-
8/6/2019 39 mia a y Adenomas Pituitarios
1/16
Hyperprolactinemia,Galactorrhea, and Pituitary
AdenomasEtiology, Differential Diagnosis, Natural History,
ManagementRogerio A. Lobo
39
KEY TERMS AND DEFINITIONS
Bromocriptine (2-Bromo--
Ergocryptine Mesylate). Semisyntheticergot alkaloid that is a
dopamine receptoragonist used to treat hyperprolactinemia.
Cabergoline. A long-acting dopaminereceptor agonist that
directly inhibitssecretion of prolactin from the pituitaryand is an
effective treatment forhyperprolactinemia.
Computed Tomography (CT). Animaging technique for detecting soft
tissueabnormalities that uses a computer tointegrate differences in
X-ray beamattenuation resulting from varying densitiesin adjacent
tissue.
Craniopharyngioma. A rare hypothalamictumor that can produce
hyperprolactinemia.
Empty Sella Syndrome. An intrasellar
extension of the subarachnoid space
resulting in compression of the pituitarygland and an enlarged
sella turcica that maybe associated with galactorrhea
andhyperprolactinemia.
Galactorrhea. Nonpuerperal secretionfrom the breast of watery or
milky fluid that
contains neither pus nor blood.
Hyperprolactinemia. Levels of circulatingprolactin above normal
(>20 to 25 ng/mL)that can cause galactorrhea or amenorrhea
orboth.
Hypocycloidal Tomography. Multipleradiographs of the sella
turcica at intervalsof 2 to 3 mm with a hypocycloidalmovement.
Macroadenoma. An uncommon type ofprolactin-secreting pituitary
adenoma(prolactinoma) greater than 1 cm in
diameter, usually with extrasellar extension.
Magnetic Resonance Imaging (MRI).
Technique for soft tissue imaging that usesresonance of hydrogen
nuclei in a staticmagnetic field exposed to
low-frequencyradiowaves.
Microadenoma. The common type ofprolactinoma less than 1 cm in
diameter.
Prolactin. Polypeptide hormone secretedby anterior pituitary
lactotrophs that hasmammotrophic and lactogenic functions.
Prolactin-Inhibiting Factor. Theneurotransmitter (believed to be
dopamine)that inhibits prolactin synthesis andrelease.
Prolactinoma. The most commonpituitary tumor arising from
chromophobiccells that secrete prolactin.
963
Prolactin (PRL) is a polypeptide hormone containing 198
aminoacids and having a molecular weight of 22,000 daltons.
Itcirculates in different molecular sizes: a monomeric (small)
form(mol wt 22,000 daltons), a polymeric (big) form (mol wt50,000
daltons), and an even larger polymeric (big-big) form(mol wt >
100,000 daltons). Big PRL is presumed to be a dimer,and big-big PRL
may represent an aggregation of monomericmolecules. The larger
forms also contain added sugar moieties(glycosylation) which
decreases biologic activity. The small formis biologically active,
and about 80% of the hormone is secreted
in this form. Most immunoassays measure both the small andlarge
forms of PRL. As stated earlier, the polymeric forms havereduced
biologic activity and reduced binding to mammarytissue membranes.
Women have been identified with high levelsof PRL on routine
immunoassay who are completely normaland have been found to have
circulating polymeric forms on gelelectrophoresis.
PRL is synthesized and stored in the pituitary gland in
chromo-phobe cells called lactotrophs, which are located mainly in
thelateral areas of the gland. PRL is encoded by its gene (10 kb)
onchromosome 6. At the molecular level, it is stimulated and
suppressed by multiple factors. The principal stimulating
factoris thyroid-releasing hormone (TRH), and the major
inhibitingfactor is dopamine. Estrogen also enhances PRL secretion
byenhancing the effects of TRH and inhibiting the effects
ofdopamine. A potential direct effect may also be mediated
viagalanin. The principal receptor dopamine interacts with is
D2,
which is the target for various dopamine agonists used in
thetreatment of hyperprolactinemia.
In addition, PRL is synthesized in decidualized stroma
ofendometrial tissue. From these tissues PRL is secreted into
the
circulation and, in the event of pregnancy, into the
amnioticfluid. The control of decidual PRL is different from that
of thepituitary and does not respond to dopamine. PRL is
normallypresent in measurable amounts in serum, with mean levels
ofabout 8 ng/mL in adult women. It circulates in an unboundform,
has a 20-minute half-life, and is cleared by the liver andkidney.
The main function of PRL is to stimulate the growth ofmammary
tissue as well as to produce and secrete milk into thealveoli;
thus, it has both mammogenic and lactogenic functions.Specific
receptors for PRL are present in the plasma membraneof mammary
cells as well as many other tissues.
-
8/6/2019 39 mia a y Adenomas Pituitarios
2/16
64 REPRODUCTIVE ENDOCRINOLOGY AND INFERTILITY
PHYSIOLOGY
PRL synthesis and release from the lactotrophs are controlledby
central nervous system neurotransmitters, which act on thepituitary
via the hypothalamus. The major control mechanismis inhibition, as
pituitary stalk section results in increased PRLsecretion. It
appears that the major physiologic inhibitor of PRLrelease is the
neurotransmitter dopamine, which acts directlyon the pituitary
gland. There are specific dopamine receptorson the lactotrophs, and
dopamine inhibits PRL synthesis andrelease in pituitary cell
cultures. Thus dopamine appears to bethe prolactin-inhibiting
factor (PIF). Although a hypothalamicprolactin-releasing factor
(PRF) has not been isolated, it isknown that both the
neurotransmitter serotonin and thyrotropin-releasing factor
stimulate PRL release. Since the latter stimulatesPRL release only
minimally unless infused, it appears that sero-tonin is PRF or is
responsible for its secretion. The rise in PRLlevels during sleep
appears to be controlled by serotonin.
PRL is secreted episodically, and serum levels
fluctuatethroughout the day and throughout the menstrual cycle,
withpeak levels occurring at midcycle. Although changes in
PRLlevels are not as marked as the pulsatile episodes of
luteinizinghormone (LH), Bckstrm and colleagues reported a
declinein both basal concentration and pulse frequency of PRL in
theluteal phase of the cycle. Estrogen stimulates PRL productionand
release. Under the influence of estrogen, PRL levels increasein
females at the time of puberty.
During pregnancy, as estrogen levels increase, there is a
con-comitant hypertrophy and hyperplasia of the lactotrophs.
Thematernal increase in PRL occurs soon after implantation,
con-comitant with the increase in circulating estrogen.
Circulatinglevels of PRL steadily increase throughout pregnancy,
reachingabout 200 ng/mL in the third trimester, and the rise is
directlyrelated to the increase in circulating levels of estrogen.
Despitethe elevated PRL levels during pregnancy, lactation does
not
occur because estrogen inhibits the action of PRL on the
breast,most likely blocking PRLs interaction with its receptor. A
day ortwo following delivery of the placenta, both estrogen levels
andPRL levels decline rapidly and lactation is initiated. PRL
levelsreach basal levels in nonnursing women in 2 to 3 weeks.
Althoughbasal levels of circulating PRL decline to the nonpregnant
rangeabout 6 months after parturition in nursing women,
followingeach act of suckling, PRL levels increase markedly and
stimulatemilk production for the next feeding.
Nipple and breast stimulation also increase PRL levels in
thenonpregnant female. Other physiologic stimuli that increasePRL
release are exercise, sleep, and stress. In addition, PRL
levelsnormally rise following ingestion of the noonday meal.
Forthese reasons PRL levels normally fluctuate throughout the
day,
with maximal levels observed during nighttime while asleep anda
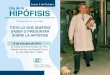
smaller increase occurring in the early afternoon (Fig. 39-1).When
the amount measured in the circulation in the nonpreg-nant woman
exceeds a certain level, usually 20 to 25 ng/mL, thecondition is
called hyperprolactinemia. The optimal time toobtain a blood sample
for assay to diagnose hyperprolactinemiais during the midmorning
hours. Increases in PRL levels abovethe normal range can occur
without a pathologic condition ifthe serum sample is drawn from a
patient who has recentlyawakened, has exercised, or has had recent
breast stimulation,such as breast palpation, during a physical
examination.
The most frequent cause of slightly elevated PRL levels
isstress, particularly the stress caused by visiting the
physiciansoffice. An excellent study demonstrating that most mildly
ele-vated PRL levels are not caused by pathologic
hyperprolactinemia
was performed by Muneyyirci-Delale and coworkers. These
in-vestigators studied 50 women without radiologic evidence of
aprolactinoma who had elevated PRL levels (23 to 156 ng/mL)measured
in two consecutive blood samples obtained 1 to 2 weeksapart. When
these women had serial blood sampling subse-quently performed in a
quiet room, 20 had normal PRL levelsin the 1-hour blood sample
(Fig. 39-2). The initial PRL levelsin these 20 women ranged from 26
to 69 ng/mL. The results ofthis study indicate that stress-related
hyperprolactinemia is acommon cause of a mild increase in PRL. All
women with initial
PRL levels less than 70 ng/mL should have subsequent
samplesdrawn 60 minutes after resting in a quiet room to
determinewhether true pathologic hyperprolactinemia is present.
Hyperprolactinemia can produce disorders of gonadotropinsex
steroid function, resulting in menstrual cycle
derangement(oligomenorrhea and amenorrhea) and anovulation, as well
asinappropriate lactation or galactorrhea. The mechanism
wherebyelevated PRL levels interfere with gonadotropin release
appearsto be related to abnormal gonadotropin-releasing
hormone(GnRH) release. Women with hyperprolactinemia have
abnor-malities in the frequency and amplitude of LH pulsations,
with
DIURNAL VARIATION OF PROLACTIN
Females (N= 5)
Males (N= 5)
Hours
Prolactin(ng/mL)
35
30
25
20
15
10
5
0
0
1100 1900 0300 1100 1900 0300
20
15
10
5
Figure 39-1. Hour-to-hour variation of serum prolactin
concentration innormal women and men studied throughout 48
consecutive hours. (FromKletzky OA, Davajan V: Hyperprolactinemia:
Diagnosis and treatment. InMishell DR Jr, Davajan V: Infertility,
Contraception and ReproductiveEndocrinology, 4th ed. Copyright 1997
by Blackwell Scientific Publications,Malden, MA. All rights
reserved. Reproduced with permission.)
-
8/6/2019 39 mia a y Adenomas Pituitarios
3/16
HYPERPROLACTINEMIA, GALACTORRHEA, AND PITUITARY ADENOMAS
a normal or increased gonadotropin response following
GnRHinfusion.
This abnormality of GnRH cyclicity thus inhibits gonado-tropin
release but not its synthesis. The reason for this
abnormalsecretion of GnRH is an inhibitory effect of dopamine
opioidpeptides at the level of the hypothalamus. In addition,
elevatedPRL levels have been shown to interfere with the
positive
estrogen effect on midcycle LH release. It has also been
shownthat elevated levels of PRL directly inhibit basal as well
asgonadotropin-stimulated ovarian secretion of both estradiol
andprogesterone. However, this mechanism is probably not theprimary
cause of anovulation, because women with hyper-prolactinemia can
have ovulation induced with various agents,including pulsatile
GnRH. Some women with moderate hyper-prolactinemia as determined by
radioimmunoassay have a greaterthan normal proportion of the
big-big forms. Because of thereduced bioactivity of this form of
PRL, these individuals canhave normal pituitary and ovarian
function.
The clinician should measure serum PRL levels in all women with
galactorrhea, as well as those with oligomenorrhea andamenorrhea
without the presence of an elevated level of follicle-
stimulating hormone (FSH). Hyperprolactinemia has been re-ported
to be present in 15% of all anovulatory women and 20%of women with
amenorrhea of undetermined cause. Galactorrheais defined as the
nonpuerperal secretion from the breast of
watery or milky fluid that contains neither pus nor blood.
Thefluid may appear spontaneously or after palpation. To
determineif galactorrhea is present, the clinician should palpate
the breast,moving from the periphery toward the nipple in an
attemptto express any secretion. The diagnosis of galactorrhea can
beconfirmed by observing multiple fat droplets in the fluid whenit
is examined under low-power magnification (Fig. 39-3). The
incidence of galactorrhea in women with hyperprolactinemiahas
been reported to range from 30% to 80%, and these differ-ences
probably reflect variations in the techniques used to detectmammary
excretion. Unless there has been continued breaststimulation after
a pregnancy, the presence of galactorrhea
serves as a biologic indicator that the PRL level is
abnormallyelevated. Davajan and associates reported that 62% of
women with galactorrhea have hyperprolactinemia. Some
individualswith galactorrhea and normal immunoassayable PRL levels
mayhave elevated biologically active PRL. The incidence of
hyper-prolactinemia is higher (88%) in those women with
galactorrhea
who have amenorrhea and low estrogen levels than in those women
with galactorrhea and normal estrogen levels (49%),regardless of
menstrual status.
ETIOLOGY
Pathologic causes of hyperprolactinemia, in addition to a
PRL-secreting pituitary adenoma (prolactinoma) and other
pitui-tary tumors that produce acromegaly and Cushings
disease,include hypothalamic disease, various pharmacologic
agents,hypothyroidism, chronic renal disease, or any chronic type
ofbreast nerve stimulation, such as may occur with thoracic
opera-tion, herpes zoster, or chest trauma. The following box
providesa list of the various causes of hyperprolactinemia.
One of the most frequent causes of galactorrhea and
hyper-prolactinemia is the ingestion of pharmacologic agents,
partic-ularly tranquilizers, narcotics, and antihypertensive agents
(seethe following box ). Of the tranquilizers, the phenothiazines
and
*
**
*
Figure 39-2. Mean plus or minus standard error ( SE) serum
prolactin levelsin women with prolactinoma (N= 20) and idiopathic
(N= 30) and stress-related (N= 20) hyperprolactinemia before
(pretest I and II) and during
hyperprolactinemia test. Differences (*p < 0.01) are in
relation to time zerovalues. (Mean prolactin values among groups
were also significantly different[p < 0.01] at all times.) (From
Muneyyirci-Delale O, Goldstein D, Reyes FI,et al: Diagnosis of
stress-related hyperprolactinemia: evaluation of
thehyperprolactinemia rest test. NY State J Med 89:205, 1989.)
Figure 39-3. Fat droplets seen under microscope from a patient
withgalactorrhea. (From Kletzky OA, Davajan V: Hyperprolactinemia:
Diagnosisand treatment. In Mishell DR, Davajan V, Lobo RA [eds]:
Infertility,Contraception and Reproductive Endocrinology, 3rd ed.
Cambridge, MA,Blackwell Scientific Publications, 1991.)
-
8/6/2019 39 mia a y Adenomas Pituitarios
4/16
-
8/6/2019 39 mia a y Adenomas Pituitarios
5/16
HYPERPROLACTINEMIA, GALACTORRHEA, AND PITUITARY ADENOMAS
Central Nervous System Disorders
Hypothalamic CausesDiseases of the hypothalamus that produce
alterations in thenormal portal circulation of dopamine can result
in hyper-prolactinemia. Such diseases include craniopharyngioma
andinfiltration of the hypothalamus by sarcoidosis,
histiocytosis,leukemia, or carcinoma. All these conditions are
rare, with cranio-pharyngioma being the most common. These tumors
arise from
remnants of Rathkes pouch along the pituitary stalk. Grosslythey
can be cystic, solid, or mixed, and calcification is usuallyvisible
on radiograph. They are most frequently diagnosedduring the second
and third decades of life and usually resultin impairment of
secretion of several pituitary hormones.
Pituitary CausesVarious types of pituitary tumors, lactotroph
hyperplasia, andthe empty sella syndrome can be associated with
hyperpro-lactinemia. It has been estimated that as many as 80% of
allpituitary adenomas secrete PRL. The most common pituitarytumor
associated with hyperprolactinemia is the prolactinoma,arbitrarily
defined as a microadenoma if its diameter is less than1 cm and as a
macroadenoma if it is larger. Hyperprolactinemiahas been reported
to occur in about 25% of individuals withacromegaly and 10% of
those with Cushings disease, indicatingthat these pituitary
adenomas, which mainly secrete growthhormone (GH) and
adrenocorticotropic hormone (ACTH),frequently also secrete PRL.
Hyperplasia of lactotrophs has beenreported to occur in about 8% of
pituitary glands examined atautopsy. Individuals with hyperplasia
of the lactotrophs cannotbe distinguished from those having a
microadenoma by anyclinical, laboratory, or radiologic method. It
is a diagnosis thatcan be made only at the time of surgical
exploration of the pitui-tary gland. Pituitary enlargement with
suprasellar extensioncaused by lactotroph hyperplasia has been
reported. Functionalhyperprolactinemia is the term used for the
clinical diagnosis ofcases of elevated PRL levels without evidence
of an adenoma.This condition may occur because of decreased
dopamineinhibition or the presence of an adenoma that is too small
tobe visualized.
Another cause of hyperprolactinemia is the primary emptysella
syndrome. The termprimary empty sella syndromedescribesa clinical
situation in which an intrasellar extension of the sub-arachnoid
space results in compression of the pituitary gland and
an enlarged sella turcica. The cause is believed to result froma
congenital or acquired (by radiation or surgery) defect in thesella
diaphragm that allows the subarachnoid membrane toherniate into the
sella turcica (Fig. 39-5). The syndrome isusually associated with
normal pituitary function except forhyperprolactinemia. Although
some individuals with primaryempty sella syndrome have a coexistent
prolactinoma, Ghariband colleagues reported a series of 11 persons
with an emptysella and hyperprolactinemia who had no histologic
evidence ofa prolactinoma or hyperplasia of the lactotrophs. They
statedthat about 5% of individuals with the empty sella have
hyper-prolactinemia or amenorrheagalactorrhea or both. It is
theo-rized that with this syndrome distortion of the
infundibularstalk results in decreased levels of dopamine reaching
the pituitary
to inhibit PRL. Serum PRL levels are usually less than 100 ng/mL
with the empty sella syndrome, and some women with thissyndrome
have galactorrhea with normal PRL levels. Kleinbergand coworkers
reported that about 10% of all individuals withan enlarged sella
turcica have the empty sella syndrome. The bestmodality for
diagnosing this condition is magnetic resonanceimaging (MRI).
Computed tomographic (CT) scanning withintrathecal injection of
metrizamide can also be used. It is im-portant to establish the
diagnosis because the syndrome has abenign course.
Pharmacologic Agents Affecting ProlactinConcentrations
Stimulators
Anesthetics including cocainePsychoactive
PhenothiazinesTricyclic antidepressantsOpiates
ChlordiazepoxideAmphetaminesDiazepamsHaloperidolFluphenazineChlorpromazineSSRIs
HormonesEstrogenOral-steroid contraceptivesThyrotropin-releasing
hormone
Antihypertensives-MethyldopaReserpineVerapamil
Dopamine receptor antagonists
MetoclopramideAntiemetics
SulpridePromazinePerphenazine
OthersCimetidineCyproheptiadineProtease inhibitors
InhibitorsL-DopaDopamineBromocriptinePergolide
CabergolineDepot bromocriptine
SSRIs, selective serotonin reuptake inhibitors.From Shoupe D,
Mishell DR Jr: Hyperprolactinemia: Diag-nosis and treatment. In
Lobo RA, Mishell DR Jr, Paulson RJ,Shoupe D (eds): Mishells
Textbook of Infertility, Contracep-tion and Reproductive
Endocrinology, 4th ed. Cambridge,MA, Blackwell Scientific
Publications, 1997.
-
8/6/2019 39 mia a y Adenomas Pituitarios
6/16
68 REPRODUCTIVE ENDOCRINOLOGY AND INFERTILITY
Prolactinomas
In an unselected series of 120 autopsies of persons who had
hadno clinical evidence of pituitary disease, Burrow and
associates
found pituitary microadenomas to be present in 32 (27%).
Morerecently Molitch described that PRL incidentalomas occur in11%
of subjects at autopsy. Abd El-Hamid and colleagues alsoreported
that adenomas were found in 78 of 486 (16%) pitui-tary glands
examined after unselected autopsies. In all seriesPRL was found in
about half the glands, indicating that morethan 1 in 10 individuals
in the general population have aprolactinoma.
Overall about 50% of women with hyperprolactinemia havea
prolactinoma. The incidence is higher when the PRL levelsexceed 100
ng/mL, and nearly all individuals with PRL levelsgreater than 200
ng/mL have a prolactinoma. The vast majorityof prolactinomas in
women are microadenomas. Kleinbergand coworkers reported that
overall 20% of individuals with
galactorrhea and 35% of women with amenorrheagalactorrheahad
radiologic evidence of pituitary tumors. Tumors are alsopresent in
about 20% of women with hyperprolactinemia andmenstrual
irregularities without galactorrhea. The incidenceof prolactinoma
is greater in those individuals with a more pro-found disturbance
of normal hypothalamicpituitaryovarianfunction. Davajan and
associates reported that 70% of women
with hyperprolactinemia, galactorrhea, and secondary amenor-rhea
with low estrogen levels had radiologic evidence of apituitary
adenoma. Evidence of a tumor occurred in only 20%to 30% of those
with hyperprolactinemia and normal menses,
oligomenorrhea, or secondary amenorrhea who had
sufficientestrogen to undergo withdrawal bleeding after
progesteroneadministration. In both these studies no evidence of
tumor
was found in individuals with normal menses, galactorrhea,
and
normal PRL levels. Therefore radiologic studies do not needto be
performed if galactorrhea is present and PRL levels arenormal.
Figure 39-6 depicts various possible causes of
prolactinomaformation. In the past it was firmly believed that
adenomas orhyperplasia were the result of hypothalamic dopamine
dys-regulation, which was either a functional defect or the result
ofaltered blood supply. Current thinking is that adenomas arisefrom
single cell mutations, with clonal proliferation
occurringsubsequently. However, a search for mutations in
oncogenes,the dopamine D2 or TRH receptor, signal transduction
mecha-nisms or transcription factors have not been very rewardingto
date. Prolactinomas that occur in 20% of patients withmultiple
endocrine neoplasia type 1 (MEN-1) may be due to an
inactivating mutation of theMENINgene, although this specialcase
is clearly different from the usual type of prolactinomas.It is
also important to note that prolactinomas may also
secrete other hormones; GH is the most frequent
combination.Also, up to 40% of GH-secreting adenomas also secrete
PRL.Combinations of PRL and ACTH, PRL and TSH, and PRL andFSH have
been described.
Long-term studies of individuals with microadenomas demon-strate
that enlargement is uncommon and that many of thesetumors regress
spontaneously. In a longitudinal retrospectivestudy of 43 women
with hyperprolactinemia and a radiologic
Figure 39-5. Diagrammatic representation ofempty sella
syndrome.A, Normal anatomicrelationship. B, C, and D, Progression
in
development of empty sella syndrome. Notethinning of floor and
symmetrical enlargementof sella turcica. (From Kletzky OA, Davajan
V:Hyperprolactinemia: Diagnosis and treatment.In Mishell DR,
Davajan V, Lobo RA [eds]:Infertility, Contraception and
ReproductiveEndocrinology, 3rd ed. Cambridge, MA,Blackwell
Scientific Publications, 1991.)
Cerebrospinal fluid
Opticchiasma
Arachnoidmembrane
Pituitarydiaphragm
Pituitary gland
Defectivediaphragm
Arachnoidherniation
Completeherniation
Thinning of sella floor
Increasedherniation
Defectivediaphragm
C D
A B
-
8/6/2019 39 mia a y Adenomas Pituitarios
7/16
HYPERPROLACTINEMIA, GALACTORRHEA, AND PITUITARY ADENOMAS
diagnosis of microadenoma, March and colleagues found that
only 2 women had evidence of enlargement of the adenoma, with a
mean duration of follow-up of 5 years. Of these 43 women, 3 had
spontaneous regression of their hyperprolac-tinemia and resumption
of normal menses. Koppelman andcoworkers reported similar results.
Of 25 women with prolacti-nomas (18 with microadenomas and 7 with
minimally enlargedsella) followed up for a mean duration of 11
years withouttreatment, only 1 woman had slight progression of a
sellaabnormality. None had visual field or other pituitary
functionchanges, seven resumed normal menses spontaneously,
andgalactorrhea spontaneously resolved in six.
The results of these retrospective studies have been confirmedby
two prospective studies of untreated microprolactinomas.In a 3- to
7-year prospective longitudinal study of 30 hyper-prolactinemic
women, Schlechte and associates found that of 13
women with initially abnormal radiographic findings, 4
becamenormal, 7 did not change, and 2 had evidence of tumor
growth.Of 17 women with initially normal radiographic findings,
4became minimally abnormal. None of the 30 developed a
macro-adenoma or pituitary hypofunction. In this study, as in the
tworetrospective studies just reported, more sensitive
radiographictechniques (tomograms, followed by CT) were used as
thestudy progressed and could account for the minimal evidence
oftumor growth. Sisam and colleagues overcame this problem
byprospectively following a group of 38 women with
hyperpro-lactinemia and microprolactinomas by serial CT scans for
amean duration of 50 months. None of these women had evi-dence of
tumor progression, even the 2 who had a marked in-crease in PRL
levels. In this group, nine (25%) had spontaneousimprovement of
their symptoms. Martin and coworkers fol-lowed the natural history
of 41 women with idiopathic hyper-prolactinemia and
amenorrheagalactorrhea for up to 11 years.During this time, 9 women
conceived spontaneously, and 16have resumed spontaneous menses with
cessation of galactorrhea.Only one woman developed a microadenoma.
Thus, hyper-prolactinemia with or without a microadenoma follows a
benignclinical course in most women, and therapy is unnecessary
unlesspregnancy is desired or estrogen levels are low.
The combination of six studies in 139 women observed forat least
8 years without treatment showed that the progressionrate is only
6.5%. Several studies have reported that pregnancyis beneficial for
women with functional hyperprolactinemia orPRL-secreting
microadenomas. Following pregnancy, PRL levelsdecrease in about
half the women. Crosignani and associatesreported that PRL levels
became normal in about 30% of 176hyperprolactinemic women after
pregnancy. PRL levels decreased
to normal in 36% of women with functional hyperprolactinemiaand
17% of those with adenomas. Therefore if women
withhyperprolactinemia desire to become pregnant they should
beencouraged to do so, as pregnancy is likely to result in normalor
lowered PRL levels.
DIAGNOSTIC TECHNIQUES
Because most prolactinomas are microadenomas that do notcause
enlargement of the sella turcica, the diagnosis usuallycannot be
made by ordinary anteroposterior and lateral coned
X-ray examination of the sella turcica. With the development
ofmore precise radiologic methods of detecting soft tissue
pituitary
abnormalities, it is now possible to detect even small
adenomas.Initially detection of microadenomas was accomplished
byobtaining tomographic radiographic examination of the
sellaturcica at intervals of 2 to 3 mm in the anteroposterior
andlateral projections with a hypocycloidal movement. These
arecalled hypocycloidal tomograms. Comparing the results of
tomo-grams with the findings of microadenoma at autopsy, Burrowand
coworkers found that the incidence of both false-positiveand
false-negative tomographic findings was about 20% each,
with an overall accuracy rate of 61%. Furthermore,
radiationexposure with polytomography may be in excess of 20
rads.
PATHOGENESIS OF PITUITARY TUMORS
HypothalamusNormal
Hyperplasia ortumor due tohypothalamicdysfunction
Tumorarising de novo
Pituitary
Pituitary hormone
HyperplasiaTumor
Tumor
Hypothalamus
Hypothalamus
Pituitary hormone
Pituitary hormone
Releasing factor(+)
Inhibiting factor()
Releasing factor(+)
Inhibiting factor()
Releasing factor(+)
Inhibiting factor()
Figure 39-6. Possible mechanisms leading to the formation of a
prolactinoma.Top: normal regulation. Middle: tumors could arise
because of an increase inPRL-releasing factor (PRF) or a decrease
in PRL-inhibiting factor (dopamine).Bottom: tumors could arise de
novo without hypothalamic influence. (FromMolitch ME: Clinical
features and epidemiology of prolactinomas in women.In Olefsky JM,
Robbins RJ [eds]: Prolactinomas: Practical Diagnosis andManagement.
New York, Churchill Livingstone, 1986, pp 6795.)
-
8/6/2019 39 mia a y Adenomas Pituitarios
8/16
70 REPRODUCTIVE ENDOCRINOLOGY AND INFERTILITY
Current recommended techniques are to obtain a CT scan with IV
contrast, or an MRI with gadolinium enhancement.The latter provides
better soft tissue definition, and the CT scanprincipally shows
bony structural abnormalities.
The MRI provides 1-mm resolution and thus should be ableto
detect all microadenomas. Stein and associates comparedresults of
CT and MRI in 22 individuals with suspected pitui-tary adenomas.
MRI was found to be the superior diagnosticmodality because of its
greater soft tissue contrast (Fig. 39-7).In addition the MRI does
not have the radiation exposure of theCT scan (23 rads, 0.03
Gy).
Recommended Diagnostic Evaluation
It is currently recommended that PRL levels be measured in
allwomen with galactorrhea, oligomenorrhea, or amenorrhea whodo not
have an elevated FSH level. If PRL is elevated, a TSHassay should
be performed to rule out the presence of primaryhypothyroidism. If
TSH is elevated, T3 and T4 should bemeasured to rule out the rare
possibility of a TSH-secretingpituitary adenoma. If TSH is elevated
and hypothyroidism ispresent, appropriate thyroid replacement
should begin, and thePRL level will usually return to normal. If
TSH is normal andthe woman has a normal PRL level with
galactorrhea, no furthertests are necessary if she has regular
menses. Because some
women with galactorrhea, abnormal menstrual function, andnormal
PRL levels have been found to have the empty sellasyndrome, an MRI
or a CT scan should be obtained to establishthe diagnosis in women
with these findings.
If PRL levels are elevated and the TSH is normal, an MRIif
available or CT scan should be obtained to detect a micro-adenoma
or macroadenoma. Macroadenomas are uncommonand rarely are present
with a PRL level less than 100 ng/mL.If the PRL level is more than
100 ng/mL or the woman com-plains of headaches or visual changes,
the likelihood of a tumorextending beyond the sella turcica is
increased. Microadenomasare a common cause of hyperprolactinemia,
but rarely enlarge.Neither pregnancy, oral contraceptives, nor
hormone replace-ment therapy stimulates the growth of these small
tumors, andtherapy is unnecessary unless ovulation induction is
desired orhypoestrogenism is present.
Visual field determination and tests of ACTH and thyroidfunction
are not necessary if a microadenoma is present, as thesesmall
tumors do not interfere with overall pituitary functionand do not
extend beyond the sella. However, these evalua-tions should be
performed in individuals with macroadenomasbecause suprasellar
extension of the tumor may exert pressure
on the optic chiasm, resulting in bitemporal visual field
defectsand interference with vision. The size of these tumors may
alsoaffect other aspects of pituitary function. Thus a test of
ACTHreserve, such as insulin-induced hypoglycemia (insulin
tolerancetest), as well as tests of thyroid function, should be
performedon all individuals with a macroadenoma.
MANAGEMENT
Expectant Treatment
Women with radiologic evidence of a microadenoma or func-tional
hyperprolactinemia who do not wish to conceive may
be followed without treatment by measuring PRL levels
onceyearly. Many of these women have deficient estrogen, and
lowestrogen levels in combination with hyperprolactinemia havebeen
shown to be associated with the early onset of osteoporosis.If the
woman has low estrogen levels, exogenous estrogen shouldbe
administered. Either replacement estrogenprogestin therapy,as is
used for postmenopausal women, or oral contraceptivescan be
utilized. Corenblum and Donovan reported that a groupof women with
both functional hyperprolactinemia and PRL-secreting pituitary
microadenomas who were treated with eithercyclic estrogen and
progestin or oral contraceptives for several
Figure 39-7. Images were selected to best demonstrate pathology
and do notexactly correspond in level of section through sella
turcica.A, CT scan (coronalsection) showing bony erosion of right
sella turcica (arrowhead) with possiblesoft tissue extension into
right cavernous sinus. Height of pituitary gland (notshown) is 9
mm. B, MRI (coronal section) showing soft tissue mass extendinginto
right cavernous sinus near carotid artery(large arrowhead). Height
ofpituitary gland is 9 mm. Normal optic chiasm is seen (small
arrowhead). (FromStein AL, Levenick MN, Kletzky OA: Computer
tomography versus magneticresonance imaging for the evaluation of
suspected pituitary adenomas. ObstetGynecol 73:996, 1989.)
A
B
-
8/6/2019 39 mia a y Adenomas Pituitarios
9/16
HYPERPROLACTINEMIA, GALACTORRHEA, AND PITUITARY ADENOMAS
years did not have an increase in the size of the adenomasor a
marked increase in PRL levels. Mean PRL levels actuallydeclined
with both treatment regimens. Testa reported that2 years of oral
contraceptive use in a group of women with hyper-prolactinemia with
microadenoma did not alter the size of theadenoma. Since side
effects and cost are less and compliance isbetter with exogenous
estrogen than with bromocriptine, it isnot necessary to use the
latter agent unless ovulation and preg-nancy are desired.
Individuals with hyperprolactinemia withor without microadenomas
who have adequate estrogen levelsas shown by the presence of
oligomenorrhea or amenorrhea
with follicular phase estradiol levels who do not wish to
con-ceive should be treated with periodic progestin
withdrawal(e.g., medroxyprogesterone acetate 510 mg/day for 10
dayseach month) or combination oral contraceptives to
preventendometrial hyperplasia.
Medical Therapy
The initial treatment for macroadenomas, as well as for
womenwith hyperprolactinemia who are anovulatory and wish to
con-ceive, should be administration of a dopamine receptor
agonist.Bromocriptine, pergolide, and cabergoline have been
used
with success for treating hyperprolactinemia; bromocriptineand
cabergoline are approved for use in the United States). Thegreatest
amount of clinical experience has been with use ofbromocriptine
(Fig. 39-8). This semisynthetic ergot alkaloid wasdeveloped in 1967
to inhibit PRL secretion. It directly stimu-lates dopamide 2
receptors, and as a dopamine receptor agonistit inhibits PRL
secretion both in vitro and in vivo. Afteringestion, bromocriptine
is rapidly absorbed, with blood levelsreaching a peak 1 to 3 hours
later. Serum PRL levels remaindepressed for about 14 hours after
ingestion of a single dose,after which time the drug is not
detectable in the circulation.
For this reason the drug is usually given at least twice daily,
withinitial therapy being started at one half of the 2.5-mg
tabletto minimize side effects. The most frequent side effects
areorthostatic hypotension (with an incidence of 15%), which
canproduce fainting and dizziness as well as nausea and vomiting.To
minimize these symptoms the initial dose should be takenin bed and
with food at nighttime. Less frequent adverse symp-
toms include headache, nasal congestion, fatigue,
constipation,and diarrhea. Most of these reactions are mild, occur
early inthe course of treatment, and are transient. To reduce the
adversesymptoms, the dose should be gradually increased every 1 to2
weeks until PRL levels fall to normal. The usual therapeuticdose is
2.5 mg twice or three times a day, but larger doses aresometimes
used when a macroadenoma is present.
Adverse effects, such as nausea, vomiting, and nasal
conges-tion, occur in about half the women taking oral
bromocriptineand may cause them to discontinue treatment. Vermesh
and col-leagues reported that the drug was very well absorbed
vaginally
without the presence of side effects. Furthermore, when asingle
tablet was placed deep in the posterior vaginal fornix,therapeutic
blood levels persisted for more than 24 hours,during which time PRL
levels remained suppressed (Fig. 39-9).Ginsburg and coworkers
subsequently reported that this methodof bromocriptine
administration was well accepted, effective,and well tolerated in a
group of 31 hyperprolactinemic women,17 of whom could not tolerate
oral bromocriptine. Minor side
effects occurred in only three women. The tablet is
placeddigitally deep in the vagina nightly at bedtime. A single
2.5-mgdose reduced PRL concentrations in 90% of patients treatedand
brought the levels to normal in one third of women. Higherdoses do
not appear to be more effective. Ginsburg and co-
workers recommended that the drug be administered
vaginallyinstead of orally for all women as a smaller dose of drug
can be
Figure 39-8. Formula of bromocriptine.
Figure 39-9. Mean ( SEM) plasma levels of bromocriptine(blue
circles) and prolactin (open circles) in a single study,extended to
48 hours, after vaginal bromocriptine (2.5 mg).(From Vermesh M,
Fossum GT, Kletzky OA: Vaginalbromocriptine: Pharmacology and
effect on serum prolactinin normal women. Obstet Gynecol 72:693,
1988.)
-
8/6/2019 39 mia a y Adenomas Pituitarios
10/16
72 REPRODUCTIVE ENDOCRINOLOGY AND INFERTILITY
used, once-daily administration is more convenient, and
sideeffects are fewer.
Bromocriptine is approved for treatment of adverse symp-toms
associated with hyperprolactinemia, such as galactorrhea,as well as
anovulatory infertility with and without the presenceof a
PRL-secreting adenoma. In hyperprolactinemic women
without adenomas, PRL levels return to normal in more than90%,
fertility is restored in 80%, and galactorrhea is eradicatedin 60%
with bromocriptine therapy. In women with hyper-prolactinemia and a
microadenoma, similar rates of successhave been reported.
Therefore, a dopamine agonist such as
bromocriptine or cabergoline is the treatment of choice forwomen
with PRL-secreting microadenomas who wish to ovulateor are bothered
by galactorrhea.
Despite administration of up to 20 mg of bromocriptine perday
orally, about 10% of individuals with microadenomas failto have PRL
levels return to normal, probably because of indi-vidual
differences in the sensitivity of lactotrophs to bromo-criptine.
Nevertheless, despite the persistently elevated PRLlevels, many of
these women ovulate and conceive (Fig. 39-10).
If pregnancy occurs after ovulation is induced with
bromo-criptine, therapy is usually discontinued, although there is
noevidence that the drug is teratogenic or adversely affects
preg-nancy outcome. If pregnancy is not desired but bromocriptineis
used to treat galactorrhea, therapy is usually continued for
at least 12 months, after which it should be discontinued for
afew weeks. Most women with microadenomas have recurrenceof
hyperprolactinemia, amenorrhea, and galactorrhea, althoughabout 10%
to 20% have permanent remission after discontinu-ing bromocriptine
treatment. Moriondo and associates reportedthat after 1 year of
bromocriptine treatment, 11% of women
with microadenomas had persistent normalization of PRL,with
return of regular menses after the drug was discontinued(Fig.
39-11). This incidence of permanent remission reached22% after 2
years of treatment. A higher rate of permanentremission occurred in
women treated with 10 mg/day than with
lower dosages, but higher doses of drug increase the incidenceof
adverse reactions and cause discontinuation of treatment.These
investigators found that after bromocriptine was dis-continued,
there was a 40% reduction in mean PRL levels inall women treated,
and about 60% had a greater than 30%reduction from pretreatment PRL
levels after the drug was dis-continued. Rasmussen and colleagues
reported the results ofdiscontinuation of long-term (median of 2
years) bromocriptinetherapy in 75 hyperprolactinemic women. In
about half the
women it was necessary to reinstate treatment because PRLlevels
rose. However, in the other half further treatment was un-
necessary because mean PRL levels decreased more than 60%and
either returned to normal or were only slightly elevated(Fig.
39-12). More than half of these 33 women resumed regularmenses
without further treatment. These data indicate thatthe remissions
were drug-related and not spontaneous. UsingCT scans before and
during bromocriptine therapy, Bonnevilleand coworkers found that
about 75% of individuals with micro-adenomas had reduction in tumor
size during bromocriptinetreatment, and in 40% the tumor had
disappeared (Fig. 39-13).To determine if permanent remission has
occurred, the PRLlevel should be measured about 6 weeks after
discontinuationof treatment because the levels plateau at this
time.
Bromocriptine treatment has also been shown to reduce tumormass
in 80% to 90% of individuals with macroadenomas. In
addition, visual disturbances, if present, are usually
promptlyrelieved. Following subsequent surgical removal of
thesebromocriptine-treated tumors, histologic examination revealeda
reduction of tumor cell size, with shrinkage of the cytoplasmbeing
greater than the nucleus. In addition, there are modifica-tions of
cell structure and morphology as compared with tumorsremoved
without prior medical treatment. The organelles respon-sible for
PRL synthesis shrink, indicating that bromocriptineimpairs PRL
synthesis as well as release. The reduction in sizeof macroadenomas
usually occurs rapidly, within a few weeksafter starting treatment,
but following withdrawal of drug the
Figure 39-10. Mean serum prolactin response tobromocriptine
therapy in five patients with radiographicevidence of pituitary
adenoma and residual hyperprolactinemia.
All five ovulated, and four conceived. (From Kletzky OA,
MarrsRP, Davajan V: Management of patients with hyper-prolactinemia
and normal or abnormal tomograms. Am JObstet Gynecol 147:528,
1983.)
-
8/6/2019 39 mia a y Adenomas Pituitarios
11/16
HYPERPROLACTINEMIA, GALACTORRHEA, AND PITUITARY ADENOMAS
tumor size may increase just as rapidly; thus the drug should
bewithdrawn cautiously. In contrast to the frequent occurrence
ofpituitary insufficiency, including diabetes insipidus, after
surgicalor radiologic treatment of large tumors, bromocriptine
treatmentis not accompanied by any type of pituitary
insufficiency.
Because permanent remission rarely occurs following with-drawal
of bromocriptine treatment from individuals with large
tumors, long-term treatment is usually necessary. The drug
hasbeen administered in some individuals for up to 12 years
with-out problems, and once biochemical, radiologic, and
clinicalresponses to treatment are established, they are generally
main-tained over a long-term period. Bromocriptine has also
beensuccessfully used to treat individuals with failure of, or
recur-rence after, operation or irradiation therapy.
Figure 39-11. Serum prolactin levels in four patientswho had
persistently normal prolactin levels afterbromocriptine (BRC)
treatment for 12 months. P,Pregnancy. (From Moriondo P, Travaglini
P, Nissim M,et al: Bromocriptine treatment of
microprolactinomas:Evidence of stable prolactin decrease after
drug
withdrawal. J Clin Endocrinol Metab 60:764, 1985. Copyright 1985
by The Endocrine Society.)
Figure 39-12. Geometric mean serum prolactin levels before
andafter discontinuation of bromocriptine treatment in 33 women
withhyperprolactinemic amenorrhea. (Reprinted from Fertility and
Sterility, 48,Rasmussen C, Bergh T, Wide L, Prolactin secretion and
menstrual functionafter long-term bromocriptine treatment, 550.
Copyright 1987, withpermission from The American Society for
Reproductive Medicine.)
Figure 39-13. Coronal CT scan of a woman with microadenoma 4
monthsafter bromocriptine therapy (5 mg per day). Clinical and
biologic results wereexcellent; pituitary gland is nearly normal,
with reconstruction of sellar floor.(From Bonneville JF, Poulignot
D, Cattin F, et al: Computed tomographicdemonstration of the
effects of bromocriptine on pituitary microadenoma size.Radiology
143:451, 1982.)
-
8/6/2019 39 mia a y Adenomas Pituitarios
12/16
74 REPRODUCTIVE ENDOCRINOLOGY AND INFERTILITY
Molitch and associates reported the results of a
1-yearprospective multicenter study of the use of bromocriptine
asprimary therapy for PRL-secreting macroadenomas in 27
indi-viduals. Bromocriptine dosage ranged from 5 to 12.5 mg
daily,
with 7.5 mg being the most frequent dose. PRL levels fell inall
individuals, and to 11% or less of pretreatment values in allbut
one. Of this group, two thirds had PRL levels decreaseto normal
during treatment. Tumor shrinkage was observed inall individuals,
being reduced by more than 50% in half thepatients and by about 50%
in an additional 20% of the studygroup. Visual field impairment
disappeared in 9 of the 10 indi-viduals with abnormalities. In two
thirds of the individualsreduction in tumor size occurred by 6
weeks, but in one thirdit was not evident until 6 months,
indicating there were bothrapid and slow responses of tumor to drug
treatment. Thereforeat least a 6-month trial of medical therapy is
warranted forindividuals with a macroadenoma.
Because of these excellent results, the poor initial results
ofoperation, and the high recurrence rates, these
investigatorsconcluded that bromocriptine should be used as the
initialmanagement of individuals with PRL-secreting
macroadenomas.
After maximal shrinkage of tumor, medical therapy can
becontinued or operative treatment used. The cost of
continuingbromocriptine treatment is considerable; it is
inconvenient totake medication several times a day, and some
individuals haveunpleasant side effects with the higher dosages
that may benecessary. Therefore some individuals prefer operative
treatment.If they elect to have an operation, the drug should be
continueduntil the time of operation to prevent tumor expansion.
Therates of success after operation are no different among
indi-viduals who received or did not receive bromocriptine before
theoperation.
Cabergoline is a long-acting dopamine receptor agonist.
Thisagent directly inhibits pituitary lactotrophs, thereby
decreasingPRL secretion. It is given orally in doses of 0.251.0 mg
twice
a week. The initial dose is half a 0.5-mg tablet twice a
week.Peak plasma levels occur in 2 to 3 hours, and this drug has
ahalf-life of 65 hours. Its slow elimination and long
half-lifeproduces a prolonged PRL-lowering effect. The initial dose
is0.25 mg twice weekly and the dosage may be increased at
inter-vals of 4 weeks to achieve a satisfactory response. In a
random-ized trial with bromocryptine, cabergoline lowered PRL
levelsto normal in 83% of women, induced ovulation in 72%,
andeliminated galactorrhea in 90%. The effectiveness of
cabergoline
was greater than that of bromocryptine. Adverse effects,
partic-ularly nausea, headaches, and dizziness, occurred with
bothagents but were less frequent, less severe, and of shorter
duration
with cabergoline. Therefore cabergoline is better tolerated
thanbromocryptine and has higher continuation rates. Recent
evi-
dence suggests that cabergoline is more effective in lowering
PRLthan bromocryptine. Even in patients who had been
treatedpreviously with bromocryptine, cabergoline has been found
tobe effective (Table 39-1).
Cabergoline has been compared with other agents in
effective-ness for reducing tumor size (see Table 39-1). It may be
concludedthat in women who have never been treated, cabergoline
iscurrently the agent of choice for reducing PRL levels and
effectingtumor shrinkage. It is recommended that after serum PRL
levelshave remained normal for 6 months cabergoline be
discontinuedto determine if the PRL levels stay low without
therapy.
Operative Approaches
Transsphenoidal microsurgical resection of prolactinoma hasbeen
widely used for therapy, and numerous reports of largeseries of
individuals treated by this technique have been pub-lished. In
general, transsphenoidal operations have minimalrisk, with a
mortality of less than 0.5%; however, the majority ofdeaths have
been reported to occur after treatment of macro-adenomas. The risk
of temporary postoperative diabetes insipidusis 10% to 40%, but the
risk of permanent diabetes insipidusand iatrogenic hypopituitarism
is less than 2%. The initial curerate, with normalization of PRL
levels and return of ovulation,is relatively high for microadenomas
(65% to 85%) and less so
with macroadenomas (20% to 40%). Vision can return to normalin
85% of patients with loss of acuity and visual field defects.
The initial cure rate is related to the pretreatment PRL
levels.Those tumors with levels less than 100 ng/mL have an
excellentprognosis (85%), and those with levels greater than 200
ng/mLhave a poor prognosis (35%). Operative treatment of tumors
in individuals older than 26 with amenorrhea for more than6
months carries a poorer prognosis than tumors in younger women with
a shorter duration of amenorrhea. Nevertheless,long-term follow-up
of patients after operation indicates thatlate recurrence of
hyperprolactinemia is common. Serri and col-leagues followed 28
women with microadenomas and 16 withmacroadenomas for 6 years after
operation. Although PRL levelsnormalized and menses resumed in 24
(85%) of those withmicroadenomas and 5 (31%) of those with
macroadenomas whohad a good initial postoperative response,
hyperprolactinemiarecurred in half of those with microadenoma and 4
of the5 with macroadenomas after a mean period of 4 and 2.5
years,respectively (Fig. 39-14). There was no significant
differencein recurrence rates for those who conceived and those
who
did not. Rodman and coworkers reported a lower
postoperativerecurrence rate (about 20% for both microadenomas
andmacroadenomas) following initial cure rates of 85% and
37%,respectively. The risk of recurrence in both series appeared to
berelated to the immediate postoperative PRL levels, being
greaterin persons with a PRL level greater than 10 ng/mL.
Overall it can be concluded that after surgery, recurrencerates
for micro- or macroadenoma are similar (21% and
19.8%,respectively). Long-term surgical cure rates are 58% of
micro-adenomas and only 26% macroadenomas using a normal PRLlevel
as a criterion.
Table 39-1 Comparison of Efficacy of Dopamine
Agonists in Affecting Tumor Size Reduction*
TUMOR SIZE REDUCTION
Dopamine Number NoAgonist of Cases >50% 25%50%
-
8/6/2019 39 mia a y Adenomas Pituitarios
13/16
HYPERPROLACTINEMIA, GALACTORRHEA, AND PITUITARY ADENOMAS
Because of the good results with medical therapy, surgery
isrecommended only for women with macroadenoma who failto respond
to medical therapy or have poor compliance with thisregimen. It is
best to reduce the size of macroadenomas maxi-mally with
bromocriptine before surgical removal of theseextrasellar
tumors.
Radiation Therapy
External radiation with cobalt, proton beam, or
heavy-particletherapy and brachytherapy with yttrium-90 rods
implanted inthe pituitary have all been used to treat macroadenomas
butare not the primary mode of treatment. Results of such
therapy
have been inconsistent, and there is a delay of several
monthsbetween treatment and resumption of ovulation.
Furthermore,damage to normal pituitary tissue occurs, frequently
leading toabnormal anterior pituitary function as well as diabetes
insipidus.Damage to the optic nerves may also occur. Thus
radiationtherapy should be used only as adjunctive management
followingincomplete operative removal of large tumors.
Pregnancy
Many women with hyperprolactinemia with or withoutadenomas wish
to become pregnant. A small percentage of these
women conceive spontaneously, but most require treatment
to induce ovulation. Barbieri and Ryan compiled a
literaturereview of the pregnancy courses of 275 women with
adenomas,the majority of whose conceptions had been induced by
bromo-criptine. They reported that of 215 women with
microprolac-tinomas, less than 1% had changes in visual fields,
radiologicevidence of tumor enlargement, or neurologic signs.
About5% developed headaches during pregnancy. Of 60 women
withmacroprolactinomas, 20% developed adverse changes in
visualfields and polytomographic or neurologic signs during
preg-nancy, and some of them required bromocriptine or
operativetreatment during pregnancy or shortly postpartum.
Overall,
although only 1.4% of women with microadenomas have symp-toms
during pregnancy, 24.4% of women with macroadenomashave symptoms.
However, only about 3% of women withmacroadenomas have symptoms if
they are treated prior topregnancy. For this reason excision of
macroprolactinomasbefore pregnancy has been recommended in some
cases. Never-theless, because pituitary function is usually
diminished afteroperation, induction of ovulation must be performed
with com-plicated and expensive gonadotropin treatment.
Bromocriptinetreatment does not interfere with pituitary function
and is thusthe therapy of choice for women with macroadenomas who
wishto conceive. Continuous bromocriptine treatment
throughoutpregnancy for women with macroadenomas has been
recom-mended by some, because with this therapy visual
disturbancesare rare. Despite a lowering of PRL levels, there is no
effect onplacental hormone production, and pregnancy outcome
doesnot appear to be affected.
Nevertheless, since bromocriptine crosses the placenta
andsuppresses fetal PRL levels, its long-term effects on the
newbornare unknown. Therefore it is now advised that women
withmacroadenomas discontinue the drug after conception (as is
thecase for those with microadenomas) and have therapy
reinitiatedif and when symptoms of visual disturbance or severe
headachesoccur. Most women who conceive after bromocriptine
treat-ment have ingested the drug for a few weeks after
conception.In a review of 1410 such pregnancies compiled by Turkalj
andassociates there was a spontaneous abortion rate of 11%,
ectopicpregnancy rate of 0.7%, and twin pregnancy rate of 1.8%.
Theincidence of minor (2.5%) and major (1%) congenital defects
was similar to pregnancy outcomes in untreated populationsof
women. The mean amount of drug ingested and durationof
postconception treatment were similar in mothers who hadnormal
children and those with defects. Thus ingestion ofbromocriptine
during pregnancy does not appear to increase therisk of congenital
abnormalities, spontaneous abortion, or multi-
ple gestation. Postnatal surveillance of more than 200
childrenborn in this series has revealed no adverse effects to
date.Ruiz-Velasco and Tolis compiled the obstetric histories of
nearly 2000 pregnancies occurring in hyperprolactinemic
womenthat have been reported in the literature. Most of these
preg-nancies were induced with bromocriptine. There was a
full-termdelivery rate of 85%, an abortion rate of 11%, a
prematurityrate of 2%, and a multiple pregnancy rate of 1.2%.
AlthoughPRL levels increased during pregnancy, after delivery the
levelsreturned to pretreatment values in about 85%. A
postpartumincrease over pretreatment levels was uncommon (3%), and
PRLlevels returned to normal in 13%. Likewise, among women whohad
postpartum radiologic sellar examination, 84% showedno change, 9%
improved, and 7% worsened. Thus stopping
treatment during pregnancy only occasionally results in
tumorgrowth. It is advised that women with macroadenomas
havemonthly visual field examination and neurologic testing
duringpregnancy, but this is probably unnecessary for women
withmicroadenomas unless they develop symptoms of headache orvisual
disturbances.
Following delivery, breast-feeding may be initiated
withoutadverse effects on the tumors. Godo and associates
reportedthat use of bromocriptine before conception and during
preg-nancy did not affect the incidence of persistent lactation
fol-lowing discontinuation of nursing. The incidence of
menstrual
Figure 39-14. Cumulative recurrence rate in patients with
microprolactinoma(group 1) or macroprolactinoma (group 2) after
initially successful operation.Figures in parentheses indicate
numbers of patients who were seen at eachyearly interval. (From
Serri O, Rasio E, Beauregard H, et al: Recurrence
ofhyperprolactinemia after selective transsphenoidal adenomectomy
in women
with prolactinoma. N Engl J Med 309:280, 1983. Copyright
1983Massachusetts Medical Society. All rights reserved.)
-
8/6/2019 39 mia a y Adenomas Pituitarios
14/16
76 REPRODUCTIVE ENDOCRINOLOGY AND INFERTILITY
abnormalities and degree of galactorrhea were usually similar
tothe state that existed before starting bromocriptine
therapy.Therefore, following completion of nursing, as well as
for
women who do not breast-feed at all, bromocriptine should
beingested for 2 to 3 weeks and then discontinued. At that
timeserum PRL measurement should be performed and
treatmentreinstituted according to the findings.
Women with Hyperprolactinemia Who Do Not Wishto Conceive
For women who do not wish to conceive and for whomgalactorrhea
is not a problem, no therapy is necessary unlessestrogen levels are
low. Thus, to prevent osteoporosis in thisclinical situation,
estrogenprogestin hormone replacement or
oral contraceptives should be given regardless of whether
anadenoma is present. Long-term evaluation of all women
withhyperprolactinemia should be performed. Unless a macro-adenoma
is present, measurement of PRL levels once a year isadvisable.
Repeat imaging studies are unnecessary unless symp-toms of
headaches or visual disturbances occur or PRL levelsincrease
substantially. If bromocriptine therapy is used, tempo-rary
discontinuation of medication every year is advisable, withPRL
measurement 6 weeks later. If the level is normal, repeatPRL
measurements should be made semiannually. If the level isincreased,
therapy may be reinitiated. During medical treatmentof
macroadenomas, MRI or CT and visual field examinationshould be
performed every 6 months to determine the effectof medication on
the tumor. At these intervals a decision canbe made about whether
to continue long-term bromocriptinetreatment or to remove the tumor
surgically.
Estrogen stimulates PRL release but blocks its action at the
receptor in the breast. Physiologic stimuli for PRL release
include breast and
nipple palpation, exercise, stress, sleep, and the
noondaymeal.
The main symptoms of hyperprolactinemia are galactorrheaand
amenorrhea, the latter caused by alterations in
normalgonadotropin-releasing hormone (GnRH) release.
Hyperprolactinemia is present in 15% of all anovulatorywomen and
20% of women with amenorrhea of undeter-mined cause.
About 60% of all women with galactorrhea have
hyper-prolactinemia, but almost 90% of women with
galactorrhea,amenorrhea, and low estrogen levels have
hyperpro-lactinemia.
Pathologic causes of hyperprolactinemia include pharma-cologic
agents (tranquilizers, narcotics, and antihyperten-sive drugs),
hypothyroidism, chronic renal disease, chronicneurostimulation of
the breast, hypothalamic disease, andpituitary tumors
(prolactinoma, acromegaly, Cushingsdisease).
About 3% to 5% of individuals with hyperprolactinemiahave
hypothyroidism.
About 80% of all pituitary tumors secrete PRL. About 25% of
individuals with acromegaly and 10% of
those with Cushings disease have hyperprolactinemia. About 10%
of individuals with an enlarged sella have the
empty sella syndrome. Autopsy studies reveal that prolactinomas
are present in
about 10% of the population. About 50% of women with
hyperprolactinemia will have
a prolactinoma, as will nearly all of those with PRL
levelsgreater than 200 ng/mL.
About 20% of women with galactorrhea and 35% of thosewith
amenorrhea and galactorrhea have prolactinomas.
About 70% of women with hyperprolactinemia, galactor-rhea, and
amenorrhea with low estrogen levels will have aprolactinoma.
Women with regular menses, galactorrhea, and normal PRL
levels do not have prolactinomas. About 13% of women with
prolactinomas do not have
galactorrhea. Most macroadenomas enlarge with time; nearly all
micro-
denomas do not. The initial operative cure rate for
microadenomas is about
80% and for macroadenomas 30%, but the long-termrecurrence rate
is at least 20% for each.
Most frequent side effects of bromocriptine are
orthostatichypotension, nausea, and vomiting.
In women with hyperprolactinemia and no
macroadenoma,bromocriptine treatment returns PRL levels to normal
in90%, induces ovulatory cycles in 80%, and eradicatesgalactorrhea
in 60%.
After 1 year of bromocriptine treatment, PRL levels remainnormal
in 11% of women with microadenomas; after2 years permanent
remission reaches 22%. After longer use,remissions of 50% have been
reported.
Bromocriptine shrinks 80% to 90% of macroadenomas. When
pregnancy occurs in women with microadenomas,
less than 1% have visual field changes, tumor enlargement,or
neurologic signs; about 20% of women with macro-adenomas have such
adverse changes.
Pregnancy increases the likelihood that PRL levels willdecrease
or become normal over time.
Estrogen replacement therapy or oral contraceptives willnot
stimulate growth of PRL-secreting microadenomas andcan be used for
therapy of hyperprolactinemia and hypo-estrogenism.
Bromocriptine induction of pregnancy is not associated withan
increased risk of congenital abnormalities, spontaneousabortion, or
multiple gestation.
About 85% of patients with prolactinomas have no changein PRL
levels or tumor size after delivery, 10% improve, and5% worsen.
The most frequent cause of mildly elevated PRL levels
isstress.
KEY POINTS
-
8/6/2019 39 mia a y Adenomas Pituitarios
15/16
HYPERPROLACTINEMIA, GALACTORRHEA, AND PITUITARY ADENOMAS
The best modality to diagnose pituitary adenomas or emptysella
syndrome is MRI.
The natural history of nearly all microprolactinomas is tostay
the same size, with adverse menstrual problems
resolvingspontaneously in about one fourth of patients.
Surgical treatment of prolactinomas is recommended onlyfor
patients who fail to respond or do not comply withmedical
management.
For women who develop side effects with oral
bromocriptine,vaginal administration usually alleviates the
problem.
Cabergoline appears to be more effective and better
toleratedthan bromocriptine.
KEY POINTS Continued
B I B L I O G R A P H Y
Abd El-Hamid MW, Joplin EF, Lewis PD: Incidentally found small
pituitaryadenomas may have no effect on fertility. Acta Endocrinol
(Copenh)117:361, 1988.
Ampudia X, Pulig-Domingo M, Schwarzstein D, et al: Outcome and
long-term effects of pregnancy in women with hyperprolactinaemia.
Eur JObstet Gynecol Reprod Biol 46:101, 1992.
Asa S: Pathology of pituitary adenomas. Endocrinol Metab Clin
North Am
28:13, 1999.Bckstrm CT, McNeilly AS, Leash RM, et al: Pulsatile
secretion of LH, FSH,prolactin oestradiol and progesterone during
the human menstrual cycle.Clin Endocrinol 17:29, 1982.
Barbieri RL, Ryan KJ: Bromocriptine: endocrine pharmacology and
therapeuticapplications. Fertil Steril 39:727, 1983.
Biller BMK, Molitch ME, Vance ML, Cannistraro KB, et al:
Treatment ofprolactin-secreting macroadenomas with the once-weekly
dopamine agonistcabergoline. J Clin Endocrinol Metab 81:2338,
1996.
Bonneville JF, Poulignot D, Cattin F, et al: Computed
tomographicdemonstration of the effects of bromocriptine on
pituitary microadenomasize. Radiology 143:451, 1982.
Burrow GN, Wortzman G, Rewcastle NB, et al: Microadenomas of
thepituitary and abnormal sellar tomograms in an unselected autopsy
series.N Engl J Med 304:156, 1981.
Ciccarelli E, Giusti M, Miola C, et al: Effectiveness and
tolerability of long-term treatment with cabergoline, a new
long-lasting ergoline derivative, in
hyperprolactinemic patients. J Clin Endocrinol Metab 69:725,
1989.Ciccarelli E, Miola C, Avateneo T, et al: Long-term treatment
with a newrepeatable injectable form of bromocriptine, Parlodel
LAR, in patients withtumorous hyperprolactinemia. Fertil Steril
52:930, 1989.
Corenblum B, Donovan L: The safety of physiological estrogen
plus progestinreplacement therapy and with oral contraceptive
therapy in women withpathological hyperprolactinemia. Fertil Steril
59:671, 1993.
Corenblum B, Taylor PJ: Long-term follow-up of
hyperprolactinemic womentreated with bromocriptine. Fertil Steril
40:596, 1983.
Crosignani PG, Mattei AM, Scarduelli C, et al: Is pregnancy the
best treatmentfor hyperprolactinemia? Hum Reprod 4:910, 1989.
Crosignani PG, Mattei AM, Severini V, et al: Long-term effects
of time,medical treatment and pregnancy in 176 hyperprolactinemic
women.Eur J Obstet Gynecol Reprod Biol 44:175, 1992.
Davajan V, Kletzky O, March CM, et al: The significance of
galactorrhea inpatients with normal menses, oligomenorrhea, and
secondary amenorrhea.
Am J Obstet Gynecol 130:894, 1978.
Fahy UM, Foster PA, Torode HW, et al: The effect of combined
estrogen/progestogen treatment in women with hyperprolactinemic
amenorrhea.Gynecol Endocrinol 6:183, 1992.
Gharib H, Frey HM, Laws ER Jr, et al: Coexistent primary empty
sellasyndrome and hyperprolactinemia: report of 11 cases. Arch
Intern Med143:1383, 1983.
Ginsburg J, Hardiman P, Thomas M: Vaginal bromocriptine:
clinical andbiochemical effects. Gynecol Endocrinol 6:119,
1992.
Godo G, Kolosziar S, Szilagyi I, et al: Experience related to
pregnancy,lactation, and the after-weaning condition of
hyperprolactinemic patientstreated with bromocriptine. Fertil
Steril 51:529, 1989.
Kleinberg DL, Noel GL, Frantz AG: Galactorrhea: a study of 235
cases,including 48 with pituitary tumors. N Engl J Med 296:589,
1977.
Kletsky OA, Vermesh M: Effectiveness of vaginal bromocriptine in
treatingwomen with hyperprolactinemia. Fertil Steril 51:269,
1989.
Klibanski A. Further evidence for a somatic mutation theory in
thepathogenesis of hyman pituitary tumors. J Clin Endocrinol
Metab71;1415, 1990.
Koppelman MCS, Jaffe MJ, Rieth KG, et al: Hyperprolactinemia,
amenorrhea,and galactorrhea: A retrospective assessment of 25
cases. Ann Intern Med100:115, 1984.
March CM, Kletzky OA, Davajan V, et al: Longitudinal evaluation
of patients
with untreated prolactin-secreting pituitary adenomas. Am J
ObstetGynecol 139:835, 1981.Martin TL, Kim M, Malarkey WB: The
natural history of idiopathic
hyperprolactinemia. J Clin Endocrinol Metab 60:855, 1985.Melmed
S: Pathogenesis of pituitary tumors. Endocrinol Metab Clin
North
Am 28:1, 1999.Molitch ME, Elton RL, Blackwell RE, et al:
Bromocriptine as primary therapy
for prolactin-secreting macroadenomas: Results of a prospective
multicenterstudy. J Clin Endocrinol Metab 60:698, 1985.
Molitch ME: Pituitary incidentalomas. Endocrinol Metab Clin
North Am26:727, 1997.
Moriondo P, Travaglini P, Nissim M, et al: Bromocriptine
treatment ofmicroprolactinomas: Evidence of stable prolactin
decrease after drug
withdrawal. J Clin Endocrinol Metab 60:764, 1985.Mornex R,
Hugues B: Remission of hyperprolactinemia after pregnancy.
N Engl J Med 324:60, 1991.Muneyyirci-Delale O, Goldstein D,
Reyes FI, et al: Diagnosis of stress-related
hyperprolactinemia: evaluation of the hyperprolactinemia rest
test. NYState J Med 89:205, 1989.Rasmussen C, Bergh T, Wide L:
Prolactin secretion and menstrual function
after long-term bromocriptine treatment. Fertil Steril 48:550,
1987.Rasmussen C, Bergh T, Nillius SJ, and Wide L: Return of
menstruation and
normalization of prolactin in hyperprolactinemic women
withbromocriptine-induced pregnancy. Fertil Steril 44:31, 1985.
Rodman EF, Molitch ME, Post KD, et al: Long-term follow-up of
transsphenoidalselective adenomectomy for prolactinoma. JAMA
252:921, 1984.
Ruiz-Velasco V, Tolis G: Pregnancy in hyperprolactinemic women.
Fertil Steril41:793, 1984.
Schlechte J, Dolan K, Sherman B, et al: The natural history of
untreatedhyperprolactinemia: A prospective analysis. J Clin
Endocrinol Metab68:412, 1989.
Serri O, Rasio E, Beauregard H, et al: Recurrence of
hyperprolactinemia afterselective transsphenoidal adenomectomy in
women with prolactinoma.N Engl J Med 309:280, 1983.
Shoupe D, Mishell DR Jr: Hyperprolactinemia: Diagnosis and
treatment. InLobo RA, Mishell DR Jr, Paulson RJ, Shoupe D (eds):
Mishells Textbookof Infertility, Contraception and Reproductive
Endocrinology, 4th ed.Blackwell Scientific Publications, Cambridge,
MA, 1997.
Sisam DA, Sheehan JP, Sheeler LR: The natural history of
untreatedmicroprolactinomas. Fertil Steril 48:67, 1987.
Slujmer AV, Lappohn RE: Clinical history and outcome of 59
patients withidiopathic hyperprolactinemia. Fertil Steril 50:72,
1992.
Stein AL, Levenick MN, Kletzky OA: Computer tomography versus
magneticresonance imaging for the evaluation of suspected pituitary
adenomas.Obstet Gynecol 73:996, 1989.
Testa G, Vegetti W, Motta T, et al: Two-year treatment with oral
contraceptivesin hyperprolactinemic patients. Contraception 58:69,
1998.
-
8/6/2019 39 mia a y Adenomas Pituitarios
16/16
78 REPRODUCTIVE ENDOCRINOLOGY AND INFERTILITY
Turkalj I, Brain P, Krupp P: Surveillance of bromocriptine in
pregnancy.JAMA 247:1589, 1982.
Vermesh M, Fossum GT, Kletzky OA: Vaginal bromocriptine:
Pharmacologyand effect on serum prolactin in normal women. Obstet
Gynecol 72:693,1988.
Webster J, Piscitelli G, Polli A, Ferrari CI, et al: A
comparison of cabergolineand bromocriptine in the treatment of
hyperprolactinemic amenorrhea.N Engl J Med 331:904, 1994.