Embed Size (px)
Citation preview

DHF in Pediatrics Patient
แพทย์�หญิ�งชารี ย์า ธานี กุ�มารีแพทย์�โรีคติ�ดเช��อ
โรีงพย์าบาลสรีรีพส�ทธ�ปรีะสงค� อ�บลรีาชธานี

WHO Case Classification Before 2009:
Currently use in Thailand
Acute Dengue Infection
Asymptomatic (90%) Symptomatic (10%)
Acute febrile illness(Viral infection) (5%)
Dengue Fever (DF) (4%)
Dengue Hemorrhagic Fever (DHF) (1%)
No shock DSS (0.1-0.2%)J Med Assoc Thai 2011; 94 (Suppl. 3): S57-S63

The Spectrum of DHF
Source: WHO. Dengue Guidelines for Diagnosis, Treatment, Prevention and Control. 2nd edition

DHF by WHO Criteria
• Currently use in Thailand 1. High continuous fever: 2 – 7 days
2. Hemorrhagic manifestations: Petechiae, Tourniquet Test positive
3. Platelet count ≤ 100,000 cells/mm3
4. Plasma leakage: rising Hct ≥ 20% from baseline, pleural effusion, ascites

Source: WHO. Dengue Guidelines for Diagnosis, Treatment, Prevention and Control. New edition 2009
North America
Africa
Latin America
EuropeAsia

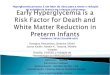
New Edition Of Dengue Guideline 2009
DENCO STUDY; Prospective hospital based multicenter, Latin America & Europe & Asia, n= 1734

SEVERE DENGUE
1.Severe plasma leakage2.Severe haemorrhage3.Severe organ impairment
DENGUE
Revised Dengue Classification
WithoutWithWARNING SIGNS
Warning Signs*• Abdominal pain or tenderness• Persistent vomiting• Clinical fluid accumulation• Mucosal bleed• Lethargy; restlessness• Liver enlargement >2cm• Laboratory: Increase in HCT concurrent with rapid decrease in platelet count
1. Severe plasma leakage leading to • Shock (DSS)• Fluid accumulation with
respiratory distress2. Severe bleeding
as evaluated by clinician3. Severe organ involvement Liver: AST or ALT>=1000 CNS: Impaired consciousness Heart and other organs
Probable DengueLive in / travel to dengue endemic area. Fever and 2 of the following criteria:
Nausea, vomiting Rash Aches and painsTourniquet test +ve LeucopeniaAny warning sign
* Requiring strict observation and medical intervention
± Warning Signs
Lab. confirmed dengue(important when no sign of plasma leakage)
Slide collection from Dr. Kulkanya Chokephaibulkit

Clinical Diagnosis of DHF
Source: WHO. Dengue Guidelines for Diagnosis, Treatment, Prevention and Control. New edition 2009

DSS Manifestations
J Med Assoc Thai 2011; 94 (Suppl. 3): S57-S63
A retrospective study, 109 children with shock, QSNICH, 2008-2009

DSS Manifestations
J Med Assoc Thai 2011; 94 (Suppl. 3): S57-S63

DSS Manifestations
J Med Assoc Thai 2011; 94 (Suppl. 3): S57-S63

DSS Manifestations
J Med Assoc Thai 2011; 94 (Suppl. 3): S57-S63

DSS Manifestations
J Med Assoc Thai 2011; 94 (Suppl. 3): S57-S63

DSS Manifestations
J Med Assoc Thai 2011; 94 (Suppl. 3): S57-S63

Laboratory Investigation 80 400 46
70 350 44
60 300 42
50 250 40
40 200 38
30 150 36
20 100 34
10 50 32
0 0 30
-5 -4 -3 -2 -1 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
* Day of shock or subsidence of fever
Serial determinations of atypical lymphocytes (buffy coat), platelets, and hematocrit in (secondary) DHF
Day of illness
HEMATOCRIT
ATYPICAL LYMPHOCYTES
PLATELETS

Confirmation Laboratory InvestigationPrimary Infection Secondary Infection

Comparison between percentage of viral detection and number of days of fever. Percentage of viral detection was inversely proportional to the number of days of fever. Number of positive/negative samples analyzed by real-time PCR on days 1 to 8 of fever: day1-2 n=3/3; day3 n=5/12; day4 n=10/23; day5 n=9/23; day6 n=8/20; day7 n=3/12 and day8 n=1/7.
Chutinimitkul S, et al. J Virol Methods.

Dengue NS1 Antigen
Slide collection from Chokephaibulkit K.

Detection of all dengue virus serotypes by PlateliaTM Dengue NS1 Ag
No significant difference is observed between the 4 dengue virus serotypes.
Slide collection from Chokephaibulkit K.

Dengue NS1 Antigen
Slide collection from Chokephaibulkit K.

0 1 2 3 4 5 6 7 80
20
40
60
80
100
PCRIgMNS1viral culture
Day of illness
% s
ensi
tivi
ty
Diagnostic Options and Sensitivity
PCR and NS1 Ag จะม sensitivity ส"งส�ดท # 1st day of fever ซึ่%#งม peak viremia
Preliminary report from QSNICH, N=772 case

Managementกุารีด"แลผู้"'ป(วย์ไข้'เล�อดออกุ ปรีะกุอบด'วย์ 3
รีะย์ะ
1 .กุารีด"แลรีะย์ะไข้'
2. กุารีด"แลรีะย์ะว�กุฤติ / shock ในีโรีงพย์าบาล
3. กุารีด"แลรีะย์ะพ.กุฟื้0� นี

กุารีด"แลรีะย์ะไข้'1. กุารีลดไข้' ให'ย์า paracetamal 10-12 mg/kg/dose
(แนีะนี1าใช'ในีกุรีณี BT ≥39 Co ท�กุ 4-6 ชม.)
ห'ามใช'ย์า aspirin, NSIAD เช3นี Ibuprofen
2. อาหารี: อาหารีอ3อนี ย์3อย์ง3าย์ ด�#มนีม นี1�าผู้ลไม' / นี1�าเกุล�อแรี3
3. ควรีหล กุเล #ย์งย์าท #ไม3จ1าเป4นีรีวมท.�ง antibiotic
4. กุารีให' IV fluid เม�#อม ข้'อบ3งช �เท3านี.�นี

• ม อากุารีเลวลงเม�#อไข้'ลง
• เล�อดออกุผู้�ดปกุติ�• อาเจ ย์นีมากุ/ปวด
ท'องมากุ• กุรีะหาย์นี1�าติลอด
เวลา• ซึ่%ม ไม3ด�#มนี1�า
• ม อากุารีช5อกุหรี�ออากุารี impending shock
- ม�อเท'าเย์5นี - กุรีะส.บกุรีะส3าย์ รี'องกุวนีมากุในีเด5กุ
เล5กุ - ติ.วเย์5นี เหง�#อออกุ ติ.วลาย์ - ป6สสาวะนี'อย์ลงหรี�อไม3ป6สสาวะ 4-6
ชม.• ความปรีะพฤติ�เปล #ย์นีแปลง เช3นี พ"ด
ไม3รี"'เรี�#อง เพ'อ เอะอะโวย์วาย์
กุารีด"แลรีะย์ะไข้'กุารีด"แลรีะย์ะไข้'5. กุารีให'ค1าแนีะนี1าอากุารีท #เป4นีส.ญิญิาณีอ.นีติรีาย์แกุ3ผู้"'ปกุครีอง

กุารีด"แลรีะย์ะไข้'6. กุารีติ�ดติามกุารีเปล #ย์นีแปลงทางคล�นี�กุและห'อง
ปฏิ�บ.ติ�กุารี
นี.ดผู้"'ป(วย์มาติรีวจติ�ดติามท�กุรีาย์
จนีกุว3าจะม ไข้'ลงอย์3างนี'อย์ 24 ชม. โดย์ไม3ได'ให'ย์าลดไข้' ปรีะว.ติ�: อากุารีท.#วไป ซึ่%ม อาเจ ย์นี เล�อดออกุ กุารีกุ�นี
อาหารี จ1านีวนีนี1�าด�#ม ปรี�มาณี/ส ข้องป6สสาวะ,อ�จจารีะ ติรีวจรี3างกุาย์: vital sign ข้นีาดข้องติ.บ Tourniquet test

Tourniquest Test
Positive Negative
- ให'ค1าแนีะนี1ากุารีปฏิ�บ.ติ�ติ.ว/ย์าลดไข้' - งดกุล�3มแอสไพรี�นีและกุล�3ม NSAIDs- กุารีด�#ม ORS นี1�าหวานี นี1�าผู้ลไม' (งดส ด1า-แดง)- กุารีติรีวจ CBC หรี�อ Dengue titer (NS1) (ถ้'าม ) ท�กุรีาย์ในีไข้' ว.นีท # 1-3
- ให'ค1าแนีะนี1ากุารีปฏิ�บ.ติ�ติ.ว/ย์าลดไข้' - งดกุล�3มแอสไพรี�นีและกุล�3ม NSAIDs- กุารีด�#ม ORS นี1�าหวานี นี1�าผู้ลไม' (งดส ด1า-แดง)- กุารีติรีวจ CBC หรี�อ Dengue titer (NS1) (ถ้'าม ) ท�กุรีาย์ในีไข้' ว.นีท # 1-3
- นี.ด F/U ว.นีติ3อว.นี - ให'ค1าแนีะนี1า (แผู้3นีพ.บ)- ท1า TT ซึ่1�า ถ้'าบวกุ ส3งเจาะ CBC- หาสาเหติ�อ�#นี/รี.กุษาติามสาเหติ�
- นี.ด F/U ว.นีติ3อว.นี - ให'ค1าแนีะนี1า (แผู้3นีพ.บ)- ท1า TT ซึ่1�า ถ้'าบวกุ ส3งเจาะ CBC- หาสาเหติ�อ�#นี/รี.กุษาติามสาเหติ�
แนีวทางกุารีด"แลผู้"'ป(วย์ไข้'เล�อดออกุ รีพ.สรีรีพส�ทธ�ปรีะสงค� อ�บลรีาชธานี : update June 2011

Tourniquest Test ใช้�เครื่��องวั�ดที่��มี�ขนาด cuff พอเหมีาะ (2/3 ของต้�นแขน)
บี�บีควัามีด�นไวั�ที่�� SBP + DBP /2
รื่�ดค�างไวั� 5 นาที่� คลายออกรื่อ 1 นาที่� ถ้�าต้รื่วัจพบีจ ดเล�อดออก ≥10 จ�ด/ติารีางนี��ว: Positive

Sensitivity Specificity
วั�นที่�� 1 ของโรื่ค 53.3 75.8
วั�นที่�� 2 ของโรื่ค 70.6 77.8
วั�นที่�� 3 ของโรื่ค 98.7 74.2
Tourniquest Test

Tourniquest Test Positive
CBC
แนีวทางกุารีด"แลผู้"'ป(วย์ไข้'เล�อดออกุ รีพ.สรีรีพส�ทธ�ปรีะสงค� อ�บลรีาชธานี : update June 2011
WBC ≤5,000
platelet ≤ 100,000
พ�จารีณีา admit
ให'สารีนี1�าติาม Flow
กุารีให'
สารีนี1�า
WBC ≤5,000
platelet ≤ 100,000
พ�จารีณีา admit
ให'สารีนี1�าติาม Flow
กุารีให'
สารีนี1�า
WBC ≤ 5,000
platelet ≥ 100,000
ด"แลติ3อเนี�#องท #บ'านี ส.งเกุติอากุารีช5อกุ อากุารีท #ติ'องมาโรีงพย์าบาลนี.ด F/U ภาย์ในี 12-24 ช.#วโมงติรีวจ CBC ซึ่1�าในีว.นีถ้.ดมา
WBC ≥ 5,000
platelet ≥ 100,000
ด"แลติ3อเนี�#องท #บ'านี ส.งเกุติอากุารีช5อกุ อากุารีท #ติ'องมาโรีงพย์าบาลนี.ด F/U ภาย์ในี 24
ช.#วโมงติรีวจ CBC ซึ่1�าในีว.นีถ้.ดมา
WBC ≥ 5,000
platelet ≥ 100,000
ด"แลติ3อเนี�#องท #บ'านี ส.งเกุติอากุารีช5อกุ อากุารีท #ติ'องมาโรีงพย์าบาลนี.ด F/U ภาย์ในี 24
ช.#วโมงติรีวจ CBC ซึ่1�าในีว.นีถ้.ดมา

ข้'อบ3งช �ในีกุารี admit• ซึ่%มอ3อนีเพล ย์ กุ�นีไม3ได' อาเจ ย์นี ปวดท'องรี�นีแรีง• ไข้'ลดลงแติ3อากุารีไม3ด ข้%�นี / ม กุารีเปล #ย์นีแปลงรีะด.บความรี"'ส%กุ
ติ.ว /
• ม เล�อดออกุมากุผู้�ดปกุติ� / ผู้"'ป(วย์ grade III/ IV • ผู้"'ป(วย์ท #ม ภาวะเส #ย์งส"ง: ผู้"'ป(วย์อ'วนี , เด5กุอาย์� ≤ 1 ป< ม โรีคปรีะจ1าติ.ว: G6PD deficiency,
Thalassemia, Heart disease, ม อากุารีทางสมองหรี�อแสดงอากุารีผู้�ดปกุติ�เรี5ว
Unusual manifestration:
Encephalopathy แนีวทางกุารีด"แลผู้"'ป(วย์ไข้'เล�อดออกุ รีพ.สรีรีพส�ทธ�ปรีะสงค� อ�บลรีาชธานี :
update June 2011

กุารีด"แลรีะย์ะว�กุฤติ• รีะย์ะว�กุฤติ (เม�#อ platelet count ≤ 100,000 cells/mm3)
• รีะย์ะเวลาท #เกุ�ด: 24-48 hours
• ปรี�มาณีสารีนี1�า = M + 5% deficit with in 48 hrs
– ค�ดติาม IBW / weight for height
• Type of fluid: Isotonic salt solution; 5%DAR, 5%DLR, 5%
DNSS
ศิ$รื่$เพ%ญ ก�ลยาณรื่ จ. แนวัที่างการื่วั$น$จฉั�ยและรื่�กษาโรื่คไข�เล�อดออก. กรื่ะที่รื่วังสาธารื่ณส ข

Dynamic Time of Plasma Leakage in DHF
ศิ$รื่$เพ%ญ ก�ลยาณรื่ จ. แนวัที่างการื่วั$น$จฉั�ยและรื่�กษาโรื่คไข�เล�อดออก. กรื่ะที่รื่วังสาธารื่ณส ข

Rate of IV Fluid in DHF grade I & II
Hrs after leakage
1.5 ml/kg/hr 3-5 ml/kg/hr
7 ml/kg/hr
ศิ$รื่$เพ%ญ ก�ลยาณรื่ จ. แนวัที่างการื่วั$น$จฉั�ยและรื่�กษาโรื่คไข�เล�อดออก. กรื่ะที่รื่วังสาธารื่ณส ข

สมาคมเวชบ1าบ.ดว�กุฤติแห3งปรีะเทศไทย์Siriraj Med J 2007; 59: 201-5.


Rate of IV fluid in DSS
10-5 ml/kg/hr
5 ml/kg/hr
3 ml/kg/hr
3-1 ml/kg/hr
Hrs after shock
Total Volume = M+5% deficit in 24 hrs
ศิ$รื่$เพ%ญ ก�ลยาณรื่ จ. แนวัที่างการื่วั$น$จฉั�ยและรื่�กษาโรื่คไข�เล�อดออก. กรื่ะที่รื่วังสาธารื่ณส ข

สมาคมเวชบ1าบ.ดว�กุฤติแห3งปรีะเทศไทย์Siriraj Med J 2007; 59: 201-5.




DSS management
• Colloidal solution: เล�อกุใช' Plasma expander group:
10%Dextran-40 in NSS/ 10% Haes-steril เท3านี.�นี
• Dose; 10ml/ kg/ dose (Max 30 ml/ kg/ day)
• ไม3ควรีใช' plasma หรี�อ colloid ในีกุล�3ม plasma
substitue ท #ม osmolarity เท3ากุ.บ plasma
• เม�#อให' Dextran ครีบชม.แล'ว ให'เปล #ย์นีเป4นี crytalloid
solution โดย์ให' rate ติามรีะย์ะท #ผู้"'ป(วย์อย์"3ในีข้ณีะนี.�นีศิ$รื่$เพ%ญ ก�ลยาณรื่ จ. แนวัที่างการื่วั$น$จฉั�ยและรื่�กษาโรื่คไข�เล�อดออก. กรื่ะที่รื่วัง
สาธารื่ณส ข

DSS management• A – Acidosis ม.กุพบในีผู้"'ป(วย์ท #ม prolonged shock/ • concealed/ internal bleeding
• B – Bleeding• C – Hypocalcemia• D – Dextrose, Blood sugar• Lab อ�#นีๆ เช3นี LFT, BUN, Creatine,
Coagulogram, Electrolyte, CXR• Cross match for blood component
ศิ$รื่$เพ%ญ ก�ลยาณรื่ จ. แนวัที่างการื่วั$น$จฉั�ยและรื่�กษาโรื่คไข�เล�อดออก. กรื่ะที่รื่วังสาธารื่ณส ข

Blood Product Transfusion in DHF
• Platelets Transfusion • Indications
• 1. Platelet < 10,000 /mm3
• 2. Platelet < 20,000 /mm3 with significant coagulopathy• 3. Platelet < 50,000 /mm3 prior to invasive procedure• 4. Platelet < 50,000 /mm3 with clinical significant
bleeding i.e. hematemesis, melena, epistaxis not response to local treatment, pulmonary hemorrhage, bleeding from wound, hematoma
สมาคมเวชบ1าบ.ดว�กุฤติแห3งปรีะเทศไทย์Siriraj Med J 2007; 59: 201-5.

Blood Product Transfusion in DHF
• FFP Transfusion • Indications
• 1. Use as colloidal replacement fluid after failure of crystalloid replacement for > 2 hr, dosage not exceed 10 ml/kg/hr (max 40 ml/kg/day)
• 2. Use for correction of coagulopathy: liver coagulopathy, DIC, dosage 10-20 ml/kg/dose q 6-12 hr
• 3. Use for plasmapheresis in hepatic failure• 4. Use in combination with PRC for blood exchange
transfusion or replacement of blood loss
สมาคมเวชบ1าบ.ดว�กุฤติแห3งปรีะเทศไทย์Siriraj Med J 2007; 59: 201-5.

Blood Product Transfusion in DHF
• PRC Transfusion • Indications
• 1. Hct < 35 % during shock stage• 2. Hct declines > 5% in less than 4 hr or > 8% in less than
24 hr (Hct prior to transfusion should not exceed 40%)• 3. Replacement therapy for massive bleeding• 4. Use with FFP for blood exchange transfusion
สมาคมเวชบ1าบ.ดว�กุฤติแห3งปรีะเทศไทย์Siriraj Med J 2007; 59: 201-5.

Coagulations Factors Replacement
• Factor VIIa (Novo seven)• Indications
• 1. Emergency life-threatening bleeding i.e. ICH• 2. Significant uncontrolled bleeding after maximum
platelet (0.4 unit of random donors platelet/kg/day) and maximum FFP transfusion (>40 ml/kg/day)
• 3. Significant life-threatening bleeding and unavailable platelet and/or FFP.
สมาคมเวชบ1าบ.ดว�กุฤติแห3งปรีะเทศไทย์Siriraj Med J 2007; 59: 201-5.

Transfusion Requirement in Children with Dengue Virus Infection
• A-7 yrs retrospective study, 694 children (DF=229, DHF=465)
• Group 1 (n=68) - Risk factors group; morbid obesity, ibuprofen
ingestion, had underlying disease.
• Group 2 (n=626) - patients without risk factors
• The overall transfusion requirement was 7.1% (49/694).
• Patients with risk factors required a higher transfusion rate
(48.5%) compared with patients without risk factors (2.5%)
(P< 0.0001) Ampaiwan Chuansumrit. J Hematol Transf Med 2008;19:43-50.

Transfusion Requirement in Children with Dengue Virus Infection
• Patients with risk factors requiring transfusion varied from DF to
different grades of DHF while those without risk factors requiring
transfusion included only DHF grades III and IV.
• PRC transfusion
Risk factor group: Required TX; median Hct 26.2% (18.3-33.1%)
Not required TX; median Hct 36.3% (31.6-39.7%) (P< 0.0001)
No risk factors group + required TX: median Hct 35.8%
(28.2-40.3%) (P = 0.005)Ampaiwan Chuansumrit. J Hematol Transf Med 2008;19:43-50.

Transfusion Requirement in Children with Dengue Virus Infection
• The platelet counts of both groups were similar ranging from
20,000 to 60,000/mL.
• The ratio of crossmatch to transfusion of platelet concentrate
among both groups was similar at 1:1.
• Requirement of rFVIIa; overall 2.4% (17/694)
Risk factors group (14): No risk factors group (3) (P < 0.0001)
Ampaiwan Chuansumrit. J Hematol Transf Med 2008;19:43-50.

• Evaluate the efficacy and safety of (rFVIIa) in children with DHF gr II /
III, Placebo (n=9) and rFVIIa (n=16)
• The efficacy (response to treatment at 2 h):
Complated: rFVIIa 75.0% VS placebo 44.4%
Partial: rFVIIa 18.7% VS placebo 11.2%
Ineffective: rFVIIa 6.3% VS placebo 44.4%
Blood Coagulation and Fibrinolysis 2005, 16:549–55.

• The subsequent efficacy of bleeding control at 6, 12 and 24 h :
comparable between the two groups
• The cumulative use of red blood cells (rFVIIa 31.3% VS placebo 33.3%)
and plasma (rFVIIa 25% VS placebo 22%) during the 24-h period
• Platelet concentrate requirement (rFVIIa group 6.3% VS placebo
(33.3%)
• Conclusion rFVIIa appears to be a useful adjunctive Rx. to blood
component transfusion for controlling active bleeding in children with
DHF especially when platelet concentrate is not readily available
Blood Coagulation and Fibrinolysis 2005, 16:549–55.

กุารีด"แลรีะย์ะพ.กุฟื้0� นี ข้'อแนีะนี1าเม�#อผู้"'ป(วย์กุล.บบ'านี• หล กุเล #ย์งกุารีกุรีะทบกุรีะแทกุอย์3างรี�นีแรีง - 35 ว.นี
(1 ส.ปดาห� ) หล.งจากุหาย์ป(วย์
• เม�#อผู้"'ป(วย์ม อากุารีปกุติ� สามารีถ้ไปโรีงเรี ย์นีได'ติามปกุติ�
• ถ้'าคนีในีบ'านีม ไข้'ส"ง แนีะนี1ามาพบแพทย์�
• แนีะนี1าให'กุ1าจ.ดแหล3งเพาะพ.นีธ��ย์�งลาย์ม #บ'านีและช�มชนี
แนีวทางกุารีด"แลผู้"'ป(วย์ไข้'เล�อดออกุ รีพ.สรีรีพส�ทธ�ปรีะสงค� อ�บลรีาชธานี : update June 2011

กุารีควบค�มและกุ1าจ.ดล"กุนี1�าย์�งลาย์

“Dengue is one disease entity with different clinical presentations and
often with unpredictable clinical evolution and outcome”