Embed Size (px)
Citation preview

Clinical Decision Making in Therapeutic Exercise Prescription
Speaker(s): Wendy Anemaet, PT, PhD, GCS; Amy Hammerich, PT, DPT, PhD, OCS Session Type: Educational Sessions Session Level: Multiple Level
Preconference Course February 16‐17, 2016 8:00 am – 5:30 pm Location: Hilton Anaheim, Salinas
1.6 CEUs Preconference Course Certificates Preconference CEU certificates are accessible in the APTA Learning Center. In order to earn CEUs for the preconference course, participants must pass a multiple‐choice assessment with a score of 70% or better. The preconference assessment can be accessed at the conclusion of CSM in the APTA Learning Center. To access your assessment and certificate, follow these easy steps:
o Go to APTA Learning Center and login. Enter your email, member number or user ID. Use the "forgot your password" link if you need to reset your password.
o Click on the "My Learning Activities/My Courses" tab in the top navigation menu, and find your preconference course.
o Click "Start" next to the course title. Follow the directions to take the assessment and print your CEU certificate.
If you require additional assistance related to your CSM attendance, please contact APTA’s Member Services: 800/999‐2782, ext. 3395, M‐F, 8:30 am to 6:00 pm, ET, or email [email protected].
This information is the property of the author(s) and should not be copied or otherwise used without the express written permission of the author(s).
Home Health Section of the American Physical Therapy Association
www.homehealthsection.org
Page 1 of 104 total pages

1/5/2016
1
Clinical Decision Making in Therapeutic Exercise
Prescription
Wendy K. Anemaet, PT, DPT, PhD, GCS, CWS, GTC, COS‐C
Amy S. Hammerich, PT, DPT, PhD, OCS
1
Objectives
• Cite indications and contraindications for specific types of therapeutic exercise
• Describe a framework for clinical decision making in exercise prescription that includes the patient’s health condition, body structure and function, activity goal, and contextual factors
• Cite evidence for therapeutic exercise with the older adult
• Determine the appropriate type of therapeutic exercise and best parameters to target specific patient problems including pain, inflammation, decreased mobility, instability, lack of motor control, weakness, power loss, endurance deficits, balance issues, and functional limitations
• Problem solve exercise prescriptions for a specific patient 2

1/5/2016
2
Exercise
• Therapeutic exercise is the systematicperformance or execution of planned physical movements, postures, or activities intended to enable the patient/client to:
– remediate or prevent impairments
– enhance function
– reduce risk
– optimize overall health
– enhance fitness, physical activity and well‐being (physical and psychosocial)
3
Therapists select, prescribe, and implement exercise activities when the examination findings, diagnosis,
and prognosis indicate the need to:
• enhance bone density
• enhance breathing
• enhance or maintain physical performance
• enhance performance in ADL and IADL
• improve safety
• increase aerobic capacity/ endurance
• increase muscle strength, power, hypertrophy, and endurance
• enhance postural control and relaxation
• increase sensory awareness
• increase tolerance to activity
• prevent or remediate impairments, functional limitations, or disabilities to improve physical function
• enhance health, wellness, and fitness
• reduce complications, pain, restriction, and swelling
• reduce risk and increase safety during activity performance 4

1/5/2016
3
Therapeutic Exercise Includes:
• Aerobic and endurance conditioning and reconditioning
• Agility training and balance training
• Body mechanics training
• Breathing exercises
• Coordination exercises
• Developmental activities training
• Gait and locomotion training
• Muscle lengthening/flexibility
• Neuromotor development activities training
• Neuromuscular education or reeducation
• Postural stabilization and training
• Range‐of‐motion exercises and soft tissue stretching
• Relaxation exercises
• Muscle performance exercises– Strength
– Power
– Endurance
– Hypertrophy5
HOW DO YOU DECIDE ON AN EXERCISE?
6

1/5/2016
4
Exercise Framework
7
Tissue Healing
Mobility
Performance Initiation, Motor Control & Stabilization
Performance Improvement
Advanced Skill, Coordination, and Agility
Where is the patient now?
HOW DO YOU DOSE AN EXERCISE PRESCRIPTION?
Program should provide the proper amount of the right activities to attain maximal benefit at the lowest risk
8

1/5/2016
5
Need to Understand:
Principles of Exercise
• Load and Overload
• Specificity
• Variation
9
LOAD AND OVERLOAD
• Load is the amount of stress placed on the body or system during exercise
• Appropriate load will determine how successful is your outcome
• Overload is gradually increasing stress placed upon the body or system during exercise training
• By placing increasing demands on the body, greater force must be generated resulting in adaptive responses
10

1/5/2016
6
OVERLOAD
• Can be accomplished by:
• Increasing load
• Increasing sets
• Altering repetition speed
• Altering rest periods
• Altering repetitions
• Combination of two or more of these
11
SPECIFICITY
• Training adaptations are specific to the stimulus applied
• Exercise prescription should be designed to target specific goals
12

1/5/2016
7
SPECIFICITY
• System
• Muscle actions or muscle groups
• Speed
• Range of motion
• Intensity
• Volume13
VARIATION
• Alteration in one or more program variables over time
• Allows for optimal training stimulus
• Can be accomplished by changing intensity, velocity, rest periods, etc.
• Lack of variation may lead to a plateau of physiological and neurophysiological adaptations
14

1/5/2016
8
Need to Understand Parameters
• Frequency– # sessions / period of time
• Intensity
– assisted, resisted
– percentage of max
– reps/sets/holds
• Time (duration)
– Within session time: time of reps/rest, time total for session
– Duration in days, weeks, months
• Type (isometric, isotonic, balance, cardiovascular, etc)
15
Need to Understand Other Parameters
• Position
– body position
– biomechanical placement
• Sequence
– What exercises first? Last?
• Learning abilities
• Environment
• Feedback
16

1/5/2016
9
Exercise Framework
17
Tissue Healing
Mobility
Performance Initiation, Motor Control & Stabilization
Performance Improvement
Advanced Skill, Coordination, and Agility
Stages of Tissue Healing
• Acute tissue healing
–Acute injury/post operative
– Inflammation
• Repair
–Proliferation
• Remodeling
18

1/5/2016
10
What is acute tissue healing?• Acute inflammatory response (24‐72 hours) removes necrotic tissue
• Healing must replace tissue defect with either: – Regeneration (growth of new tissue)
– Repair (connective tissue scar)
• Macrophages and neutrophils remove debris, clean injured area, and signal fibroblasts to the area
• Repair begins in 24 hours with fibroblast migration from viable tissue at edges of wound
• Fibroblasts proliferate and synthesize proteins (proteoglycans, elastin, collagen)
19
Tissue Healing in Skeletal MuscleMuscle regeneration depends on:
• The extent of the injury– If sarcolemma sheaths are intact (basement membrane & endomysium) muscle cells regenerate in sheaths
– If basement membrane damaged, then repair occurs with connective tissue scar (structural integrity but impairs function)
• The inflammatory phase– Amount and type of macrophages
• The age of the person– Number of satellite cells
– Slowed phagocytosis
– Less Notch signaling and more Wnt signaling
– Fewer growth factors20

1/5/2016
11
Tissue Healing in Skeletal Muscle
• Clinical implications
– Control inflammation to minimize fibrosis
• Light contraction
• Midrange passive, active, and active assisted ROM
– Protect the newly regenerating muscle cells
• No high stresses/strains
• Let pain and inflammation be your guide
– Facilitate muscle function
• Gradually progressing forces21
Tissue Healing in Bone• Primarily regeneration and remodeling (no permanent scar)
• Immediate vascular response
• Precursor cells for chondrocytes come from periosteum, bone marrow, endosteum
• Chondroblasts from periosteal cells proximal to fracture site form hyaline cartilage
• Osteoblasts from periosteal cells distal to fracture site form woven bone
• The hyaline cartilage and woven bone meet to form callus
22

1/5/2016
12
Tissue Healing in Bone
• Reparative phase (2‐6 weeks)
– Soft callus hard callus
• Hyaline cartilage and woven bone is replaced with lamellar bone/trabecular bone
• Near full strength when all hyaline cartilage and woven bone is replaced with trabecular bone
• Remodeling Phase (up to 5 years)
– Osteoclasts resorb trabecular bone
– Howship’s lacuna form
– Lacuna filled in with compact bone
23
Tissue Healing in Bone
• Clinical Implications
–Protect the fracture site until callus formation (2 weeks)
–Provide controlled stress on bone during reparative phase (2‐6 weeks)
– Full activity after hard callus formation
24

1/5/2016
13
Tissue Healing of Tendons/Ligaments
• Repair
• Heal by proliferation of tenoblasts from cut ends of tendon or vasculature and proliferation of fibroblasts from neighboring tissue
• Capillary sprouts allow fibroblasts to secrete collagen which forms into fibrils, in 2 weeks these fibrils have some strength – Bands of fibrous connective tissue (78% water, 20% collagen, 2%
glycosaminoglycans)
– Composition allows viscoelastic processes
• Final maturation occurs at about 10 weeks
• Complete healing at about 1 year25
Tissue Healing in Tendons/Ligaments
• Clinical implications
– Immobilize or decrease stress during the initial 2 week period
–Movement and very gradually increasing loads from 2 weeks through 10 weeks
–Risk for re‐injury up through about 1 year if loads are too intense
26

1/5/2016
14
Tissue Healing in Cartilage
• Articular cartilage is avascular• No vascular response if there is isolated cartilage damage
• Chondrocytes can divide
• Chondrocytes can increase proteoglycan production
• Healing will be slow
• Best healing will occur at the periphery of the cartilage
• Amount of healing depends on depth of injury—the deeper the injury the better the healing
27
Tissue Healing in Cartilage
• Clinical implications
–May never heal or at best will take a long time (months to years) to heal
–Unloaded motion aids in healing because it stimulates synovial fluid
28

1/5/2016
15
Assessing Tissue Healing
• Pain
– VAS
– NPRS
– Disease specific scales
• Inflammation
– Temperature with skin thermometer
– Girth
– Rubor
29
Exercise for Tissue Healing
30

1/5/2016
16
Exercises for Tissue Healing
• Light muscle contractions “flickers”
– Turn muscle on and off quickly
– 1 second or less on/off time
• Short contraction time limits number of motor units activated in motor unit pool
– Cue < 50% of 1RM or maximum
• Use words like “light” contraction
• PT should be able to palpate muscle activity but not see muscle shorten
– Isometric or small mid‐range contraction
– High volume, low load, high rest time
• Muscle performance is not goal31
Is Muscle Contraction Beneficial for Tissue Healing?
• Mechanotransduction
– Deformation of muscle links the mechanical forces with biochemical signals
• Parameters to consider:• Frequency• Intensity• Duration• Site
32
• Stabilization• Posture• Sequence• Learning ability

1/5/2016
17
Exercises for Tissue Healing
• Mid‐range motion– Avoid soft‐tissue and joints stress
• ROM– PROM – may start with passive
• To teach an active movement/ demonstrate correct movement patterns in mid‐range
• Will not assist circulation the way voluntary muscle contraction with AAROM or AROM
– AAROM or AROM• AAROM only if unable to go through range without assistance or to teach movement
• AROM best for circulation but greater stresses on tissues33
Exercises for Tissue Healing
• Aerobic activity
– Increases vasodilation to working muscles
• increases blood flow and immune response to damaged cells
– Clears tissue damage and debris
– Light intensity
• <50% of HR maximum for age
• RPE <11 on Borg 6‐20 scale
• Goal is not cardiorespiratory changes–Only to increase temporary blood flow to assist with tissue healing
34

1/5/2016
18
LAB 1: EXERCISE FOR TISSUE HEALING
35
CASE 1: PRESCRIBING EXERCISE FOR TISSUE HEALING
36

1/5/2016
19
Exercise Framework
37
Tissue Healing
Mobility
Performance Initiation, Motor Control & Stabilization
Performance Improvement
Advanced Skill, Coordination, and Agility
Criteria for Mobility Exercises
• Little to no signs of inflammation or stabilized inflammation
• Little to no pain or stabilized pain
38

1/5/2016
20
Assessing Mobility
• Goniometry
• Distance measures
• Joint play
39
Mobility: Exercise Prescription
• ROM
• Stretching
40

1/5/2016
21
Mobility: Range of Motion
• What affects range of motion
– Functional excursion = range of a muscle
• Active insufficiency
• Passive insufficiency
– Soft tissue restriction
– Joint mobility
–Disease/pathology
– Immobility
–Pain
– Edema 41
Why Perform ROM for Mobility?
• Maintain or improve joint and soft tissue integrity
• Minimize the effects of forming contractures and bone demineralization
• Maintain elasticity of muscle
• Assist in circulation and vascular dynamics; diffusion of materials in joint
• Improve synovial movement
• Inhibit pain
• In preparation for stretching 42

1/5/2016
22
Mobility: When Would You Use PROM?
• Patient unable/restricted from AROM
• Examination
• To teach an active movement/ demonstrate correct movement patterns
• In preparation for stretching
43
Mobility: When Would You Use AAROM?
• All of previous, plus:– Patient is permitted to contract muscle, but is unable to go through range without assistance
– When sensory feedback is needed
– To stimulate bone and joint
– To increase circulation
44

1/5/2016
23
Mobility: When Would You Use AROM?
• As previous, plus:–Patient is permitted to contract muscle and is able to go through range without assistance
– To enhance coordination and motor control
45
Limitations of ROM
• PROM will not…
–Prevent muscle atrophy
– Increase strength or endurance
–Assist circulation the way voluntary muscle contraction will
46

1/5/2016
24
Limitations of ROM
• AAROM and AROM will not…
–Maintain or increase strength of strongmuscles
–Develop skill or coordination outside of movement patterns used
47
Mobility Guidelines for ROM
• Monitor patient tolerance
• Recognize value of ROM and potential for abuse (injury)
• Watch for signs of trauma
• Parameters to consider:
– Frequency
– Intensity
– Duration
– Site
– Stabilization
– Posture
– Sequence
– Learning ability
48

1/5/2016
25
Mobility: Stretching
• Stretching is a therapeutic procedure to lengthen pathologically shortened muscles
–Passive
• Patient relaxed, external force applied
–Active
• Patient participates to inhibit tone in a tight muscle
49
Stretching
• Selective stretching
–Muscles stretched (or left tight) purposefully to improve function
• Overstretch
–May be necessary for a given functional task (athletes)
–Detrimental if it causes hypermobility to the point of weakness (stretch weakness)
50

1/5/2016
26
Considerations When Stretching
• Temperature
• Immobilization
• Inactivity
• Age
• Corticosteroids
51
General Guidelines for Passive Stretching
• Takes structures passively past free range of motion
• Force applied no less than 6 seconds up to 2 minutes
• Intensity and duration based on patient’s tolerance (longer tolerable stretches are best)
• Results temporary (elastic)
52

1/5/2016
27
Passive Stretch Techniques
• Static stretching
–Manual
– Self stretching
• Prolonged mechanical passive stretching
53
Prolonged Mechanical Passive Stretch
• Low weight external force applied
–5‐15# or 5‐10% of body weight
• Weighted traction, pulleys, dynamic splints, serial casts
• 20‐30 minutes to several hours
• Permanent lengthening (plastic)
54

1/5/2016
28
Active Stretch Techniques
• Autogenic Inhibition
• Reciprocal Inhibition
55
Autogenic Inhibition
• Patient reflexively relaxes the muscle prior to or during stretching maneuver
–1. Hold relax (HR) (isometric autogenic inhibition)
–2. Contract relax (CR) (concentric autogenic inhibition)
56

1/5/2016
29
Reciprocal Inhibition• Agonist muscle concentrically contracts causing the antagonist muscle (the muscle you want to stretch) to in turn relax
– relaxation of the antagonist muscle allows the agonist muscle to move the limb through the total allowed range of motion without interfering tension
• Perform:
– Instruct contraction of a agonist muscle
– Instruct the patient to relax; stretch the antagonist
• concentrically for agonist contraction– agonist contraction (AC)
• isometrically for hold relax agonist contractionh ld l i i (HR AC)
57
58

1/5/2016
30
Stretching Precautions
• Monitor force used
• Stabilize fracture sites
• Osteoporosis (known or suspected)
• Vigorous stretch of recently immobilized muscles
• Pain lasting >24 hours after stretch
• Edematous tissue
• Overstretching weak muscles
59
Contraindications
• Bony block limiting motion
• After recent fracture
• Acute inflammation
• Infection
• Sharp acute pain with stretch
• Hematoma
• Joint stability required by tight muscle
60

1/5/2016
31
Summary
• Mobility impairments can significantly impair function and quality of life
• Accurately determining the cause of the restricted mobility informs best practice for treatment strategies
• Mobility exercises should be prescribed at a high frequency, low intensity, and long duration
61
LAB 2: EXERCISE FOR MOBILITY
62

1/5/2016
32
CASE 2: PRESCRIBING EXERCISE FOR MOBILITY
63
Exercise Framework
64
Tissue Healing
Mobility
Performance Initiation, Motor Control & Stabilization
Performance Improvement
Advanced Skill, Coordination, and Agility

1/5/2016
33
Criteria for Initiation, Stability, and Motor Control Exercises
• Little to no signs of inflammation or stabilized inflammation
• Little to no pain or stabilized pain
• Mobility
– Functional ranges
65
What’s Involved in Initiation, Stability, and Motor Control?
• Neural input
• Vascular regulation
• Metabolic responses
• Muscle contractility
66

1/5/2016
34
How Does A Muscle Contract?
• Sliding Filament Theory
–Muscle fibers shorten or lengthen because thick and thin myofilaments slide past each other
• It all starts with an action potential
– Excitation contraction coupling67
Neuromuscular Junction (NMJ)
68

1/5/2016
35
Why Do We Want Exercises That Cause Muscle Contraction?
• Initiate loading to tissues
• Proper recruitment of muscles
– synergists and stabilizers
• Increase cardiovascular and muscle endurance
– Initial loads won’t alter capacity
• Increase muscle effective acceleration and deceleration responses (motor control at end ranges)
• Demonstrate muscle control during functional activities
69
Factors that Increase Muscle Performance
Neural Factors
• Activation or “recruitment” of motor units
• Afferent & efferent pathways
• Synchronization
• Cross‐education
• Specificity
Mechanical Factors
• Cross‐sectional area
• Muscle length
• Rate of change of muscle length
• Alignment of muscle with respect to axis of joint rotation
70

1/5/2016
36
Muscle Initiation Exercise: How Do We Dose Them?• Frequency
– 2‐3x/wk, non consecutive days
• Intensity
– 40‐60% 1RM; goal is activate motor neurons
• Time
– To or before fatigue; rest breaks incorporated
• Type
– Isometric
– Isotonic• Eccentric
• Concentric
– Open Chain
– Close Chain 71
Stability
• Static control
• Coordination of motor and sensory components
• Balance of soft tissue function around a joint or body part
• Provides a stable foundation from which to move
72

1/5/2016
37
Consequences of Instability
• Altered joint mechanics
• Limited ROM with a compensatory hypermobility
• Change in proprioceptive input
• Impaired reciprocal inhibition
• Altered programming of movement patterns
73
Stability Exercises: How Do We Dose Them?
• Frequency
– High volume
• Intensity
– Light to moderate
• Specificity of muscles
• Time
– Increase time to fatigue
• Type
– Isometric hold
– High repetitions74

1/5/2016
38
Motor Control
• Study of human movement and the systems that control it under normal and pathological conditions
• Motor programming theory
–Create generalized motor program of classes of skilled movement
• Other theories
• Reflex
• Hierarchical
75
Motor Control Techniques Include
• Graded resistance
• Reinforcement
– Verbal and visual stimulation
– Traction
– Approximation
• Timing
• Neural inputs
– Rhythmic initiation
– Rhythmic stabilization
– Reflex inhibiting postures
– Combined isotonics and dynamic reversals76

1/5/2016
39
Exercise Prescription for Stability and Motor Control Exercise
• Similar to concepts for other muscle initiation exercise
• Isometrics for stability with prolonged hold
• Isotonics for motor control through functional range at slow velocity with emphasis on control
– Facilitory tactile, verbal, visual techniques to improve recruitment, synergies, and better movement strategies
77
Motor Control
• Macedo 2009 PTJ– systematic review motor control exercise for LBP
• Motor control better than minimal intervention in the short term, intermediate, and long term for pain– Exercise is medicine – get people moving!
• Motor control better than manual therapy in intermediate duration for pain, disability and QOL– Motor control when tissue healing and pain decreased and mobility restored
• Motor control better than other exercise for disability in short term– Overloading tissues should happen but not in short term with more acute or subacute injury 78

1/5/2016
40
Motor Control Exercises: How Do We Dose Them?
• Frequency – Often; multiple times a day, most days of the week
• Intensity– Low to moderate intensity (40‐60% 1RM)
• Need proper activation of motor units– Avoid faulty movement patterns
• Time– Avoid fatigue; short bouts with rest
• Type– Isometric – isometric with increasing movement of limbs and then trunk
79
Assessing Initiation, Stability, and Motor Control
80

1/5/2016
41
LAB 3: EXERCISE FOR INITIATION, STABILITY, AND MOTOR CONTROL
81
CASE 3: PRESCRIBING EXERCISE FOR INITIATION, STABILITY, AND MOTOR
CONTROL
82

1/5/2016
42
Exercise Framework
83
Tissue Healing
Mobility
Performance Initiation, Motor Control & Stabilization
Performance Improvement
Advanced Skill, Coordination, and Agility
Performance Improvement
84

1/5/2016
43
Neural FactorsEnhanced neural facilitation largely accounts for rapid and
significant strength increases early in resistance training (this often occurs without an increase in muscle size and cross‐sectional area)
85
Keep in Mind: Goal of Treatment
• Components of Muscle Performance
–Hypertrophy
• Increase of muscle mass by increasing size
– Strength
• Force generating capacity of a muscle
–Power
• Ability of the muscle to use strength quickly
– Endurance
• Ability of muscle to contract repetitively with low load or to maintain a low load contraction 86

1/5/2016
44
HOW DO WE MEASURE MUSCLE PERFORMANCE IMPROVEMENT?
• Hypertrophy
– Girth measures for under 40 years
– Strength as a proxy
• Strength
– Repetition maximum testing
– Hand held dynamometry
• Power
– Chair rise
– Gait velocity
– Stair climb
– Medicine ball toss
• Muscle endurance
– Repetitions to failure
– Duration to failure
PARAMETERS TO CONSIDER
• Muscle action
• Loading
• Training volume
• Exercise selection
• Mode
• Exercise order
• Rest periods
• Velocity
• Frequency
88
What component of muscle performance do you want to target?

1/5/2016
45
MUSCLE ACTION
Concentric
• muscle shortening
• usually the load limiting portion of an exercise
Eccentric
• muscle lengthening
• produces greater force per unit of muscle size
• more conducive to hypertrophy
• result in more delayed onset muscle soreness
89
MUSCLE ACTION
Isometric• No change in muscle length
• Good for selective recruitment training
• Good for postural, spinal stabilization exercise
90

1/5/2016
46
LOADING
• Amount of resistance per repetition
• Also known as intensity
• Dictates the number of repetitions
• Appropriate load differs depending on treatment goal and training level
91
LOAD AND REPSNumber of Reps
• 1 rep
• 2‐3 reps
• 4 reps
• 5‐6 reps
• 7‐8 reps
• 9 reps
• 10 reps
• 11 reps
• 12‐13 reps
• 15 reps
• 30 reps
Corresponding % of 1RM
• 100%
• 95%
• 90%
• 85%
• 80%
• 75%
• 70%
• 65%
• 60%
• 50%
• 30%92

1/5/2016
47
0
0.5
1
1.5
2
2.5
3
40 45 50 55 60 65 70 75 80 85 90
Str
en
gth
Ga
ins
Intensity of training (% of 1 RM)
Strength Gains With Different Intensities of Training
Untrained
Trained
Athletes
93
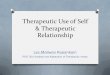
LOADING - Strength• 50% of 1RM is recommended initially to allow
learning of proper form and technique
• 45-50% of 1 RM increases strength in untrained individuals
• At least 80% of 1 RM is needed to increase strength for experienced individuals
• Using a variety of training loads is most conducive to maximizing strength
94

1/5/2016
48
LOADING- Other
• Endurance gains are made with low loads and high repetitions
• Power gains are made with low to high loads and fast velocities
• Hypertrophy gains are made with high loads and low repetitions
95
Can you just let patients self‐select the intensity?
• Self‐selected intensities are lower than recommendations13‐15
96

1/5/2016
49
SETS• The number of groups of repetitions for
each exercise• May depend in part in how much time is
available• Generally, better gains are made with
multiple sets
97
0
0.5
1
1.5
2
2.5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Str
en
gth
Ga
ins
Number of Sets Per Muscle Group
Strength Gains and Number of Sets
UntrainedTrainedAthletes
98

1/5/2016
50
SETS AND TRAINING VOLUME
• Low volume programs• high load, low repetitions, moderate to high
number of sets
• result in strength gains
• High volume programs• Low load, high repetitions, moderate to high
number of sets
• Result in endurance gains
• Not all exercises need to be performed with the same number of sets
99
EXERCISE SELECTION
• Both single and multiple joint exercises are effective for increasing strength of targeted muscle groups
• Multiple joint exercises are more neurallycomplex
• Single joint exercises require less skill and technique
100
When possible, use exercise that targets functional limitation

1/5/2016
51
REST PERIODS• Amount of rests between sets of exercises
• Affect performance of subsequent sets
• Performance compromised with short rest periods (<1 minute) and >60% 1RM
• Greater strength increases with long rest periods (2-3 minutes)
• Vary based on goals of exercise
101
Generally, with higher intensities, want longer rest periods. With endurance training, you want shorter
rest periods.
MODE• If you establish an appropriate muscle
action, training volume, load, and rest period, you can achieve your resistance training goals with any mode
• Weight machines are safer to use and easy to learn
• Free weights allow mimicking of functional tasks
• Resistance bands are inexpensive and readily available in any setting
102

1/5/2016
52
EXERCISE ORDER
• Affects muscular strength
– Generally, exercise performed first will have gest results
• Maximize performance of exercises targeting your primary functional goal
103
OTHER CONSIDERATIONS:EXERCISE ORDER
• Large muscle group exercises before small muscle group exercises
• Perform multiple joint exercises before single joint exercises
• Higher intensity exercises before lower intensity exercises
104

1/5/2016
53
VELOCITY• The speed of contraction
• High velocity improves power—as fast as they can, hold for a second, then lower
• Slow velocity yields better strength and endurance gains
• What velocity you choose depends on the functional goal
105
EFFECTS OF REGULAR AND SLOW SPEED RESISTANCE TRAINING ON MUSCLE
STRENGTHWestcott WL: J Sports Med Phys Fitness 41(2):154-158, 2001
Two studies (one on men and one on women)
Compared regular speed repetitions (2 second lift, 1 second pause, 4 second lowering) to super slow repetitions (10 second lift, 4 second lowering)
106

1/5/2016
54
EFFECTS OF REGULAR AND SLOW SPEED RESISTANCE TRAINING ON MUSCLE
STRENGTHWestcott WL: J Sports Med Phys Fitness 41(2):154-158, 2001
Super slow training resulted in a 50% greater increase in strength for both men and women than regular speed training
Regardless of speed, all groups exercised at 70% of 1RM
Super slow training is an effective method for middle-aged and older adults to increase strength
107
HIGH VELOCITY RESISTANCE TRAINING INCREASES SKELETAL MUSCLE PEAK
POWER IN OLDER WOMENFielding RA. J Am Geriatr Soc. 2002; 50:655-662.
30 subjects randomized into:
high velocity (concentric as fast as possible, hold 1 sec, eccentric 2 sec )
low velocity (2 sec concentric, hold 1 sec, 2 sec eccentric ) training
70% 1RM, 3x/week, 16 weeks, 3 sets, 10 reps
108

1/5/2016
55
HIGH VELOCITY RESISTANCE TRAINING INCREASES SKELETAL MUSCLE PEAK
POWER IN OLDER WOMENFielding RA. J Am Geriatr Soc. 2002; 50:655-662.
Both groups increased strength similarly
High velocity: leg press ↑ 35%; knee extension ↑45%
Low velocity: leg press ↑ 33%; knee extension ↑41%
High velocity had twice the gains in power
High velocity: 97%
Low velocity: 45%109
FREQUENCY• Number of workouts per week
• When training in the performance improvement phase, need at least one day of rest between sessions
110

1/5/2016
56
0
0.5
1
1.5
2
2.5
1 2 3
Str
en
gth
Ga
ins
Frequency of Training (days/week)
Strength Gains and Frequency of Training
Untrained
Trained
Athletes
111
Cardiovascular Performance Improvement
• Frequency
• Intensity
• Type
• Time
112

1/5/2016
57
Balance Performance Improvement
113
Physiology of Balance
• Postural control, or balance is an interaction of the individual, task, and environment
• Requires coordination of multiple systems– Musculoskeletal
• ROM, strength and power, joint sense, muscle tone
– Central set• Motor programs from past experiences, fine tuning
– Environment• Surface, movement, distractions
• Results in up‐regulation or down‐regulation

1/5/2016
58
Physiology of Balance
• Motor coordination– Movement strategies based on motor plans, feed back and feed forward control, adjustment and tuning of strategies
• Somatosensory system– Muscle spindle, GTOs, joint receptors, cutaneous receptors
– Dominant sensory system
• Visual system– Eye and visual tracts, thalamic nuclei, visual cortex with projections to parietal and temporal lobes
Physiology of Balance
• Vestibular system
– Cerebellum,, brain stem, ear
– Not under conscious control
• Cognitive
– Attention, adaptation, confidence, fear, anticipation

1/5/2016
59
Physiology of Balance
• Balance is the ability to generate and apply forces appropriately to control body position in space
• In order to do this, the forces must be organized in such a way for efficient stability, response to perturbation, and preparation for movement
Balance Reactions‐‐Stability
• Quiet stance
• Activity in anti‐gravity muscles
• Coordinated low level forces
• CNS integrates and organizes information
• Requires some attention—not automatic
• Dual tasking possible as long as demand is low

1/5/2016
60
Balance Reactions—Reactive Postural Adjustments
• Response to perturbation
• Muscles act in synergy
• Relies on somatosensory information
• Increased reliance on vision during learning and after neurological insult
• Requires attention
• Adaptation occurs with repeated perturbation
• Anticipation possible based on central set—using previous experience to fine tune current
Balance Reactions‐Anticipatory Postural Adjustments
• Preparation of movement in space
• Muscle activity similar to RPA
• Anticipatory muscle activity occurs before agonist
• Visual information is used to predict trajectory and needed force
• Can be trained to occur faster with practice

1/5/2016
61
Balance Strategies‐‐Ankle
• Used when perturbation is slow or low amplitude, the surface is firm, wide, and longer than the feet
• Muscles are recruited distal to proximal
• Head movements are in phase with hip
Balance Strategies‐‐Hip
• Used when perturbation is fast or large, surface is unstable or shorter than the foot
• Muscles are recruited proximal to distal
• Head movement is out of phase with hips

1/5/2016
62
Balance Strategies‐‐Stepping
• Used to prevent a fall
• Used when perturbations are fast, large, and other strategies fail
• Base of support is trying to “catch up”
Balance Strategies‐‐Suspensory
• Forward bend of trunk with hip and knee flexion
• Lowers center of gravity
• Strategies are automatic and occur 85 to 90 milliseconds after the perception of instability is realized

1/5/2016
63
Aging and Balance
• Older adults tend to shift to hip or stepping strategies rather than use an appropriate ankle strategy
• Older adults try to gain sensory information by co‐activating muscles or increasing sway rather than using effective motor strategies to adjust to balance challenges
Aging and Balance
• When these responses to perturbation happen and sway increases there is often insufficient time for muscles to react in time to prevent the balance challenge
• Older adults holding a cane seldom reach for a more stable handrail, suggesting that when something is in the hands, the nervous system prioritizes that object rather than using t he hand to reach and improve balance support

1/5/2016
64
Prescribing Balance Performance Improvement Exercise
• Frequency
• Intensity
• Type
• Time
127
Summary: Performance Improvement
• Identify targeted components
–Muscle
–Cardiovascular
–Balance
• Accurately prescribe each parameter to improve primary component and achieve functional outcome
128

1/5/2016
65
LAB 4: EXERCISE FOR PERFORMANCE IMPROVEMENT
129
CASE 4: PRESCRIBING EXERCISE FOR PERFORMANCE IMPROVEMENT
130

1/5/2016
66
Exercise Framework
131
Tissue Healing
Mobility
Performance Initiation, Motor Control & Stabilization
Performance Improvement
Advanced Skill, Coordination, and Agility
Advanced Coordination and Skill
• Exercise Prescription Variables• Body position• Proximal joints then distal joints
• Complexity of task
• Surface– Stable
– Compliant
–Moving
• Resistance• Speed • Accuracy
132

1/5/2016
67
Performance Elements
• Speed
–Acceleration over a short period of time
• Agility
–Ability to move quickly and easily with speed and coordination
• Coordination
–Ability to perform a task using reciprocal motions (agonist to antagonist) and synergy (muscle groups acting together) with accuracy
133
Performance Elements
• Synergy
–A particular group of muscles that have been linked together in a certain sequence responding to consistent and precise muscle activation
• Accuracy
–Ability to gauge or judge distance correctly
• Proprioception
– The awareness of the body in space134

1/5/2016
68
Who is Appropriate for Advanced Coordination and Skill Activities?
• Joint/local stability and regional/global stability essential during muscle performance improvement – Must have prior to progression to advanced coordination and skill
• Illustrate strength and power gains
• Appropriate goals of coordination, agility, and plyometric training
• Advanced motor control goals • Specificity, reaction time, synergies, dynamic motor programs
–Speed, agility, coordination, quick response
135
Examples of Advanced Coordination and Skill Exercises
• Drills
– Speed
–Agility
–Coordination
• Complex tasks
–Maximizing muscle performance according to goal
• Dynamic stability with advanced parameters
• Plyometrics 136

1/5/2016
69
Training Modality ‐ Plyometrics
• Actually means “measurable increases”
– “Jump training”
–Can be small or big motions
• Links (a) physiological properties of muscle with (b) strength and (c) speed to produce POWER
• Advanced neuromotor control
• Produces long term muscle endurance
137
Plyometric Theory
• Exploits the elastic components of the muscle and musculotendinous unit to increase power through the stretch‐shortening cycle
– Stretch = eccentric
– Shortening = concentric
138

1/5/2016
70
Plyometric Theory
• Energy stored during eccentric contraction
• Stored energy converted to power during concentric contractions
• Conversion between eccentric and concentric contraction = amortization phase
139
Energy stored Energy ReleasedSpring at rest
Reasons for Plyometric Training
• Combination of:
–Advanced strength performance
–Advanced joint ROM and muscle flexibility
–Neurological effect (training effect)
– Eccentric loading/preparation for quick response to unplanned athletic movement
140

1/5/2016
71
Advanced Coordination and Skill Exercises: How Do We Dose Them?
• Frequency
– 2‐3x/wk; non‐consecutive days; rest is important!
• Intensity
– Low to high intensity (30‐90% 1RM)• Increase activation of motor units
– Start with lower intensity to ensure proper movement patterns but move quickly to overload
• Time
– Endurance goals ‐ push to fatigue and beyond
– Power goal ‐ short bouts with rest
• Type
– Dynamic and multiplanar movment• Change surfaces, distraction, speeds 141
CASE 5: PULLING IT ALL TOGETHER
142

1/5/2016
72
143
THANK YOU!!!
144

ClinicalDecisionMakinginTherapeuticExercisePrescriptionAppendicesandReferences
1

ASSESSING VARIOUS ASPECTS OF THE EXERCISE FRAMEWORK Phase of Exercise
Framework What is Being Assessed Method of Assessment
Tissue Healing Pain Numeric Pain Rating Scale Baker‐Wong FACES scale Visual Analog Scale
Inflammation Skin thermometer Observation of color Girth (for edema) Stiffness index ( subscale of WOMAC)
Mobility Joint motion Goniometry Inclinometry Accessory motion
Muscle length Goniometry Tape measure
Stability Endurance and strength Balance
Duration of holds (time to failure) One‐legged Stance Time (OLST) Romberg/Sharpened Romberg Functional reach (multi‐directional)
Initiation Aerobic initiation Muscle initiation
Submaximal aerobic exercise tests (e.g. Astrand Rhyming Cycle Ergometer Test) 1RM submaximal prediction tests
Motor Control Anticipatory postural reactions Synergy Coordination
Timed up and go test Four square step test Obstacle course Diagonal motions Rhythmic Initiation/Stabilization Combined isotonics Dynamic reversals Repeated Stretch Contract‐relax/Hold‐relax
Performance Improvement
Aerobic capacity Seated step test 6 minute walk test (6MWT) Astrand Rhyming bike test YMCA cycle test Bruce Treadmill test Steady State Treadmill test Talk test
Muscle strength Hand held dynamometry 1RM
Muscle hypertrophy Girth measurements in younger adults Use strength as a proxy in older adults
Muscle power Chair rise (5xSTS, 10xSTS, 30 sec CR) Gait velocity Stair climb Medicine ball toss
Muscle endurance Repetition to failure Duration to failure
Advanced Coordination Reactive postural adjustments External perturbations Dual tasking
Advanced skill Timed tests Accuracy
2

Wong Baker FACES Scale for Pain Assessment
Numeric Pain Rating Scale (NPRS) for Pain Assessment
3

Chair Rise
1. Ask the subject to sit as far back as possible in the chair seat and k Keep feet firmly planted on the floor
approximately hip width apart with arms crossed over the chest.
2. Show the subject how to stand up one time and sit down, returning completely to the correct starting position.
Indicate the importance of proper technique, e.g. not standing all the way up, not sitting all the way back, lifting
feet off the floor, etc.
3. Have the subject try one chair stand to be sure he/she has proper technique
4. Instruct the subject that the timed assessment will begin on the command; “Go” and that they are to stand up
as quickly and safely as possible.
5. Start timing at the command “Go” the tester begins timing by starting the stopwatch.
6. Stop timing when the patient attains a fully upright position.
7. If subjects are unable to stand up one time without assistance, they can use their hands to assist them in rising
and returning to the seated position while following all other procedures as described above.
5 x Sit to Stand
1. Ask the subject to sit as far back as possible in the chair seat and k Keep feet firmly planted on the floor
approximately hip width apart with arms crossed over the chest.
2. Show the subject how to stand up one time and sit down, returning completely to the correct starting position.
Indicate the importance of proper technique, e.g. not standing all the way up, not sitting all the way back, lifting
feet off the floor, etc.
3. Have the subject try one chair stand to be sure he/she has proper technique
4. Instruct the subject that the timed assessment will begin on the command; “Go” and that they are to stand up
and sit back down 5 times as quickly and safely as possible.
5. Start timing at the command “Go” the tester begins timing by starting the stopwatch.
6. Count each chair stand out loud when the subject is in the standing position. Provide continuous verbal
encouragement during the test.
7. At the fifth repetition click the stopwatch off when the subject’s back hits the chair (or returns to proper seated
position).
8. If subjects are unable to stand up one time without assistance, they can use their hands to assist them in rising
and returning to the seated position while following all other procedures as described above.
10 x Sit to Stand
1. Ask the subject to sit as far back as possible in the chair seat and k Keep feet firmly planted on the floor
approximately hip width apart with arms crossed over the chest.
2. Show the subject how to stand up one time and sit down, returning completely to the correct starting position.
Indicate the importance of proper technique, e.g. not standing all the way up, not sitting all the way back, lifting
feet off the floor, etc.
3. Have the subject try one chair stand to be sure he/she has proper technique
4. Instruct the subject that the timed assessment will begin on the command; “Go” and that they are to stand up
and sit back down 10 times as quickly and safely as possible.
5. Start timing at the command “Go” the tester begins timing by starting the stopwatch.
4

6. Count each chair stand out loud when the subject is in the standing position. Provide continuous verbal
encouragement during the test.
7. At the tenth repetition click the stopwatch off when the subject’s back hits the chair (or returns to proper seated
position).
8. If subjects are unable to stand up one time without assistance, they can use their hands to assist them in rising
and returning to the seated position while following all other procedures as described above.
30 Second Chair Rise
8. Ask the subject to sit as far back as possible in the chair seat and k Keep feet firmly planted on the floor
approximately hip width apart with arms crossed over the chest.
9. Show the subject how to stand up one time and sit down, returning completely to the correct starting position.
Indicate the importance of proper technique, e.g. not standing all the way up, not sitting all the way back, lifting
feet off the floor, etc.
10. Have the subject try one chair stand to be sure he/she has proper technique 11. Instruct the subject that the timed assessment will begin on the command; “Go” and that they are to stand up
and sit back down as many times as they can during a 30 second period.
12. Start timing at the command “Go” the tester begins timing by starting the stopwatch.
13. Count each chair stand out loud when the subject is in the standing position. Provide continuous verbal encouragement during the test.
14. At 30 seconds, stop counting and record the number of chair rises completed.
15. If subjects are unable to stand up one time without assistance, they can use their hands to assist them in rising
and returning to the seated position while following all other procedures as described above.
Multi‐Directional Reach Test
1. Position a yardstick at the level of the subject’s acromion process.
2. Ask subject to stand with feet shoulder width apart and arm raised to 90 degrees and fisted
3. Ask subject to reach as far forward with their fist as possible without letting their feet raise off the floor or their
hand touch the yardstick.
4. Record the distance reached measuring from location of the second knuckle (in inches) at the start and the
location of the second knuckle (in inches) at the farthest point reached without loss of balance.
5. Perform 2 trials.
6. Keeping patient in the same position, repeat similar protocol for reach backwards, left and right.
Gait Velocity
1. Place tape on the floor: start line, end of 3 meter acceleration zone, end of 10 meter timing zone and end of 3
meter deceleration zone
2. Ask the subject to stand at the start line and explain that when you say “go” he/she should walk at their normal
pace to the line at the end of the deceleration zone
3. Begin timing when the subject’s front foot crosses the tape at the end of the acceleration zone/beginning of the
timing zone.
4. Stop timing when the subject’s back foot crosses the tape at the end of the timing zone/beginning of the
deceleration zone
5. Divide 10 meters by the number of seconds and record on the data sheet as usual gait speed in m/sec
5

6. Repeat the same procedure but ask the patient to walk as fast as they can (no running). Record this as maximum
gait speed in m/sec
Acceleration Timing Deceleration
Zone Zone Zone
3 m 10 m 3 m
Timed Up and Go Test
1. Ask subject to sit comfortably in chair with feet flat on floor behind the line and arms across chest. 2. Instruct subject that when you say “go” they should stand up as quickly as possible without using their hands,
walk as quickly as possibly (no running) down to and around the cone positioned 3 meters away and return to sitting in the chair.
3. Demonstrate for the patient 4. Allow the patient a practice trial to ensure understanding 5. Start timing when you say, “Go.” 6. Stop timing when subject returns to seated position (i.e., when back touches the back of the chair if they were
able to sit with back against chair and feet on floor OR when bottom touches seat of chair if they were not able to sit in chair with back against chair and feet flat on floor)
7. Record time on data sheet. If subject uses hands add 5 seconds to the time. 8. Repeat for second trial
6 MWT
1. Mark off a walking course in 10 meter increments.
2. Record the subject’s resting heart rate, blood pressure, and assistive device.
3. Ask the subject to begin walking when you say, “Go,” and continue walking until you say, “Stop” in 6 minutes.
4. Instruct the subject that he/she may stop and rest and even sit and rest if needed and for as long as needed.
5. Keep track of how far the subject walks.
6. At the end of 6 minutes, record on the data sheet the subject’s resting heart rate and blood pressure and the
distance walked during the 6 minutes .
The One‐Legged Stance Test (OLST)
1. Instruct subjects to stand on one leg without upper extremity support, and without resting the suspended leg on
the stance leg for as long as possible up to 60 seconds.
2. Begin timing when subjects lift their foot off the floor and continued until:
a. The suspended foot touches the ground
b. The suspended foot rests against the stance leg
c. subjects need support to prevent loss of balance
d. the stance foot moves/changes location on the floor
3. Repeat the test 3 times. Their best trial will be utilized for data processing.
4. If patient performed test for 60 seconds on the first trial, subsequent trials are not attempted and instead
recorded as 60 seconds. If they cannot perform the test without the use of an assistive device then record 0
seconds.
5. Perform testing first by testing the subject’s balance on their right lower extremity followed by their left lower
extremity.
6

Romberg
1. Ask subjects to stand with feet side by side and knees touching.
2. You can assist subjects unable to attain the position independently into the position.
3. Begin timing when the subject stands in testing position without external support.
4. Stop timing when the subject moves their feet or can no longer maintain balance without support.
5. Repeat the test a total of three times. Their best trial will be utilized for data processing.
6. If the subject performs test for 60 seconds on the first trial, subsequent trials are not attempted and instead
recorded as 60 seconds
7. Repeat this procedure with the subjects’ eyes closed.
Sharpened Romberg
1. Ask subjects to stand with one foot in front of the other in a heel‐to‐toe position
2. You can assist subjects unable to attain the position independently into the position.
3. Begin timing when the subject stands in testing position without external support.
4. Stop timing when the subject moves their feet or can no longer maintain balance without support.
5. Repeat the test a total of three times.
6. If the subject performs test for 60 seconds on the first trial, subsequent trials are not attempted and instead
recorded as 60 seconds
7. Repeat this procedure with the subjects’ eyes closed.
Astrand Rhyming Cycle Ergometer Test to predict maximal oxygen uptake (VO2max)
1. Adjust seat on cycle so knee is almost fully extended at the furtherest point on the pedal.
2. Take and record resting heart rate and blood pressure
3. Subjects cycle at 50 revolutions per minute for six minutes at a work load dependent on gender and conditioning
level (unconditioned males = 75 watts; unconditioned females = 50 watts; conditioned males = 125 watts;
conditioned females =75 watts).
4. Take and record heart rate by radial pulse in the last ten seconds of the two final minutes of exercise, These two
measures should be very close to each other to show the subject has reached their steady state. If they are not
(i.e., the 6 minute heart rate is 10 bpm higher than the 5 minute one), stop the test, increase the workload and
repeat.
5. Average the 5 and 6 minute heart rate together, and use to estimate VO2max using a nomogram (Appendix B)
or equation. Adjust this value for age by multiplying by 0.68 for those aged 60‐64 and by 0.65 for those aged 65
and older. Correlation of an estimated VO2max through this method compared to maximal oxygen uptake
testing is 0.90 (p<0.05).
The Four Square Step Test (FSST)
PVC pipes are arranged to form a large square (5 ft x 5t) divided into 4 small squares (each 2.5 ft x 2.5 ft). Patients stand
in a square wearing a gait belt and facing the next square. When told, “go,” the patient steps into the next square
touching both feet in the square prior to moving to the next without losing their balance and without touching the
pipes. Once both feet have touched in each square, the patient reverses direction and again touches both feet in each
square until they again reach their start position. Time is started as soon as the patient moves the first foot and 7

concluded when the second leg returns to the starting position. One practice trial is completed and two official times are
collected and the two times averaged for a score. A trial is repeated if the patient fails to complete the sequence
successfully, loses balance, or makes contact with a cane during the sequence. Patients who are unable to face forward
during the entire sequence and need to turn before stepping into the next square are still given a score.
Obstacle Navigation
Patient performs a task of navigating obstacles placed on the floor. Patient walks along a marked walkway consisting of
a 10 foot long acceleration/deceleration zone, a 16foot walking zone with bricks placed at the 5 foot and 10 foot marks
and a waste can placed at the 16 foot mark. When told, “Go,” patient begins walking along the walkway, steps over the
bricks, walks around the waste can, and continues walking until they again reached the starting point. Patients are timed
in seconds beginning when their front foot crossed the beginning of the walking zone and ending when their front foot
crossed the end of the walking zone.
Motor Control Techniques
Diagonal motions
Focuses on synergistic muscle combinations by combining motions in all 3 planes of movement; sagittal ( flexion,
extension), coronal/frontal ( abduction, adduction), transverse plane (rotation). In addition, motion can be unilateral
or bilateral and symmetrical or asymmetrical.
Rhythmic Initiation
Involves rhythmic motion of the limb through ROM. Start with PROM where you provide manual movement of the
limb and provide contacts with constant speed and verbal commands. Progress to AROM that is resisted motion by
PT and speed maintained by verbal commands. You can add increased cueing and manual input to eccentric,
concentric and isometric holds at end ROM.
Rhythmic Stabilization
Patient maintains alternating isometric contractions (no ROM) with manual PT resistance where the PT switches
positions and patient responds in new direction of force but with no movement (isometric). Purpose is to increase
stability. The PT can add verbal commands. Resistance can be built up as patient matches force. Also, approximation
or traction can be used in conjunction with resistance.
Repeated Stretch
PT provides a quick stretch at initiation of ROM (end range) of agonist muscle. The resistance can be given for
movement into the ROM. In addition, a repeated stretch through ROM can be provided by the PT in order to initiate
the Initial stretch reflex at beginning ROM or at mid‐range with instructions to contract (overcome stretch with
increased resistance) and continue move through ROM.
Contract‐Relax
Purpose is to increase PROM by using a resisted isotonic contraction of antagonist muscles followed by relaxation of
antagonist and increased ROM of agonist. The limb is moved to the end of the ROM and the patient is to resist
antagonist muscle at end range. Next the PT is to stretch into increased ROM OR patient can actively move into
ROM.
8

Hold‐Relax
Purpose is to perform an isometric contraction of antagonist muscle to increase ROM. The limb is moved to end
ROM (PROM or AROM). Next the PT provides isometric resistance to antagonists at end ROM. The patient relaxes
allowing limb to move into new ROM (PROM or AROM). Then you can repeat isometrics in the new range.
Combined Isotonics
Combined manually resisted concentric, eccentric, and isometric contraction of one muscle group (agonists) without
rest/relaxation.
Dynamic Reversals (fast or slow)
Active motion changing by the patient and/or manual input from the PT from one direction (agonists) to opposite
direction (antagonists) without pause or rest/relaxation.
Goals for Motor Control Techniques
Increasing ROM and strength through newly gained ROM:
Rhythmic initiation / stabilization
Contract‐relax, Hold‐relax
Dynamic reversal patterns
Isotonic contraction throughout ROM
Decrease muscle fatigue in strengthening phases:
Repeated stretch
Dynamic (fast or slow) reversal patterns
Combined Isotonics
The Talk Test
Subject recites the pledge of Allegiance and is asked, “Can you speak comfortably?” Patient scores 1 if they can speak comfortably Patient scores a 2 if unsure if they can speak comfortably Patient scores a 3 if they cannot speak comfortably
The Seated Step Test
Position patient in a comfortable straight back chair
Place a 6” step in front of the patient so when the patient steps, the instep rests on the step top
Set a metronome for 60 clicks per minute
Patient steps up with right foot, down with right foot, up with left foot, then down with left foot staying with the
beat of the metronome.
Record HR, BP and RPE at 2 minutes. If no angina or inappropriate vital responses, patient continues for
another 3 minutes. 9

Record HR, BP and RPE at 5 minutes. If no angina or inappropriate vital responses, replace 6” step with 12” step
and continue.
Record HR, BP and RPE at 2 minutes. If no angina or inappropriate vital responses, patient continues for
another 3 minutes.
Record HR, BP and RPE at 5 minutes. If no angina or inappropriate vital responses, replace 6” step with 18” step
and continue.
Record HR, BP and RPE at 2 minutes. If no angina or inappropriate vital responses, patient continues for
another 3 minutes.
Record HR, BP and RPE at 5 minutes. If no angina or inappropriate vital responses, continue with 18” step and
have patient raise alternate arms with legs.
Record HR, BP and RPE at 2 minutes. If no angina or inappropriate vital responses, patient continues for
another 3 minutes.
Record HR, BP and RPE at 5 minutes. Testing is complete.
When patient is unable to continue with the test because of fatigue, abnormal vitals, angina, etc., note the HR
and MET level of last completed level. Use this data to predict VO2
SEATED STEP TEST
Workload/METs HR BP RPE Dyspnea Angina Comments
6 inch step @2 min
6 inch step @ 5 min (2.3 MET)
12 inch step@ 2 min
12 inch step@ 5 min (2.9 MET)
18 inch step@ 2 min
18 inch step@ 5 min (3.5 MET)
18 inch step @ 2 min with arms
18 inch step@ 5 min with arms (3.9 MET)
Treadmill Steady State Test General: Steady state treadmill test requires that you first determine what speed reaches the patient in a submax HR range (60‐85% of HRmax) then patient goes additional 4 minutes at steady state workload (same speed with added 5% grade). Patient maintains steady state workload once submax HR range is reached (ie DON’T change speed) and monitor HR, BP, and RPE. Protocol:
1. Take resting vitals (HR, BP and explain RPE) 2. Calculate submaximal HR range for your patient (60‐85% of HR max) 3. Begin warm up at a low intensity for 3 minutes (5 minutes for less fit/poor health) 4. Adjust speed (DO NOT ADD GRADE) to a workload that subject reaches submax HR (60‐85% of HRmax)
a. If HR in submax range, continue for a total of 4 minutes at that speed and monitor HR, BP, and RPE b. If HR not in submax range (60‐85% of HR max)by minute 2‐3, increase speed for 4 total minutes in
submax range 5. Take HR at minute 3 and minute 4 once in submax workload to measure steady state HR values (1‐5 bpm apart)
a. If steady state HR, progress to next step to increase GRADE i. If in submax HR range but not steady state HR (1‐5 bpm apart), continue 1 minute and retake HR
6. Continue at same speed but increase grade 5% for 4 additional minutes (HR should still be in submax range 60‐85% of HR max)
7. Take HR at minute 3 and minute 4 for steady state HR values (1‐5 bpm apart)
10

a. If steady state HR then test is complete and cool down i. If in submax HR range but not steady state HR, continue 1 minute and retake HR
8. Cool down with minimal resistance for 3‐5 minutes, retaking HR and BP every 2‐3 minutes and end of cool down VO2 Max Prediction Equation: VO2max = 15.1 + 21.8* SPEED (mph) – 0.327*HR(bpm) ‐ .263*SPEED*AGE(yr) + 0.00504*HR*AGE +5.98*GENDER (0=female; 1=male)
Ebbeling, 1991, Waddoups, 2008 YMCA Cycle Test General: 9‐12 minute multistage test (2‐4 stages of 3 minutes in duration). Patient must complete 2 stages with HR in submaximal range (60‐85% of HRmax) with a steady state HR (1‐5bpm apart) determined at each stage. All patients start at same workload of 150 kg*m/min (0.5 KP or kg) or (25 Watts). The 2nd stage workload is dependent on 1st stage steady state HR value (take highest). You must use the YMCA chart in ACSM text for workload determination (see chart below). Protocol:
1. Take resting vitals (HR, BP and explain RPE) 2. Calculate submaximal HR range for your patient (60‐85% of HR max) 3. Set bike seat at proper height
a. Hip: Standing at greater trochanter b. Knee: approx. 5‐10 degrees bend
4. Begin warm up at low resistance for 2‐3 minutes at 50 RPM (5 minutes for less fit/poor health)
Adjust resistance to workload 150 kg*m/min (0.5 KP or kg) or (25 Watts) a. Take HR at minute 2 and 3 for steady state HR (1‐5 bpm apart)
i. If not steady state HR, continue 1 minute and retake HR o Use steady state HR at last minute to determine workload using YMCA chart (ACSM Guide pg82, Manual
pg 122) 5. Stage 2: Adjust resistance to higher workload based on 1st stage HR value
a. Take HR at minute 2 and 3 for steady state HR (1‐5 bpm apart) i. If steady state HR at minute 3, move to next stage ii. If not steady state, continue 1 minute and retake HR*
b. Take BP between HRs or at end of stage c. Note – if submax HR isn’t achieved in Stage 2, two more stages are needed
6. Stage 3: Adjust resistance to higher workload a. Take HR at minute 2 and 3 for steady state HR (1‐5 bpm apart)
i. If steady state HR at minute 3, move to next stage ONLY if stage 2 wasn’t subaxial HR range. If stage 2 AND 3 were in submaximal HR range, start cool down
ii. If not steady state HR, continue 1 minute and retake HR b. Take BP between HRs or at end of stage
i. Note if submaximal HR range achieved in Stage 2 and 3, test can be terminated after Stage 3 ii. If submaximal HR range was not achieved in Stage 2, continue to Stage 4
7. Stage 4: Adjust resistance to higher workload a. Take HR at minute 2 and 3 for steady state HR (1‐5 bpm apart)
i. If steady state HR at minute 3, move to cool down (test too long). If stage 3 AND 4 were in submaximal HR range, start cool down and test is complete. Test is incomplete but can be stopped if over 12 minutes if not in submaximal HR range.
ii. If not steady state HR, continue 1 minute and retake HR* b. Take BP between HRs or at end of stage
8. Submax HR range and steady state HR values (5 bpm or less apart) needs to be achieved in 2 stages of the test for a complete test by the end of Stage 3 or 4
9. Test should be terminated if:
11

a. Shows adverse signs and symptoms b. Request stopping
10. Cool down with minimal resistance for 3‐5 minutes, retaking HR and BP every 2‐3 minutes and end of cool down VO2 max Prediction Equation:
VO2 in stage second highest called submax VO21
VO2 in stage highest called submax VO22
HR in 2nd highest stage called HR1
HR in highest stage called HR2
Maximal predicted HR = 208 * (0.7 *age) First calculate the slope: b = (VO22‐ VO21)/(HR2– HR1) Then predict VO2 max = VO22 + b(HRmax – HR2) Bruce Treadmill Test General: multistage treadmill test with 2‐4 stages with “steady state” HR determined in each stage. Note that the original protocol states that HR should be between 110 and 170 bpm (note that this is written in the protocol but this only corresponds to young‐middle age adults. Older adult 65yrs 60% HR max = 100bpm so remember to keep this in perspective). Protocol:
1. Take resting vitals HR, BP and explain RPE 2. Calculate submaximal HR range for your patient (60‐85% of HR max) 3. Determine where to start (modified or standard protocol). Regardless of “stage” of start, it needs to be near
subjects submaximal HR range:
Stage *M1(modified): Begin warm up 1.7 mph with 0% grade (no elevation) for 3 minutes o Take HR at minute 2 and 3 for steady state HR determination (5 bpm or less apart)
If not steady state HR, continue 1 minute and retake HR
Stage *M2(modified): Adjust resistance to 1.7 mph and 5% grade o Take HR at minute 2 and 3 for steady state HR determination (5 bpm or less apart)
If not steady state HR, continue 1 minute and retake HR
Stage 1: Adjust resistance to 1.7 mph and 10% grade o Take HR at minute 2 and 3 for steady state HR determination (5 bpm or less apart)
If not steady state HR, continue 1 minute and retake HR o Take BP between HRs (and RPEs) or at end of stage o If submax HR achieved in 2 stages, cool down
note – if submax HR isn’t achieved in 2 stages, continue
Stage 2: Adjust resistance to 2.5 mph and 12% grade o Take HR at minute 2 and 3 for steady state HR determination (5 bpm or less apart)
If not steady state HR, continue 1 minute and retake HR o Take BP between HRs (and RPE) or at end of stage o If submax HR achieved in 2 stages, cool down
note – if submax HR isn’t achieved in 2 stages, continue
Stage 3: Adjust resistance to 3.4 mph and 14% grade* o Take HR at minute 2 and 3 for steady state HR determination (5 bpm or less apart)
If not steady state, continue 1 minute and retake HR o Take BP between HRs (and RPE) or at end of stage o If submax HR achieved in 2 stages, cool down
note – if submax HR isn’t achieved in 2 stages, continue
Stage 4: Adjust resistance to 4.2 mph and 16% grade* o Take HR at minute 2 and 3 for steady state HR determination (5 bpm or less apart)
If not steady state, continue 1 minute and retake HR 12

o Take BP between HRs (and RPE) or at end of stage o If submax HR achieved in 2 stages, cool down
note – if submax HR isn’t achieved in 2 stages, test might need to be terminated depending how long the test has been running. If >12 minutes, then terminate testing and cool down.
Stage 5: Adjust resistance to 5.0 mph and 18% grade* o Take HR at minute 2 and 3 for steady state HR determination (5 bpm or less apart)
If not steady state, continue 1 minute and retake HR o Take BP between HRs (and RPE) or at end of stage o If submax HR achieved in 2 stages, cool down
note – if submax HR isn’t achieved in 2 stages, test might need to be terminated depending how long the test has been running. If >12 minutes, then terminate testing and cool down.
4. Submaximal HR range (60‐85% of HR max) and steady state HR (1‐5 bpm apart) needs to be achieved in 2 stages for a complete test
5. Test should be terminated if: a. Shows adverse signs and symptoms b. Request stopping
6. Cool down with minimal resistance for 3‐5 minutes, retaking HR and BP at 2‐3 minutes and end of cool down *If treadmill doesn’t go up to the percent % grade stated in the protocol, you must calculate new higher speed using VO2 equations to make up for a lower grade. VO2 max Prediction Equation:
VO2 in stage second highest called submax VO21
VO2 in stage highest called submax VO22
HR in 2nd highest stage called HR1
HR in highest stage called HR2
Maximal predicted HR = 208 * (0.7 *age) First calculate the slope: b = (VO22‐ VO21)/(HR2– HR1) Then predict VO2 max = VO22 + b(HRmax – HR2)
13

Objectively Measuring Hypertrophy, Strength, Power, and Muscle Endurance Hypertrophy
The best way to assess increases in muscle mass is with dual x‐ray absorptiometry or DEXA. While this is very accurate, it
is not very applicable in the clinic. When muscles hypertrophy there is an increase in the size of the muscle. So girth
measures are the most clinically relevant way to assess hypertrophy. However, keep in mind that girth measures are
only accurate for hypertrophy in younger adults and children. In middle aged and older adults the replacement of
muscle mass by adipose and connective tissue makes girth measurements unreliable. Strength measures are used as a
proxy measure of hypertrophy because as a muscle hypertrophies, strength increases.
Strength
There are two objective methods for assessing strength presented here‐‐ hand held dynamometry and repetition
maximum testing. Manual muscle testing is another method for assessing strength, but it lacks the reliability and
sensitivity to make it a good outcome measure for the effects of therapeutic exercise. It can however be used as an
effective screen to determine muscles or muscle groups that require a more in‐depth assessment.
Hand held dynamometry uses a strain gauge to detect how much force an individual is exerting. It measures isometric
strength and provides a sensitive, objective measure of strength. In addition it has good to excellent reliability—intra
tester, intertester, intrasession, and among units.
When doing hand held dynamometry, the first step is choosing a test position. There is no “one” way to do hand held
dynamometry. Manual muscle test positions, positions used in other research studies, or positions developed by the
tester are all options. The important thing is to document the test position so it can be duplicated on subsequent tests.
Included in the test position is not only the body position, but also the angle at which the test occurs. Remember hand
held dynamometry is an isometric test and since the muscle is stronger at different points in the arc of movement, the
angle at which is tested is important. Hand held dynamometry values should be the average of at least two tests and the
two tests should be within 10% of each other. If they are not, there was some error in the method. The most important
thing to keep in mind for accurate measures is the patient’s force needs to be met, but not overcome. As a result, the
tester should not move the patient and the patient should not move the tester. If the tester moves the patient, all the
dynamometer is measuring is how strong is the tester Similarly, if the patient moves the tester, the dynamometer is not
assessing the patient’s full strength—it is only measuring how much force is needed to overcome the tester. When
patients are stronger than testers, the tester can position his or herself to have a mechanical advantage over the
patient.
Another way to assess strength is to determine the repetition maximum (RM). This method is reliable and valid and
measures strength isotonically so it lays the foundation for the intensity of the exercise program. A 1RM is simply the
amount of weight an individual can lift one time and one time only with good form through the intended range. If one
more pound is added the patient cannot go through the intended range, or compensates in order to go through the
intended range. If one pound is removed, the patient is able to perform more than one repetition.
In performing a 1RM assessment, determine which muscle to test. This is often done by using a manual muscle test to
screen and the patient’s subjective information to help determine which muscle or muscles most need resistance
training. Next, determine the test position. This should be the same position in which the patient will exercise. Assessing
a patient’s hip abduction strength in standing then exercising in sidelying because you are concerned he could fall in
14

standing results in an inaccurate intensity prescription. The 1RM determined in standing will be much lighter than the
1RM in sidelying because of the effect of gravity and the weight of the leg. So prescribing an exercise off a different
position will not provide an accurate intensity. Once the test position is established, instruct the patient in how to do the
exercise. Then observe the patient performing the exercise without any weight. This observation accomplishes two
purposes: ensuring the patient is performing the exercise correctly and determining how far the patient can move in the
exercise because the 1RM is through the intended range and it is necessary to know what is the intended range. Next
resistance is added. How much resistance is really just a guessing game. With practice and experience, it gets easier.
After adding the weight, have the patient do the exercise. If he cannot go through the intended range or if he
compensates, the weight is too heavy. If he does more than one repetition with good form, the weight is too light. The
weight is adjusted accordingly and this trial and error method continues until the patient can do one repetition and one
repetition only with good form. This is their 1RM. It generally takes 3‐5 attempts.
There are other versions of repetition maximum testing like 5 RM and 10 RM. These are very similar to what was just
described except the goal is to determine at what weight the patient can do 5 or 10 repetitions through the intended
range with good form. These alternate methods can be quite fatiguing, but were developed because there are times
when a maximal contraction is not indicated. The 5 RM and 10 RM are solutions for that. Prediction equations are also
solutions for this issue.
These equations allow the tester to choose an arbitrary amount of weight, preferably a weight the patient can lift less
than 20 times and ideally less than 10 times, have the patient lift it as many times as possible with good form, record the
number of repetitions performed and enter the weight used along with the number of repetitions the patient lifted the
weight into the equation. The value obtained is the predicted 1RM. Two such equations are the Lander’s: 1RM = 100 x
rep wt/[101.3‐2.67123(reps)]
and the O’Connor: 1RM = repetition weight [1 + .025 (reps)]. Both of these equations, however, become inaccurate
above 20 repetitions so a weight that is fairly difficult and can be lifted by the patient less than 20 times should be
chosen.
A final method for predicting a 1RM is the Oddvar Holten method. For this method the number of repetitions
corresponds to a specific percentage. (Table A1) This is not the percentage of 1RM. It is simply the Oddvar Holten
percentage. This percentage is divided into the weight used to get the 1RM. This is an acceptable method for predicting
1RM, but is much more conservative than the other prediction equations.
No. of Reps Percentage
1 100
2 95
4 90
7 85
11 80
16 75
22 70
29 65
37 60
46 55
56 50
Oddvar Holten number of repetitions and corresponding percentages
15

Hand Held Dynamometry Testing Positions
Muscle Action
Joint Position
Dynamometer Placement
Subject Stabilization
wrist extension
ashoulder: neutral; elbow: 90º; wrist neutral; fingers relaxed
bshoulder: neutral; elbow 90º; forearm: neutral
a,bjust proximal to the metacarpophalengeal joints
adistal forearm
elbow extension
a,bshoulder: neutral; elbow 90º; forearm: neutral
celbow 90º
a,b,cjust proximal to lateral styloid process aanterior aspect of shoulder or arm
cover biceps belly
elbow flexion
a,bshoulder: neutral; elbow: 90º; forearm: supinated
cshoulder: neutral; elbow 90º; forearm: neutral
a,b,cjust proximal to styloid processes
asuperior aspect of shoulder or arm
cunder epicondyles
shoulder extension
a,bshoulder: flexed 90º; elbow flexed cshoulder: flexed 90º
a,bjust proximal to epicondyles of humerus cproximal to olecranon
asuperior aspect of shoulder cover the acromion
shoulder flexion
ashoulder: flexed 90º; elbow extended
cshoulder: flexed 90º
a,just proximal to epicondyles of humerus cproximal to olecranon
aaxillary region cat thorax
shoulder abduction
a,bshoulder: abducted 45º; elbow extended
a,bjust proximal to lateral epicondyle of humerus
asuperior aspect of shoulder or arm
shoulder lateral rotation
a,bshoulder: abducted 45º; elbow 90º
a,bjust proximal to styloid processes
aelbow
shoulder medial rotation
ashoulder: abducted 45º; elbow 90º ajust proximal to styloid processes
aelbow
hip extension
ctrunk supported at 20º; hip 20º; knee 90º
Cproximal to knee csupport contralateral limb hip and knee at 90º
hip flexion
ahip: flexed 90º; knee relaxed; contralateral limb in neutral
bhip: flexed 90º; knee flexed; contralateral limb in neutral
ctrunk supported at 20º; hip 20º; knee 90º
aat femoral condyles bjust proximal to femoral condyles cproximal to knee
opelvis cover both ASIS
hip abduction
a,bboth lower limbs in neutral aat lateral femoral condyles bjust proximal to lateral joint line of knee
acontralateral limb held in neutral
knee extension
ahip: 90º; knee 90º; hands resting in lap
b,chip: flexed 90º; knee 90º
a,b,cjust proximal to malleoli astabilization at shoulders by assistant
cover the distal thigh
knee flexion
ahip: 90º; knee 90º; hands resting in lap
chip: 90º; knee 90º
a,cjust proximal to malleoli astabilization at shoulders by assistant
cover both shoulders
ankle dorsiflexion
a,bhip, knee, ankle in neutral cankle: in plantarflexion
a,bjust proximal to metatarsophalangeal joints
aknee maintained in full extension; leg supported with foot off table
cover proximal calf
aAndrews AW, Thomas MW, Bohannon RW: Normative values for isometric muscle force measurements obtained with hand-held dynamometers. Phys Ther 76(3):248-59, 1996. Test position: all done supine except knee extension and knee flexion in sitting bBohannon RW: Reference values for extremity muscle strength obtained by hand-held dynamometry from adults aged 20 to 79 years. Arch Phys Med Rehabil 78:26-32, 1997. Test position: all done supine except knee extension in sitting cThe National Isometric Muscle Strength (NIMS) Database Consortium: Muscular weakness assessment: use of normal isometric strength data. Arch Phys Med Rehabil 77:1251-55, 1996. Test position: all done supine except knee extension, knee flexion in sitting and hip extension and hip flexion in 20º trunk supported position.
16

Hand Held Dynamometry Normative Data—Older Male Subjects
Non-Dominant Side Dominant Side
50-59 years 60-69 years 70-79 years Muscle Action
50-59 years 60-69 years 70-79 years
lbs. % BW lbs. % BW lbs. % BW lbs. % BW lbs. % BW lbs. % BW
31.3 (6.2)
16.6 (2.3)
27.3 (5.4)
15.9 (3.3)
27.0 (4.6)
16.4 (3.0)
Wrist Ext
33.5 (7.0)
16.6 (2.3)
29.6 (4.9)
17.1 (3.3)
28.1 (4.4)
16.9 (2.6)
39.9 (7.7)
21.3 (3.8)
35.4 (7.6)
20.4 (3.8)
34.4 (6.4)
20.8 (3.4)
Elbow Ext
42.2 (7.4)
22.5 (3.3)
36.7 (9.3)
21.2 (4.2)
34.6 (7.6)
20.7 (4.0)
61.2 (12.3)
32.7 (5.8)
55.8 (8.0)
32.3 (4.2)
52.0 (9.1)
31.4 (5.7)
Elbow Flex
65.7 (10.8)
35.0 (5.1)
58.2 (10.6)
24.5 (5.0)
53.1 (34.4)
32.0 (5.5)
68.0 (11.5)
36.3 (4.7)
60.8 (11.3)
35.3 (6.0)
56.5 (10.6)
34.1 (6.9)
ShouldExt
72.1 (12.2)
38.4 (4.9)
63.0 (12.8)
36.5 (6.5)
59.2 (12.1)
35.8 (7.6)
57.3 (11.5)
30.9 (5.3)
50.0 (7.4)
29.2 (4.8)
46.8 (8.8)
28.3 (4.9)
ShouldFlex
60.2 (10.3)
32.1 (4.3)
52.1 (9.5)
30.3 (5.3)
46.8 (8.8)
28.3 (5.3)
49.9 (8.8)
26.8 (3.8)
43.5 (9.5)
25.3 (5.5)
41.7 (6.8)
25.2 (4.3)
ShouldAbd
53.5 (12.5)
28.5 (5.7)
45.1 (10.3)
26.1 (5.6)
43.2 (8.6)1
26.1 (5.5)
34.2 (6.1)
18.4 (2.6)
29.5 (5.6)
17.3 (4.3)
29.1 (6.4)
17.7 (4.3)
ShouldER
35.1 (7.4)
18.7 (3.3)
31.3 (6.1)
18.2 (3.6)
29.9 (5.5)
18.2 (4.2)
41.0 (8.5)
21.8 (3.3)
35.1 (5.1)
20.3 (2.7)
33.7 (6.4)
20.5 (4.2)
ShouldIR
43.4 (9.0)
23.1 (3.5)
36.7 (6.5)
21.2 (3.1)
34.1 (7.5)
20.6 (4.8)
46.3 (11.5)
24.6 (5.5)
41.4 (9.5)
24.2 (6.2)
36.2 (10.0)
21.6 (5.5)
Hip Flex
45.4 (13.0)
24.1 (6.1)
41.0 (10.3)
24.0 (6.6)
36.6 (9.3)
22.0 (5.4)
66.1 (15.0)
35.3 (7.5)
60.1 (14.2)
35.0 (8.5)
53.9 (12.2)
32.6 (7.9)
Hip AB
68.2 (14.5)
36.3 (6.7)
58.6 (12.1)
34.3 (7.7)
56.5 (12.1)
34.2 (8.1)
98.7 (15.3)
52.9 (8.1)
85.1 (15.6)
49.3 (8.0)
81.9 (15.1)
49.3 (8.2)
Knee Ext
100.6 (15.0)
53.9 (8.4)
81.5 (16.1)
47.4 (8.5)
80.3 (18.1)
48.2 (10.2)
54.5 (11.8)
29.0 (5.0)
50.6 (10.6)
29.2 (5.7)
46.4 (8.3)
27.9 (4.8)
Knee Flex
56.4 (13.6)
29.9 (5.7)
52.3 (9.8)
30.4 (5.7)
48.6 (9.2)
29.3 (5.4)
63.8 (17.1)
34.0 (8.2)
54.5 (13.5)
31.4 (8.8)
47.3 (11.8)
28.6 (7.6)
AnkleDF
65.4 (18.7)
34.7 (8.3)
52.9 (13.4)
30.6 (7.7)
49.8 (12.7)
30.1 (8.2)
From: Andrews AW, et al: Normative values for isometric muscle force measurements obtained with hand-held dynamometers. Phys Ther 76:248-59, 1996. n = 77 asymptomatic healthy males (50-79 years) Standard Deviation: noted below force measure in ( ): any value below two standard deviations from mean may be considered a below normal force measure % = muscle force/body weight measured in the same units (i.e. muscle lbs./body weight lbs.; expresses muscle force percentage of body weight
17

Hand Held Dynamometry Normative Data—Older Female Subjects
Non-Dominant Side Muscle Action
Dominant Side
50-59 years 60-69 years 70-79 years 50-59 years 60-69 years 70-79 years
lbs. % BW lbs. % BW lbs. % BW lbs. % BW lbs. % BW lbs. % BW
18.6
(4.4) 12.3
(2.6) 15.8
(3.0) 11.0
(2.1) 16.0
(3.0) 12.0
(2.4) Wrist Ext
20.4
(4.9) 13.4
(2.7) 17.8
(3.5) 12.4
(2.4) 17.8
(3.9) 13.4
(3.3)
23.5
(5.2) 15.5
(3.2) 21.7
(5.4) 15.0
(3.5) 20.3
(3.5) 15.3
(2.7) Elbow
Ext 24.4
(5.5) 16.0
(2.7) 21.6
(5.1) 15.0
(3.6) 20.7
(4.0) 15.7
(3.7)
36.0
(6.0) 23.9
(4.3) 33.9
(5.9) 23.5
(4.2) 31.8
(5.2) 23.8
(3.4) Elbow Flex
37.5
(6.4) 24.8
(4.0) 35.2
(6.6) 24.5
(5.0) 31.1
(5.9) 23.3
(3.7)
38.9
(8.9) 25.7
(6.2) 33.0
(6.1) 22..9
(4.2) 31.3
(7.0) 23.5
(5.3) Should
Ext 40.6
(8.5) 26.9
(5.8) 34.4
(7.8) 23.9
(5.5) 32.9
(7.2) 24.6
(5.0)
33.6
(5.9) 22.2
(3.9) 31.6
(6.1) 21.9
(3.7) 27.1
(4.8) 20.5
(4.2) Should
Flex 36.3
(6.8) 24.0
(4.2) 33.2
(6.9) 23.0
(4.9) 27.4
(5.0) 20.7
(4.3)
28.1
(5.7) 18.6
(4.3) 25.7
(4.6) 17.8
(3.0) 24.4
(4.7) 18.4
(4.0) Should
Abd 30.4
(5.5) 20.1
(3.9) 28.1
(5.8) 19.5
(3.9) 24.1
(4.7) 17.9
(3.4)
21.6
(4.6) 14.3
(2.9) 19.2
(3.7) 13.3
(2.1) 17.9
(3.1) 13.6
(3.2) Should
ER 22.6
(4.6) 15.0
(3.2) 19.9
(4.2) 13.7
(2.7) 18.5
(2.8) 13.9
(2.6)
22.7
(4.5) 15.0
(3.1) 20.2
(4.1) 14.0
(2.5) 18.9
(3.1) 14.2
(2.3) Should
IR 22.9
(4.5) 15.1
(3.1) 20.8
(4.2) 14.4
](3.0) 19.3
(3.9) 14.5
(2.6)
28.9
(5.9) 19.3
(4.8) 27.3
(4.7) 19.0
(2.5) 22.9
(5.7) 17.2
(4.3) Hip
Flex 30.3
(6.5) 20.2
(5.0) 27.6
(5.2) 19.2
(3.7) 23.3
(5.8) 17.6
(4.6)
44.9
(9.3) 30.1
(7.8) 42.1
(10.0) 29.0
(5.9) 36.1
(8.0) 27.2
(6.2) Hip
AB 45.5
(9.1) 30.3
(7.0) 42.4
(9.9) 29.2
(6.0) 38.6
(9.1) 28.8
(6.2)
66.1
(17.5) 43.6
(10.8) 55.7
(14.9) 38.4
(8.8) 50.6
(11.5) 38.0
(8.6) Knee
Ext 67.0
(19.4)44.2
(12.4)57.8
(13.0) 39.9
(8.0) 50.7
(10.7) 38.0
(7.2)
38.1
(10.4) 25.0
(5.8) 34.5
(6.6) 23.9
(4.1) 31.8
(8.5) 23.7
(5.5) Knee Flex
38.0
(9.0) 25.0
(5.0) 35.3
(6.1) 24.6
(4.6) 30.8
(7.7) 23.0
(5.2)
42.5
(11.1) 28.5
(8.9) 39.9
(11.3) 27.6
(6.7) 34.5
(8.2) 25.9
(6.6) Ankle
DF 43.7
(13.4)29.4
(11.0)38.5
(9.5) 26.5
(5.2) 35.9
(9.9) 27.1
(8.9)
From: Andrews AW, et al: Normative values for isometric muscle force measurements obtained with hand-held dynamometers. Phys Ther 76:248-59, 1996. n = 70 asymptomatic healthy females (50-79 years) Standard Deviation: noted below force measure in ( ): any value below two standard deviations from mean may be considered a below normal force measure % = muscle force/body weight measured in the same units (i.e. muscle lbs./body weight lbs.; expresses muscle force percentage of body weight
18

Power Testing
When assessing power, strength can be used as a proxy measure because power has a component of strength and as
strength improves, so too should power. In addition, it is helpful to try to assess power more directly. Clinically this
presents a challenge unless there is isokinetic equipment or a fitrodyne on weight stack machines. For the majority of
rehabilitation professionals who do not have these, the use of functional measures can be useful when those measures
are correlated with power. For example chair rise, gait velocity, and stair climb are all correlated with lower extremity
power and therefore as lower extremity power improves, scores on these tests will also. Similarly, the seated medicine
ball toss is correlated to upper extremity power and scores will improve on this test as upper extremity power improves.
Muscle Endurance Testing
Muscle endurance is assessed primarily using one of two methods—repetitions to failure and duration to failure. Both
assess endurance but repetitions to failure assesses dynamic endurance whereas duration to failure assesses static
endurance. Dynamic endurance is the ability of the muscle to repetitively contract over time. This occurs with the tibialis
anterior during gait in order to repetitively achieve dorsiflexion for each step. There is a low load—just the weight of the
foot and shoe– and the tibialis anterior contracts hundreds of time consecutively. Static endurance is the ability of the
muscle to maintain a contraction over time. This occurs with the quadriceps in standing (unless you lock out your knees
and hang on your ligaments). The quadriceps must maintain a low level contraction for the duration of standing. If it
does not remain contracted, the knee buckles.
Assessing repetitions to failure is similar to predicting a 1RM except the patient is intentionally given a low load
performs as many contractions as possible stopping only when fatigue is reached and form breaks down. The weight
used and the number of repetitions performed is recorded and used as a benchmark against which to compare progress.
Upon reassessment the same weight is used and the number of repetitions counted. Progress is shown by the ability to
perform more repetitions.
Assessing duration to failure is the same concept but instead of having the patient do as many repetitions possible, the
patient holds the contraction as long as possible. A weight is placed on the limb, the patient to contracts the muscle, and
holds until fatigue occurs and the same angle can no longer be maintained. The length of time the muscle contracted is
recorded and used as a benchmark against which to compare progress. Upon reassessment the same weight is used and
length of time counted. Progress is shown by the ability to hold for a longer period of time.
19

Parameters for Novice Resistance Training
STRENGTH HYPERTROPHY POWER ENDURANCE
MUSCLE ACTION
concentric and eccentric
concentric and eccentric
concentric and eccentric
concentric and eccentric
LOAD 60‐80% of 1 RM 70‐85% of 1 RM 30‐80% of 1 RM 30‐60% of 1 RM
VOLUME (reps and sets)
7‐12R X 1‐4S 6‐10R X 1‐3S 7‐30R X 1‐3S
12‐30R X 4‐7S
EXERCISE SELECTION
multi joint and single joint
multi joint and single joint
multi joint multi joint and single joint
EXERCISE ORDER
large before small
multi joint before single joint
higher intensity before lower intensity
large before small
multi joint before single joint
higher intensity before lower intensity
large before small
multi joint before single joint
higher intensity before lower intensity
various sequencing combinations
REST PERIODS 2‐3 minutes for multi joint exercises using heavy loads
1‐2 minutes for assistance exercises
1‐2 minutes 2‐3 minutes for multi joint exercises using heavy loads
1‐2 minutes for assistance exercises
<1 minute
VELOCITY slow and moderate slow to moderate fast intentionally slow
FREQUENCY 2‐3 x/week 2‐3 x/week 2‐3 x/week 2‐3 x/week
Parameters for resistance training in individuals who are novice. A side‐by‐side comparison of parameters for strength,
hypertrophy, power, and endurance (RM=repetition maximum; R=repetition; S=sets; <=less than; x=times; /=per)
20

Parameters for Intermediate Resistance Training
STRENGTH HYPERTROPHY POWER ENDURANCE
MUSCLE ACTION
concentric and eccentric
concentric and eccentric
concentric and eccentric
concentric and eccentric
LOAD 60‐80% of 1 RM 70‐85% of 1 RM 30‐80% of 1RM 30‐60% of 1 RM
VOLUME (reps and sets)
7‐12R X 1‐4
6‐10R X 1‐3 7‐30R X 1‐3
12‐30R X 4‐7
EXERCISE SELECTION
multi joint and single joint
multi‐joint and single joint
multi joint multi joint and single joint
EXERCISE ORDER
large before small
multi joint before single joint
higher intensity before lower intensity
large before small
multi joint before single joint
higher intensity before lower intensity
large before small
multi joint before single joint
higher intensity before lower intensity
various sequencing combinations
REST PERIODS 2‐3 minutes for multi joint exercises using heavy loads
1‐2 minutes for assistance exercises
1‐2 minutes 2‐3 minutes for multi joint exercises using heavy loads
1‐2 minutes for assistance exercises
<1 minute
VELOCITY moderate slow to moderate fast to very fast intentionally slow
FREQUENCY 2‐3 x/week 2‐3 x/week 2‐3 x/week 2‐3 x/week
Parameters for resistance training in individuals who are intermediate. A side‐by‐side comparison of parameters for
strength, hypertrophy, power, and endurance (RM=repetition maximum; R=repetition; S=sets; <=less than; x=times;
/=per)
21

Parameters for Advanced Resistance Training
STRENGTH HYPERTROPHY POWER ENDURANCE
MUSCLE ACTION
concentric and eccentric
concentric and eccentric
concentric and eccentric
concentric and eccentric
LOAD 70‐85% of 1 RM 70‐100% of 1RM
30‐85% of 1 RM 30‐60% of 1 RM
VOLUME (reps and sets)
6‐10R X 4‐6
1‐10R X 3‐6
6‐308R X 3‐6 12‐30R X 4‐7
EXERCISE SELECTION
multi joint and single joint
multi joint and single joint
multi joint multi joint and single joint
EXERCISE ORDER
large before small
multi joint before single joint
higher intensity before lower intensity
large before small
multi joint before single joint
higher intensity before lower intensity
large before small
multi joint before single joint
higher intensity before lower intensity
various sequencing combinations
REST PERIODS 2‐3 minutes for multi joint exercises using heavy loads
1‐2 minutes for assistance exercises
2‐3 minutes for high intensity
1‐2 minutes for moderate to moderate high intensity
2‐3 minutes for multi joint exercises using heavy loads
1‐2 minutes for assistance exercises
1‐2 minutes for > 15R
<1 minute for 10‐15R
VELOCITY unintentionally slow to fast
slow to fast fast very fast
intentionally slow with 10‐15R
moderate to fast for > 15R
FREQUENCY 2‐3 x/week 2‐3x/week 2‐3 x/week 2‐3 x/week
Parameters for resistance training in individuals who are advanced. A side‐by‐side comparison of parameters for
strength, hypertrophy, power, and endurance (RM=repetition maximum; R=repetition; S=sets; <=less than; x=times;
/=per)
22

Advanced Coordination Examples (dual tasking and perturbations):
Walking Tasks with dual/multi tasking: Balance during walking can be trained over three different domains. Choose the
activity from each domain that the participant has the hardest time performing (lowest level of performance). Attempt
to perform 3 repetitions of each. Document the level and repetitions for each corresponding activity.
Domain 1: 1) Fast walking, 2) Fast walk wide circle, 3) Fast walk narrow circle, 4) Fast walk figure 8
Domain 2: 1) Line walking, 2) Heel walking, 3) Toe walking
Domain 3: 1) Side stepping , 2) Braiding, 3) Backward walking
Level 1: firm surface
Level 2: firm surface carrying 5 pound object
Level 3: firm surface with cognitive dual task (spelling or simple math)
Level 4: foam
Level 5: foam carrying 5 pound object
Level 6: foam with cognitive dual task (spelling or simple math)
Level 7: random direction changes
Static Stance with Manual Perturbation: Patients will receive manual unpredictable perturbations in ML/AP directions
while in stance positions for 3x30 seconds to knee first then progress to full body. You can progress difficulty of stance
positions and surfaces as well as perturbations.
Level 1: Bilateral Stance progress to increased loading
Level 2: Single limb stance
Level 3: Single limb stance on foam
Level 4: Single limb stance on balance board
Level 5: Single limb stance on balance board with foam
23

References
ACSM. ACSM’s Guidelines for Exercise Testing and Prescription (9th ed). Baltimore, MD: Lippincott William &Wilkins,
2013.
American Physical Therapy Association. Guide to physical therapy practice; 2003 Archer SK, Wellwood I, Smith CH, Newham DL. Dysphagia therapy in stroke: a survey of speech and language therapists.
Int J Lang Commun Disord. 2013;48(3)283‐296.
Anemaet WK, Hammerich AS. A framework for exercise prescription. Top Geriatr Rehabil 2014;30(2):79‐101.
Argolo N, Sampaio M, Pinho P, Melo A, Nobrega AC. O swallowing exercises improving swallowing dynamic and quality
of life in Parkinson’s disease? Neuro Rehabil. 2013;32:949‐955.
Avin KG, Law LA. Age related differences in muscle fatigue vary by contraction type: a meta‐analysis. Phys Ther.
2011;91(8):1153‐1165.
Behm DG, Chaouachi A. A review of the acute effects of static and dynamic stretching on performance. Eur J Appl
Physiol. 2011;111(11):2633‐2651.
Brack AS, Rando TA. Tissue‐specific stem cells: lessons from the skeletal muscle satellite cell. Cell Stem Cell.
2012;10(5):504‐514.
Brenantano MA, Kruel LF. A review on strength exercise‐induced muscle damage: applications, adaptation mechanisms
and limitations. J Sports Med Phys Fit. 2011;51(1):1‐10.
Brett D. A review of collagen and collagen‐based wound dressings. Wounds Compend Clin Res Pract. 2008;20(12):347‐
356.
Carroll TJ, Herbert RD, Munn J, Lee M, Gandevia SC. Contralateral effects of unilateral strength training: evidence and
possible mechanisms. J Appl Physiol. 2006;101:1514‐1522.
Chalmers G. Re‐examination of the possible role of Golgi tendon organ and muscle spindle reflexes in proprioceptive
neuromuscular facilitation muscle stretching. Sports Biomech. 2004;3(1):159‐183.
Chang Y, Pan C, Chen F, Tsai C, Huang C. Effect of resistance exercise training on cognitive function in healthy older
adults: a review. J Aging Phys Act. 2012;20(4):497‐517.
Chen MR, Dragoo JL. The effect of nonsteroidal anti‐inflammatory drugs on tissue healing. Knee Surg Sports Traumatol
Arthrosc. 2013;21(3):540‐549.
Clark HM. Specificity of training in the lingual musculature. J Speech Lang Hear Res. 2012; 55:657‐667.
Clark, DJ, Projednic RM, Reid KF, et al. Longitudinal decline of neuromusclular activation and power in healthy older
adults. J Gerontol Biol Sci Med Sci. 2013;68(11):1419‐1425.
Corti M, McGuirk TE, Wu SS, Patten C. Differential effects of power training versus functional task practice on compensation and restoration of arm function after stroke. Neurorehabil Neural Repair. 2012;26(7):842‐854.
24

Crary MA, Carnaby GD, LaGorio LA, Carvajal PJ. Functional and physiological outcomes from an exercise based dysphagia
therapy: a pilot investigation fo the McNeill Dysphagia Therapy Program. Arch Phys Med Rehabil. 2012; 93:1173‐1180.
Crary MA, Carnaby GD. Adoption into clinical practice of two therapies to manhage swallowing disorders: exercise‐based
swallowing rehabilitation and electrical stimulation. Curr Opin Olotlaryngol Head Neck Surg. 2014; 22(3):172‐180.
Cyarto EV, Brown WJ, Marshall AL, Trost SG. Comparison of the effects of a home based and group based resistance
training program on functional ability in older adults. Am J Health Prom. 2008;23(1):13‐17.
da Costa TC, Locks RR, Koppe S, et al. Strength and stretching training and detraining on flexibility of older adults. Top
Geratr Rehabil. 2013;29(2):142‐148.
De Deye PG. Application of passive stretch and its implications for muscle fibers. Phys Ther. 2001;81(2):819‐827.
Delavary BM, van der Veer WM, vanEgmond M, Niessen FB, Beelen RHJ. Macrophages in skin injury and repair.
Immunobiol. 2011;216(7):753‐762.
deVos NJ, Singh NA, Ross DA, et al. Effect of power training intensity on the contribution of force and velocity to peak
power in older adults. J Aging Phys Act. 2008;16(4):393‐407.
Dragert K, Zehr EP. High intensity unilateral dorsiflexor resistance training results in bilateral neuromuscular plasticity
after stroke. Exp Brain Res. 2013;225:93‐104.
Endres M, Neumann K, Haupl T, et al. Synovial fluid recruits human mesenchymal progenitors from subchondral
spongious bone marrow. J Orthop Res. 2007;25(10):1299‐1307.
Escalante Y, Saavedra JHM, Garcia‐Hermosa A, et al. Physical exercise and reduction of pain in adults with lower limb
osteoarthritis: a systematic review. J Back Musculoskel Rehabil 2010;23:175‐186.
Fahs C, Rossow L, Seo D, et al. Effect of different types of resistance exercise on arterial compliance and calf blood flow.
Eur J Appl Physiol. 2011;11(12):2969‐2975.
Farmer SE, James M. Contractures in orthopaedic and neurological conditions: a review of causes and treatment. Disabil
Rehabil. 2001;23(13):549‐558.
Fielding RA, LeBrasseur NK, Cuoco A, et al. High velocity resistance training in increases skeletal muscle peak power in
older women. J Am Geriatr Soc. 2002;50(4):655‐662.
Flansbjer UB, Miller M, Downham D, Lexell I. Progressive resistance training after stroke: effects on muscle strength,
muscle tone, gait performance, and perceived participation. J Rehabil Med. 2008;40(1):42‐48.
Folland J, Hawker K, Leach B, Little T, Jones D. Strength training : isometric training at a range of joint angles versus
dynamic training. J Sports Sci. 2005;23(8):817‐824.
Foster C, Porcari JP, Gibson M, Wright G, Greany J, Talati N, Recalde P. Translation of submaximal exercise test responses
to exercise prescription using the talk test. J Strength Cond Res. 2009; 23(9):2425‐2429.
Fuentes JP, Armijo‐Olivo S, Magee DJ, Gross DP. Effects of exercise therapy on endogenous pain‐relieving peptides in
musculoskeletal pain: a systematic review. Clin J Pain 2011; 27:365‐374.
25

Galvao DA, Taaffe DR. Resistance exercise dosage in older adults: single‐ versus multiset effects on physical performance
and body composition. J Am Geriatr Soc. 2005;53(12):2090‐2097.
Galvao DA, Taaffe DR. Single vs multiple set resistance training: recent developments in the controversy. J Strength Cond
Res. 2004;18(3):660‐667.
Gill SD, McBurney J. Does exercise reduce pain and improve physical function before hip or knee replacement surgery? A
systematic review and meta‐analysis of randomized controlled trials. Arch Phys Med Rehabil 2013;94:164‐176.
Goddard AA, Pierce CS, McLeod KJ. Reversal of lower limb edema by calf muscle pump stimulation. J Cardiopulm Rehabil
Prev. 2008;28:174‐179.
Goodwill AM, Pearce AJ, Kidgell DJ. Corticomotor plasticity following unilateral strength training. Muscle Nerve.
2012;46:384‐393.
Grana WA. Healing of articular cartilage: a review. Am J Knee Surg. 2000;13(1):29‐32.
Granacher U, Muehlbauer T, Zahner L, et al. Comparison of traditional and recent approaches int eh promotion of
balance and strength in older adults. Sports Med 2011; 41(5):377‐400.
Greaves NS, Ashcroft KJ, Baguneid M, Bayat A. Current understanding of molecular and cellular mechanisms in
fibroplasia and angiogenesis during acute wound healing. J Dermatol Sci. 2013;72(3):206‐217.
Griffin JW, McClure MH, Bertorini TE. Sequential isometric and manual muscle testing in patients with neuro muscular
disease. Phys Ther. 1986;66:32‐5.
Gupta A,Gupta Y. glucocorticoid induced myopathy: Pathophysiology, diagnosis, and treatment. Ind J Endocr Metab.
2013;17(5):913‐916.
Hall CM, Brody LT. Therapeutic exercise: Moving toward function. 2nd ed. Philadelphia: Lippincott Williams & Wilkins;
2005.
Harris C, DeBeliso MA, Spitzer‐Gibson TA, Adams KJ. The effect of resistance training intensity on strength gain response
in the older adult. J Strength Cond Res. 2004;18(4):833‐838.
Harris ML, Polkey MI, Bath PM, Moxham J. Quadriceps muscle weakness following acute hemiplegic stroke. Clin Rehabil. 2001;15(3):274‐281. Hearps AC, Martin GE, Angelovich TA, et al. Aging is associated with chronic innate immune activation and dysregulation
of monocyte phenotype and function. Aging Cell. 2012;11(5):867‐875.
Hopf HW, Rollins MD. Wounds: an overview of the role of oxygen. Antioxid Redox Sign. 2007;9(8):1183‐1192.
Hortobagyi T, Taylor JL, Petersen NT Russell G, Gandevia SC. Changes in segmental andmomtor cortical output with
contralateral muscle contractions and altered sensory inputs in humans. J Neurophysiol. 2003;90:2451‐2459.
Hovanec N, Sawant A, Overend TJ, Petrella RJ, Vandervoort AA. Resistance training and older adults with type 2 diabetes
mellitus: strength of the evidence. J Aging Res. 2012;1‐12.
Hunter GR, McCarthy JP, Bamman MM. Effects of resistance training on older adults. Sports Med. 2004;34(5):329‐348.
26

Inaba Y, Obuchi S, Arai T, Satake K, Takahira N. The long term effects of progressive resistance training on health related
quality in older adults. J Phyiol Antropol. 2008;27(2):57‐61.
Isherwood L, Lew L, Dean E. Indirect evidence for eccentric muscle contraction during isometric muscle testing
performed with a modified sphygmomanometer. Physio Canada. 1989;41:138‐42.
Katula JA, Rejeski WJ, Marsh AP. Enhancing quality of life in older adults: a comparison of muscular strength and power
training. Health Qual Life Outcomes. 2008;6:1‐8.
Khan KM, Scott A. Mechanotherapy: how physical therapists’ prescription of exercise promotes tissue repair. Br J Sports
Med. 2009;43:247‐251.
Khosla S, Westendorf JJ, Modder UI. Concise review: insights from normal bone remodeling and stem cell‐based
therapies for bone repair. Stem Cells. 2010;28(12):2124‐2128.
Kjaer M. Role of extracellular matrix in adaptation of tendon and skeletal muscle to mechanical loading. Physiol Rev.
2004;84(2):649‐698.
Kokotilo KJ, Eng JJ, Boyd LA. Reorganization of brain function during force production after stroke: A systematic review
of the literature. J Neuro Phys Ther. 2009;33:45‐54.
Kortebein P, Symons TB, Ferrando A, et al. Functional impact of 10 days of bed rest in healthy older adults. J Gerontol A Biol Sci Med Sci. 2008;63:1076–1081. Lee CR, Grodzinsky AJ, Spector M. The effects of cross‐linking of collagen‐glycosaminoglycan scaffolds on compressive
stiffness, chondrocyte‐mediated contraction, proliferation, and biosynthesis. Biomaterials. 2001;22(23):3145‐3154.
Lee M, Gandevia SC, Carroll TJ. Unilateral strength training increases voluntary activation of the opposite untrained limb.
Clin Neurophysiol. 2009;120:802‐808.
Liu C, Latham NK. Progressive resistance strength training for improving physical function in older adults. Coch Data Syst
Rev. 2009;3.
Lotz MK, Draus VB. New developments in osteoarthritis. Post traumatic osteoarthritis: pathogenesis and
pharmacological treatment options. Arthr Res Ther. 2010;12(3):211.
Mackenzie C, Nuir M, Alen C. Non‐speech oro‐motor exercise use in acquired dysarthria management: regimes and
rationales. Int J Lang Commun Disord. 2010; 45(6):617‐629.
Mangione KK, Miller AH, Naughton IV. Improving physical function and performance with progressive resistance
strength training in older adults. Phys Ther. 2010:90(12):1711‐1715.
Markovic G, Mikulic P. Neuro‐musculoskeletal and performance adaptations to lower extremity plyometric training.
Sports Med. 2010;40(10):859‐895.
Marzolini S, Oh P, McIlroy W, Brooks D. The effects of an aerobic and resistance training program on cognition following
stroke. Neurorehabil Neural Repair. 2013; 27:392‐ 402.
Matsuo S, Suzuki S, Iwata M, et al. Acute effects of different stretching durations on passive torque, mobility, and
isometric muscle force. J Strength Cond Res. 2013;27(12):3367‐3376.
27

Mepani R, Antonik S, Massey B, Kern M, Logemann J, et al. Augmentation of deglutitive thyrohyoid muscle shortening by
the Shaker Exercise. Dysphagia. 2009; 24:26‐31.
Miloro KV, Pearson WG, Langmore SE. Effortful pitch glide: a potential new exercise evaluated by dynamic MRI. J Speech
Lang Hearing Res. 2014; 57:1243‐1250.
Mirailes I, Beceiro J, Montull S, Monterde S. Physiopathology of articular stiffness: preventive bases. Fisoterapia.
2007;29(2):90‐98.
Mirhadi S, Ashwood N, Karagkevrekis B. Factors influencing fracture healing. Trauma. 2013;15(2):140‐155.
Moreland JD, Goldsmith CH, Huijbregts MP, et al. Progressive resistance strengthening exercises after strok: a single
blind randomized controlled trial. Arch Phys Med Rehabil. 2003;84(10):1433‐1440.
Morley JE, DeVos JN, Singh NA, et al. Optimal load for increasing muscle power during explosive resistance training in
older adults. J Gerontol Biol Med Sci. 2005;60A(5):638‐647.
Muellbacher W, Facchini S, Boroojerdi B, Hallett M. Changes in motor cortex excitability during ipsilateral hand muscle
activitaion in humans. Clin Neurophysiol. 2000;111:344‐349.
Muller SA, Todorov A, Heisterbach PE, Martin I, Majewski M. Tendon healing: an overview of physiology, biology, and
pathology of tendon healing and systematic review of state of the art in tendon bioengineering. Knee Surg Sports
Traumatol Arthrosc. 2013;21(9):1957‐1962.
Murray PJ, Wynn TA. Protective and pathogenic functions of macrophage subsets. Nat Rev Immunol. 2011;11(11):723‐
737.
Naugle KM, Fillingim RB, Riley JL. A meta‐analytic review of the hypoalgesic effects of exercise J Pain 2012; 13(12):1139‐1150. O’Brien JA, Edwards HE, Finlayson KJ, Kerr G. Understanding the relationships between the calf muscle pump, ankle range of motion, and healing for adults with venous leg ulcers: a review of the literature. Wound Pract Res 2012; 20(2):80‐85. O’Shea SD, Taylor NF, Paratz JD. Progressive resistance exercise improves muscle strength and may improve elements of performance of daily activities for people with COPD: a systematic review. Chest 2009; 136:1269‐1283. O’Sullivan K. McAuliffe S, DeBurca N. The effects of eccentric training on lower limb flexibility: a systematic review. Br J Sports Med 2012; 46:838‐845. Pak S, Patten C. Strengthening to promote functional recovery poststroke: An evidence‐based review. Top Stroke Rehabil. 2008;15(3)177‐199. Peterson MD, Rhea MR, Alvar BA: Applications of the dose‐response for muscular strength development: a review of
meta‐analytic efficacy and reliability for designing training prescription. J Strength Cond Res 19(4):950‐958, 2005.
Raymond MJ, Bramley‐Tzerefos RE, Jeffs KJ, Winter A, Holland AE. Systematic review of high‐intensity progressive
resistance strength training of the lower limb compared with other intensities for strength training in older adults. Arch
Phys Med Rehabil. 2013;94(8):1458‐1472.
Reinke JM, Sorg H. Wound repair and regeneration. Eur Surg Res. 2012;49(1):35‐43.
28

Rice CL, Cunninghan DA, Peterson DH, Rechnitzer PA. Strength in an elderly population. Arch Phys Med Rehabil.
1989;70:391‐7.
Robbins JA, Gangnon RE, Theis SM, Kays SA, Hewitt AL, Hind JA. The effects of lingual exercise on swallowing in older
adults. J Am Geriatr Soc. 2005; 53:1483‐1489.
Sahrmann SA. Diagnosis and treatment of movement impairment syndromes. St. Louis: Mosby; 2002.
Sayers SP. High velocity power training in older adults. Curr Aging Sci 2008; 1(1):62‐67.
Sayers SP, Gibson K. High speed power training in older adults: a shift of the external resistance at which peak power is
produced. J Strength Cond Res. 2013;epub ahead of print
Sereysky JB, Flatow EL, Andarawis‐Puri N. Musculoskeletal regeneration and its implications for the treatment of
tendinopathy. Int J Exp Pathol. 2013;94(4):293‐303.
Sharp SA, Brouwer BJ. Isokinetic strength training of the hemiparetic knee:effects on funcitona nd spasticity. Arch Phys
Med Rehabil. 1997;78(11):1231‐1236.
Simonsick E, Fried LP. Exercise tolerance and body composition. In: Guralniik JM Fried LP, Simonsick EM, et al. eds. The Women’s Health and Aging Study: Health and Social Characteristics of Older Women With Disability. Behedsda, Md: NIA; 1995:106‐117. NIH Publication No. 95‐4009. Singh NA, Stavrinos TM, Scarbek Y, et al. A randomized controlled trial of high versus low intensity weight training versus
general practitioner care for clinical depression in older adults. J Gerontol Biol Sci Med Sci. 2005;60A(6):768‐776.
Sinno H, Prakash S. Complements and the wound healing cascade: an updated review. Plast Surg Int. 2013;146764.
Smith EL, Gilligan C. Physical Activity for the Older Adult. Physician and Sportsmedicine 11:8: 91‐101, 1983. Sran MM. Manual therapy and the osteoporotic spine. 2005. University of British Columbia. Doctoral dissertation.
Stathokostas LD, Little RM, Vandervoor A Patterson DH. Flexibility training and functional ability in older adults: a
systematic review. J Aging Res. 2012;1‐30.
Steib S, Schoene D, Pfeifer K. Dose‐response relationship of resistance training in older adults: a meta‐analysis. Med Sci
Sports Exerc. 2010;42(5):902‐914.
Teller P, White TK. The physiology of wound healing: injury through maturation. Surg Clin North Am. 2009;89(3):599‐
610.
Texiera‐Salmela LF, Olney SJ, Nadeau S, Brouwer B. Muscle strengthening and physical conditioning to reduce impairment and disability in chronic stroke survivors. Arch Phys Med Rehabil. 1999;80(10)1210‐1218.
Thacker SN, Gilchrist J, Stroup DF, Kimsey CD. The impact of stretching on sports injury risk: a systematic review of the
literature. Med Sci Sprts Exerc. 2004;36(3):371‐378.
Tonino RP, Driscoll PA. Reliability of maximal and submaximal parameters of treadmill testing for the measurement of physical training in older persons. J Gerontol. 1988;43:101‐104.
Tsivitse S. Notch and Wnt signaling, physiological stimuli and postnatal myogenesis. Int J Biol Sci. 2010;6(3):268‐281. 29

Turner AN, Jeffreys I. The stretch shortening cycle: proposed mechanisms and methods for enhancement. Strength Cond
J. 2010;32(4):87‐99.
VanSwearingen JM Brach JS. Making Geriatric Assessment Work: Selecting Useful Measures. Phys Ther. 2001;81:1233‐1252. Vescovi J, Fernhall B. Cardiac rehabilitation and resistance training: are they compatible? J Strength Cond Res.
2000;14(3):350‐358.
Vila‐Cha C, Falla D, Correia MV, Farina D. Adjustments in motor unit properties during fatiguing contractions after
training. Med Sci Sports Exerc. 2012;44(4):616‐624.
Voet NBM, van der Kooi EL, Riphagen II, et al. Strength training an aerobic exercise training for muscle disease. Cochrane
Database Syst Rev 2010; 1.
Wada S, Tohara H, Iida T, Inoue M Sato M, Ueda K. Jaw opening exercise for insufficient opening of upper esophageal
sphincter. Arch Phys Med Rehabil. 2012; 93:1995‐1999.
Wallman HW. Stretching and flexibility in the aging adult. Home Health Care Manage Pract. 2009;21:355‐357.
Weier AT, Pearce AJ, Kidgell DJ. Strength training reduces intracortical inhibition. Acta Physiol. 2012;206:109‐119.
Westcott WL, Winett RA, Anderson ES, et l. Effects of regular and slow speed resistance training on muscle strength. J
Sports Med Phys Fitness. 2001;41(2):154‐158.
White ES, Mantovani AR. Inflammation, wound repair, and fibrosis: reassessing the spectrum of tissue injury and
resolution. J Pathol. 2013;229:141‐144.
Wicke J, Gainey K, Figueroa M. A comparison of self‐administered proprioceptive neuromuscular facilitation to static
stretching on range of motion and flexibility. J Strength Cond Res. 2014;28(1):1689‐172.
Yusuf F, Brand‐Saben B. Myogenesis and muscle regeneration. Histochem Cell Biol. 2012;138(2):187‐199.
Zakas A, Balaska P, Grammatikopoulou MG Zakas N, Vergou A. Acute effects of stretching duration on the range of
motion of elderly women. J Body Move Ther. 2005;9(4):270‐276.
30





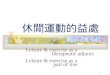



![Vitti] : (Hiroshi Yamaoka) : "J 7 (Sam Kawa) : ANTENNNA VWD-300 . exercise 35 exercise 36 exercise 37 exercise 38 exercise 39 exercise 40 : exercise 41](https://img.pdfslide.tips/doc/110x75/5b479fdd7f8b9a824f8c0adb/anthony-vitti-hiroshi-yamaoka-j-7-sam-kawa-antennna-vwd-300-exercise.jpg)