Embed Size (px)
Citation preview
362 Ann. Ital. Chir., 87, 4, 2016
Comparison of the effects of PRP and hyaluronic acid in promoting peripheral nerve regenerationAn experimental study with vascular conduit model in rats’
Ann. Ital. Chir., 2016 87: 362-374pii: S0003469X16025690
Pervenuto in Redazione Marzo 2016. Accettato per la pubblicazioneMaggio 2016Correspondence to: Ahmet Hamdi Aytekin, MD, Malatya State Hospital,Department of Plastic, Reconstructive and Aesthetic Surgery, TR-44280Malatya, Turkey (e-mail: [email protected])
Cemal Firat*, Ahmet Hamdi Aytekin**, Mehmet Akif Durak***, Yilmaz Geyik°, Serkan Erbatur°°, Metin Dogan°°, Ömer Elmas§, Adile Ferda Dagli§§, Hamit Çelik§§§
* Inonu University School of Medicine, Department of Plastic Surgery, Associate Professor, Malatya, Turkey** Malatya State Hospital, Department of Plastic Surgery, Specialist, Malatya, Turkey *** Inonu University School of Medicine, Department of Neurosurgery, Assistant Professor, Malatya, Turkey ° Bingöl State Hospital, Department of Plastic Surgery, Specialist, Bingöl, Turkey°° Dicle University School of Medicine, Department of Plastic Surgery, Assistant Professor, Diyarbaki r, Turkey°°° Inonu University School of Medicine, Department of Radiology, Associate Professor, Malatya, Turkey§ Bayburt State Hospital, Department of Plastic Surgery, Specialist, Bayburt, Turkey§§ Inonu University School of Medicine, Department of Pathology, Associate Professor, Malatya, Turkey§§§ Bayburt State Hospital, Department of Neurology, Specialist, Bayburt, Turkey
Comparison of the effects of PRP and hyaluronic acid in promoting peripheral nerve regeneration. An experi-mental study with vascular conduit model in rats’
AIM: Peripheral nerve defects generally occur due to mechanical, chemical, thermal and pathologic causes and the recon-struction is still a challenging problem. In the present study, we aimed to compare the effects of platelet rich plasma(PRP) that has high levels of growth factors and hyaluronic acid (HA) that is known to have positive effects on nerveregeneration by decreasing scar formation in a rat model where they were injected through allogeneic aorta graft inperipheral nerve defects using histopathologic and functional methods. MATERIAL AND METHODS: The study involved 20 Wistar Albino male rats that weighed 200 to 250 grams and agedabout 1 year old. Of the rats, two were used as donor for PRP and aorta graft harvest. Three random groups of 6 ratswere composed. In all of the groups, the left sciatic nerves were used and 1 cm of defects were created. The right sci-atic nerves were used as control groups. Group 1 was the group repaired with autograft, Group 2 was the group repairedwith HA injected through aorta graft and Group 3 was the group repaired with PRP injected through aorta graft. Thefindings were evaluated in terms of functional (electromyography and walk test analysis) and histopathologic parametersat 12 weeks. RESULTS: In all of the groups varying degrees of axonal regeneration was observed. Group 1 was the closest group to thecontrol group showing highest rate of nerve regeneration followed by Group 3 where PRP was injected through aortagraft and group 2 where ha was used respectively. CONCLUSION: The study demonstrates that PRP enhances peripheral nerve regeneration more than HA when used in avascular conduit model.
KEY WORDS: Hyaluronic acid, Peripheral nerve regeneration, PRP
Introduction
Peripheral nerve injury is a common casualty, consider-ably more common than spinal cord injury 1. Luckily,unlike injuries requiring reconstruction to the central
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED

nervous system, delicate surgical treatments for periph-eral nerve lesions do exists. Numerous experimental andclinical studies have been conducted in order to obtainbetter sensory and functional outcomes. The micro-instruments, conduit tubes, growth stimulators thatincrease nerve regeneration as well as advances in mol-ecular biology enhanced success rates in peripheral nerverepair. Because complete nerve regeneration does notoccur regardless of the cause of the injury, abnormalnerve regeneration usually results in functional loss andpain 2.The basic principle for peripheral nerve repair is to excisethe scar and fibrotic tissues of the proximal and distaledges of the nerve and a tension-free end-to-endapproach preserving the neurotrophic factors within therepair site. In cases where primary repair is not possi-ble, the gold standard is autograft, however some unde-sired results like scarring, neuroma and denervation ofthe donor site may be observed. So far, several techniques and materials were tested asan alternative to autologous nerve grafts 3. One alterna-tive is the use of allografts, which have shown promis-ing results 4,5. Another option is the use of conduits.Autogenous conduits made of veins or arteries were eval-uated, but they did not show any benefits and demon-strated the same donor area morbidity problems 6-8.In order to increase the functional outcomes of the pri-mary nerve repairs and autografts as well as to decreasethe morbidity, many topical agents have been used onthe anastomosis site including various neurotrophic fac-tors like nerve growth factor (NGF), mitomicin C, apro-tinin, thyroid hormone, human amniotic fluid, hyaluron-ic acid and platelet rich plasma (PRP) 6-15.PRP is a biologic product that found clinical use espe-cially in maxillofacial surgery offering positive impactson bone healing in the recent years. The enhancing effectof PRP is based on the premise that the large numberof platelets in PRP release significant quantities of growthfactors that aid the healing process 16-18. Of the numer-ous growth factors contained, particularly PDGF, FGF,VEGF and IGF-I are well-known to have positive effectson nerve regeneration 19. Hyaluronic acid (HA) is anoth-er popular agent that is used both in experimental andclinical studies due to its effects on preventing scar for-mation. HA is a single-chain, unbranched glucose-amino-glycan polymer found mostly in the extracellular matrixof the soft connective tissue and synovial fluid of thehumans. It is thought that topical application of HAmay prevent from epineural and extraneural scar forma-tion and facilitate nerve regeneration due to its effectson reducing the migration, proliferation and chemotaxisof lymphocytes as well as inhibiting effects on phagocy-tosis of granulocytes and macrophage motility 20,21.In the present study, we aimed to evaluate and comparethe effects of PRP that has high levels of growth factorsand HA that is known to have promoting effects onnerve regeneration by decreasing scar formation in a 1
Ann. Ital. Chir., 87, 4, 2016 363
Comparison of the effects of PRP and hyaluronic acid in promoting peripheral nerve regeneration
cm of rat sciatic nerve defect model using histopatho-logic and functional methods.
Materials and Methods
Twenty Wistar Albino male rats weighing from 200 to250 g were involved in the study. Eighteen were divid-ed into 3 groups with 6 rats randomly assigned to each.The remaining two rats were used as donor in order toharvest PRP and aorta graft. The left sciatic nerve waslesioned in all the groups and the right sciatic nerveremained intact and was used as the control. The ratswere housed 3 or 4 to a cage under standard laborato-ry conditions and carefully observed during the preop-erative and postoperative periods by expert veterinarians.The animals were fed regularly with food and water.
SURGICAL TECHNIQUE
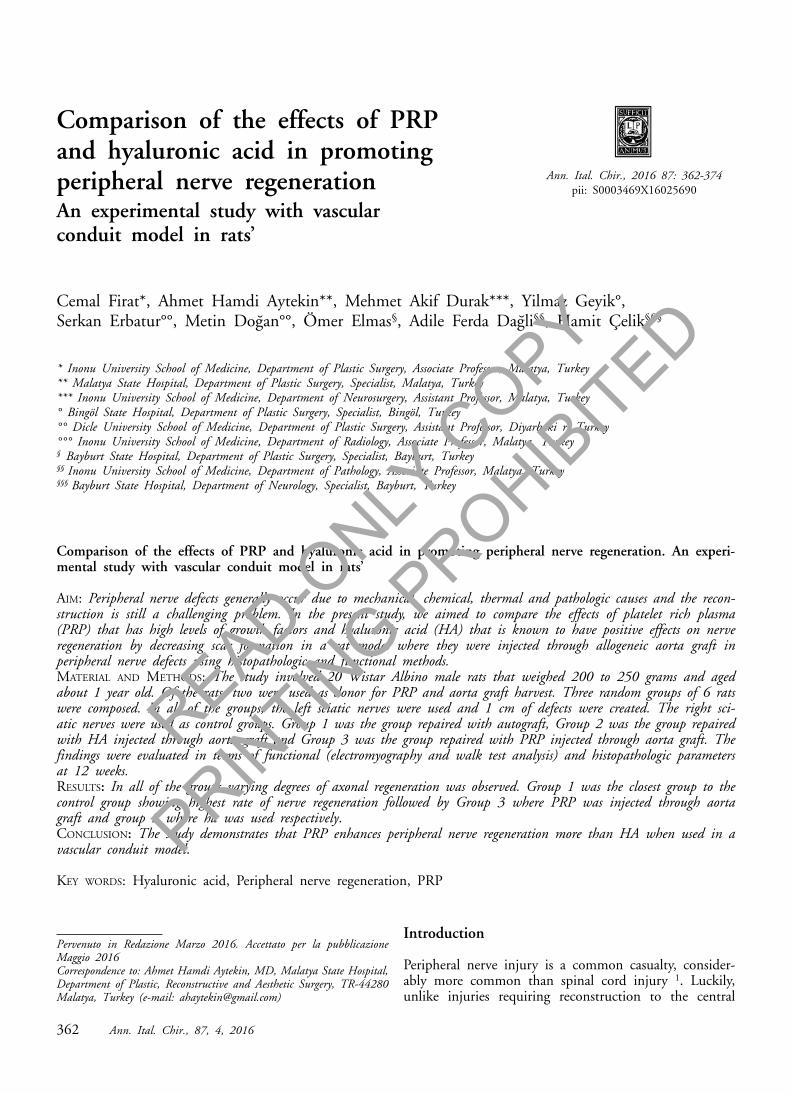
The rats were anesthetized with the combination of 10mg/kg Xylazine (Alfazine %2 20 mg/ml, Bayer) and 100mg/kg ketamine (Ketalar 50 mg/ml, Pfizer) intraperi-toneally. The required blood to prepare PRP was har-vested from the donor rats taking the blood of the entirebody through intracardiac way followed by harvestingaorta grafts. The left sides of the rats were shaven and cleaned withpovidone-iodine followed by an oblique gluteal incision.The gluteal fascia and muscular structures were passedand the sciatic nerve was exposed. The defect was cre-ated by resecting a nerve segment 10 mm in length prox-imal to the bifurcation of peroneal and tibial branches.In Group 1, the excised nerve segment was backapproached to the defect as an autograft using 10/0nylon sutures in an epineural way. Both in Group 2 andGroup 3, the defects were repaired using an allogeneicaorta conduit with 10/0 nylon sutures. In Group 2 0.3ml of HA and in Group 3, 0.3 ml of PRP was inject-ed through the aorta conduit (Figs. 1, 2).
Fig. 1: HA injection into allogeneic aorta graft.
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED
C. Firat, et al.
364 Ann. Ital. Chir., 87, 4, 2016
EVALUATION
In all of the groups, a walk test analysis was applied 12weeks after the left nerve surgery, followed by elec-tromyographic (EMG) analysis. All the rats were sacri-ficed and samples from the proximal anastomosis, graftand 10 mm distally to the distal anastomosis of the leftsciatic nerve were taken for histopathologic assessment.
WALK TEST ANALYSIS
Motor function was evaluated by analyzing free walkingpatterns. De Medinaceli was the first to describe thismethod 22,23. Walking test analyses were performed 12weeks after the left nerve surgery. The following para-meters were measured: print length (PL); the distancefrom the heel to the toe, toe spread (TS); the distancefrom the first to the fifth toes and intermediary toespread (ITS); the distance from the second to the fourthtoes. The sciatic functional index (SFI) was calculatedfor each animal using the formula proposed by Bain etal. 24,25. The SFI is a measure of dysfunction and isexpressed as a percentage. An SFI equal to -100% indi-cates that a complete sciatic nerve lesion is present,whereas SFI values from -10% to +10% reflect normalfunction 26.
SFI : [-38:3 x ( EPL – NPL) / NPL] + [109.5 x ( ETS– NTS) / NTS] + [13:3 x (EIT – NIT)/ NIT] - 8:8E = experimental, N = normal
ELECTROPHYSIOLOGICAL EVALUATION
In all of the groups, electrophysiological evaluation withclose needle technique was applied following walk testanalysis. Motor conduction from the sciatic nerve to the
gastrocnemius muscle was measured in all animals. Thelatency and amplitude values of the compound maximalaction potentials (CMAPs) of the gastrocnemius musclesboth in the lesioned and non-lesioned legs were record-ed followed by the calculation of lesioned/non-lesionedleg rates.
HISTOPATHOLOGIC EVALUATION
The tissue samples taken from the left sciatic nerves 12weeks after the surgical process were fixed in 10% forma-lin for 24 hours for histopathological examination. Afterfixation and routine histologic tissue preparation proce-dures, the nerve tissue specimens were embedded in paraf-fin blocks. Sections of 4 μm thicknesses were preparedusing a microtome and stained with phosphotungstic acidhematoxylin (PTAH), Giemsa and Mason’s trichrome.Images were captured using a Leica DFC 280 light micro-scope and analyzed using the Leica QWin Image AnalysisSystem (Leica Microsystems Imaging Solutions, Cambridge,UK). In the examination, myelination, edema, fibrosis andmast cell amounts were analyzed. The sections were scoredin terms of myelination (no myelinated axons, 0; raremyelinated axons, 1; scattered, irregular, and thin myeli-nated axons, 2; dense, regular, and thick myelinated axons,3), fibrosis (no fibrosis, 0; mild fibrosis, 1; moderate fibro-sis, 2; and severe fibrosis, 3), edema (no edema, 0; mildedema, 1; moderate edema, 2; and severe edema, 2), andmast cell density (no mast cells, 0; 1-2 mast cells, 1; 3-4mast cells, 2; 5 or more mast cells, 3; observed at 12.6magnification).
STATISTICAL METHODS
All the data obtained after the functional and histo-morphological evaluation of the groups were exported toSPSS for Windows v.10.0 (Statistical Package for theSocial Sciences) for statistical analysis. A general com-parison of the differences between groups was performedusing the Kruskal-Wallis test, a nonparametric test, andthe paired comparisons between groups were performedusing the Mann Whitney U test. In the analyses, P<0.05was accepted as statistically significant.
Results
WALK TEST ANALYSIS
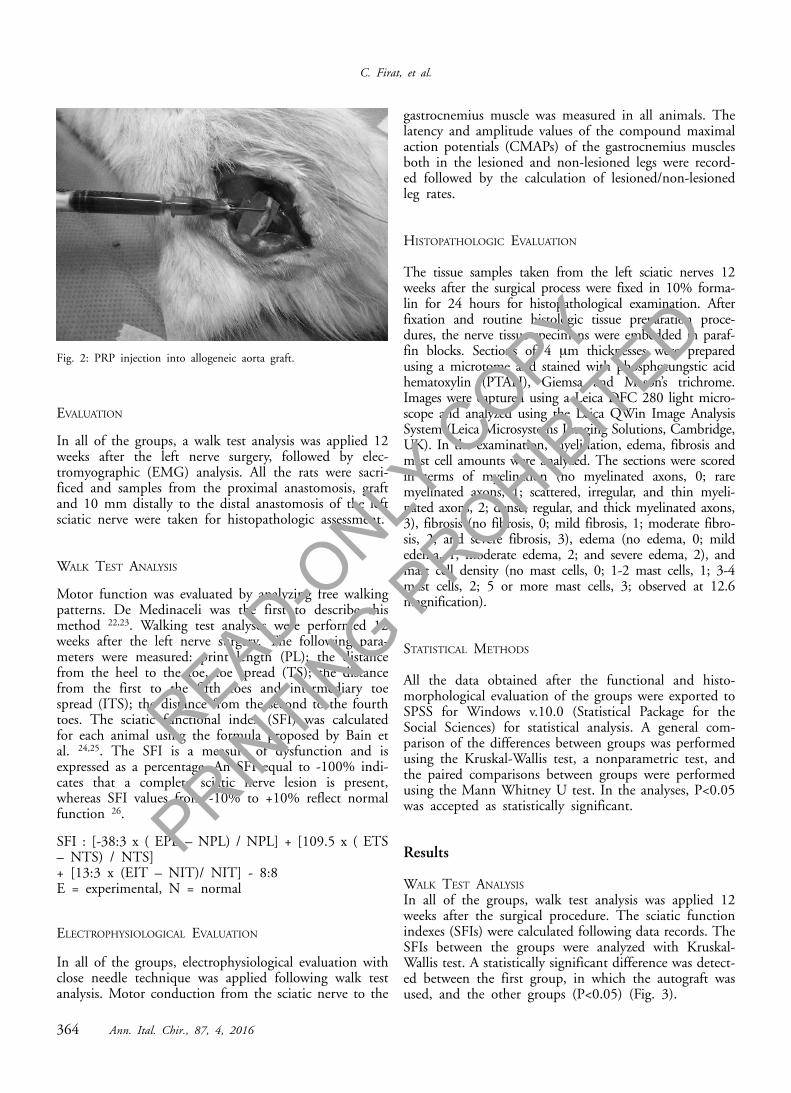
In all of the groups, walk test analysis was applied 12weeks after the surgical procedure. The sciatic functionindexes (SFIs) were calculated following data records. TheSFIs between the groups were analyzed with Kruskal-Wallis test. A statistically significant difference was detect-ed between the first group, in which the autograft wasused, and the other groups (P<0.05) (Fig. 3).
Fig. 2: PRP injection into allogeneic aorta graft.
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED
Ann. Ital. Chir., 87, 4, 2016 365
Comparison of the effects of PRP and hyaluronic acid in promoting peripheral nerve regeneration
ELECTROPHYSIOLOGICAL EVALUATION
The median latencies between the groups were analyzedwith Kruskal-Wallis test and a statistically significant dif-ference was detected (p<0.001). The other comparisons
were made with Mann Whitney U test (P<0.05). Group1 was the most similar to the control group and therewas a statistically significant difference between all of thegroups except Group 1-3.However, a statistically significant difference in Kruskal-Wallis test was detected in the comparison of medianamplitude values (p<0.001) and in Mann Whitney Utest, a statistically significant difference between all ofthe groups was detected (p=0.004) (Fig. 4).
SUBJECTIVE HISTOLOGICAL FINDINGS OF PROXIMAL ANASTOMOSIS
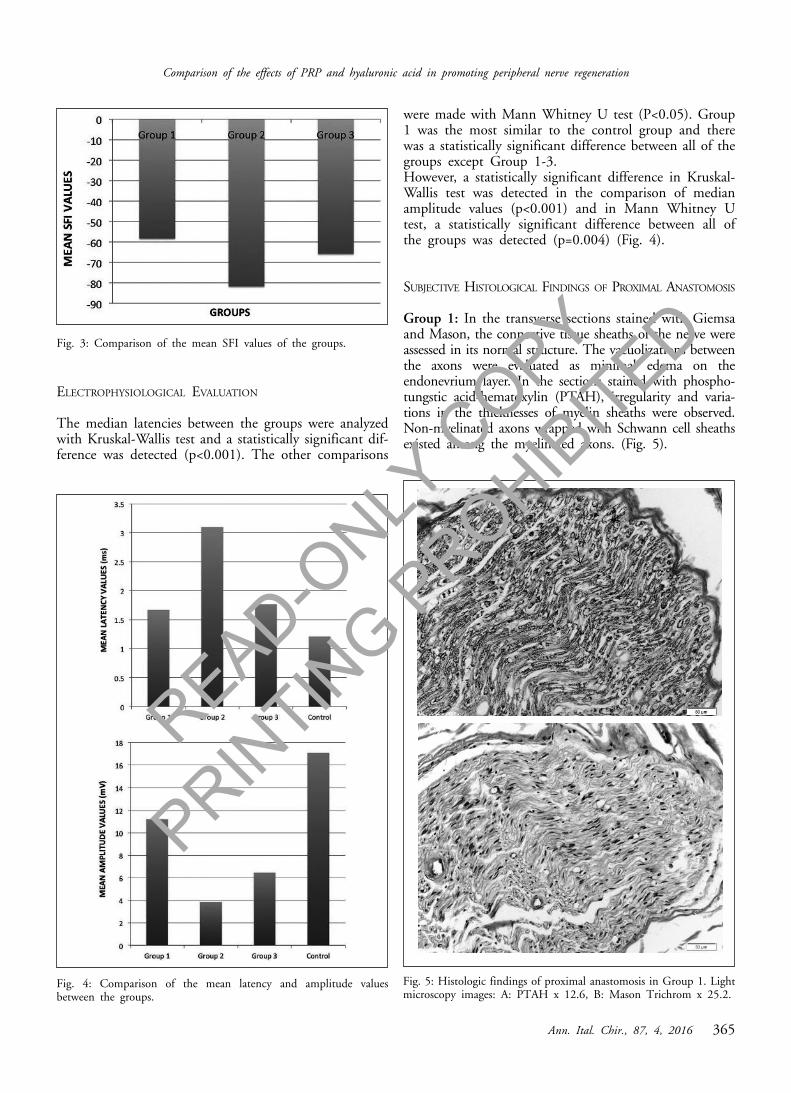
Group 1: In the transverse sections stained with Giemsaand Mason, the connective tissue sheaths of the nerve wereassessed in its normal structure. The vacuolizations betweenthe axons were evaluated as minimal edema on theendonevrium layer. In the sections stained with phospho-tungstic acid-hematoxylin (PTAH), irregularity and varia-tions in the thicknesses of myelin sheaths were observed.Non-myelinated axons wrapped with Schwann cell sheathsexisted among the myelinated axons. (Fig. 5).
Fig. 3: Comparison of the mean SFI values of the groups.
Fig. 4: Comparison of the mean latency and amplitude valuesbetween the groups.
Fig. 5: Histologic findings of proximal anastomosis in Group 1. Lightmicroscopy images: A: PTAH x 12.6, B: Mason Trichrom x 25.2.
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED
C. Firat, et al.
366 Ann. Ital. Chir., 87, 4, 2016
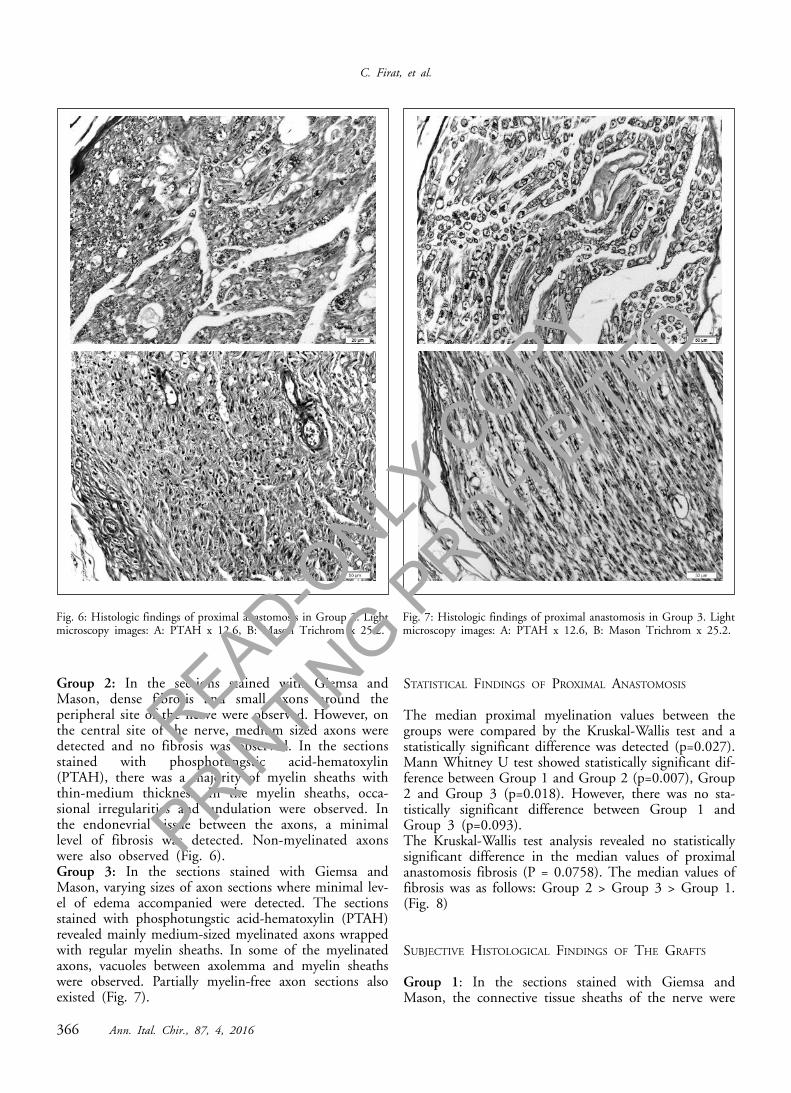
Group 2: In the sections stained with Giemsa andMason, dense fibrosis and small axons around theperipheral site of the nerve were observed. However, onthe central site of the nerve, medium sized axons weredetected and no fibrosis was observed. In the sectionsstained with phosphotungstic acid-hematoxylin(PTAH), there was a majority of myelin sheaths withthin-medium thickness. In the myelin sheaths, occa-sional irregularities and undulation were observed. Inthe endonevrial tissue between the axons, a minimallevel of fibrosis was detected. Non-myelinated axonswere also observed (Fig. 6). Group 3: In the sections stained with Giemsa andMason, varying sizes of axon sections where minimal lev-el of edema accompanied were detected. The sectionsstained with phosphotungstic acid-hematoxylin (PTAH)revealed mainly medium-sized myelinated axons wrappedwith regular myelin sheaths. In some of the myelinatedaxons, vacuoles between axolemma and myelin sheathswere observed. Partially myelin-free axon sections alsoexisted (Fig. 7).
STATISTICAL FINDINGS OF PROXIMAL ANASTOMOSIS
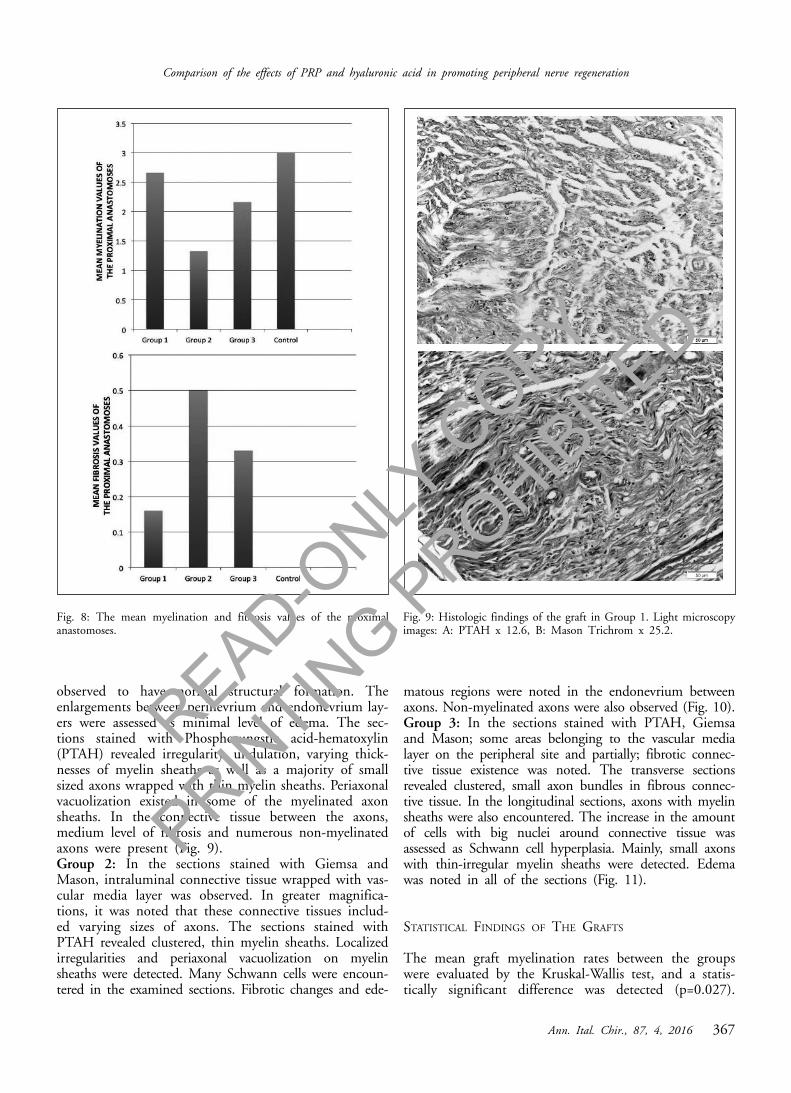
The median proximal myelination values between thegroups were compared by the Kruskal-Wallis test and astatistically significant difference was detected (p=0.027).Mann Whitney U test showed statistically significant dif-ference between Group 1 and Group 2 (p=0.007), Group2 and Group 3 (p=0.018). However, there was no sta-tistically significant difference between Group 1 andGroup 3 (p=0.093). The Kruskal-Wallis test analysis revealed no statisticallysignificant difference in the median values of proximalanastomosis fibrosis (P = 0.0758). The median values offibrosis was as follows: Group 2 > Group 3 > Group 1.(Fig. 8)
SUBJECTIVE HISTOLOGICAL FINDINGS OF THE GRAFTS
Group 1: In the sections stained with Giemsa andMason, the connective tissue sheaths of the nerve were
Fig. 6: Histologic findings of proximal anastomosis in Group 2. Lightmicroscopy images: A: PTAH x 12.6, B: Mason Trichrom x 25.2.
Fig. 7: Histologic findings of proximal anastomosis in Group 3. Lightmicroscopy images: A: PTAH x 12.6, B: Mason Trichrom x 25.2.
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED
Ann. Ital. Chir., 87, 4, 2016 367
Comparison of the effects of PRP and hyaluronic acid in promoting peripheral nerve regeneration
observed to have normal structural formation. Theenlargements between perinevrium and endonevrium lay-ers were assessed as minimal level of edema. The sec-tions stained with Phosphotungstic acid-hematoxylin(PTAH) revealed irregularity, undulation, varying thick-nesses of myelin sheaths as well as a majority of smallsized axons wrapped with thin myelin sheaths. Periaxonalvacuolization existed in some of the myelinated axonsheaths. In the connective tissue between the axons,medium level of fibrosis and numerous non-myelinatedaxons were present (Fig. 9).Group 2: In the sections stained with Giemsa andMason, intraluminal connective tissue wrapped with vas-cular media layer was observed. In greater magnifica-tions, it was noted that these connective tissues includ-ed varying sizes of axons. The sections stained withPTAH revealed clustered, thin myelin sheaths. Localizedirregularities and periaxonal vacuolization on myelinsheaths were detected. Many Schwann cells were encoun-tered in the examined sections. Fibrotic changes and ede-
matous regions were noted in the endonevrium betweenaxons. Non-myelinated axons were also observed (Fig. 10).Group 3: In the sections stained with PTAH, Giemsaand Mason; some areas belonging to the vascular medialayer on the peripheral site and partially; fibrotic connec-tive tissue existence was noted. The transverse sectionsrevealed clustered, small axon bundles in fibrous connec-tive tissue. In the longitudinal sections, axons with myelinsheaths were also encountered. The increase in the amountof cells with big nuclei around connective tissue wasassessed as Schwann cell hyperplasia. Mainly, small axonswith thin-irregular myelin sheaths were detected. Edemawas noted in all of the sections (Fig. 11).
STATISTICAL FINDINGS OF THE GRAFTS
The mean graft myelination rates between the groupswere evaluated by the Kruskal-Wallis test, and a statis-tically significant difference was detected (p=0.027).
Fig. 8: The mean myelination and fibrosis values of the proximalanastomoses.
Fig. 9: Histologic findings of the graft in Group 1. Light microscopyimages: A: PTAH x 12.6, B: Mason Trichrom x 25.2.
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED
C. Firat, et al.
368 Ann. Ital. Chir., 87, 4, 2016
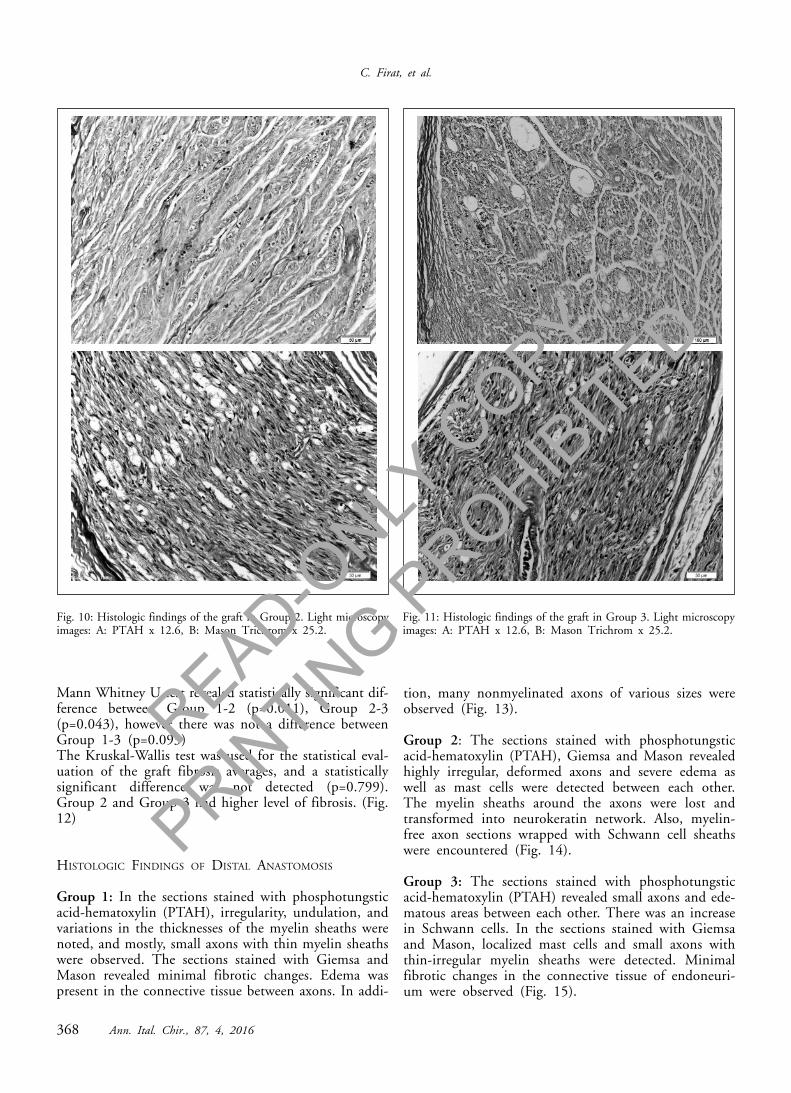
Mann Whitney U test revealed statistically significant dif-ference between Group 1-2 (p=0.011), Group 2-3(p=0.043), however there was not a difference betweenGroup 1-3 (p=0.093) The Kruskal-Wallis test was used for the statistical eval-uation of the graft fibrosis averages, and a statisticallysignificant difference was not detected (p=0.799).Group 2 and Group 3 had higher level of fibrosis. (Fig.12)
HISTOLOGIC FINDINGS OF DISTAL ANASTOMOSIS
Group 1: In the sections stained with phosphotungsticacid-hematoxylin (PTAH), irregularity, undulation, andvariations in the thicknesses of the myelin sheaths werenoted, and mostly, small axons with thin myelin sheathswere observed. The sections stained with Giemsa andMason revealed minimal fibrotic changes. Edema waspresent in the connective tissue between axons. In addi-
tion, many nonmyelinated axons of various sizes wereobserved (Fig. 13).
Group 2: The sections stained with phosphotungsticacid-hematoxylin (PTAH), Giemsa and Mason revealedhighly irregular, deformed axons and severe edema aswell as mast cells were detected between each other.The myelin sheaths around the axons were lost andtransformed into neurokeratin network. Also, myelin-free axon sections wrapped with Schwann cell sheathswere encountered (Fig. 14).
Group 3: The sections stained with phosphotungsticacid-hematoxylin (PTAH) revealed small axons and ede-matous areas between each other. There was an increasein Schwann cells. In the sections stained with Giemsaand Mason, localized mast cells and small axons withthin-irregular myelin sheaths were detected. Minimalfibrotic changes in the connective tissue of endoneuri-um were observed (Fig. 15).
Fig. 10: Histologic findings of the graft in Group 2. Light microscopyimages: A: PTAH x 12.6, B: Mason Trichrom x 25.2.
Fig. 11: Histologic findings of the graft in Group 3. Light microscopyimages: A: PTAH x 12.6, B: Mason Trichrom x 25.2.
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED

Ann. Ital. Chir., 87, 4, 2016 369
Comparison of the effects of PRP and hyaluronic acid in promoting peripheral nerve regeneration
STATISTICAL FINDINGS OF DISTAL ANASTOMOSIS
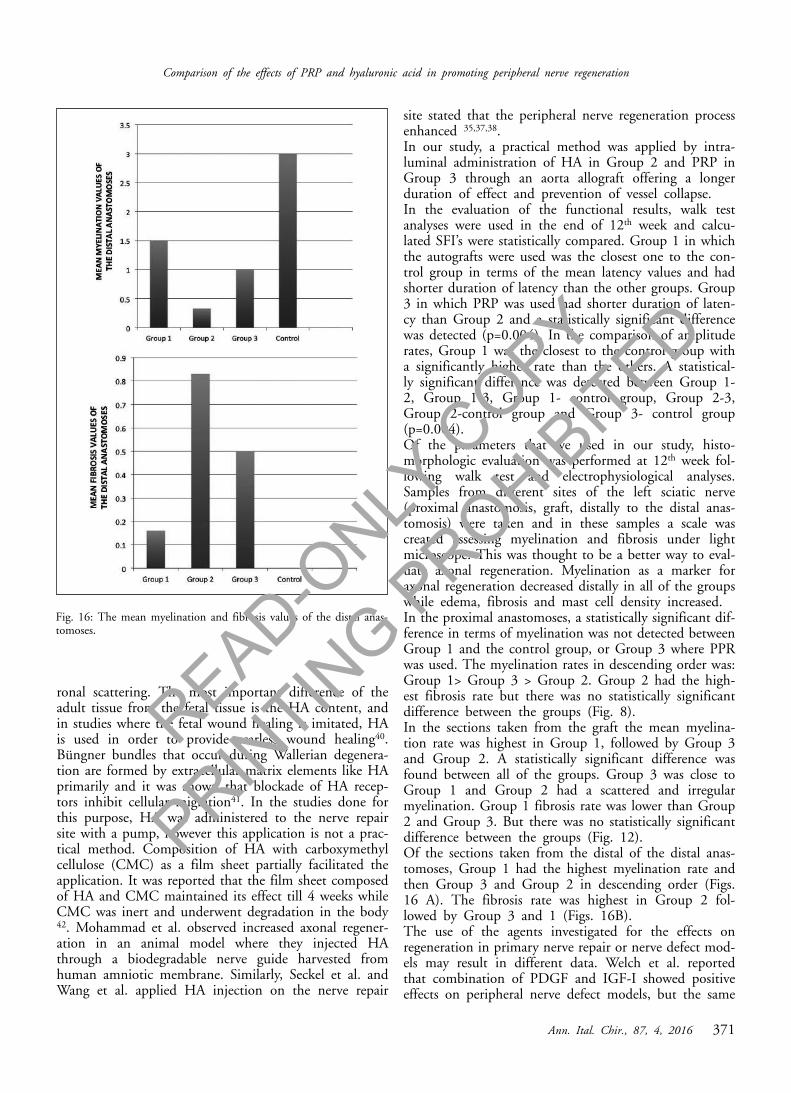
The Kruskal-Wallis test revealed a statistically significantdifference in mean distal anastomosis myelination ratesbetween the groups (p=0.105). The order of the meanmyelination rates was as follows: Group 1 > Group 3 >Group 2. Similarly, the mean distal anastomosis fibrosisrates were evaluated with the Kruskal-Wallis test and astatistically significant difference was detected (p=0.041).The order of the mean fibrosis rates was as follows:Group 2 > Group 3 > Group 1. However, MannWhitney U test showed no statistically significant dif-ference between the groups (Fig. 16).
Discussion
The treatment of the peripheral nerve injuries has stillbeen a challenging problem and there is not a certaincompromise for the treatment protocol and outcomes.
The gold standard for treating large peripheral nervedefects is reconstruction with autologous nerve grafts27,28. However, the extent of the injury may be a limit-ing factor for autografts. During repair, altered fascicu-lar architecture in the graft may hinder nerve regenera-tion due to the scattering of axons 29. Graft donor-sitemorbidity is another limitation, since serious problemsmay occur such as loss of sensation and donor-site nervefunction, as well as painful neuroma 27,28. Therefore, inconsideration of these disadvantages, many studies havebeen conducted in search of alternatives against autolo-gous nerve grafts that offer easier methods with betterfunctional outcomes and less morbidity in peripheralnerve defect repairs.Vein tracts are frequently used as conduits for peripher-al nerve defect repair, offering less donor site morbidityand harvesting without the need of a secondary incision.However, limitation of nerve regeneration due to the col-lapse of the vein grafts is still a problem that could notbe overcome. In order to prevent vein graft collapse,
Fig. 12 A,B: The mean myelination and fibrosis values of the grafts. Fig. 13: Histologic findings of the distal anastomosis in Group 1. Lightmicroscopy images: A: PTAH x 12.6, B: Mason Trichrom x 25.2.
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED

C. Firat, et al.
370 Ann. Ital. Chir., 87, 4, 2016
metal spiral supports and nerve grafts placed into thevein grafts were studied 29-31. Therefore, we used aortaallograft to obtain least collapse by intraluminal injec-tion of HA and PRP in our study.PRP is a fraction of autologous plasma that containshigher rates of platelet than in the normal blood. As aconcentrated source of autologous platelets, PRP con-tains all of the coagulation factors and many growth fac-tors as well as other cytokines that stimulate wound heal-ing. Of the main growth factors it primarily includesPDGF, TGF-beta, VEGF, EGF and IGF. The effect ofthe PRP occurs due to the synergistic impact of thesegrowth factors 32-36. PRP preserves its bioactive proper-ty duration for a long time due to fibrin clotting by theactivation of platelets through thrombin on the appliedregion. Aspenberg et al. reported that PRP continued toeffect on the Achilles tendon of the rats for 4 weeks fol-lowing a single dose application 33. The studies revealedthat the scarring around the nerve just affected, the early
term of the healing and the actual part of the regener-ation realized before the developed scar tissue. In thestudies where the effects of PRP on wound healing wereinvestigated, it was prompted that PRP caused extracel-lular matrix collection and increased connective tissueproliferation particularly due to TGF-beta and PDGF 15.In contrast, Anitua et al. observed that PRP applied onthe titanium implants decreased inflammation 37. Hyaluronic acid (HA) is another popular agent that isused both in experimental and clinical studies due to itseffects on preventing scar formation. HA is a single-chain, unbranched glucose-amino-glycan polymer foundmostly in the extracellular matrix of the soft connectivetissue and synovial fluid of the humans 20,21.HA exists almost in all of the extracellular spaces andholds important roles in the maintenance of hydrody-namic property of the extracellular matrix 38,39. It hasvarious structural functions in nerve cell as well as manycellular interactions such as migration, adhesion, neu-
Fig. 14: Histologic findings of the distal anastomosis in Group 2. Lightmicroscopy images: A: PTAH x 12.6, B: Mason Trichrom x 25.2.
Fig. 15: Histologic findings of the distal anastomosis in Group 3. Lightmicroscopy images: A: PTAH x 12.6, B: Mason Trichrom x 25.2.
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED
Ann. Ital. Chir., 87, 4, 2016 371
Comparison of the effects of PRP and hyaluronic acid in promoting peripheral nerve regeneration
ronal scattering. The most important difference of theadult tissue from the fetal tissue is the HA content, andin studies where the fetal wound healing is imitated, HAis used in order to provide scarless wound healing40.Büngner bundles that occur during Wallerian degenera-tion are formed by extracellular matrix elements like HAprimarily and it was shown that blockade of HA recep-tors inhibit cellular migration41. In the studies done forthis purpose, HA was administered to the nerve repairsite with a pump, however this application is not a prac-tical method. Composition of HA with carboxymethylcellulose (CMC) as a film sheet partially facilitated theapplication. It was reported that the film sheet composedof HA and CMC maintained its effect till 4 weeks whileCMC was inert and underwent degradation in the body42. Mohammad et al. observed increased axonal regener-ation in an animal model where they injected HAthrough a biodegradable nerve guide harvested fromhuman amniotic membrane. Similarly, Seckel et al. andWang et al. applied HA injection on the nerve repair
site stated that the peripheral nerve regeneration processenhanced 35,37,38. In our study, a practical method was applied by intra-luminal administration of HA in Group 2 and PRP inGroup 3 through an aorta allograft offering a longerduration of effect and prevention of vessel collapse. In the evaluation of the functional results, walk testanalyses were used in the end of 12th week and calcu-lated SFI’s were statistically compared. Group 1 in whichthe autografts were used was the closest one to the con-trol group in terms of the mean latency values and hadshorter duration of latency than the other groups. Group3 in which PRP was used had shorter duration of laten-cy than Group 2 and a statistically significant differencewas detected (p=0.004). In the comparison of amplituderates, Group 1 was the closest to the control group witha significantly higher rate than the others. A statistical-ly significant difference was detected between Group 1-2, Group 1-3, Group 1- control group, Group 2-3,Group 2-control group and Group 3- control group(p=0.004).Of the parameters that we used in our study, histo-morphologic evaluation was performed at 12th week fol-lowing walk test and electrophysiological analyses.Samples from different sites of the left sciatic nerve(proximal anastomosis, graft, distally to the distal anas-tomosis) were taken and in these samples a scale wascreated assessing myelination and fibrosis under lightmicroscope. This was thought to be a better way to eval-uate axonal regeneration. Myelination as a marker foraxonal regeneration decreased distally in all of the groupswhile edema, fibrosis and mast cell density increased.In the proximal anastomoses, a statistically significant dif-ference in terms of myelination was not detected betweenGroup 1 and the control group, or Group 3 where PPRwas used. The myelination rates in descending order was:Group 1> Group 3 > Group 2. Group 2 had the high-est fibrosis rate but there was no statistically significantdifference between the groups (Fig. 8). In the sections taken from the graft the mean myelina-tion rate was highest in Group 1, followed by Group 3and Group 2. A statistically significant difference wasfound between all of the groups. Group 3 was close toGroup 1 and Group 2 had a scattered and irregularmyelination. Group 1 fibrosis rate was lower than Group2 and Group 3. But there was no statistically significantdifference between the groups (Fig. 12).Of the sections taken from the distal of the distal anas-tomoses, Group 1 had the highest myelination rate andthen Group 3 and Group 2 in descending order (Figs.16 A). The fibrosis rate was highest in Group 2 fol-lowed by Group 3 and 1 (Figs. 16B). The use of the agents investigated for the effects onregeneration in primary nerve repair or nerve defect mod-els may result in different data. Welch et al. reportedthat combination of PDGF and IGF-I showed positiveeffects on peripheral nerve defect models, but the same
Fig. 16: The mean myelination and fibrosis values of the distal anas-tomoses.
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED

agents did not show the similar effects on primary nerverepair model19. The same authors concluded that in casethe nerve edges came end-to-end tightly without gap for-mation, mechanical factors would act and this effectwould be more dominant than the trophic effect thatwould develop due to the tested factors. Although Welchet al. declared that primary nerve repair model was nota proper model in search for the effects of trophic fac-tors on regeneration, in numerous studies where thismodel was used it could be possibly seen that trophicfactors had positive effects 12, 14, 45, 46. In the previous studies, it was strongly recommendedthat a six-week period for epineural scarring formationwas sufficient while a twelve-week healing period wasrequired for the evaluation of functional recovery 47.Therefore, end of the 12nd week when the functionalrecovery is complete was waited for evaluation. In thecurrent literature allogeneic vessel grafts, muscle, carti-lage, polyglycolic acid (PGA) and silicone tubes wereused successfully as alternative to the gold standard treat-ment of autograft use 12. The rate of myelination in the PRP group gave betterresults than the HA group in all sections. Although therewas not statistically significant difference in terms offibrosis rates between the groups, the rate of fibrosis inthe PRP group was lower compared to the HA group. In our this study we compared the effects of PRP andHA on nerve regeneration, by intraluminal injectionthrough aorta conduit in terms of functional and histo-morphologic parameters. In the study revealed varyingdegrees of nerve regeneration in all of the groups, how-ever PRP showed higher rate of axonal regeneration thanHA. In conclusion, this study demonstrates that PRPenhances peripheral nerve regeneration more than HAwhen used in a vascular conduit model. We believe thatthese findings will enlighten further studies on the alter-native treatment of nerve injuries.
Riassunto
SCOPO: Le interruzioni dei nervi periferici sono in gene-re provocate da cause meccaniche, chimiche, termiche opatologiche e la loro ricostruzione rappresenta tutt’orauna sfida. Con questo studio ci siamo proposti di met-tere a confronto in un modello murino, con controlliistopatologici e funzionali, gli effetti di un plasma arric-chito di piastrine (PRP), dotato di una elevata presenzadi fattori della crescita, e l’acido ialuronico (HA), notoper esercitare effetti positivi sulla rigenerazione nervosamediante la diminuzione di formazione del tessuto cica-triziale, dopo somministrazione iniettiva mediante uninnesto allogenico di aorta nei difetti di nervi periferici.MATERIAL E METODI. Per lo studio sono stati utilizzati20 ratti albini Wistar, di sesso maschile e del peso varia-bile tra 200 e 250 grammi e dell’età di circa 1 anno.Due di questi ratti sono stati usati come donatori di
C. Firat, et al.
372 Ann. Ital. Chir., 87, 4, 2016
PRP e per la raccolta del tratto di aorta a destinare cometutore.I restanti sono stati divisi in tre gruppi a random di 6ratti, ed in tutti è stato creato un difetto delle dimen-sioni di 1 cm del nervo sciatico di sinistra. I nervi scia-tici di destra sono stati usati come controllo.Lo sciatico sinistro del Gruppo 1 è stato riparato conautoinnesto; nel Gruppo 2 è stato riparato con l’iniezionedi HA attraverso il tutore aortico; nel Gruppo 3 è sta-to riparato con PRP e sempre mediante il tutore aorti-co.I risultati sono stati valutati in termini di funzionalità(analisi elettromiografica e test di locomozione), e conparametric istopatologici a 12 settimane. Come risultato in tutti i gruppi è stato osservato unvario grado di rigenerazione assonale. Il Gruppo 1 si èdimostrato il più vicino al controllo perché ha dimo-strato il più elevato livello di rugenerazione nervosa,seguito dal Gruppo 3 trattato con iniezione di PRP attra-verso il tutore aortico, e dal Gruppo 2 in cui era statoiniettato HA.Il conclusione lo studio ha dimostrato che il PRP esal-ta la rigenerazione nervosa maggiormente rispetto all’HAin un modello con tutore vascolare.
References
1. Evans GR: Peripheral nerve injury: a review and approach to tis-sue engineered constructs. Anat Rec, 2001; 263(4):396-404.
2. Firat C, Geyik Y, Aytekin AH, Gul M, Kamisli S, Yigitcan B,Ozcan C: Comparison of Nerve, Vessel, and Cartilage Grafts inPromoting Peripheral Nerve Regeneration. Ann Plast Surg, 2014;73(1):54-61.
3. Iemionow M, Uygur S, Ozturk C, Siemionow K: Techniquesand materials for enhancement of peripheral nerve regeneration: A lit-erature review. Microsurgery, 2013; 33(4):318-28.
4. Siemionow M, Sonmez E: Nerve allograft transplantation: Areview. J Reconstr Microsurg, 2007; 23(8):511-20.
5. Tang P, Kilic A, Konopka G, Regalbuto R, Akelina Y, GardnerT: Histologic and functional outcomes of nerve defects treated withacellular allograft versus cabled autograft in a rat model. Microsurgery,2013 (6);33:460-67.
6. Colen KL, Choi M, Chiu DTW: Nerve Grafts and Conduits.Plast Reconstr Surg, 2009; 124(6 Suppl.): 386e,394e.
7. Chiu DT, Strauch B: A prospective clinical evaluation of auto-genousvein grafts used as a nerve conduit for distal sensory nerve defectsof 3 cm or less. Plast Reconstr Surg, 1990; 86(5):928-34.
8. Battiston B, Geuna S, Ferrero M, Tos P: Nerve repair by meansof tubulization: Literature review and personal clinical experience com-paring biological and synthetic conduits for sensory nerve repair.Microsurgery, 2005; 25(4):258-67.
9. Frostick SP, Yin Q. Kemp GJ: Schwann cells, neurotrophic fac-tors, and peripheral nerve regeneration. Microsurgery, 1998;18(7):397-405.
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED

Ann. Ital. Chir., 87, 4, 2016 373
Comparison of the effects of PRP and hyaluronic acid in promoting peripheral nerve regeneration
10. Ilbay K, Etus V, Yildiz K, Ilbay G, Ceylan S: Topical applica-tion of mitomycin C prevents epineural scar formation in rats.Neurosurg Rev 2005; 28(2):148-53.
11. Gorgulu A, Imer M, Simsek O, Sencer A, Kutlu K, Cobanoglu:The effect of aprotinin on extraneural scarring in peripheral nervesurgery, an experimental study. Acta Neurochi, 1998; 140(12):1303-307.
12. Voinesco F, Glauser L, Kraftsik R, Barakat-Walter I: Localadministration of thyroid hormones in silicone chamber increases regen-eration of rat transected sciatic nerve. Exp Neurol, 1998; 150(1): 69-81.
13. Ozgenel GY, Filiz G: Combined application of human amnioticmembrane wrapping and hyaluronic acid injection in epineurectomizedrat sciatic nerve. J Reconstr Microsurg, 2004; 20(2): 153-57.
14. Ozgenel GY: Effects of hyaluronic acid on peripheral nerve scar-ring and regeneration in rats. Microsurgery, 2003; 23(6):575-81.
15. Sariguney Y, Yavuzer R, Elmas C, Yenicesu I, Bolay H, AtabayK: Effect of platelet-rich plasma on peripheral nerve regeneration. JReconstr Microsurg, 2008; 24(3):159-67.
16. Yu W, Wang J, Yin J: Platelet-rich plasma: a promising productfor treatment of peripheral nerve regeneration after nerve injury. IntJ Neurosci, 2011; 121(4):176-80.
17. Elgazzar RF, Mutabagani MA, Abdelaal SE, Sadakah AA: Plateletrich plasma may enhance peripheral nerve regeneration after cyano-acrylate reanastomosis: a controlled blind study on rats. Int J OralMaxillofac Surg, 2008; 37(8):748-55.
18. Farrag TY, Lehar M, Verhaegen P, Carson KA, Byrne PJ: Effectof platelet rich plasma and fibrin sealant on facial nerve regenerationin a rat model. Laryngoscope, 2007; 117(1):157-65.
19. Welch JA, Kraus KH, Wells MR, Blunt DG, Weremowitz J:Effect of combined administration of insulin-like growth factor andplatelet-derived growth factor on the regeneration of transected andanastomosed sciatic nerve in rats. Am J Vet Res, 1997; 58(9):1033-37.
20. Burd DA, Greco RM, Regauer S, Longaker MT, Siebert JW,Garg HG: Hyaluronan and wound healing: A new perspective. Br JPlast Surg, 1991; 44(8):579-84.
21. Bora FW Jr, Bednar JM, Osterman AL, Brown MJ, SumnerAJ: Prosthetic nerve grafts: A resorbable tube as an alternative to auto-genous nerve grafting. J Hand Surg Am, 1987; 12(5 Pt 1):685-92.
22. Yüce S, Cemal Gökçe E, I kdemir A, Koç ER, Cemil DB,Gökçe A, Sargon MF: An Experimental Comparison of the Effects ofPropolis, Curcumin, and Methylprednisolone on Crush Injuries of theSciatic Nerve. Ann Plast Surg, 2015; 74(6):684-92
23. De Medinaceli L: Use of sciatic function index and walking trackassessment. Microsurgery, 1990; 11(2):191-92.
24. Pavic, R, Pavic ML, Tot OK, et al.: Side distinct sciatic nerverecovery differences between rats and mice. Somatosens Mot Res. 2008;25(3):163-70.
25. Bain JR, Mackinnon SE, Hunter DA: Functional evaluation ofcomplete sciatic peroneal and posterior tibial nerve lesions in the rat.Plast Reconstr Surg, 1989; 83(1):129-38.
26. Hare GM, Evans PJ, Mackinnon SE, et al.: Walking track analy-sis: A long-term assessment of peripheral nerve recovery. Plast ReconstrSurg, 1992; 89(2):251-58.
27. Lohmeyer JA, Mailander P: Nerve reconstruction by means oftubulization. In: Eisenmann-Klein M, Neuhann-Lorenz C(eds):Innovations in Plastic and Aesthetic Surgery. Berlin, Germany:Springer-Verlag; 2008:78-81.
28. Ghaznavi AM, Kokai LE, Lovett ML, et al.: Silk fibroin conduitsa cellular and functional assessment of peripheral nerve repair. AnnPlast Surg, 2011; 66(3): 273-79.
29. Strauch B, Ferder M, Lovelle-Allen S, Moore K, Kim DJ, LlenaJ: Determining the maximal length of a vein conduit used as an inter-position graft for nerve regeneration. J Reconstr Microsurg, 1996;12(8):521-27.
30. Walton RL, Brown RE, Matory WE Jr: Autogenous vein graftrepair of digital nerve defects in the finger: A retrospective clinicalstudy. Plast Reconstr Surg, 1989; 84(6):944-49.
31. Fawcett JW, Keynes R: Muscle basal lamina: A new graft mate-rial for peripheral nerve repair. J Neurosurg 1986; 65(3):354-63.
33. Aspenberg P,Virchenko O: Platelet concentrate injection improvesAchilles tendon repair in rats. Acta Orthop Scand, 2004; 75(1): 93-99.
34. Haynesworth S: Platelet-rich plasma stimulates stem cell chemo-taxis, proliferation and potentiates osteogenic differentiation. The SpineJournal, 2006; 2(5):68-72.
35. Marx RE: Platelet-rich plasma: Evidence to support its use. J OralMaxillofac Surg, 2004; 62(4):489-96.
36. DelRossi AJ, Cernaianu AC, Vertrees RA, Wacker CJ, FullerSJ, Cilley JH, Baldino WA: Platelet-rich plasma reduces postoperativeblood loss after cardiopulmonary bypass. J Thorac and CardiovascSurg, 1990; 100(2): 281-286
37. Anitua E, Andia I, Ardanza B. Nurden P, Nurden AT:Autologous platelets as a source of proteins for healing and tissue regen-eration. Thromb Haemos, 2004; 91(1):4-15.
38. Collier JH, Camp J.P., Hudson TW, Schmidt CE: Synthesisand characterization of polypyrrole-hyaluronic acid and composite bio-materials for tissue engineering applications. J Biomed Mater Res,2000; 50(4):574-84.
39. Gong H, Ye W, Freddo TF, Hernandez MR: Hyaluronic acidin the normal and glaucomatous optic nerve. Exp Eye Res, 1997(4);64:587-95.
40. Eggli PS, Lucocq J, Ott,P, Graber W, Van der Zypen E:Ultrastructural localization of hyaluronan in myelin sheaths of the ratcentral and rat and human peripheral nervous systems using hyaluro-nan-binding proteingold and link protein-gold. Neuroscience, 1992;48(3):737-44.
41. Mohammad J, Warnke PH, Pan YC, Shenaq S: Increased axon-al regeneration through a biodegradable amnionic tube nerve conduit:Effect of local delivery and incorporation of nerve growth fac-tor/hyaluronic acid media. Ann Plast Surg, 2000; 44(1):59-64.
42. Hookern GD, Taylor BM, Driman DK: Prevention of adhesionformation with use of sodium hyaluronate-based bioresorbable mem-brane in a rat model of ventral hernia repair with polypropylene mesh.A randomized, controlled study. Surgery, 1999; 125(2): 211-16.
43. Wang KK, Nemeth IR, Seckel BR. Chakalis-Haley DP, SwannDA, Kuo JW, Bryan D, Cetrulo CL Jr: Hyaluronic acid enhancesperipheral nerve regeneration in vivo. Microsurgery, 1998; 18(4): 270-275.
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED
C. Firat, et al.
374 Ann. Ital. Chir., 87, 4, 2016
44. Yoshii S, Oka M, Shima M, Taniguchi A, Akagi M.: 30 mmregeneration of rat sciatic nerve along collagen filaments. Brain Res,2002; 949(1-2):202-08.
45. Badylak SF, Record R, Lindberg K, Hodde J, Park K: Smallintestinal submucosa: A substrate for in vitro cell growth. J BiomaterSci Polym Ed, 1998; 9(8):863-78.
46. Corral CJ, Siddiqui A, Wu L, Farrell CL, Lyons D, MustoeTa: Vascular endothelial growth factor is more important than basicfibroblastic growth factor during ischemic wound healing. Arch Surg,1999; 134(2):200-05.
47. Cordeiro PG, Seckel BR, Lipton SA, D’Amore PA, Wagner J,Madison R: Acidic fibroblast growth factor enhances peripheral nerveregeneration in vivo. Plast Reconstr Surg, 1989; 83(6):1013-19.
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED