or germline) pathogenic variants of PIK3CA are causative. As noted above suggestive pheno-types, even when genetic testing is negative, should be considered sufficient for diagnosis. PIK3CA muta-tions are not synonymous with PROS, and isolated vascular malformations with PIK3CA mutations have
■ 대한인터벤션영상의학회 제29차 정기학술대회 및 총회
7/25
Sp
ec
ial Le
ctu
re III
▌ 112
been described without overgrowth. PIK3CA mutations can be seen in patients with KTS, CLOVES, FAVA (Fibro-Adipose Vascular Anomaly), and DCMO (Diffuse Capillary Malformation with Overgrowth). On the other hand, RASA1 mutations can be seen in CM-AVM1 and Parkes Weber Syndrome.
Klippel-Trenaunay Syndrome (KTS): Diagnostic criteria include segmental overgrowth, capillary malforma-tion (CM) in the area of overgrowth, and a venous (VM) or lymphatic (LM) malformation. Diagnostic cri-teria are usually met at birth although the degree of abnormalities ranges from mild to severe. In some pa-tients CM can fade over time, complicating diagnosis. There are two known persistent embryonic veins af-fect KTS patients; marginal vein and sciatic vein. These embryonic veins are frequently large, tortuous, dys-plastic, and may not contain valves. These incompetent embryonic veins can attain a substantial size with gravitational pooling and stagnation of blood in the lower limbs resulting in pain, postural hypotension, and increased risk of thromboembolism. There is a reported pulmonary embolism incidence of 12.5% in the KTS patients. Due to the large size of the anomalous veins, venous return from the limb is preferentially diverted from the smaller, underdeveloped deep venous system into these anomalous and incompetent veins. Closure of the dilated veins may reduce the risk of thromboembolism, particularly prior to the surgi-cal procedures, and may divert the venous return into the deep venous system and improve venous devel-opment and hemodynamics. The reported prevalence of persistent embryonic veins in the legs of KTS pa-tients ranges from 9% to 72%. Closure of these anomalous veins can be performed with endovenous laser therapy for the veins superficial to the fascia, however any veins located deeper than the fascia should be closed with coils or other endovascular occlusion devices due to the risk of nerve injury with laser therapy. Sclerotherapy can be performed for the treatment of VM or LM. Preferred sclerosing agents for the VM sclerotherapy are Sodium Tetradecyl Sulfate (STS) foam or alcohol. Doxycycline or dehydrated alcohol can be used for the sclerotherapy of macrocystic LM and Bleomycin has been popularly being used for the scle-rotherapy of microcystic LM. Cutaneous lymphatic vesicles can be treated with CO2 laser evaporation or Bleomycin sclerotherapy.
CLOVES Syndrome: The constellation of Congenital Lipomatous Overgrowth with Vascular malformations, Epidermoid nevi, Skeletal/Spinal abnormalities including Scoliosis was recognized as a syndrome. The over-growth is typically dramatic and noted prenatally or at the time of delivery. Lipomatous overgrowth usu-ally involves the back, flanks, axilla, abdomen, and buttocks. Hands and feet are characteristically large and wide with sandal gap toes. Although overgrowth can be bilateral, a tendency to asymmetry contributes to progressive scoliosis, uneven shoe sizes, and gross and fine motor delays. In addition to cutaneous CMs which overlie areas of overgrowth, patients have VMs an LMs frequently noted within fatty masses or in the abdomen, chest and extremities. Spinal and para-spinal AVMs have been documented in a significant proportion of CLOVES and can cause congestive heart failure or neural insufficiency. Central and thoracic phleboliths place patients at high risk for pulmonary emboli.
Parkes Weber Syndrome (PWS): PWS is a congenital disorder defined by overgrowth (usually of the low-er extremity) associated with congenital atypical CMs (round to oval in shape, and pinkish red or “salmon” in color) and AVM or AV shunt. VM or LM may be seen but always with a fast flow AVM or AV shunt as the distinctive feature. Leg length discrepancy may be a great as 10 cm, which can result in pelvic tilting
Korean Society of Interventional Radiology ■
7/25
Sp
ec
ial Le
ctu
re III
113 ▌
and scoliosis. Other complications of PWS include venous hypertension, leg ulcers, high output heart failure, lymphedema, distal vascular steal, distal arterial ischemia and pain, all of which typically develop during childhood. PWS is one of a group of related CM-AV malformation syndromes due to germline RASA1 mutations. Some CM-AVMs but not PWS have been associated with EPHB4. Atypical CMs should trigger RASA mutation analysis.
Conclusion
The diversity of presentations and complications among patients with vascular anomalies-overgrowth syn-drome underscores the need for multidisciplinary care. Although pediatric hematology, dermatology, and vascular & interventional radiology commonly are the focal points for continuity of care, at different times in a patient’s course, individuals may need help from multiple subspecialties. It is crucial to identify persis-tent embryonic veins and any other abnormal veins and close these veins given there is a substantial risk of thromboembolism. Treatment of combined VM, LM, or AVM should be also performed as early as possible because the treatment in older patients is more difficult and time-consuming. The risks in the patients of complex vascular malformation should be defined early in life and complete baseline imaging will provide the treatment strategy in long-term care.
References
1. Blei F. Overgrowth syndromes with vascular anomalies. Curr Probl Pediatr Adolesc Health Care. 2015; 45: 118-131.
2. Bertino F, Chaudry G. Overgrowth syndromes associated with vascular anomalies. Semin Roentgenol 2019; 54:349-358.
3. Martinez-Lopez A, Salvador-Rodriguez L, Montero-Vilchez T, Molina-Leyva A, Tercedor-Sanchez J, Arias-Santiago S. Vascular malformations syndromes: an update.Curr Opin Pediatr. 2019; 31:747-753.
4. Kalish JM, Biesecker LG, Brioude F, et al. Nomenclature and definition in asymmetric regional body overgrowth. Am J Med Genet A. 2017; 173:1735-1738.
5. Alomari AI. Diversion venography--a modified technique in Klippel-Trenaunay syndrome: initial experience. J Vasc Interv Radiol. 2010;21(5):685-9.
6. Reis J, 3rd, Alomari AI, Trenor CC, 3rd, Adams DM, Fishman SJ, Spencer SA, et al. Pulmonary throm-boembolic events in patients with congenital lipomatous overgrowth, vascular malformations, epidermal nevi, and spinal/skeletal abnormalities and Klippel-Trenaunay syndrome. J Vasc Surg Venous Lymphat Disord. 2018;6(4):511-6.
7. Bastarrika G, Redondo P, Sierra A, Cano D, Martinez-Cuesta A, Lopez-Gutierrez JC, et al. New techni-ques for the evaluation and therapeutic planning of patients with Klippel-Trenaunay syndrome. J Am Acad Dermatol. 2007;56(2):242-9.
8. Cherry KJ, Gloviczki P, Stanson AW. Persistent sciatic vein: diagnosis and treatment of a rare condition. J Vasc Surg. 1996;23(3):490-7.
■ 대한인터벤션영상의학회 제29차 정기학술대회 및 총회
7/25
Sp
ec
ial Le
ctu
re III
▌ 114
11:00-11:20 Special Lecture III. Vascular Malformation and Budd-Chiari Syndrome Saturday 25, July
Moderators: 윤현기 (울산의대), 김만득 (연세의대)
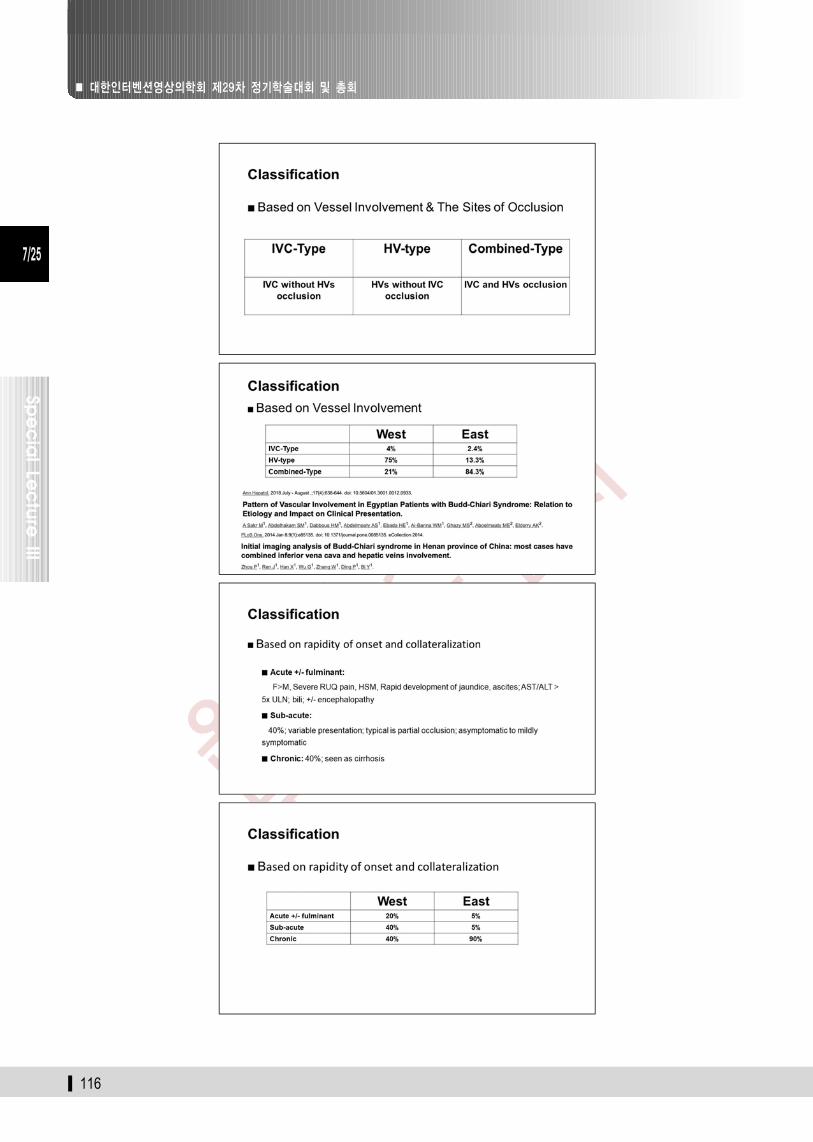
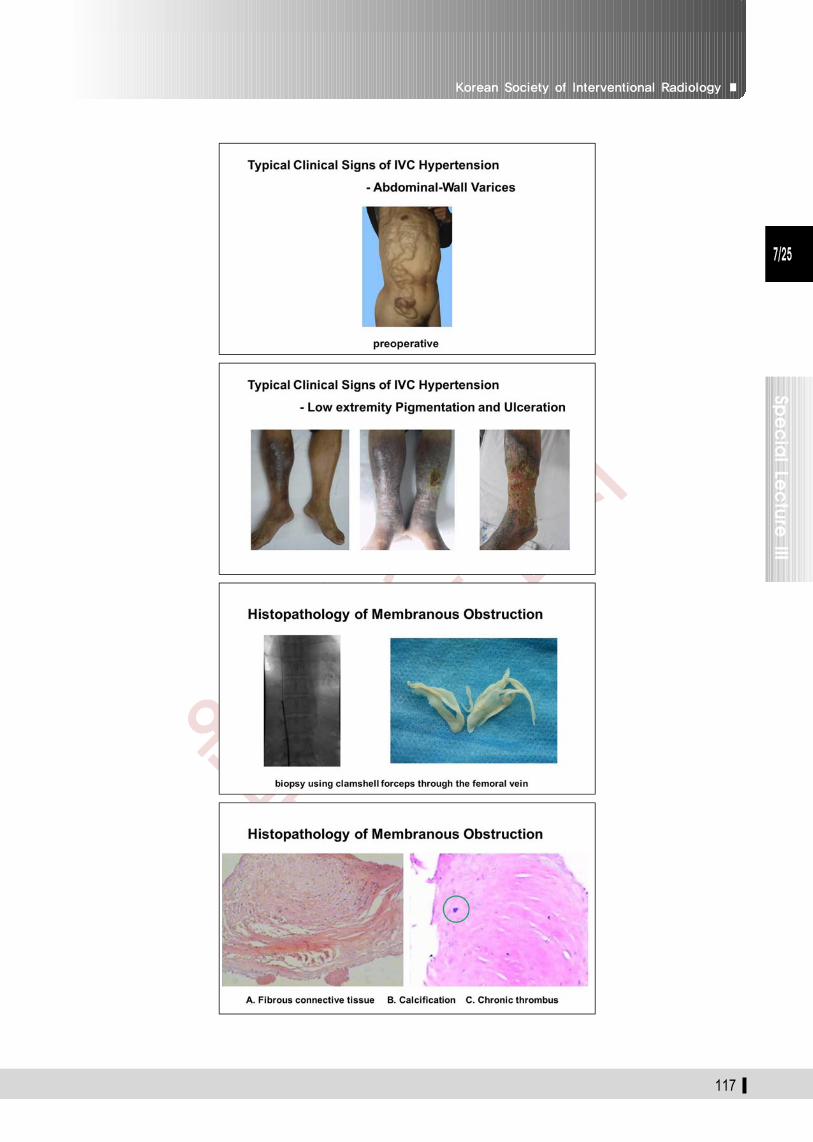
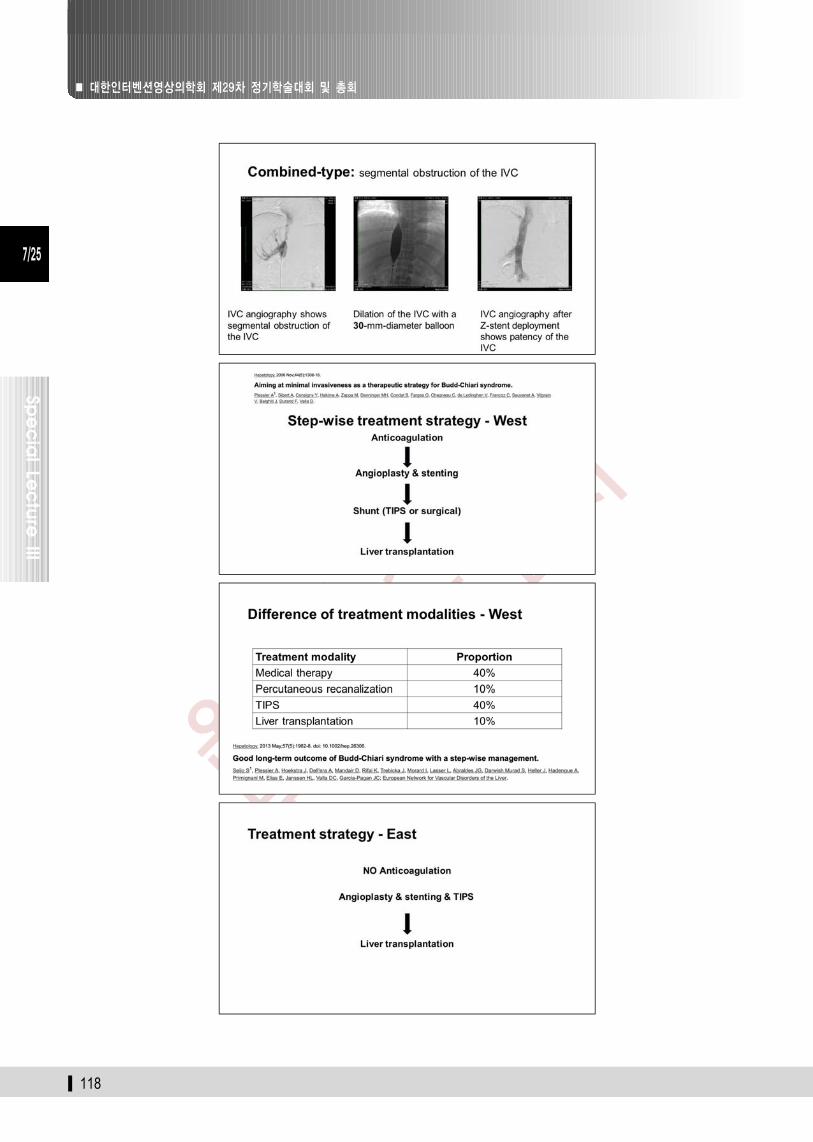
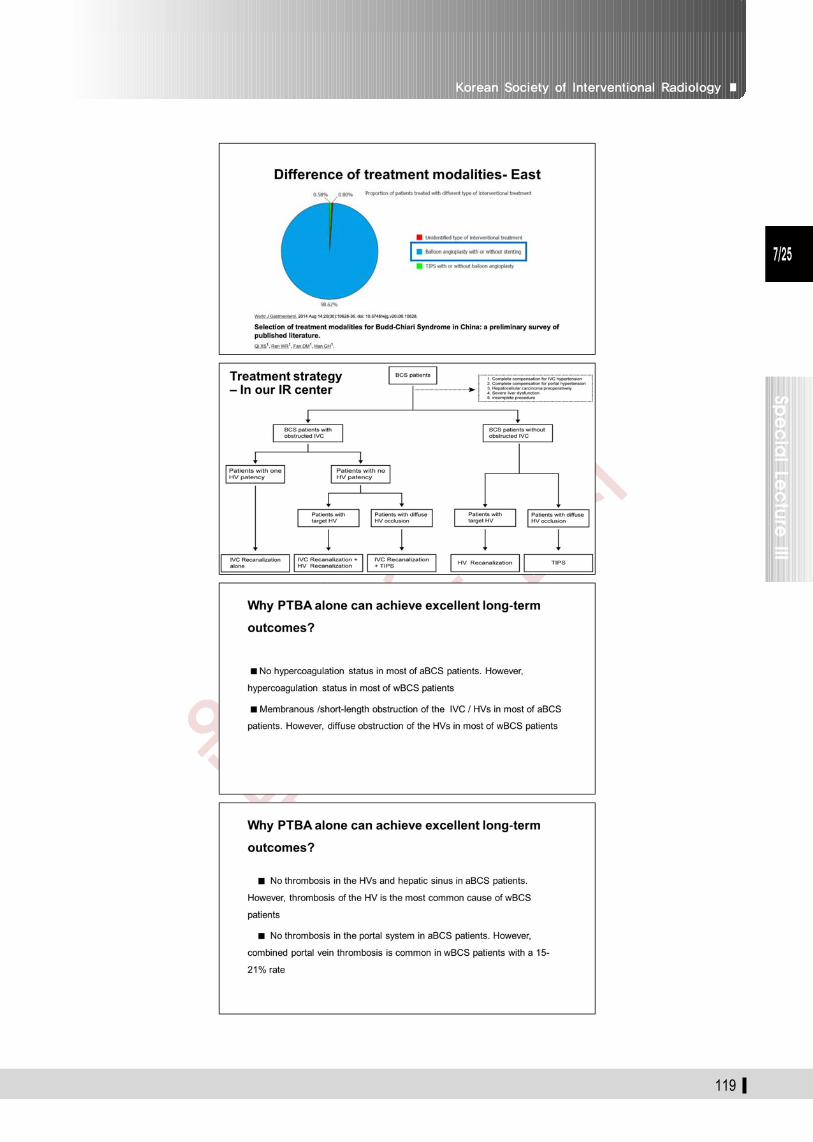
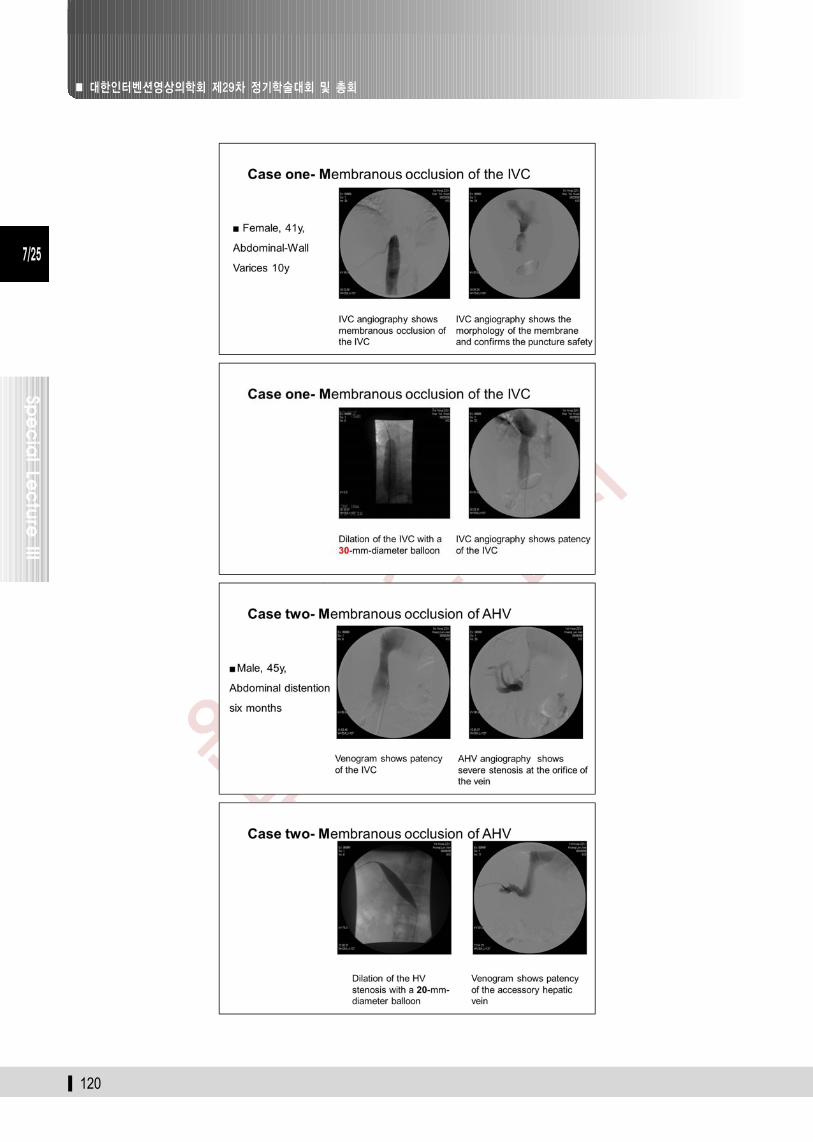
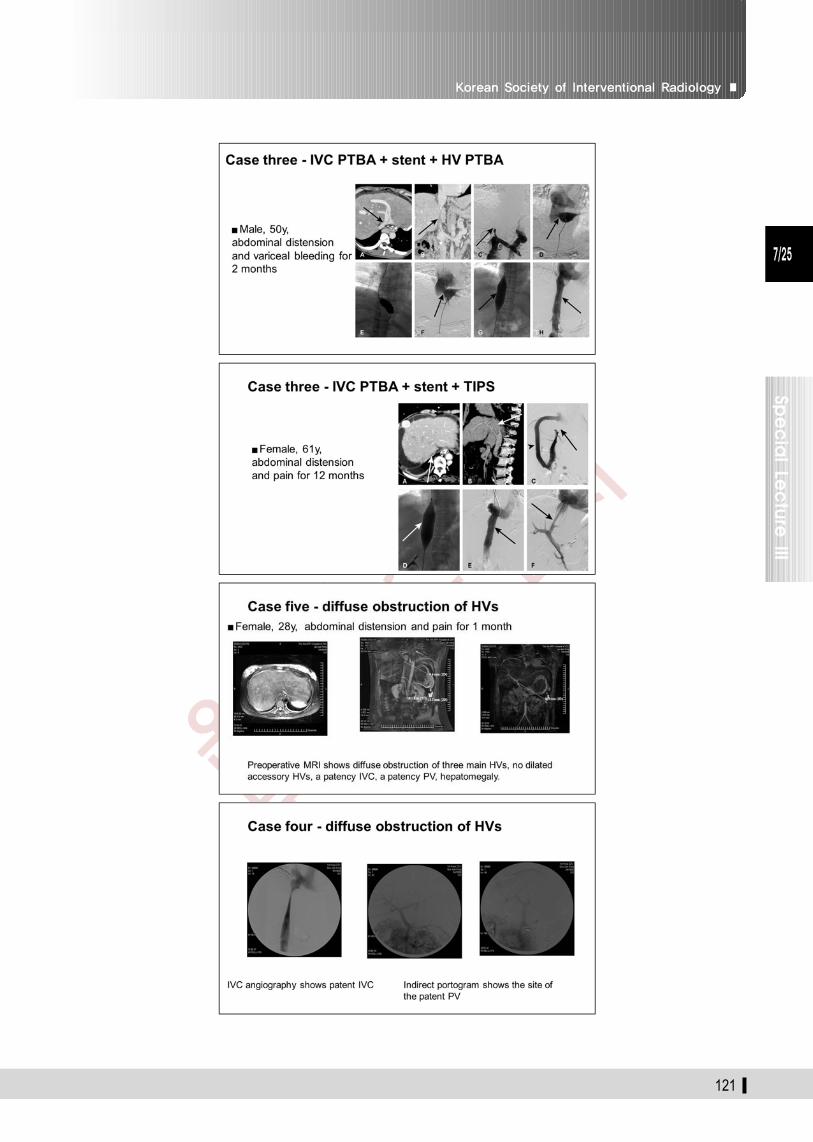
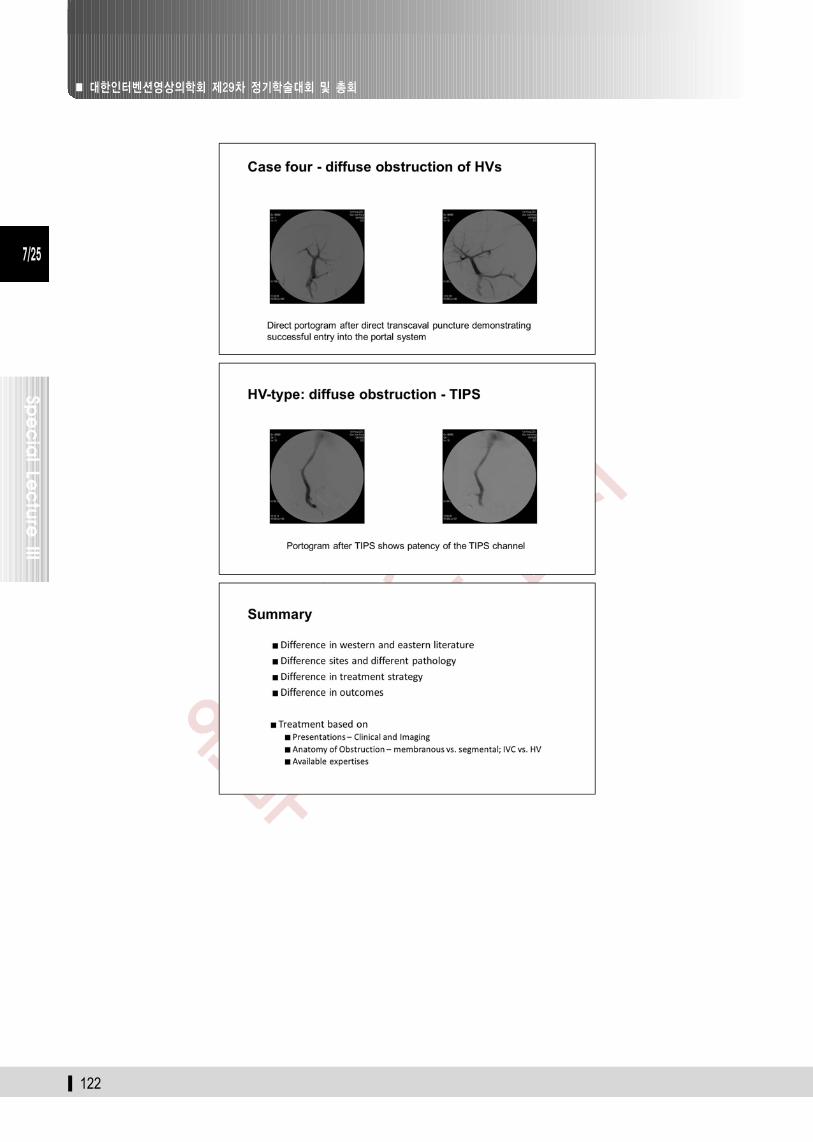
Budd-Chiari Syndrome: East vs. West
Penguin-xu Ding
(First Affiliated Hosp. of Zhengzhou Univ., China)
Korean Society of Interventional Radiology ■
7/25
Sp
ec
ial Le
ctu
re III
115 ▌
■ 대한인터벤션영상의학회 제29차 정기학술대회 및 총회
7/25
Sp
ec
ial Le
ctu
re III
▌ 116
Korean Society of Interventional Radiology ■
7/25
Sp
ec
ial Le
ctu
re III
117 ▌
■ 대한인터벤션영상의학회 제29차 정기학술대회 및 총회
7/25
Sp
ec
ial Le
ctu
re III
▌ 118
Korean Society of Interventional Radiology ■
7/25
Sp
ec
ial Le
ctu
re III
119 ▌
■ 대한인터벤션영상의학회 제29차 정기학술대회 및 총회
7/25
Sp
ec
ial Le
ctu
re III
▌ 120
Korean Society of Interventional Radiology ■
7/25
Sp
ec
ial Le
ctu
re III
121 ▌
■ 대한인터벤션영상의학회 제29차 정기학술대회 및 총회
7/25
Sp
ec
ial Le
ctu
re III
▌ 122



![최시원초등학교교육과정 기출문제해설 토-2016 [11.28( )] · 110010 최시원초등학교교육과정 기출문제해설 토-2016 [11.28( )] 35면중110010면](https://img.pdfslide.tips/doc/110x75/5fdf766279f7ce390868b446/oeoeeeeoee-eoeeoe-2016-1128-110010.jpg)

























![[2013년 6월 25일] it 총아 자동차 산업전망](https://img.pdfslide.tips/doc/110x75/587284891a28abc7068b6dbd/2013-6-25-it-.jpg)