Embed Size (px)
Citation preview

Comer, Abnormal PsychologyDSM-5 Update, 8e
Stress Disorders
Chapter 6
Slides & Handouts by Karen Clay Rhines, Ph.D.American Public University System

2Comer, Abnormal Psychology, 8e
DSM-5 Update
Stress, Coping, and the Anxiety Response
The state of stress has two components: Stressor – event that creates demands
Stress response – person’s reactions to the demands
Influenced by how we judge both the events and our capacity to react to them effectively
People who sense that they have the ability and resources to cope are more likely to take stressors in stride and respond well

3Comer, Abnormal Psychology, 8e
DSM-5 Update
Stress, Coping, and the Anxiety Response
When we view a stressor as threatening, the natural reaction is arousal and fear Fear is a “package” of responses that are
physical, emotional, and cognitive
Stress reactions, and the fear they produce, are often at play in psychological disorders People who experience a large number of
stressful events are particularly vulnerable to the onset of anxiety and other psychological disorders

Stress, Coping, and the Anxiety Response
Stress also plays a more central role in certain psychological disorders, including: Acute stress disorder Posttraumatic stress disorder (PTSD) Technically, DSM-5 lists these patterns within
a group called "trauma- and stressor-related disorders“
These disorders are triggered by traumatic stressors and include symptoms such as heightened arousal, anxiety, and mood disturbance, and memory difficulties
4Comer, Abnormal Psychology, 8e
DSM-5 Update

Stress, Coping, and the Anxiety Response
The physical disorders of stress are typically called psychophysiological disorders These disorders are listed in DSM-5
under “psychological factors affecting medical condition”
Here significant stressors set in motion an interaction of biological, psychological, and sociocultural factors to help produce or worsen a physical illness or ailment
5Comer, Abnormal Psychology, 8e
DSM-5 Update

6Comer, Abnormal Psychology, 8e
DSM-5 Update
Stress and Arousal: The Fight-or-Flight
Response The features of arousal and fear are
set in motion by the hypothalamus Two important systems are activated:
Autonomic nervous system (ANS) An extensive network of nerve fibers that
connect the central nervous system (the brain and spinal cord) to all other organs of the body
Endocrine system A network of glands throughout the body that
release hormones

7Comer, Abnormal Psychology, 8e
DSM-5 Update
Stress and Arousal: The Fight-or-Flight
Response There are two pathways, or routes,
by which the ANS and the endocrine system produce arousal and fear reactions: Sympathetic nervous system pathway
Hypothalamic-pituitary-adrenal pathway

8Comer, Abnormal Psychology, 8e
DSM-5 Update
Stress and Arousal: The Fight-or-Flight
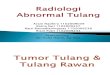
Response When we face a dangerous situation,
the hypothalamus first excites the sympathetic nervous system, which stimulates key organs either directly or indirectly
When the perceived danger passes, the parasympathetic nervous system helps return body processes to normal

The Autonomic Nervous System
9Comer, Abnormal Psychology, 8e
DSM-5 Update

10Comer, Abnormal Psychology, 8e
DSM-5 Update
Stress and Arousal: The Fight-or- Flight
Response The second pathway is the
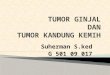
hypothalamic-pituitary-adrenal (HPA) pathway When we are faced by stressors, the
hypothalamus signals the pituitary gland, which stimulates the adrenal cortex to release corticosteroids – stress hormones – into the bloodstream

The Endocrine System
11Comer, Abnormal Psychology, 8e
DSM-5 Update

12Comer, Abnormal Psychology, 8e
DSM-5 Update
Stress and Arousal: The Fight-or-Flight
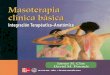
Response The reactions on display in these two
pathways are collectively referred to as the fight-or-flight response
Each person has a particular pattern of autonomic and endocrine functioning and so a particular way of experiencing arousal and fear…

Pathways of Arousal and Fear
13Comer, Abnormal Psychology, 8e
DSM-5 Update

14Comer, Abnormal Psychology, 8e
DSM-5 Update
Stress and Arousal: The Fight-or-Flight
Response People differ in:
Their general level of arousal and anxiety Called “trait anxiety”
Some people are usually somewhat tense; others are usually relaxed
Differences appear soon after birth
Their sense of which situations are threatening
Called “state anxiety”
Situation-based (example: fear of flying)

The Psychological Stress Disorders
During and immediately after trauma, we may temporarily experience levels of arousal, anxiety, and depression For some, symptoms persist well after the
trauma These people may be suffering from:
Acute stress disorder Posttraumatic stress disorder (PTSD)
The precipitating event usually involves actual or threatened serious injury to self or others
The situations that cause these disorders would be traumatic to anyone (unlike the anxiety disorders)
15Comer, Abnormal Psychology, 8e
DSM-5 Update

16Comer, Abnormal Psychology, 8e
DSM-5 Update
The Psychological Stress Disorders
Acute stress disorder Symptoms begin within four weeks of
event and last for less than one month
Posttraumatic stress disorder (PTSD) Symptoms may begin either shortly after
the event, or months or years afterward As many as 80% of all cases of acute stress
disorder develop into PTSD

The Psychological Stress Disorders
Aside from the differences in onset and duration, the symptoms of acute stress disorders and PTSD are almost identical: Reexperiencing the traumatic event
Avoidance
Reduced responsiveness
Increased arousal, anxiety, and guilt
17Comer, Abnormal Psychology, 8e
DSM-5 Update

18Comer, Abnormal Psychology, 8e
DSM-5 Update
What Triggers a Psychological Stress
Disorder? Can occur at any age and affect all aspects of life At least 3.5% of people in the U.S. are affected each year
7–9% of people in the U.S. are affected sometime during their lifetime
Around two-thirds seek treatment at some point Ratio of women to men is 2:1
After trauma, around 20% of women and 8% of men develop disorders
In addition, people with low incomes are twice as likely as people with higher incomes to experience one of the stress disorders
Some events – including combat, disasters, abuse, and victimization – are more likely to cause disorders than others

19Comer, Abnormal Psychology, 8e
DSM-5 Update
What Triggers a Psychological Stress
Disorder? Combat and stress disorders
For years clinicians have recognized that soldiers experience distress during combat
Called “shell shock” or “combat fatigue” Post-Vietnam War clinicians discovered that soldiers
also experienced psychological distress after combat As many as 29% of Vietnam combat veterans
suffered acute or posttraumatic stress disorders An additional 22% had some stress symptoms 10% still experiencing problems
A similar pattern is currently unfolding among veterans of wars in Afghanistan and Iraq

20Comer, Abnormal Psychology, 8e
DSM-5 Update
What Triggers a Psychological Stress
Disorder? Disasters and stress disorders
Acute and posttraumatic stress disorders may also follow natural and accidental disasters
Types of disasters include earthquakes, floods, tornadoes, fires, airplane crashes, and serious car accidents
Because they occur more often, civilian traumas have been implicated in stress disorders at least 10 times as often as combat traumas

What Triggers a Psychological Stress
Disorder? Victimization and stress disorders
People who have been abused or victimized often experience lingering stress symptoms
Research suggests that more than one-third of all victims of physical or sexual assault develop PTSD
As many as half of those directly exposed to terrorism or torture may develop this disorder
21Comer, Abnormal Psychology, 8e
DSM-5 Update

What Triggers a Psychological Stress
Disorder? Victimization and stress disorders
A common form of victimization is sexual assault/rape
Around 1 in 6 women is raped at some time during her life
Psychological impact is immediate and may be long-lasting
One study found that 94% of rape survivors developed an acute stress disorder within 12 days after assault
22Comer, Abnormal Psychology, 8e
DSM-5 Update

23Comer, Abnormal Psychology, 8e
DSM-5 Update
What Triggers a Psychological Stress
Disorder? Victimization and stress disorders
Ongoing victimization and abuse in the family may also lead to stress disorders

24Comer, Abnormal Psychology, 8e
DSM-5 Update
What Triggers a Psychological Stress
Disorder? Terrorism and torture
The experience of terrorism or the threat of terrorism often leads to posttraumatic stress symptoms, as does the experience of torture
Unfortunately, these sources of traumatic stress are on the rise in our society

25Comer, Abnormal Psychology, 8e
DSM-5 Update
Why Do People Develop a Psychological Stress Disorder?
Clearly, extraordinary trauma can cause a stress disorder However, the event alone may not be the entire
explanation To understand the development of these
disorders, researchers have looked to the: Survivors’ biological processes Personalities Childhood experiences Social support systems Cultural backgrounds Severity of the traumas

26Comer, Abnormal Psychology, 8e
DSM-5 Update
Why Do People Develop a Psychological Stress Disorder?
Biological and genetic factors Traumatic events trigger physical changes in
the brain and body that may lead to severe stress reactions and, in some cases, to stress disorders
Some research suggests abnormal neurotransmitter and hormone activity (especially norepinephrine and cortisol)
Evidence suggests that once a stress disorder sets in, further biochemical arousal and damage may also occur (especially in the hippocampus and amygdala)
There may be a biological/genetic predisposition to such reactions

27Comer, Abnormal Psychology, 8e
DSM-5 Update
Why Do People Develop a Psychological Stress Disorder?
Personality factors Some studies suggest that people with certain
personalities, attitudes, and coping styles are particularly likely to develop stress disorders
Risk factors include: Preexisting high anxiety Negative worldview
A set of positive attitudes (called resiliency or hardiness) is protective against developing stress disorders

28Comer, Abnormal Psychology, 8e
DSM-5 Update
Why Do People Develop a Psychological Stress Disorder?
Childhood experiences Researchers have found that certain childhood
experiences increase risk for later stress disorders
Risk factors include: An impoverished childhood Psychological disorders in the family The experience of assault, abuse, or catastrophe at
an early age Being younger than 10 years old when parents
separated or divorced

Why Do People Develop a Psychological Stress
Disorder? Social support
People whose social support systems are weak are more likely to develop a stress disorder after a traumatic event
29Comer, Abnormal Psychology, 8e
DSM-5 Update

Why Do People Develop a Psychological Stress
Disorder? Multicultural factors
There is a growing suspicion among clinical researchers that the rates of PTSD may differ among ethnic groups in the US
It seems that Hispanic Americans might be more vulnerable to PTSD than other cultural groups
Possible explanations include cultural beliefs systems about trauma and the cultural emphasis on social relationships and social support
30Comer, Abnormal Psychology, 8e
DSM-5 Update

Why Do People Develop a Psychological Stress
Disorder? Severity of the trauma
Generally, the more severe the trauma and the more direct one’s exposure to it, the greater the likelihood of developing a stress disorder
Especially risky: Mutilation and severe injury; witnessing the injury or death of others
31Comer, Abnormal Psychology, 8e
DSM-5 Update

How Do Clinicians Treat the Psychological Stress
Disorders? About half of all cases of PTSD improve
within 6 months; the remainder may persist for years
Treatment procedures vary depending on type of trauma General goals:
End lingering stress reactions
Gain perspective on painful experiences
Return to constructive living
32Comer, Abnormal Psychology, 8e
DSM-5 Update

How Do Clinicians Treat the Psychological Stress
Disorders? Treatment for combat veterans
Drug therapy Antianxiety and antidepressant medications are most
common Behavioral exposure techniques
Reduce specific symptoms, increase overall adjustment Use flooding and relaxation training Use eye movement desensitization and reprocessing
(EMDR) Insight therapy
Bring out deep-seated feelings, create acceptance, lessen guilt
Often use couple, family, or group therapy formats; rap groups
33Comer, Abnormal Psychology, 8e
DSM-5 Update

How Do Clinicians Treat the Psychological Stress
Disorders? Psychological debriefing
A form of crisis intervention that has victims of trauma talk extensively about their feelings and reactions within days of the critical incident
Four-stage approach: Normalize responses to the disaster Encourage expressions of anxiety, anger, and
frustration Teach self-help skills Provide referrals
34Comer, Abnormal Psychology, 8e
DSM-5 Update

How Do Clinicians Treat the Psychological Stress
Disorders? Psychological debriefing
The approach has come under careful scrutiny
While many health professionals continue to believe in the approach despite unsupportive research findings, the current climate is moving away from outright acceptance
It’s possible that certain high-risk individuals may profit from debriefing programs but that others shouldn’t receive such interventions
35Comer, Abnormal Psychology, 8e
DSM-5 Update

36Comer, Abnormal Psychology, 8e
DSM-5 Update
The Physical Stress Disorders: Psychophysiological Disorders
In addition to affecting psychological functioning, stress can also have great impact on physical functioning
The idea that stress and related psychosocial factors may contribute to physical illnesses has ancient roots, yet it had few supporters before the 20th century

37Comer, Abnormal Psychology, 8e
DSM-5 Update
The Physical Stress Disorders: Psychophysiological Disorders
About 80 years ago, clinicians first identified a group of physical illnesses that seemed to result from an interaction of biological, psychological, and sociocultural factors
Early versions of the DSM labeled these illnesses psychophysiological, or psychosomatic, disorders DSM-5 labels them as psychological factors
affecting medical condition

38Comer, Abnormal Psychology, 8e
DSM-5 Update
The Physical Stress Disorders: Psychophysiological Disorders
It is important to recognize that these psychophysiological disorders bring about actual physical damage They are different from “apparent”
physical illnesses like factitious disorders or somatic symptom disorders, which will be discussed in Chapter 7

39Comer, Abnormal Psychology, 8e
DSM-5 Update
Traditional Psychophysiological Disorders
Before the 1970s, the best known and most common of the psychophysiological disorders were ulcers, asthma, insomnia, chronic headaches, high blood pressure, and coronary heart disease
Recent research has shown that many other physical illnesses may be caused by an interaction of psychosocial and physical factors

40Comer, Abnormal Psychology, 8e
DSM-5 Update
Traditional Psychophysiological Disorders
Ulcers Lesions in the wall of the stomach that result
in burning sensations or pain, vomiting, and stomach bleeding
Experienced by over 25 million people at some point in their lives
Causal psychosocial factors: Environmental pressures, intense feelings of anger or
anxiety Causal physiological factors:
Bacterial infection

41Comer, Abnormal Psychology, 8e
DSM-5 Update
Traditional Psychophysiological Disorders
Asthma A narrowing of the body’s airways that makes breathing
difficult Affects up to 25 million people in the U.S. each year
Most victims are children at the time of first attack
Causal psychosocial factors: Environmental pressures or anxiety
Causal physiological factors: Allergies, a slow-acting sympathetic nervous system,
weakened respiratory system

42Comer, Abnormal Psychology, 8e
DSM-5 Update
Traditional Psychophysiological Disorders
Insomnia Difficulty falling asleep or maintaining sleep
Affects 10% of people in the U.S. each year
Causal psychosocial factors: High levels of anxiety or depression
Causal physiological factors: Overactive arousal system, certain medical ailments

43Comer, Abnormal Psychology, 8e
DSM-5 Update
Traditional Psychophysiological Disorders
Chronic headaches Frequent intense aches of the head or neck that are not
caused by another physical disorder Tension headaches affect 45 million Americans each year Migraine headaches affect 23 million Americans each year
Causal psychosocial factors: Environmental pressures; general feelings of helplessness,
anger, anxiety, depression
Causal physiological factors: Abnormal serotonin activity, vascular problems, muscle
weakness

44Comer, Abnormal Psychology, 8e
DSM-5 Update
Traditional Psychophysiological Disorders
Hypertension Chronic high blood pressure, usually
producing few outward symptoms Affects 75 million Americans each year Causal psychosocial factors:
Constant stress, environmental danger, general feelings of anger or depression
Causal physiological factors: 10% caused by physiological factors alone Obesity, smoking, poor kidney function, high
proportion of collagen (rather than elastic) tissue in an individual’s blood vessels

Traditional Psychophysiological Disorders
Coronary heart disease Caused by blockage in the coronary arteries The term refers to several problems, including
myocardial infarction (heart attack) Nearly 18 million people in the US suffer from some
form of coronary heart disease It is the leading cause of death in men older than 35 years and
women older than 40 Causal psychosocial factors:
Job stress, high levels of anger or depression Causal physiological factors:
High level of cholesterol, obesity, hypertension, the effects of smoking, lack of exercise
45Comer, Abnormal Psychology, 8e
DSM-5 Update

46Comer, Abnormal Psychology, 8e
DSM-5 Update
Traditional Psychophysiological Disorders
A number of variables contribute to the development of psychophysiological disorders, including: Biological factors
Psychological factors
Sociocultural factors

47Comer, Abnormal Psychology, 8e
DSM-5 Update
Traditional Psychophysiological Disorders
Biological factors Defects in the autonomic nervous
system (ANS) are believed to contribute to the development of psychophysiological disorders
Other more specific biological problems may also contribute
For example, a weak gastrointestinal system may create a predisposition to developing ulcers

48Comer, Abnormal Psychology, 8e
DSM-5 Update
Traditional Psychophysiological Disorders
Psychological factors According to many theorists, certain
needs, attitudes, emotions, or coping styles may cause people to overreact repeatedly to stressors – increasing their chances of developing psychophysiological disorders
Examples: a repressive coping style, a Type A personality style – particularly hostility and time urgency

Traditional Psychophysiological Disorders
Sociocultural factors Adverse social conditions may set the
stage for psychophysiological disorders One of society’s most adverse social
conditions is poverty
Research also reveals that belonging to an ethnic or cultural minority group increases the risk of developing these disorders and other health problems
49Comer, Abnormal Psychology, 8e
DSM-5 Update

New Psychophysiological Disorders
Clearly, biological, psychological, and sociocultural variables combine to produce psychophysiological disorders
In fact, the interaction of psychosocial and physical factors is now considered the rule of bodily function, not the exception
In recent years, more and more illnesses have been added to the list of psychophysiological disorders
50Comer, Abnormal Psychology, 8e
DSM-5 Update

51Comer, Abnormal Psychology, 8e
DSM-5 Update
New Psychophysiological Disorders
Since the 1960s, researchers have found many links between psychosocial stress and a wide range of physical illnesses

52Comer, Abnormal Psychology, 8e
DSM-5 Update
New Psychophysiological Disorders
Are physical illnesses related to stress? The development of the Social
Adjustment Rating Scale in 1967 enabled researchers to examine the relationship between life stress and the onset of illness

53Comer, Abnormal Psychology, 8e
DSM-5 Update

54Comer, Abnormal Psychology, 8e
DSM-5 Update
New Psychophysiological Disorders
Are physical illnesses related to stress? Using the Social Adjustment Rating Scale,
studies have linked stressors of various kinds to a wide range of physical conditions
Overall, the greater the amount of life stress, the greater the likelihood of illness
Researchers have even found a relationship between traumatic stress and death

55Comer, Abnormal Psychology, 8e
DSM-5 Update
New Psychophysiological Disorders
Are physical illnesses related to stress? One shortcoming of the Social Adjustment
Rating Scale is that it does not take into consideration the particular stress reactions within specific populations
For example, members of minority groups may respond to stress differently and women and men have been shown to react differently to certain life changes measured by the scale

Psychoneuroimmunology
Researchers have increasingly looked to the body’s immune system as the key to the relationship between stress and infection
This area of study is called psychoneuroimmunology
56Comer, Abnormal Psychology, 8e
DSM-5 Update

Psychoneuroimmunology
The immune system is the body’s network of activities and cells that identify and destroy antigens (foreign invaders, such as bacteria) and cancer cells Among the most important cells in this
system are the lymphocytes Lymphocytes are white blood cells that circulate
through the lymph system and the bloodstream, attacking invaders
Lymphocytes include helper T-cells, natural killer T-cells, and B-cells
57Comer, Abnormal Psychology, 8e
DSM-5 Update

Psychoneuroimmunology
Researchers now believe that stress can interfere with the activity of lymphocytes, slowing them down and increasing a person’s susceptibility to viral and bacterial infections
Several factors influence whether stress will result in a slowdown of the system, including biochemical activity, behavioral changes, personality style, and degree of social support
58Comer, Abnormal Psychology, 8e
DSM-5 Update

Psychoneuroimmunology
Biochemical activity Stress leads to increased activity by the
sympathetic nervous system, including a release of norepinephrine
In addition to supporting nervous system activity, this chemical also appears to slow down the functioning of the immune system
Similarly, the body’s endocrine glands reduce immune system functioningduring periods of prolonged stress through the release of corticosteroids
In addition, corticosteroids also trigger increased cytokines, which lead to chronic inflammation
59Comer, Abnormal Psychology, 8e
DSM-5 Update

Psychoneuroimmunology
Behavioral changes Stress may set in motion a series of
behavioral changes – poor sleep patterns, poor eating, lack of exercise, increase in smoking and/or drinking – that indirectly affect the immune system
Personality style An individual’s personality style (including
their level of optimism, constructive coping strategies, and resilience) experience better immune system functioning and are better prepared to fight off illness
60Comer, Abnormal Psychology, 8e
DSM-5 Update

Psychoneuroimmunology
Social support People who have few social supports and
feel lonely seem to display poorer immune functioning in the face of stress than people who do not feel lonely
Studies have found that social support and affiliation with others may actually protect people from stress, poor immune system functioning, and subsequent illness, and can help speed up recovery from illness or surgery
61Comer, Abnormal Psychology, 8e
DSM-5 Update

62Comer, Abnormal Psychology, 8e
DSM-5 Update
Psychological Treatments for Physical Disorders
As clinicians have discovered that stress and related psychosocial factors may contribute to physical disorders, they have applied psychological treatment to more and more medical problems The most common of these interventions are
relaxation training, biofeedback training, meditation, hypnosis, cognitive interventions, support groups, and therapies designed to increase awareness and expression of emotion

63Comer, Abnormal Psychology, 8e
DSM-5 Update
Psychological Treatments for Physical Disorders
The field of treatment that combines psychological and physical interventions to treat or prevent medical problems is known as behavioral medicine

Psychological Treatments for Physical Disorders
Relaxation training People can be trained to relax their muscles
at will, a process that sometimes reduces feelings of anxiety
Relaxation training can help prevent or treat medical illnesses that are related to stress
Often used in conjunction with medication in the treatment of high blood pressure
Often used alone to treat headaches, insomnia, asthma, pain after surgery, certain vascular diseases, and the undesirable effects of cancer treatments
64Comer, Abnormal Psychology, 8e
DSM-5 Update

Psychological Treatments for Physical Disorders
Biofeedback Patients given biofeedback training are
connected to machinery that gives them continuous readings about their involuntary bodily activities
Somewhat helpful in the treatment of anxiety disorders, this procedure has been used successfully to treat headaches and muscular disabilities caused by stroke or accident
Some biofeedback training has been effective in the treatment of heartbeat irregularities, asthma, migraine headaches, high blood pressure, stuttering, and pain
65Comer, Abnormal Psychology, 8e
DSM-5 Update

Psychological Treatments for Physical Disorders
Meditation Although meditation has been practiced since
ancient times, Western health care professionals have only recently become aware of its effectiveness in relieving physical distress
Meditation is a technique of turning one’s concentration inward and achieving a slightly changed state of consciousness
Meditation has been used to manage pain, treat high blood pressure, heart problems, insomnia, and asthma
66Comer, Abnormal Psychology, 8e
DSM-5 Update

Psychological Treatments for Physical Disorders
Hypnosis Individuals who undergo hypnosis are
guided into a sleeplike, suggestible state during which they can be directed to act in unusual ways, to remember unusual sensations, or to forget remembered events
With training, hypnosis can be done without a hypnotist (self-hypnosis)
67Comer, Abnormal Psychology, 8e
DSM-5 Update

Psychological Treatments for Physical Disorders
Hypnosis This technique seems to be particularly
helpful in the control of pain; is now used to treat such problems as skin diseases, asthma, insomnia, high blood pressure, warts, and other forms of infection
68Comer, Abnormal Psychology, 8e
DSM-5 Update

Psychological Treatments for Physical Disorders
Cognitive interventions People with physical ailments have
sometimes been taught new attitudes or cognitive responses as part of treatment
One intervention is stress inoculation training, in which patients are taught to rid themselves of negative self-statements and to replace these with coping self-statements
69Comer, Abnormal Psychology, 8e
DSM-5 Update

Psychological Treatments for Physical Disorders
Emotion expression and support groups If negative psychological symptoms (e.g.,
depression, anxiety) contribute to a person’s physical ills, intervention to reduce these emotions should help reduce the ills
These techniques have been used to treat a variety of illnesses including HIV, asthma, cancer, and arthritis
70Comer, Abnormal Psychology, 8e
DSM-5 Update

Psychological Treatments for Physical Disorders
Combination approaches Studies have found that the various
psychological interventions for physical problems tend to be equal in effectiveness
Psychological treatments are often of greatest help when they are combined and used with medical treatment
With these combined approaches, today’s practitioners are moving away from the mind–body dualism of centuries past
71Comer, Abnormal Psychology, 8e
DSM-5 Update