A Fresh Outlook on Osteoarthritis and Physical Capabilities. Randy Raugh, PT, DPT. Osteoarthritis (OA). 37.4% > age 60 with knee OA 2030 - 25% of Americans Leading cause of immobility/disability > 60 Symptoms: pain, stiffness, noisy and local swelling “Wear and tear?” CDC: - PowerPoint PPT Presentation
A Fresh Outlook on Osteoarthritis and Physical Capabilities
A Fresh Outlook on Osteoarthritis and Physical CapabilitiesRandy
Raugh, PT, DPT1Osteoarthritis (OA)37.4% > age 60 with knee
OA2030 - 25% of AmericansLeading cause of immobility/disability
> 60Symptoms: pain, stiffness, noisy and local swellingWear and
tear?CDC: Incurable, progressive and degenerative???focal and
progressive loss of the hyaline cartilage of joints, underlying
bony changes.A disease or a Mechanical problem?A cartilage
problem?2CDCOA knee: 1 of 5 leading causes of disability among
non-institutionalized adults. ~ 80% of patients - some degree of
movement limitation 25% cannot perform major activities of daily
living 11% knee OA need help with personal care14% require help
with routine needs.~ 40% of adults with knee OA reported their
health poor or fair.1999, knee OA - more than 13 days of lost work
due to health problems3Excessive stress to entire jointArticular
(hyaline) cartilageSynovial liningBone beneath
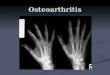
cartilageLigamentsDiagnosed by X-Rays and symptomsJoint space
narrowingSclerosis (increased bone density)Spurs, lipping
4
Normal kneeOsteoarthritic kneeX-Rays of OA joints5X-Rays dont
correlate well to painDecreased space: meniscus or articular
cartilageCartilage: no nerves = no pain X-Rays activityFear/anxiety
= activityUntreated OA lesions fared no worseWiduckowski et al
(2009) 2-4 cm lesions w/out tx no worse in 13 17 year
follow-upSurgical debridement of OA no better than physical
therapy/medication Risberg et al; Kirkley et al; Moseley et al
6Risks for OAExcess weight For OA riskNot for progression unless
misalignments Trauma, surgery, etc. NO
movementImmobilizationSedentary lifestyleRepetitive, excessive
twistingRapid impact activitiesExcessive Joint
flexibilityMisalignments/movement impairments
7Articular cartilageHyaline cartilage bluish, opalescent,
glassy, homogenousThinner with ageNo blood vessels / no nervesHeals
very slowlyNo pain80% water-filled matrixMust have dynamic (cyclic)
loading to move nutrients in/damaged cells/waste products out.
8Functions of articular cartilageAbsorb and distribute
compressive forcesLike a gel bicycle seatLying down (~0 compressive
force) - kneeJumping (~24 x body weight) kneeFlow of fluid through
porous matrix, away from force.Stiffer to higher loadsShock
absorption (deformation of cancellous bone most, then subchondral
bone and slightly cartilage (1-3%)Slippery 500 to 2000 x slipperier
than ice on ice.Synovial fluid consistency like egg whiteHelps
cartilage resist sliding forces
9
Tensile stress-strain curve of articular cartilage10TENSILE
FORCES
The non-linear response of articular cartilage to compressive
force on fluid flow through the matrix11Compressive
forcesStretching (tensile) forces
Compressive forces
Sliding (shear) forces
Types of physical stresses encountered by articular
cartilage
12Compressive loadsShort termEckstein et al Eckstein et al
(2005) MRI before/after deep knee bends, squatting, walking,
cycling decreased thickness 5.0 to 8.8%After 100 knee bends, return
to original thickness took 90 minutes. Long term changesInadequate
load/immobilizationJortikka et al (1997) 11 weeks of immobilization
PG in beagle knees did not fully recover after 50 weeks or
remobilization.Hinterwimmer et al (2004) 20 patients mean knee
cartilage thickness after partial LE immobilization for ankle fx x
7 weeks. Vanwanseele et al (2002) after 2 years post-injury, spinal
cord patients cartilage thickness patella 23%, medial tibia 25%,
lateral tibia 19%.
13CompressionExcess load = cartilageLow compression synthesis;
high decreased it. Weak quadriceps (Youssef et al, 2009) saline or
botox injected into quads.Segal et al (2010) weak quads correlated
to JSN in womenSlemenda et al (1997)- each 10-lb/ft increase knee
extensor strength = 20% knee OAMikesky et al (2006) 221 older
adults, strength vs ROM Strength group showed slower rate of JSN at
30 months.Excess weight increases load and riskFelson et al in
Framingham Study (1992), wt loss risk of knee OASharma et al (2000)
BMI correlated more with risk than progression except in bowed
legs
14Shear (sliding force)Wong et al (2008) cadaveric osteochondral
cores subjected in vitro to shear with 15% compression.More
irregular surface had 5 x > shear than normal cartilage. More
irregular surface = > friction = more degradation with
shear)Shear more inflammation, production of degrading enzymes,
etc. Shear more common than excess compression with people over
60?Clinically patients often report more pain with movements that
increase shear Twisting and bending knees sidewaysLess pain with
movement impairment corrections
15Causes of compression problemsInadequate (rhythmic)
compressionI better not wear it out fasterSedentary lifestyleStatic
postures Prolonged standing Excess compressionExcess body
weightHigh impact or rapid loading activitiesWeak muscles (or
muscles untrained for faster loads)
16Causes of excessive shearActivities which twist joints with
compressionSkiingTennisDancingRunning with flexible kneesPoor
movement patternsSit stand with knees in/outUp/Down steps with
hip/knees in/outPoor body mechanics with activities
17 TISSUE RESPONSE TO PHYSICAL STRESSMore physical
stressHealthierOptimum HealthCell deathCell death18General advice
about joint careAvoid static postures especially bad ones move!No
pain, no gain = no brain. Avoid joint noise if possibleMaintain
adequate strengthStretch muscles, not jointsHealthy weightAll
joints need regular movement to feel their best.If you cant find
comfort, seek helpStart with conservative care (physical therapy)If
no improvement in 6 8 visits, change therapistsTreat it as a
mechanical problem19Feet are the foundationDo not tolerate
uncomfortable shoes ever!Maintain healthy weightAlternate sport
shoes each dayShock absorption is slow to recover after
compressionChoose activities that dont hurt.Walking is better than
standingFoot exercises? 20Knees to last a lifetimeHealthy
weightAvoid unnecessary twistingBiking? Avoid breaststroke, scissor
or frog kicks in swimmingFocus on alignmentMaintain strong legs and
HIPSWear proper shoes
21Hip, hip hooray!IF flexible, avoid extreme stretches for
hipAvoid performing splits, race-walking, extreme yoga asanas that
take hips back beyond neutral with pelvicMaintain strong buttock
and hip musclesAvoid becoming hamstring dominantJogging worse than
runningIF you have very stiff hips with OA, stretch the hips and
strengthen them too22Spine painSeek help if:Bowel/bladder
problemsDecreased strength in lower extremity or upper
extremityTingling/numbness in genital regionSensory changes in both
sides of UE or LEStart with conservative care proceed slowly on
that route.But my MRI showed that23
24
2526
Spine:Spine pain is a mechanical problem tooPostureExercise
Avoid heavy liftingNever bend and lift or worse, bend, twist and
liftFor heavy objects the Raugh Method
27ShouldersAllow your shoulders to rise when you reach.Lift in
line with the shoulder bladesDont keep them down (for your neck
too).28Questions?29