Embed Size (px)
Citation preview

香港中文大學The Chinese University of Hong Kong
Continuous Cuffless Blood Pressure Estimation with Respiratory-modulated Pulse Transit Time
and Photoplethysmogram Intensity Ratio
Xiaorong DING
Supervisor: Prof. Hon Ki Tsang
Co-supervisor: Prof. Yuan-Ting Zhang
Department of Electronic Engineering
June 24, 2016
PhD Oral Defense

Outline
Introduction
Effect of Cardiovascular Disease and Calibration
Interval on Blood Pressure Estimation
Pulse Transit Time for Respiratory Rate Estimation
Cuffless BP Estimation with Pulse Transit Time and
Photoplethysmogram Intensity Ratio
Conclusions and Suggestions for Future Work

1
1
1
1
Background
BP Measurement Techniques
PTT Method for Cuffless BP
Research Problems
Study Objectives
1Introduction
Effect of Cardiovascular Disease and Calibration
Interval on Blood Pressure Estimation
Pulse Transit Time for Respiratory Rate
Estimation
BP Estimation with Pulse Transit Time and
Photoplethysmogram Intensity Ratio
Conclusions and Suggestions for Future Work

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•Cardiovascular diseases (CVDs) - No. 1 Killer
Background
CVDs
Global Atlas on Cardiovascular Disease Prevention and Control. WHO (2011).
4/50

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
Hypertension
Chow, et al. JAMA (2013).
•Blood pressure (BP) variability and continuous BP
- Early detection and prevention of hypertension
•Accurate measurement of BP
- Diagnose, evaluate, management
47% 33%40%
5/50
Hypertension

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
BP Measurement Techniques
Ding, Liu, et al., IEEE Life Sciences Newsletter (2014).
Noninvasive
Invasive
Intrusive Unobtrusive
Intra-arterial
Auscultatory
Oscillometric
TomometryVolume clamp
Cuffless BP monitor
6/50
Intermittent
Continuous Beat-to-beat/continuous
Implantable

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•Pulse transit time (PTT)
•Pulse wave velocity (PWV) recording- Moens-Korteweg (M-K) equation:
Principle of PTT-based BP Measurement
𝐏 =1
γlnρL2
E0+ lnd − lnh − 2ln𝐏𝐓𝐓
L: pulse travelling distanceE: elastic modulush: blood vessel thicknessd: arterial diameter𝝆: blood densityγ: relevant to measurement siteE0: zero-pressure modulusP: blood pressure
Electrocardiogram (ECG)
Photoplethysmogram (PPG)
R Wave
PTT
𝐏𝐖𝐕 =𝐄𝐡
𝛒𝐝
𝐄 = 𝐄𝟎𝐞𝛄𝐏
Moens, A. and Korteweg, D. J., et al, (1878). Hughes et al. (1979). Bramwell JC, and Hill AV, (1922).
L
𝐏𝐖𝐕 =𝐋
𝐏𝐓𝐓
7/50
𝐏𝐖𝐕 =𝐕
𝛒∆ 𝐕 ∆𝐏B-H equation:

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
Author Method (Model)
Calibration &
Reference
Method
Subjects SBP DBP
Error (mmHg) Correlation Error (mmHg) Correlation
Young et
al (1995)
SBP=a1/PTT+b1
DBP=a2/PTT+b2
Oscillometric
BP35 patients
-0.37 (-
29.0~28.2)
-0.01 (-
14.9~14.8)
Chen
et al
(2000)
𝐒𝐁𝐏 = 𝐒𝐁𝐏𝟎 −𝟐
𝛄𝐏𝐓𝐓𝟎𝐏𝐓𝐓 − 𝐏𝐓𝐓𝟎
Intermittent
BP from
Invasive BP (5
min)
20 patientsRMSE:
3.70 ± 1.850.97±0.02
Poon
et al
(2005)
𝐃𝐁𝐏 = 𝐌𝐁𝐏𝟎 +𝟐
𝛄𝐥𝐧𝐏𝐓𝐓𝟎
𝐏𝐓𝐓−𝟏
𝟑𝐏𝐏𝟎 ∙
𝐏𝐓𝐓𝟎
𝐏𝐓𝐓
𝟐
𝐒𝐁𝐏 = 𝐃𝐁𝐏 + 𝐏𝐏𝟎 ∙𝐏𝐓𝐓𝟎
𝐏𝐓𝐓
𝟐
Cuff BP
(Initial
calibration)
85 (39
hypertensive
s)
Mean±SD:
0.6±9.8
Mean±SD:
0.9±5.6
Douniama
et al
(2009)
SBP=a1*PTT+b1
DBP=a2*PTT+b2Invasive BP
14 ICU
patientsSD: 6.73 SD: 5.28
Muehlsteff
et al
(2006)
SBP=a*lnPTT+bCuff BP
(Physical test)18 healthy RMSE: 7.5
Masè
et al
(2011)
SBP=a1/PTT+b1
DBP=a2/PTT+b2
Cuff
sphygmomano
meter
(exercise) / 1
month
33 healthy-0.06
95% CI: -
13.0~+12.9
0.94
-0.25
95% CI: -
11.3~+10.8
0.88
Muehlstef
f et al
(2006)
SBP=a*(L/PTT)2+bCuff BP
(Physical test)18 healthy
RMSE: 6.9
RMSE: 7.30.93
Previous Study
Young, et al. Journal of Clinical Monitoring (1995).
Chen, et al. Medical & Biological Engineering & Computing (2000).
Poon and Zhang. EMBC’05 (2005).
Douniama, et al. Computer in Cardiology (2009).
Muehlsteff, et al. EMBC’06 (2006).
Mase, et al. Journal of Electrocardiology (2011).
8/50
Standards Reference Device Sample
Size
Difference between standard and
test device (mmHg)
Recommendation
for clinical use
AAMI Mean Standard Deviation (SD)
Mercury sphygmomanometer ≥85 ≤5 ≤ 8 Yes
Intra-arterial BP ≥15 ≤5 ≤ 8 Yes
BHS Grade Absolute difference
≤5 ≤10 ≤15
Mercury sphygmomanometer ≥85
A 60% 85% 95% Yes
B 50% 75% 90% Yes
C 40% 65% 85% No
D Worse than C No
ESH Grade Absolute difference
Mercury sphygmomanometer 33
≤5 ≤10 ≤15
1 73% 87% 96% Yes
2/3≤5 0/3≤5 -
2 ≥24% ≤3% Yes
3 - - - No
IEEE 1708 Grade Mean absolute difference (MAD)
Mercury sphygmomanometer 45
A ≤5 Yes
B 5-6 Yes
C 6-7 Yes
D ≥7 No
(2002)
(1993)
(2010)
(2014)
AAMI, American National Standard (2002). BHS protocol (1993).
European Society of Hypertension International Protocol (2010).
IEEE Standard for Wearable, Cuffless BP Measuring Device (2014).
Brief summary of the major works on PTT study for BP estimation.

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•BP is a hemodynamic parameter
•Unobtrusive way to address various factors and measure BP with acceptable accuracy
Challenge
9/50
Systolic (SBP)
Diastolic (DBP)
Mean (MBP)
Pulse Pressure (PP)
Determinants of arterial BP

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
Problem Statement
Potential factors
• Cardiovascular disease
• Calibrate interval
• Destroy assumptions
PTT
• PTT – high frequency
variation (Ma et al; Liu
et al)
• Dynamic BP – high
frequency + low frequency
• Sole PTT
• Regression models
• Cardiovascular system
is complex
PTT-BP models
𝐏𝐖𝐕 =𝐄𝐡
𝛒𝐝
PTT ~ f(HF)
𝐁𝐏 = 𝐟 𝐋𝐅 + 𝐟 𝐇𝐅
10/50
Cardiovascular
System
PTTBP
?
Accuracy
Ma, et al. EMBC’06 (2006); Liu, et al. Biomedical Signal Processing and Control (2011).

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•To analyze the potential factor affecting the accuracy
- Cardiovascular disease
- Calibration interval
•To research PTT and respiration
- Whether PTT reflect the respiratory-induced variation BP
- PTT for respiratory rate measurement
•To improve BP estimation accuracy
- Propose a new indicator
- Establish new BP models
Purpose of the Study
11/50

1
1
1
1
Motivation and Objective
Methodology
Accuracy of Healthy and Patients Group
Accuracy of Different Calibration Intervals
Conclusions
1
Introduction
Effect of Cardiovascular Disease and Calibration
Interval on Blood Pressure Estimation
Pulse Transit Time for Respiratory Rate
Estimation
BP Estimation with Pulse Transit Time and
Photoplethysmogram Intensity Ratio
Conclusions and Suggestions for Future Work

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•Simplifying assumption
- Thin, pure elastic artery E
- No change h, d
•Physiologically
- E alters with age and
cardiovascular disorders
- d changes during each cardiac cycle
- h would change with disorder
•Aim
- Impact of cardiovascular disease
- Impact of calibration interval
Problems of PTT Study with M-K Equation
𝑳
𝑷𝑻𝑻=𝑬𝒉𝝆𝒅
E: elastic modulush: blood vessel thicknessd: arterial diameter𝝆: blood densityP: blood pressureL: pulse travelling distance
https://cnx.org/contents/A4QcTJ6a@3/Blood-Flow-Blood-Pressure-and-
13/50

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•PTT-BP model
•Experimental data
Approach
DBP = MBP0 +2
γlnPTT0PTT−1
3PP0 ∙
PTT0PTT
2
SBP = DBP + PP0 ∙PTT0PTT
2
Poon and Zhang. EMBC’05 (2005).
Subjects
(n=85)
Health Group
(n=37)
Patient Group
(n=48)
Mean age (range) 57 (18-96) 27 (22-54) 80 (78-96)
Gender (M/F, n) 37/48 21/16 16/32
Hypertension (n) 36 0 36
Congestive heart failure (n) 9 0 9
Atrial fibrillation (n) 5 0 5
Ischemia heart disease (n) 5 0 5
MBP0, PP0: calibrated MBP and PP
PTT0: calibrated PTT
PTT: calculated PTT
SBP, DBP: estimated BP
14/50

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•Data collection
•Data analysis
- Mean ± SD, mean absolute difference (MAD)
- Bland-Atman plot, limit of agreement mean±1.96*SD
Data Collection and Analysis
ECG, PPG; cuff-BP
PTT for BP estimation
Reference BP
Calibrated BP
Calibrated PTTDay 1
Week 1
Week 2
Week 6
ECG, PPG
cuff-BP
PTT calculation:
15/50

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
Accuracy: Healthy versus Patient
Overall Healthy Group Patient GroupMean±SD
(mmHg)
MAD
(mmHg)
Mean±SD
(mmHg)
MAD
(mmHg)
Mean±SD
(mmHg)
MAD
(mmHg)
SBP 1.87±14.43 11.18 -0.48±11.57 9.26 3.63±16.02*** 12.62
DBP 0.11±8.51 6.49 -1.17±9.08 7.15 1.07±7.92** 5.99
SBP for patient group higher than healthy group (SD ~ 5 mmHg)
DBP estimation of patient group was lower than healthy group (~ 1 mmHg)
***p<0.001, **p<0.01
16/50
35.03 mmHg
-27.70 mmHg
22.20 mmHg
-23.13 mmHg
16.59 mmHg
-14.45mmHg
16.63 mmHg
-18.97 mmHg
Bland-Altman plot of the BP estimations for the healthy group and patient group.

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
Accuracy: Different Calibration Intervals
17/50
The accuracy significantly decreased 1 week after the calibration
Day 1 Week 1 Week 2 Week 6
Mean±SD
(mmHg)
MAD
(mmHg)
Mean±SD
(mmHg)
MAD
(mmHg)
Mean±SD
(mmHg)
MAD
(mmHg)
Mean±SD
(mmHg)
MAD
(mmHg)
SBP 1.65±10.71 7.81 2.55±14.87 12.18 3.19±14.84 11.99 0.15±16.54 12.76
DBP 1.31±4.94 3.94 -0.16±9.77 7.58 0.53±9.17 7.29 -1.23±9.14 7.17
***p<0.001
The variance of BP estimation error with increase of calibration interval.

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•Cardiovascular disorder
- Development of disease would influence the effectiveness of PTT to estimate BP
- Increase the arterial stiffness - alternation of the fluid dynamics - impairment ventricular-arterial coupling (PTT-BP)
•Calibration intervals
- Accuracy decreased with the increase of calibration period
•Explore extra parameters and modify the model to
improve the accuracy for disease population and for
longer calibration interval
Summary
18/50

1
1
1
1
Motivation and Objective
PTT for Respiration Rate Estimation
Capnobase Data
Cardiac Activities Experiment
Results
Closed-loop Model
1
Introduction
Effect of Cardiovascular Disease and Calibration
Interval on Blood Pressure Estimation
Pulse Transit Time for Respiratory Rate
Estimation
BP Estimation with Pulse Transit Time and
Photoplethysmogram Intensity Ratio
Conclusions and Suggestions for Future Work

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•Dynamic fluctuations of BP
- High frequency (HF, 0.20-0.35 Hz) – respiratory activity
- Low frequency (LF, 0.01-0.15 Hz) – arterial vasomotion
•PTT: inadequate to follow dynamic BP variations
- PTT mainly presents HF variation
- Evaluation of inspiratory effort, detect breathing events
•Objectives:
- To investigate the relationship of PTT with respiration
- To monitor breathing pattern and measure respiratory rate (RR)
Motivation and Objective
Drinnan, et al. Physiological Measurement (2001). Pitson and Stradling, European Respiratory Journal (1998).
20/50

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•Experimental Data
- Recorded signal (fs=300 Hz) (8 min)- Reference respiratory signal - Capnography (EtCO2)
- ECG
- PPG
- 42 subjects (5 excluded)- 19 Spontaneous ventilation (15.8±19.3 years)
- 18 Control ventilation (27.6±20.2)
•Algorithm procedure
- PTT for RR
- Fusion method to improve RR estimation accuracy
- Comparison with Smart Fusion (SF) method
Capnobase Dataset
http://www.capnobase.org/ Karlen et al. TBME (2013).
21/50
Average & SD>4breaths/min (×)The control method

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
RR Measurement
Respiratory
frequencyRespiratory
frequency
•Number of Breaths (RR#)
- Number of breaths in one minute
• Instantaneous RR (RRinst)
- Peak detection
- RRinst=60
𝑇𝑖𝑚𝑒 𝑖𝑛𝑡𝑒𝑟𝑣𝑎𝑙 𝑏𝑒𝑡𝑤𝑒𝑒𝑛 𝑐𝑢𝑟𝑟𝑒𝑛𝑡 𝑎𝑛𝑑 𝑝𝑟𝑒𝑣𝑖𝑜𝑢𝑠 𝑏𝑟𝑒𝑎𝑡ℎ
•RR detected from PSD (RRPSD)
- PSD: pwelch (△f=0.036 Hz)
- RRPSD=1
𝑅𝑒𝑠𝑝𝑖𝑟𝑎𝑡𝑜𝑟𝑦 𝑓𝑟𝑒𝑞𝑢𝑒𝑛𝑐𝑦
- Physiological range (0.10-0.65 Hz)
22/50

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
PTT for RR – Capnobase DataPTT
Reference respiratory signal
23/50
PTT varied each breathing cycle, spectrum at respiratory frequency
PTT could predict continuous RR quite well, particularly at stable state
Continuous RR estimations with PTT vs. reference RR

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
r=0.973.85 brpm
-2.61 brpm
r=0.955.77 brpm
-2.51 brpm
r=0.963.50 brpm
-3.80 brpm
PTT Fusion for RR
PTT, HRI and PRI have
similar variation patterns
with the reference
respiratory signal.
The fused estimations were
highly correlated with
reference RR with good
agreement.
24/50
The fused estimation
significantly agreed better
with the reference than the
controlled method.
6.59 brpm
-5.17 brpm
3.50 brpm
-3.80 brpm
p<0.001Bland-Altman plot of the estimations by the fused RRPSD
with PTT and the control method
Scatter plot of the RRPSD estimations
vs. reference RRPSD

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•30 Subjects
- 18 healthy subjects (24.8±2.3 years)
- 12 hypertensive patients (67.8±8.8 years)
•Recorded signal (fs=1000 Hz)
- One-lead ECG
- PPG from left index finger
- Continuous BP (Finapres)
- Respiratory signal (respiratory belt)
•Experimental procedure
- Position transition: supine - standing –sitting
- Maneuvers: DB – VM – HG
Cardiac Autonomic Nervous Activity
25/50

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
PTT, SBP and Respiration at Cardiac Activities
Supine ASSitting
DB VM HG
PTT varied in phase with the respiratory signal and HF spectral of SBP
26/50
PTT
SBP
Respiration
PTT
SBP
Respiration
PTT
SBP
Respiration
PTT
SBP
Respiration
PTT
SBP
Respiration
PTT
SBP
Respiration
Time series variations of PTT, SBP and respiration and their corresponding spectrum

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
RR parameters
RR# RRinst RRPSD
RMSE
(breaths/min)1.58 1.95 3.33
MAE
(breaths/min)1.06 1.26 1.64
PTT for RR Cardiac Activities
2.70 brpm
-3.38 brpm
2.91 brpm
-4.27 brpm
6.72 brpm
-6.34 brpm
Different postures
Different maneuvers
27/50
PTT is able to track RR at different positions and maneuvers
Bland-Altman plot of RR from PTT vs. reference RR Estimation error of RR with PTT
Estimation error comparison at different postures
Estimation error comparison at different maneuvers

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
Effect of Respiration on BPCentral Effect
Mechanical Effect
△V: fluctuation in respiratory volume
△RRI: fluctuation in R-R interval
△SBP: fluctuation in systolic BP
△PP: fluctuation in pulse pressure
△DBP: fluctuation in diastolic BP
△SCO: surrogate cardiac output
RSA: Respiratory Sinus Arrhythmia
ABR: Arterial Baroreflex
DER: Direct Effects of Respiration
CID: Circulatory Dynamics
The effect of respiration on BP:
- Mechanical transmission of intrathoracic pressure to arterial BP
- The respiratory-cardiac coupling through RSA and the circulation dynamics
The HR variability is under regulation:
- Arterial baroreflex mechanism
- RSA
28/50

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
Simplified Closed-loop Model
𝐏𝐓𝐓~𝒇 ∆𝑽
∆𝐒𝐁𝐏 𝐧 = 𝐢=𝟎
𝐌
𝐇𝐃𝐄𝐑 𝐢, 𝐧 ∙ 𝐏𝐓𝐓 𝐧 − 𝐢 + 𝐢=𝟎
𝐌
𝐇𝐂𝐈𝐃 𝐢, 𝐧 ∙ ∆𝐂𝐎 𝐧 − 𝐢 − 𝛕𝐂𝐈𝐃
∆𝐑𝐑𝐈 𝐧 = 𝐢=𝟎
𝐌
𝐇𝐑𝐒𝐀 𝐢, 𝐧 ∙ 𝐏𝐓𝐓 𝐧 − 𝐢 − 𝛕𝐑𝐒𝐀 + 𝐢=𝟎
𝐌
𝐇𝐀𝐁𝐑 𝐢, 𝐧 ∙ ∆𝐒𝐁𝐏 𝐧 − 𝐢 − 𝛕𝐀𝐁𝐑
29/50
HDER: transfer function
representing the direct influence of
respiratory-related intrathoracic
pressure changes on BP
HCID: transfer function representing
the circulatory dynamics
△CO=△PP/△RRI
HRSA: transfer function representing
respiratory-cardiac coupling
HABR: transfer function
representing baroreflex dynamics
Chaicharn. ProQuest (2007).

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•PTT and respiration
- PTT varies with respiration
- PTT could monitor different breathing patterns
•PTT and RR
- PTT is able to predict continuous RR
- Fusion method with PTT for RR estimation derived
improved accuracy
- RR estimation with PTT obtained acceptable accuracy
at different activities
•Hypothesis: PTT is respiratory-modulated
Summary
30/50

1
1
1
1
Background
PPG Intensity Ratio
BP model (1) – M-K Equation
BP model (2) – B-H Equation
Experimental Validation
Results
1
Introduction
Effect of Cardiovascular Disease and Calibration
Interval on Blood Pressure Estimation
Pulse Transit Time for Respiratory Rate
Estimation
BP Estimation with Pulse Transit Time and
Photoplethysmogram Intensity Ratio
Conclusions and Suggestions for Future Work

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•Continuous BP
- 1st order – heartbeat- 2nd order – HF variation- 3rd order – LF variation
•PTT
- Respiratory frequency
- 2nd order variation of BP
•3rd order
- Slow variation
- Sympathetic vasomotor
- Arterial diameter change (LF variation)
Background
Pagani, et al. Blood Pressure Variability. Ann N Y Acad Sci. 1996
𝐑𝐞𝐬𝐢𝐬𝐭𝐚𝐧𝐜𝐞 =𝟖𝛈𝐋
𝛑𝐑𝟒
32/50
Determinants of arterial BP

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
Light Source
PP
G W
avef
orm
Io
I
PPG Intensity Ratio (PIR)
Arterial diameter varies with
arterial pressure
I = I0 ∙ e−ε∙c∙l
𝐈𝐋 = I0 ∙ e−αDC∙dDC ∙ e−α∙Ds
𝐈𝐇 = I0 ∙ e−αDC∙dDC ∙ e−α∙Dd
∆𝐝 = Ds − Dd =1
α∙ ln𝐈𝐇𝐈𝐋
PIR =IHIL= eα∙∆d
PPG Intensity Ratio (PIR) can reflect the
relative change of arterial diameter
∆d
Tissues
Venous blood
Non-pulsatile
component of
arterial blood
Pulsatile
component of
arterial blood
Ds
IL
Systolic
Dd
IH
Diastolic
Beer-Lambert Law:
33/50
ε: absorption coefficient
c: concentration of the material
l: effective light path
α= ε•c

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•Cardiovascular nervous autonomic function tests- AS – mainly sympathetic
- DB – parasympathetic
- VM – sympathetic
- HG - sympathetic
•ECG, PPG, and continuous BP (fs=1000 Hz)
•5 subjects
•Heart rate interval (RRI), PTT, PIR, SBP, DBP, PP - Time domain
- Spectral domain: - PSD
- LF:HF ratio- evaluation of sympatho-parasympathetic balance
Experimental Analysis of PIR
34/50

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
PTT mainly coupled with SBP/PP at HF band
PIR coupled SBP/DBP at LF band
SupineRRI
PTT
PIR
SBP
DBP
PP
AS Sitting
DB VM HG
RRI
PTT
PIR
SBP
DBP
PP
RRI
PTT
PIR
SBP
DBP
PP
RRI
PTT
PIR
SBP
DBP
PP
RRI
PTT
PIR
SBP
DBP
PP
RRI
PTT
PIR
SBP
DBP
PP
PIR – LF Variation
PIR evaluate BP regulation in LF range, which is the sympathetic
modulation that is due to the change of arterial diameter
PSD of HRI, PTT, PIR and SBP at different maneuvers
LF:HF ratio
35/50
Time series variations and spectrum at different states

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
• PP estimation with PTT
(M-K equation)
BP Model (1) –M-K Equation
E =∆P
∆Ro∙2 1 − σ2 RoRi
2
Ro2 − Ri
2 PWV ∝1
PTT
L
PTT=∆P
∆Ro∙2 1 − σ2 RoRi
2
Ro2 − Ri
2 ∙ℎ
𝜌𝐷
PP ∝1
PTT2
𝐏𝐏 = 𝐏𝐏𝟎 ∙𝐏𝐓𝐓𝟎𝐏𝐓𝐓
𝟐
• DBP estimation with PIR
(Windkessel Model)
DBP = P0 ∙ e− t RC
1
PIR= e−α∙∆d
DBP ∝1
PIR
Bergel, et al. The Journal of Physiology (1961). Parker, et al. Medical & Biological Engineering & Computing (2009).
𝐃𝐁𝐏 = 𝐃𝐁𝐏𝟎 ∙𝐏𝐈𝐑𝟎𝐏𝐈𝐑
𝐒𝐁𝐏 = 𝐃𝐁𝐏𝟎 ∙𝐏𝐈𝐑𝟎𝐏𝐈𝐑+ 𝐏𝐏𝟎 ∙
𝐏𝐓𝐓𝟎𝐏𝐓𝐓
𝟐
△P: PP in the artery
Ro: the external radius
△Ro: external radius change
Ri: the internal radius
σ: Poisson’s ratio
P0: end-systolic aortic pressure
R: peripheral resistance
C: the compliance
36/50
𝐏𝐖𝐕 =𝐄𝐡
𝛒𝐝

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•Subjects
- 27 healthy adults (14 males, 25.6±2.1 years)
- Rest at seated position
•Recorded signals (fs=1000 Hz)
- Finapres BP (left arm and left thumb)
- One-lead ECG (left and right arms)
- PPG (left index finger)
•Accuracy evaluation
- Mean±SD, MAD
- Bland-Altman plot
- Comparison with other two control methods
Experimental Validation
37/50
𝐏𝐓𝐓𝐌𝐞𝐭𝐡𝐨𝐝 𝟐 :
𝐃𝐁𝐏 = 𝐌𝐁𝐏𝟎 +𝟐
𝛄𝐥𝐧𝐏𝐓𝐓𝟎
𝐏𝐓𝐓−𝟏
𝟑𝐏𝐏𝟎 ∙
𝐏𝐓𝐓𝟎
𝐏𝐓𝐓
𝟐
𝐒𝐁𝐏 = 𝐃𝐁𝐏 + 𝐏𝐏𝟎 ∙𝐏𝐓𝐓𝟎
𝐏𝐓𝐓
𝟐
𝐏𝐓𝐓𝐌𝐞𝐭𝐡𝐨𝐝 𝟏 :
𝐒𝐁𝐏 = 𝐒𝐁𝐏𝟎 −𝟐
𝛄𝐏𝐓𝐓𝟎𝐏𝐓𝐓 − 𝐏𝐓𝐓𝟎
Chen, et al. Medical & Biological Engineering & Computing (2000). Poon and Zhang. EMBC’05 (2005).

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
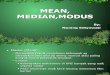
Overall BP estimations against the reference BP.
Overall Accuracy
SBP
MBP
DBP
SBP
MBP
DBP
SBP DBP MBPr=0.91 r=0.88 r=0.89
Mean±SD: -0.37±5.21
MAD: 4.09
Mean±SD: -0.08±4.06
MAD: 3.18
Mean±SD: -0.18±4.13
MAD: 3.18
38/50
Scatter diagram of estimated BP vs. reference
Bland-Altman plot of estimations with the reference

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
Beat-to-beat BP estimation by the proposed methods (green), the control
methods (blue) with the reference (red) as the benchmark.
Comparison with Other Methods
PTT Method (1) PTT Method (2) Proposed Method
Mean
(mmHg)
SBP 0.19 -0.11 -0.37
DBP - 0.19 -0.08
MBP - 0.09 -0.18
SD
(mmHg)
SBP 6.21 7.31 5.21*†
DBP - 6.03 4.06†
MBP - 6.25 4.13†
MAD
(mmHg)
SBP 4.94 5.76 4.09*†
DBP - 4.80 3.18†
MBP - 4.96 3.18†
* compare with PTT method (1) with p<0.05;
† compare with PTT method (2) with p<0.05.
The proposed BP model achieved better accuracy than the two
compared PTT methods in estimating SBP/DBP/MBP
39/50

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
BP Model (2) – B-H Equation
40/50
• MBP is determined by
- Cardiac output, systemic vascular
resistance
- LF variation
• PP derivation – B-H equation
∆d = Ds − Dd =1
α∙ lnPIR ≈
PIR
α
𝐌𝐁𝐏 = 𝐌𝐁𝐏𝟎 ∙𝐏𝐈𝐑𝟎𝐏𝐈𝐑
𝐏𝐖𝐕 =𝐕
𝛒∆ 𝐕 ∆𝐏
∆V
V ∙ ∆P=Ds2 − Dd
2
Dd2 ∙ PP
=Ds + Dd
Dd2 ∙∆d
PP
L
PTT=
1
ρ ∙ (Ds + Dd ) Dd2 ∙PP
∆d
PP =ρL2 Ds + Dd
Dd2 ∙ ∆d ∙
1
PTT2PP ∝
PIR
PTT2
𝐏𝐏 = 𝐏𝐏𝟎 ∙𝐏𝐈𝐑
𝐏𝐈𝐑𝟎∙𝐏𝐓𝐓𝟎
𝐏𝐓𝐓
𝟐
𝐒𝐁𝐏 = 𝐌𝐁𝐏𝟎 ∙𝐏𝐈𝐑𝟎𝐏𝐈𝐑+𝟐
𝟑∙ 𝐏𝐏𝟎 ∙
𝐏𝐈𝐑
𝐏𝐈𝐑𝟎∙𝐏𝐓𝐓𝟎𝐏𝐓𝐓
𝟐
𝐃𝐁𝐏 = 𝐌𝐁𝐏𝟎 ∙𝐏𝐈𝐑𝟎𝐏𝐈𝐑−𝟏
𝟑∙ 𝐏𝐏𝟎 ∙
𝐏𝐈𝐑
𝐏𝐈𝐑𝟎∙𝐏𝐓𝐓𝟎𝐏𝐓𝐓
𝟐
𝐌𝐁𝐏 =𝟏
𝟑𝐒𝐁𝐏 +
𝟐
𝟑𝐃𝐁𝐏
𝐏𝐏 = 𝐒𝐁𝐏 − 𝐃𝐁𝐏
• PIR
- Arterial diameter change –
peripheral resistance
- LF variations of BP

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•Subjects
- 10 healthy adults (6 males, 24.9±1.9 years)
- Rest at seated position
•Recorded Signals (fs=1000 Hz)
- One-lead ECG (left and right arms)
- PPG (left index finger)
- Finapres BP (left arm and left thumb)
•Accuracy evaluation
- Finapres BP – reference
- Mean±SD
- Bland-Altman plot
Experimental Validation
41/50
MethodMean
(mmHg)
SD
(mmHg)
MAD
(mmHg)
Proposed
method
SBP -0.41 5.15* 4.18*
DBP -0.84 4.05† 3.43†
PTT Method
(1)
SBP 0.62 7.19 5.82
DBP 1.18 6.12 5.03
*SBP: Significant different level <0.05; †DBP: significant different level <0.05;
The proposed BP model agreed good with the reference
Achieved better accuracy than one of the control method for SBP/DBP
9.68 mmHg
-10.05 mmHg
7.10 mmHg
-8.78 mmHg
Bland-Altman plot of SBP and DBP estimation.

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
PTT-BP Model
SBP DBP MBP
PM1 SBP = DBP + PP0 ∙PTT0PTT
2
DBP = DBP0 ∙PIR0PIR
MBP =1
3SBP +
2
3DBP
PM2 SBP = MBP0 ∙PIR0PIR+2
3∙ PP0 ∙
PIR
PIR0∙PTT0PTT
2
DBP = MBP0 ∙PIR0PIR−1
3∙ PP0 ∙
PIR
PIR0∙PTT0PTT
2
MBP = MBP0 ∙PIR0PIR
CM1 SBP = SBP0 −2
γPTT0∙ PTT − PTT0 DBP = DBP0 −
2
γPTT0∙ PTT − PTT0 MBP =
1
3SBP +
2
3DBP
CM2 SBP = DBP + PP0 ∙PTT0PTT
2
DBP = MBP0 +2
γlnPTT0PTT−1
3PP0 ∙
PTT0PTT
2
MBP = MBP0 +2
γlnPTT0PTT
CM3 SBP = a3 ∙ PTT + b3 DBP = a3′ ∙ PTT + b3
′MBP =
1
3SBP +
2
3DBP
CM4 SBP = a4 ∙ lnPTT + b4 DBP = a4′ ∙ lnPTT + b4
′MBP =
1
3SBP +
2
3DBP
CM5 SBP =a5PTT+ b5 DBP =
a5′
PTT+ b5
′ MBP =1
3SBP +
2
3DBP
CM6 SBP =a6PTT2+ b6 DBP =
a6′
PTT2+ b6
′ MBP =1
3SBP +
2
3DBP
Comparison Study
Chen, et al. Medical & Biological Engineering & Computing, 2000.
Poon, et al. EMBC’05, 2005.
Douniama, et al. Computer in Cardiology, 2009.
Muehlsteff, et al. EMBC’06, 2006.
Mase, et al. Journal of Electrocardiology. 2011.
Proposed method (PM); Comparison method (CM)
42/50

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
Subjects
(n=33)
Normotensive Group
(n=19)
Hypertensive Group
(n=14)
Mean age (range) 43 (21-77) 26 (21-47) 67 (43-77)
Hypertension (n) 14 0 14
Prehypertension 7 0 7
Stage I hypertension 6 0 6
Stage II hypertension 1 0 1
SBP (mmHg) 121.12±19.52 107.74±10.04 139.30±13.50
DBP (mmHg) 68.92±8.16 65.21±6.96 74.00±7.00
Experimental Validation
•Subjects (N=33)
•Recorded signal- ECG, PPG, Finapres BP
•Experiment protocol- Different positions (supine, standing, sitting); DB, VM, HG
- Following on the second day (8 subjects, sitting rest)
43/50

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
Overall Accuracy Comparison
SBP DBP MBP
PM better than CM; PM1-PM2, CM1-CM2, SD<8 mmHg
44/50
Indicating the best performance
Overall estimation error of the proposed methods (PM) and comparison methods (CM) at
steady state.

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
Comparison of Different Maneuvers
Supine
45/50
HGVMDB
Sitting AS
PM1 and PM2 on the whole were better than other methods, followed by CM1-CM2
Physiological model provides more accurate estimation that regression model
Indicating the best performance
Estimation errors at different positions and different maneuvers.

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
Different Calibration Interval
***
***
***
***
***
***
***
***
***
46/50
Estimation error significantly increased second day after the initial calibration
Accuracy by using proposed method remained better for SBP and MBP estimation
Indicating the best performance
Estimation error of the Day 1 and Day 2 after the initial calibration for PM1-PM2, CM1-CM2.

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•A new parameter PIR
- Relative change in arterial diameter
- Evaluate LF variation of BP
•Two BP models established with PTT and PIR
- PTT could reflect HF range of BP
- PTT for LF variation of BP, and arterial diameter change
•The performance of the proposed models
- Comparison of other PTT methods
- Extended calibration interval
Summary
47/50
•The combination of PTT and PIR improved the accuracy of BP estimation
- The 2nd and 3rd order variation
- Short-term variability
•The accuracy over
the second day decreased
- The circadian fluctuations?
- Long-term variability (24 h)
•Controlling mechanism of
circadian BP rhythm
- Hemodynamic circadian rhythms
- Neural and hormonal (Sympatho-adrenergic mechanism)Furlan, et al. Circulation (1990). Millar-Craig, et al. Lancet (1978).

1
1
1
1
Conclusions
Suggestions for Future Work
1
Introduction
Effect of Cardiovascular Disease and Calibration
Interval on Blood Pressure Estimation
Pulse Transit Time for Respiratory Rate
Estimation
BP Estimation with Pulse Transit Time and
Photoplethysmogram Intensity Ratio
Conclusions and Suggestions for Future Work

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•The examination of the impact of the cardiovascular disease and calibration interval on the accuracy of PTT-based cuffless BP estimation
•A new interpretation of PTT for its contribution to track BP changes; the usage of PTT for continuous RR estimation
•Propose of a new indicator, PIR, to evaluate the LF variation of BP
•Establishment of novel BP models with the integration of PTT and PIR to improve the estimation accuracy
Contribution
49/50

Analysis PTT for RR PIR and PTT for BPIntroduction Conclusion and Future Work
•To further validate the proposed models
- Intra-arterial BP as reference
- Following standard IEEE 1708
•To improve the accuracy for subject with CVDs
- Potent parameter other than PTT
- Modify models
•To address the calibration issue
- Investigate the minimal interval ensuring the accuracy
- Explore ways to extend the calibration interval
Future Work
50/50

Prof. Hon Ki Tsang
Prof. Yuanting Zhang
Prof. Ni Zhao
Prof. Carmen Poon
Prof. Toshiyo Tamura
Prof. Bryan Yan
Prof. Walter Karlen
Acknowledgement
Jing Liu
Wenxuan Dai
Yali Zheng
Peng Su
EE Colleagues- Terahertz group- Robotics group- Biosensing group
Friends
Wei and my family

Journal publications:
Ding, X., Zhang, Y., Liu, J., Dai, W., & Tsang, H. (2016). Continuous Cuffless Blood Pressure Estimation Using Pulse TransitTime and Photoplethysmogram Intensity Ratio. IEEE Transactions on Biomedical Engineering, 63(5), 964-972.
Ding, X., Zhang, Y., & Tsang, H. (2016). Impact of Heart Disease and Calibration Interval on Accuracy of Pulse Transit TimeBased Blood Pressure Estimation. Physiological Measurement, 37(2), 227-237.
Zheng, Y., Ding, X., Poon, C., Lo, B., Zhang, H., Zhou, X., Yang, G., Zhao, N. & Zhang, Y. (2014). Unobtrusive Sensing andWearable Devices for Health Informatics. IEEE Transactions on Biomedical Engineering, 61(5), 1538-1554.
Ding, X., Yan, B., Karlen, W., Zhang, Y., Liu, J., Dai, W., & Tsang, H. Estimation of Respiratory Rate with Pulse Transit timeunder the modulation of Cardiac Autonomic Nervous Activity. (Preparing)
Ding, X., Zhang, Y., Yan, B., Liu, J., Dai, W., & Tsang, H. A Comprehensive Study on Pulse Transit Time Based ContinuousCuffless Blood Pressure Measurement. (Preparing)
Newsletter:
Ding, X., Liu, J., Zhao, N., & Zhang, Y. T. (2014). Cardiovascular Health Informatics: Wearable Medical Device and FlexibleBiosensor for m-Health. IEEE Life Science Newsletter, Mar 2014.
Conference publications:
Ding, X., Zhang, Y., Tsang, H., & Karlen, W. (2016). A Pulse Transit Time Based Fusion Method for the Noninvasive andContinuous Monitoring of Respiratory Rate. 38th Annual International Conference of the IEEE Engineering in Medicine andBiology Society, (EMBC’16) (Accepted).
Ding, X., Zhang, Y., & Tsang, H. (2016). A New Modeling Methodology for Continuous Cuffless Blood PressureMeasurement. Proceedings of the International Conference on Biomedical and Health Informatics, (BHI 2016), Las Vegas,2016.
Ding, X., Jing, L., Dai, W., Carvalho, P., Magjarevic, R., & Zhang, Y. (2015). An Attempt to Define the Pulse Transit Time.Proceedings of the International Conference on Biomedical and Health Informatics (ICBHI 2015), Haikou, China.
Ding, X., Dai, W., Luo, N., Liu, J., Zhao, N., & Zhang, Y. (2015). A Flexible Tonoarteriography-Based Body Sensor Networkfor the Cuffless Measurement of Arterial Blood Pressure. Proceedings of 12th Annual Body Sensor Networks Conference2015 (BSN 2015), MIT, Cambridge, USA.
Publication

Conference publications:
Ding, X., & Zhang, Y. (2015). Photoplethysmogram Intensity Ratio: A Potential Indicator for Improving the Accuracy ofPTT-Based Cuffless Blood Pressure Estimation. Proceedings of the 37th Annual International Conference of the IEEEEngineering in Medicine and Biology Society. Milan, Italy, 2015.
Liu, J., Zhang, Y., Ding, X., Dai, W., & Zhao, N. (2016). A Preliminary Study on Multi-Wavelength PPG Based Pulse TransitTime Detection for Cuffless Blood Pressure Measurement. 38th Annual International Conference of the IEEE Engineering inMedicine and Biology Society, (EMBC’16) (Accepted).
Liu, J., Li, Y., Ding, X., Dai, W., & Zhang, Y. T. (2015). Effects of Cuff Inflation and Deflation on Pulse Transit TimeMeasured from ECG and Multi-Wavelength PPG, Proceedings of the 37th Annual International Conference of the IEEEEngineering in Medicine and Biology Society, Milan, Italy, 2015.
Ding, X., Zheng, Y., Dai, W., & Zhang, Y. T. (2014). Changes in Blood Pressure with Different Postures While Swallowing.The International Conference on Health Informatics, pp. 179-181.
Dai, W., Ding, X., Zheng, Y., & Zhang, Y. T. (2014). Amplitude Index for the Quality Assessment of Pulsatile Signals inNoise. The International Conference on Health Informatics, pp. 228-230.
Ding, X., Zhang, Y. T. (2014). Cuff-less Continuous Blood Pressure Estimation with Pulse Transit Time andPhotoplethysmogram Intensity Ratio. Proceedings of International Biomedical Engineering Conference 2014, pp. 351.
Book Chapter:
Poon, C., Zheng, Y., Luo, N., Ding, X., & Zhang, Y. T. (2014). Wearing Sensors Inside and Outside of the Human Body forthe Early Detection of Diseases. Wearable Sensors. Elsevier Inc.
Patents:
Zhang Y., Ding, X., Liang, Y., Liu J., Dai, W., and Yuan, S (2015). License Agreement on software “m-Health and WearableTechnologies for Physiological Watch” with Huawei Device (Dongguan) Co., Ltd.
Zhang, Y., Tsang, H, Zhao, N, Ding, X., Liu, J, and Dai, W. Unobtrusive Multi-sensor Array for Pulse Wave velocity/BloodPressure Imaging. (Pending).
Zhao, N., Zhang, Y., Liu, J, Ding, X., Dai, W., Yuan, S., Li Yao. Method for Measuring Cardiovascular and RespiratoryParameters Based on Multi-Wavelength Photoplethysmography. (Provisional)
Publication

Thank you!