Abshari Ainisabila
LAPORAN PAGIAbshari Ainisabila10/304664/KU/14083IDENTITAS Nama:
Tn. LTTL: 03/05/1942Alamat: Moyudan, Sleman, YogyakartaNo. RM:
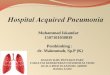
01013xxxTanggal Hasil : 04/03/2015Keterangan Klinis : CAP cr IV,
CHF cf IIProyeksi APPosisi SemierectTampak konsolidasi semiopak
inhomogen di paracardial dextra, batas tidak tegas, air bronchogram
(+)Tampak corakan bronchovascular meningkat dan mengabur, hilar
haze (+), batwing appearence (-), cotton wool appearence (-)Tak
tampak pemadatan limfonodi hilus bilateralTak tampak pelebaran
pleural space bilateralTampak diafragma bilateral licin dan tak
mendatarCor, CTR= 0,68, tampak arcus aorta prominentSistema tulang
yang tervisualisasi intak
Kesan Edema pulmo disertai pneumonia dextraCardiomegali dengan
elongation aortaTEORIPULMONARY EDEMAEdema pulmo/wet lung ialah
akumulasi cairan di extravaskular jaringan paru karena perubahan
tekanan hidrostatik kapiler atau peningkatan permeabilitas.
Ditandai dengan dyspneu, frothy pink expectoran serous fluid,
cyanosis
ETIOLOGYCardiogeniktekanan hidrostatikeg. LHF aritmia, fluid
overload (kidney failure)
NonCardiogenikperubahan permeability membran kapiler atau
tekanan onkotik plasma
PATOFISIOLOGI Imbalance Starlings ForcePeningkatan tekanan
kapiler paru eg. Stenosis mitr al, LHFPenurunan tekanan onkotik
plasma eg. hipoalbuminPeningkatan tekanan negatif interstitial eg.
Asma bronkialKerusakan alveolar-capillary barrierObstruksi
limpatikIdiopathik GAMBARAN RADIOLOGICardiogenikKerley B lines
(septal lines)Seen at the lung bases, usually no more than 1 mm
thick and 1 cm long, tegak lurus terhadap permukaan pleuraPleural
effusionsUsually bilateral, frequently the right side being larger
than the leftIf unilateral, more often on the rightFluid in the
fissuresThickening of the major or minor fissurePeribronchial
cuffingVisualization of small doughnut-shaped rings representing
fluid in thickened bronchial wallsThe heart may or may not be
enlargedWhen the fluid enters the alveoli themselves, the airspace
disease is typically diffuse, and there are no air bronchograms
CTRBatwing appearencePeri-bronchial thickeningKerley B
linesSepalisasi
Perihilar distributionAlveolar infiltrate
Collectively, the above four findings comprisepulmonary
interstitial edema
11
Stage 1 RedistributionRedistribution/cephalisation
Artery-to-bronchus ratioNormally the vessels in the upper lobes
are smaller than the accompanying bronchus with a ratio of 0.85
(3).At the level of the hilum they are equal and in the lower lobes
the arteries are larger with a ratio of 1.35.When there is
redistribution of pulmonary blood flow there will be an increased
artery-to-bronchus ratio in the upper and middle lobes.This is best
visible in the perihilar region.On the left a patient with
cardiomegaly and redistribution.The upper lobe vessels have a
diameter > 3 mm (normal 1-2 mm).Notice the increased
artery-to-bronchus ratio at hilar level (arrows).
14Stage 2 Interstitial EdemaCHF fluid leakage into the
interlobular and peribronchial interstitium pressure in the
capillaries & Kerley B lines
Kerley B line/septal line are due to fluid leakage into
peripheral interlobular septa1-2cm horizontal line near
costophrenic angle. Tegak lurus dengan pleuraSpesifik untuk edema
pulmo terutama yang cardiogenik
Ketika cairan keluar ke peribronchovascular interstitium akan
terlihat sebagai penebalan dinding bronchus (peribronchial cuffing)
Gambaran vasa kabur (perihilar haze) karena di kelilingi oleh
edema
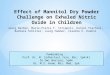
Stage 3 Alveolar Edema/Cotton Wool AppearenceFluid leakage tidak
bisa dikompensasi oleh drainase limfatik sehingga cairan leakage ke
alveolar (alveolar edema) dan ke pleural space (efusi pleura)Panah
Biru: efusi pleuraPanah Kuning: edema alveolar dengan konsolidasi
perihilar consolidations dan air bronchogramsPanah Merah: pelebaran
vascular pedicleKepala Panah: enlarged cardiac silhouette
Filling alveolar space w/ exudate
Hazines mulai dari hilus = butterfly appearenceSevere =
patcy/cotton wool appearence18GAMBARAN RADIOLOGINon-cardiogenic
pulmonary edemaBilateral, peripheral air space disease with air
bronchograms or central bat-wing patternKerley B lines and pleural
effusions are uncommonTypically occurs 48 hours or more after the
initial insultStabilizes at around five days and may take weeks to
completely clear
Batwing/butterfly appearenceGambaran opasitas yang menunjukkan
pattern of perihilar shadowing
TERAPICardiogenic pulmonary edemaOxygenDiureticsLasix,
etc.NitratesNitroglycerin, etc.Natriuretic peptidesNesiritide,
etc.MorphineInotropic agentsDopamine, dobutamine, digoxin,
etc.Angiotensin converting enzyme (ACE)
inhibitorsBeta-blockersCarvedilol, etc.
Non-cardiogenic pulmonary edemaTreatment is supportiveVentilator
management.Antibiotic therapy, when necessaryCorticosteroids
ELONGASIO AORTAMenilai Elongasio Aorta
< 30 tahun : tidak dapat menilai elongasio aorta karena
jantung masih turun> 30 tahunjarak bagian bawah clavicula dengan
arcus aorta normal = 1-2cm.elongasio aorta jika jarak < 1cm>
50 tahun- ambil garis tengah thorax- ukur lengkung aorta terjauh
dengan garis tengah thorax- elongasio aorta = > 4cm
TERIMAKASIH