Embed Size (px)
Citation preview
Emergency Ultrasound (EUS)教學(8)
急診超音波在深部靜脈栓塞之應用
新光醫院急診醫學科
陳國智醫師
中華民國醫用超音波學會指導醫師
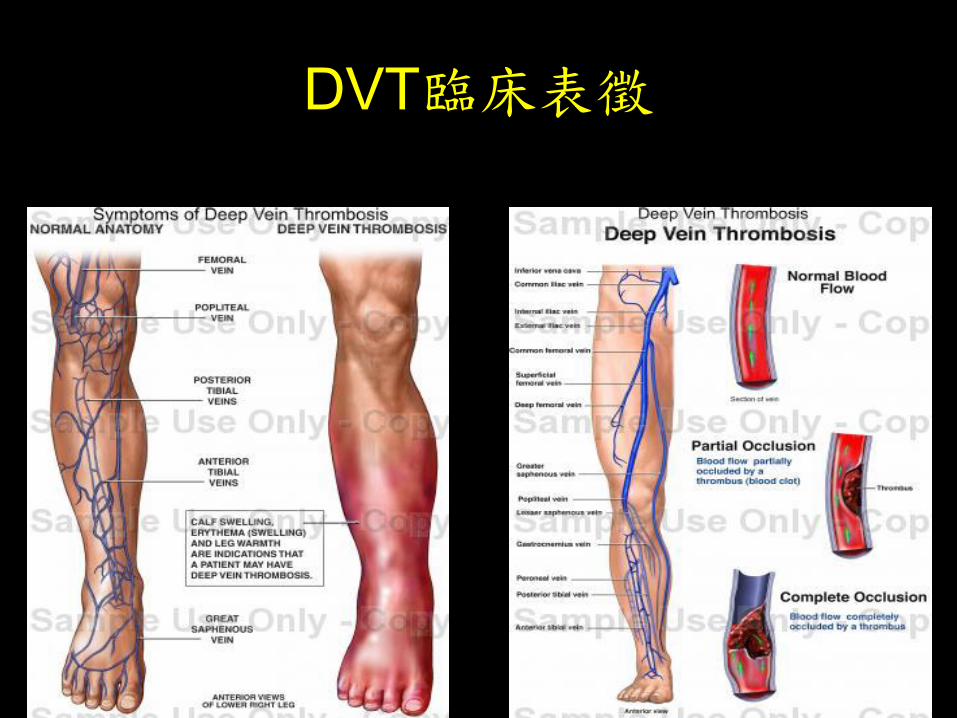
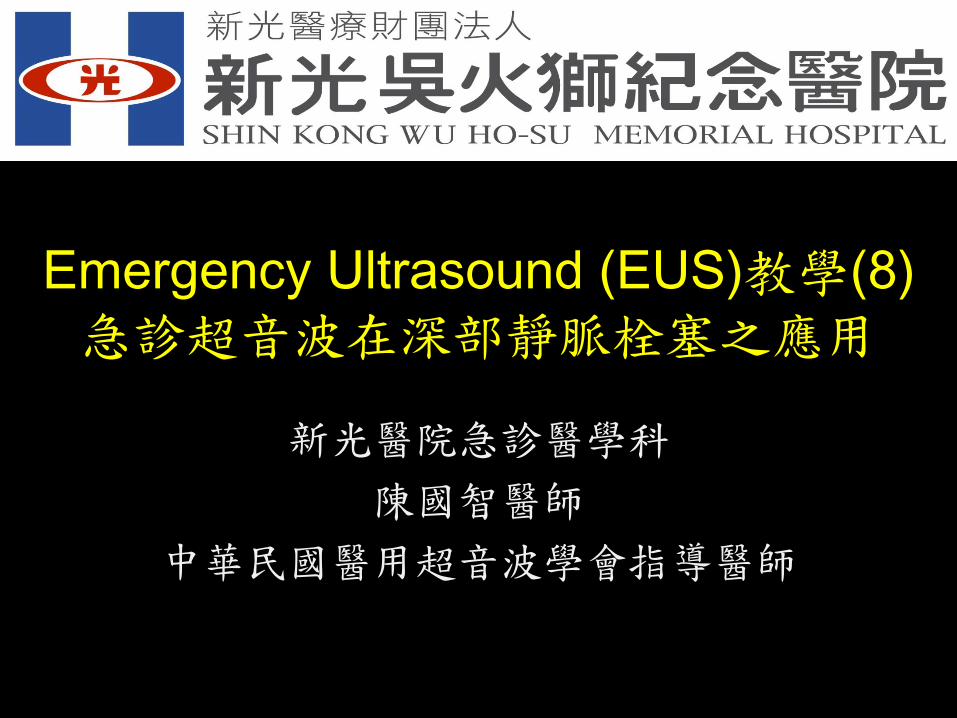
DVT臨床表徵
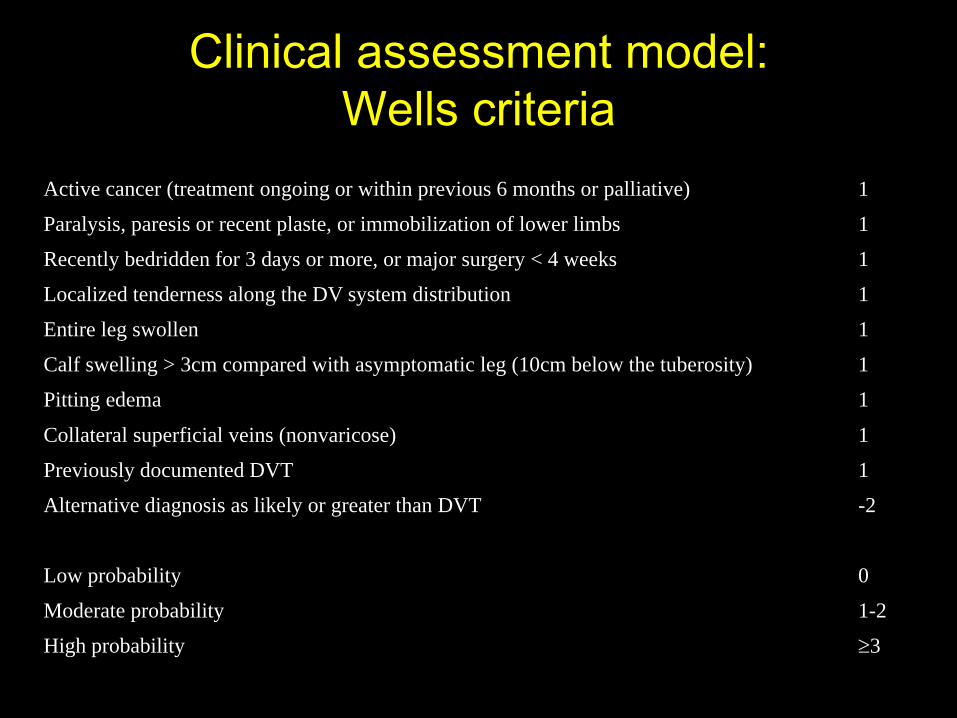
Clinical assessment model:
Wells criteria
Active cancer (treatment ongoing or within previous 6 months or palliative) 1
Paralysis, paresis or recent plaste, or immobilization of lower limbs 1
Recently bedridden for 3 days or more, or major surgery < 4 weeks 1
Localized tenderness along the DV system distribution 1
Entire leg swollen 1
Calf swelling > 3cm compared with asymptomatic leg (10cm below the tuberosity) 1
Pitting edema 1
Collateral superficial veins (nonvaricose) 1
Previously documented DVT 1
Alternative diagnosis as likely or greater than DVT -2
Low probability 0
Moderate probability 1-2
High probability 3
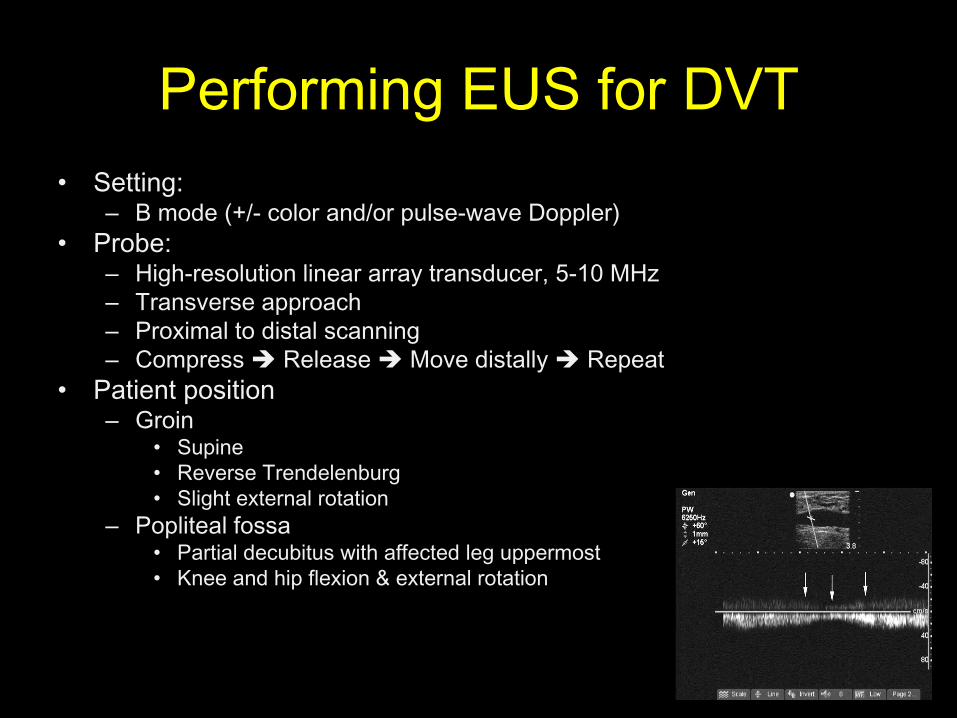
Performing EUS for DVT
• Setting:– B mode (+/- color and/or pulse-wave Doppler)
• Probe:– High-resolution linear array transducer, 5-10 MHz
– Transverse approach
– Proximal to distal scanning
– Compress Release Move distally Repeat
• Patient position– Groin
• Supine
• Reverse Trendelenburg
• Slight external rotation
– Popliteal fossa• Partial decubitus with affected leg uppermost
• Knee and hip flexion & external rotation
EUS for DVT
• Non-compression of the vessel
– Inability to completely compress the vessels
– With proper pressure
– After ensuring good position
• FYI:
– Only complete compression r/o DVT
– Only the lack of total compression means DVT
EUS for DVT
• Compression US
– Sensitivity and specificity: 98-100% for
proximal DVT
– Time saving: formal 37 min v.s. limited 3.5
min
– Round-the-clock access
Landmark for DVT Scan
• Mid-point of inguinal ligment– Vessels: CFV & CFA
– Until CFV splits into DFV & SFV (Mid-thigh)
• Popliteal fossa– Vessels: PV & PA
– The last 2 cm of PV and end just distal to the trifurcation
– “ the vein comes to the top in the pop”
• Contralateral leg scanning– Optional
• Documentation– Dual-image feature: w/ & w/o compression
EUS for DVT survey
• Primary component
– Visualize the venous structures
– Detect gray-scale compressibility
– Lack of compressibility DVT
• Secondary component
– Use of Doppler to evaluate for abnormal flow
No complete compression
1. Presence of a clot
2. Inadequate pressure on the
transducer
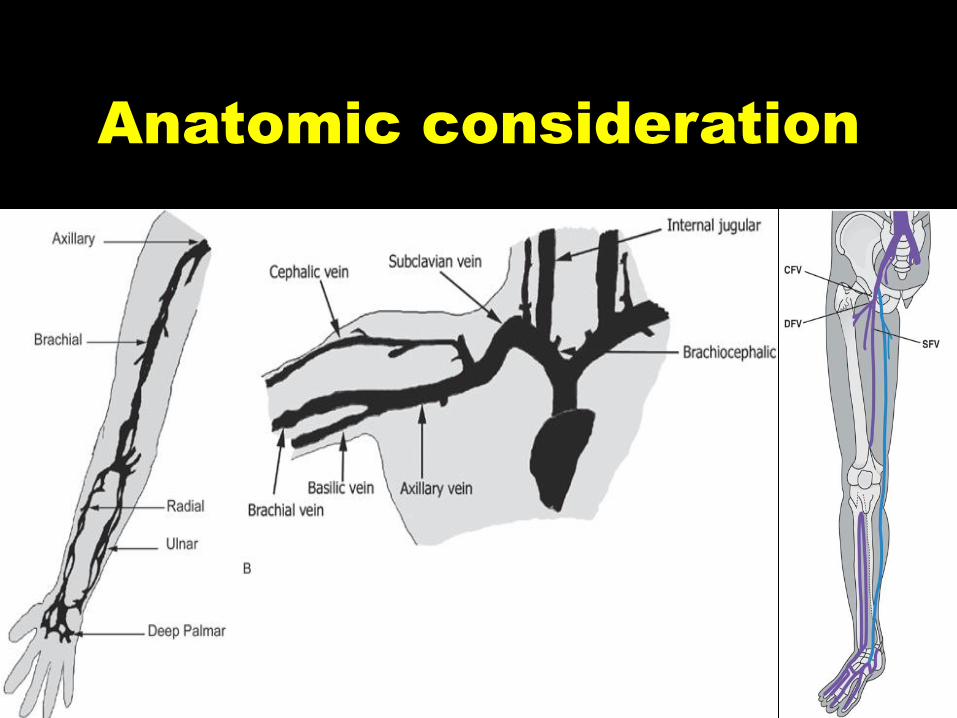
Anatomic consideration
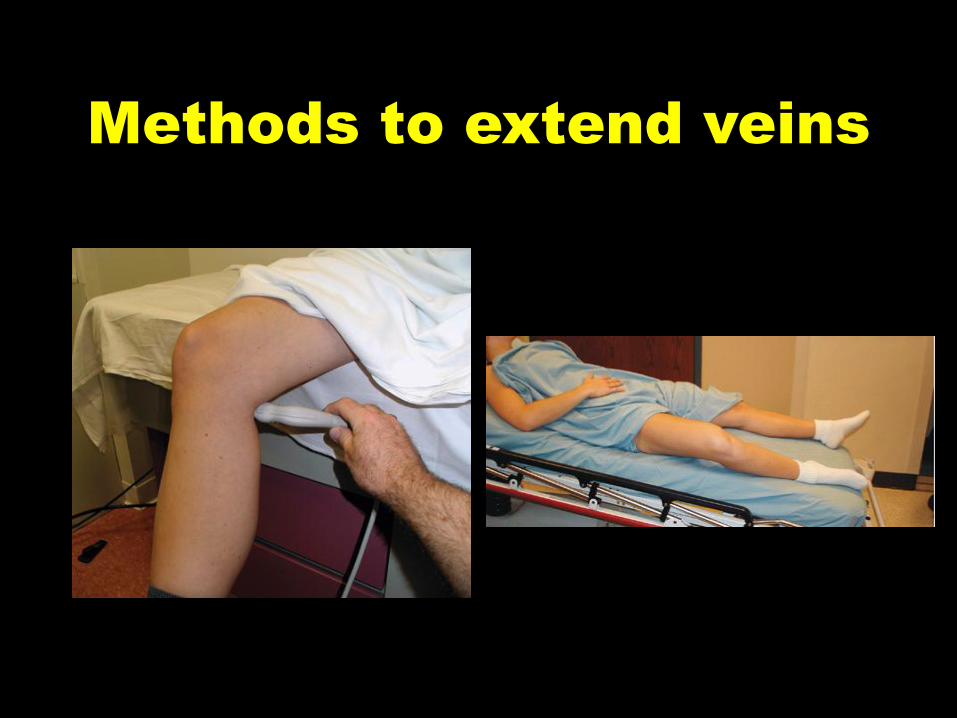
Methods to extend veins

Ideal transducer
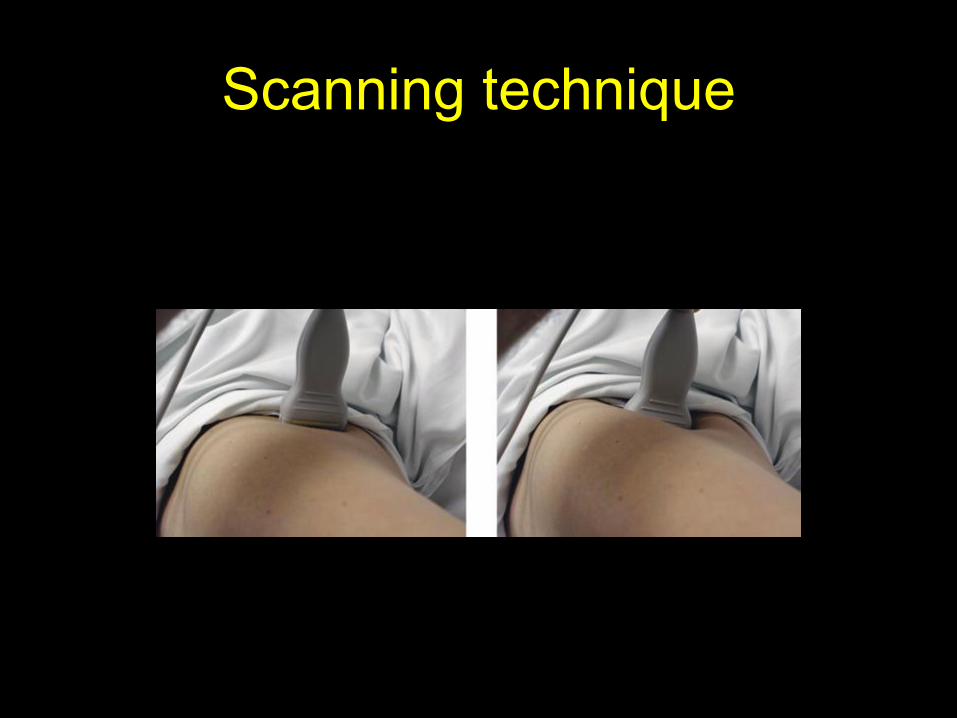
Scanning technique
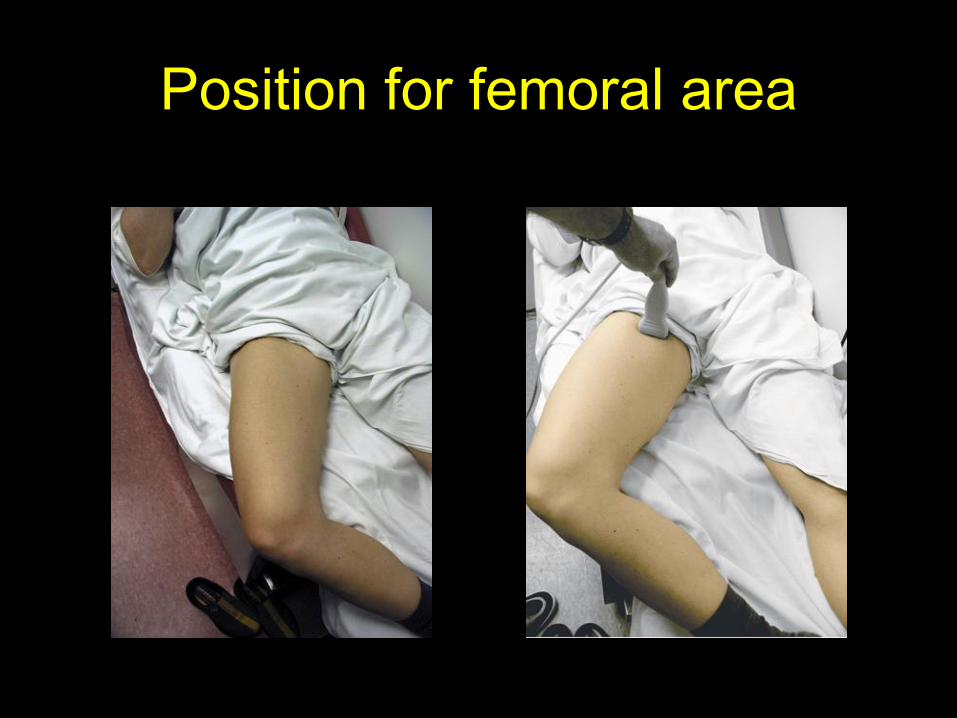
Position for femoral area
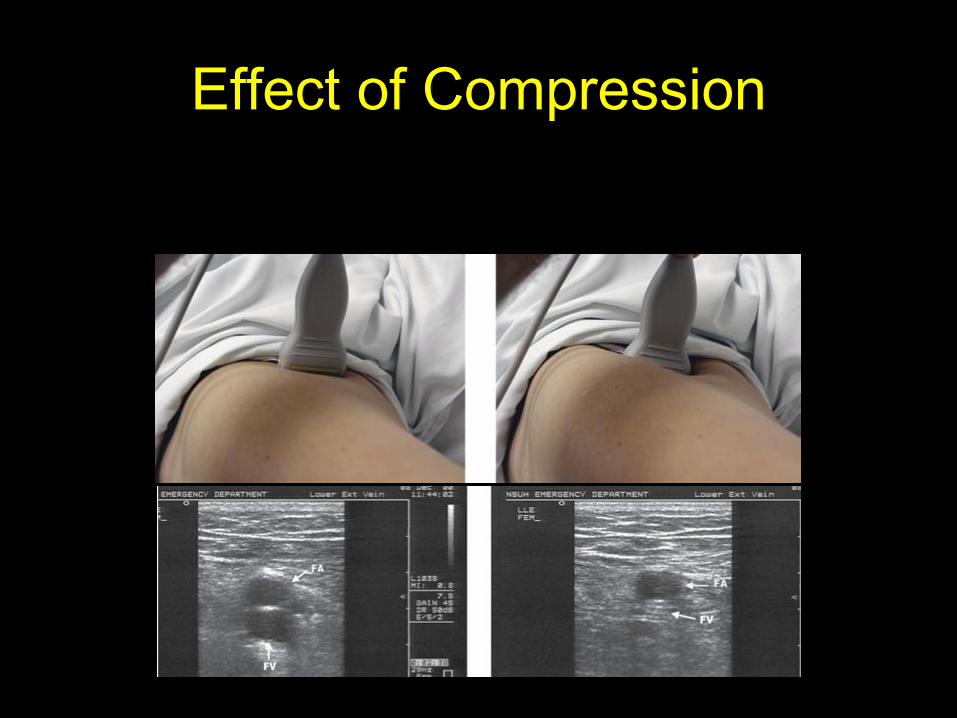
Effect of Compression
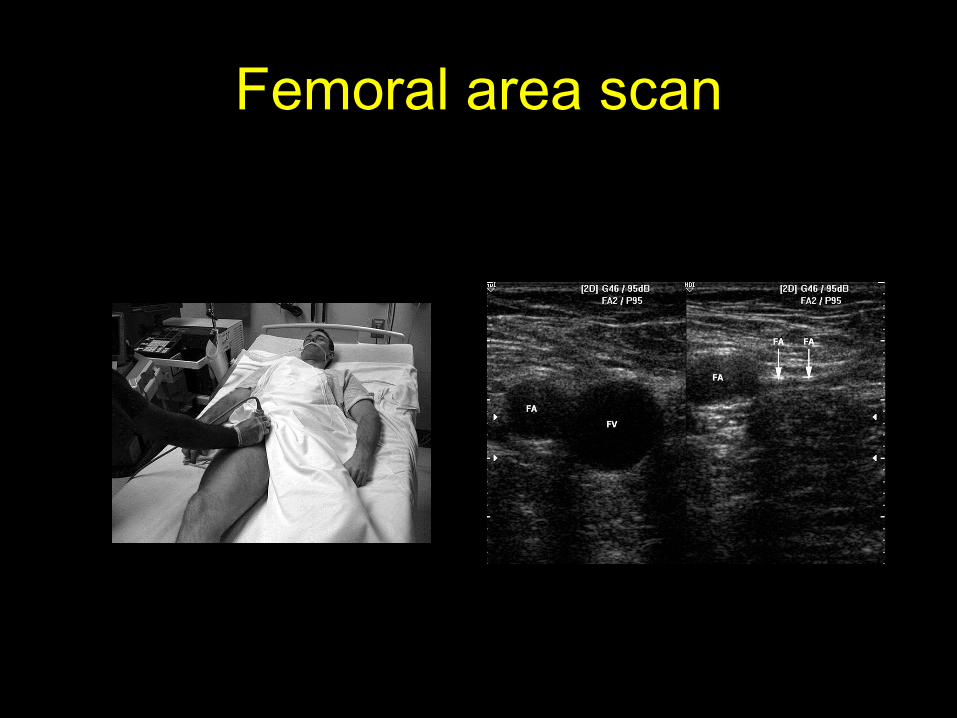
Femoral area scan
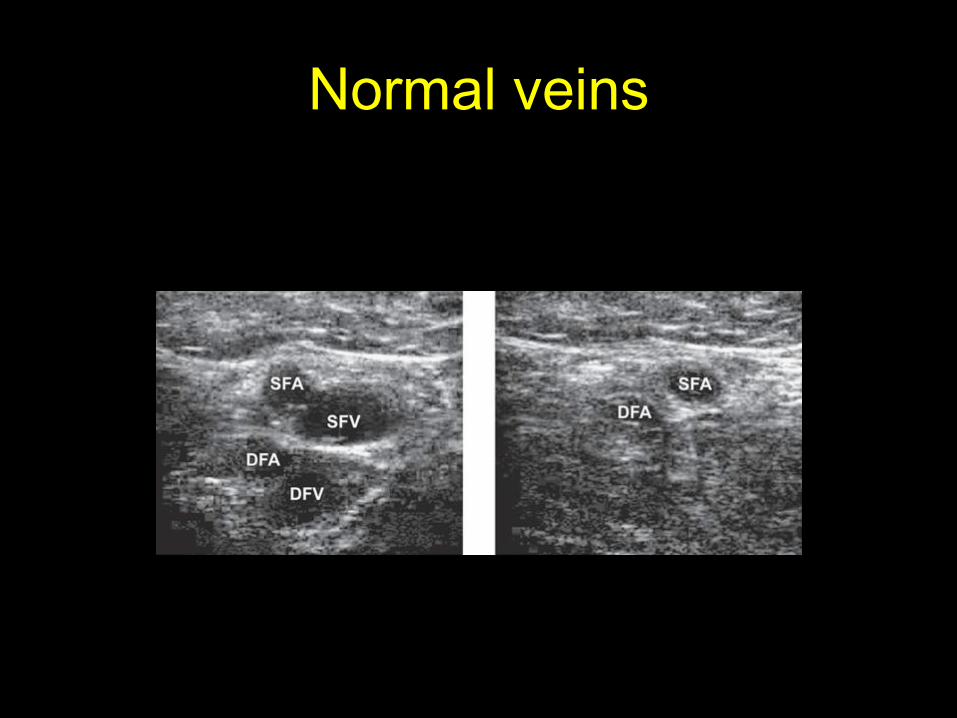
Normal veins
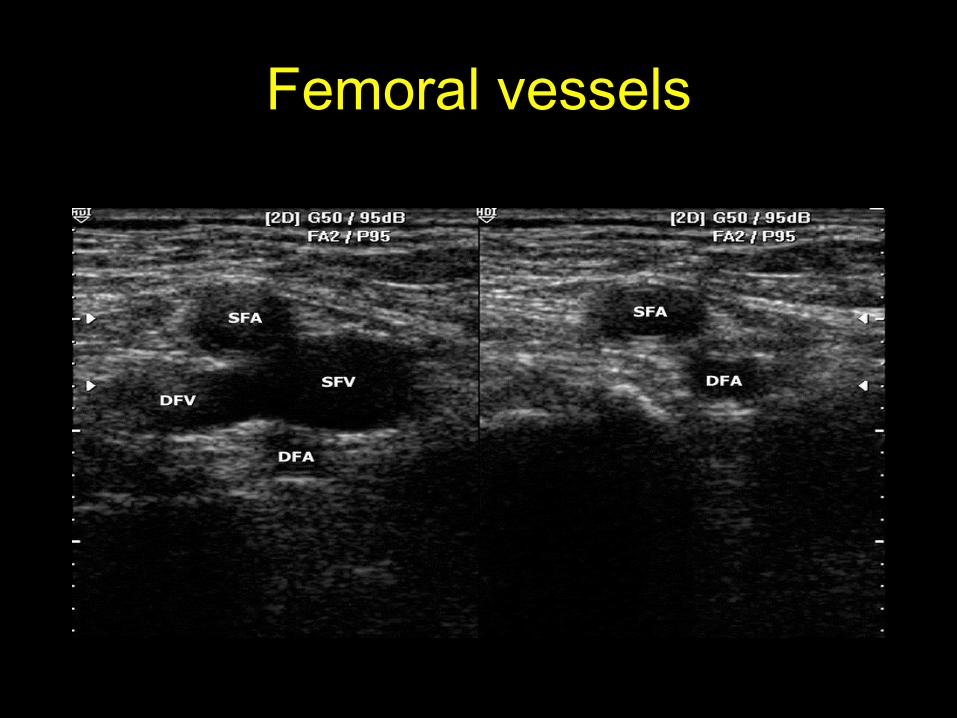
Femoral vessels
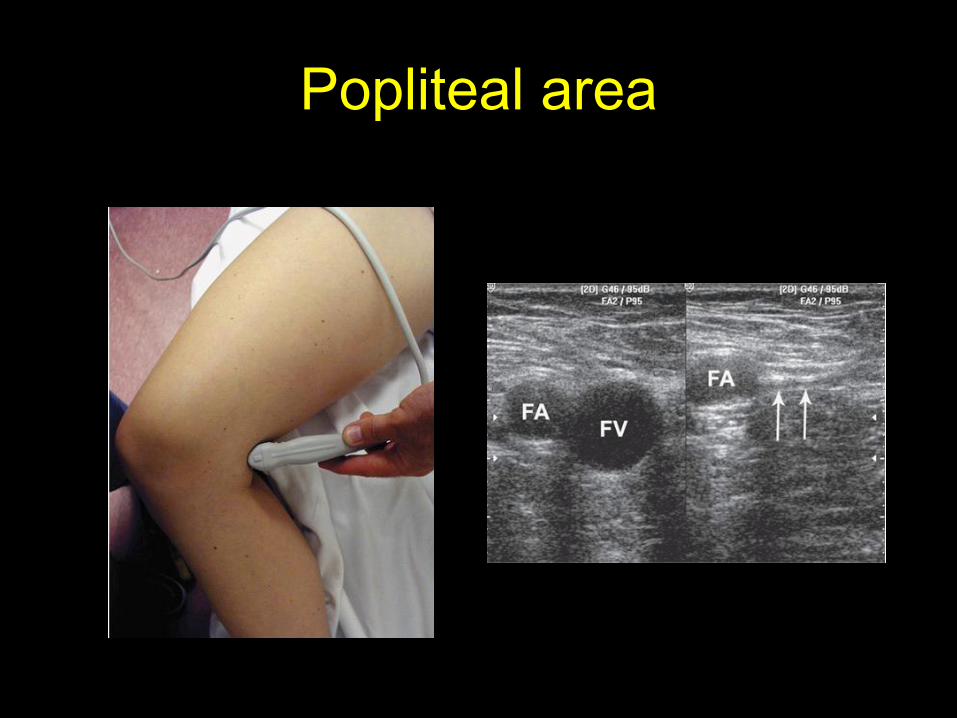
Popliteal area
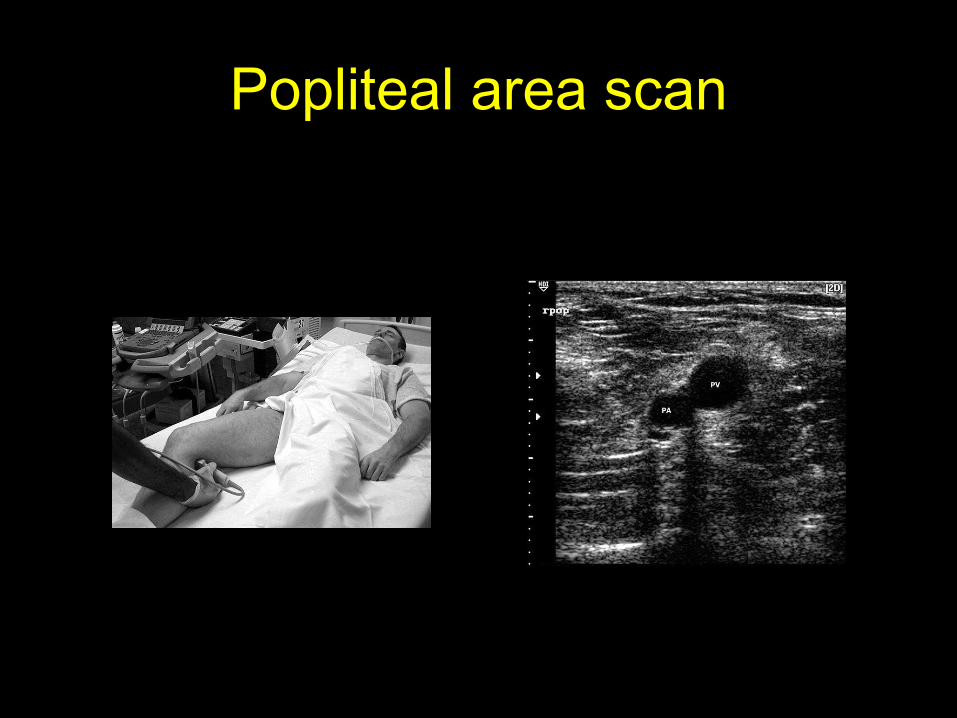
Popliteal area scan
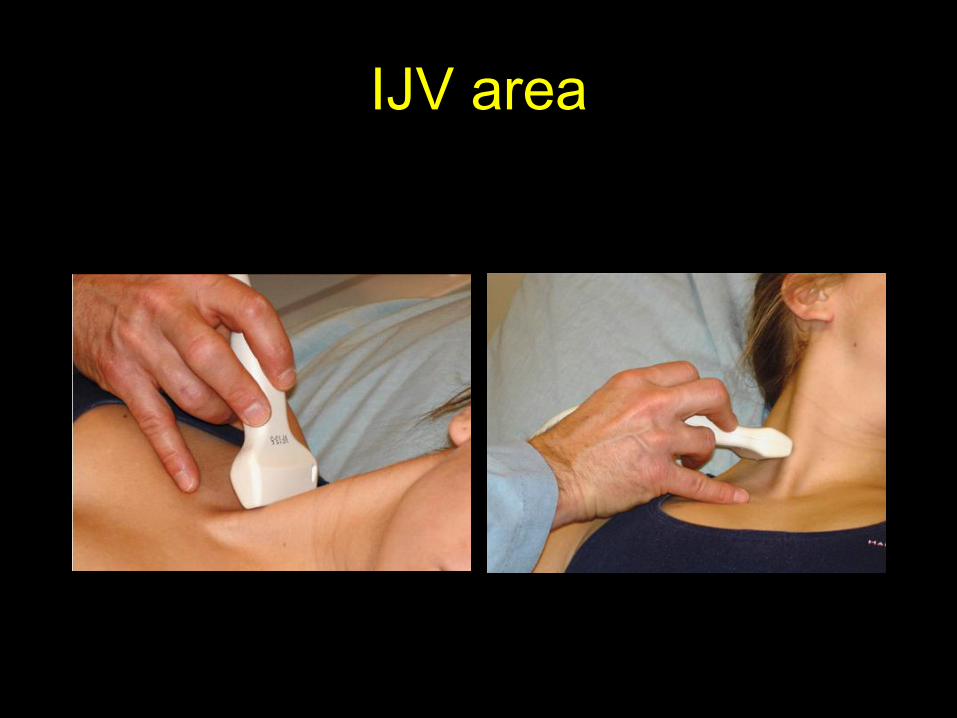
IJV area
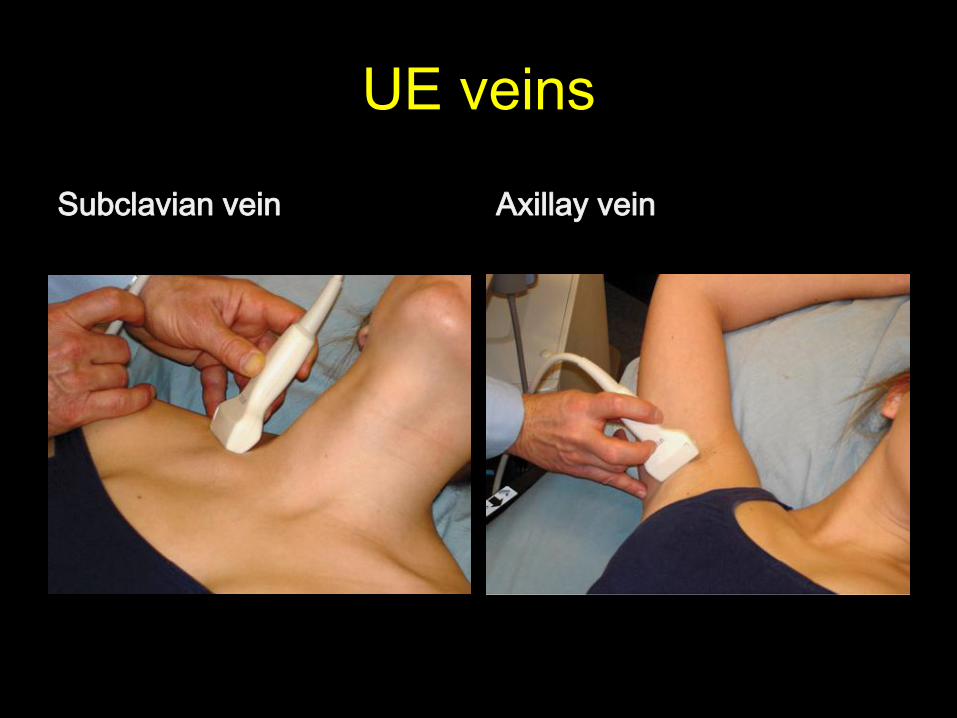
UE veins
Subclavian vein Axillay vein
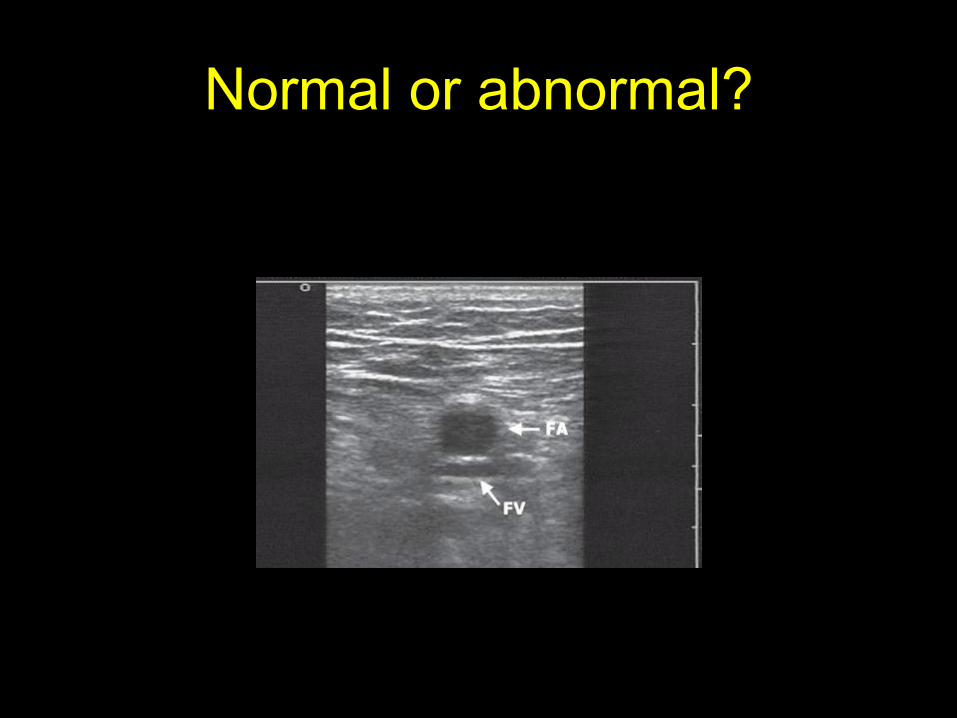
Normal or abnormal?
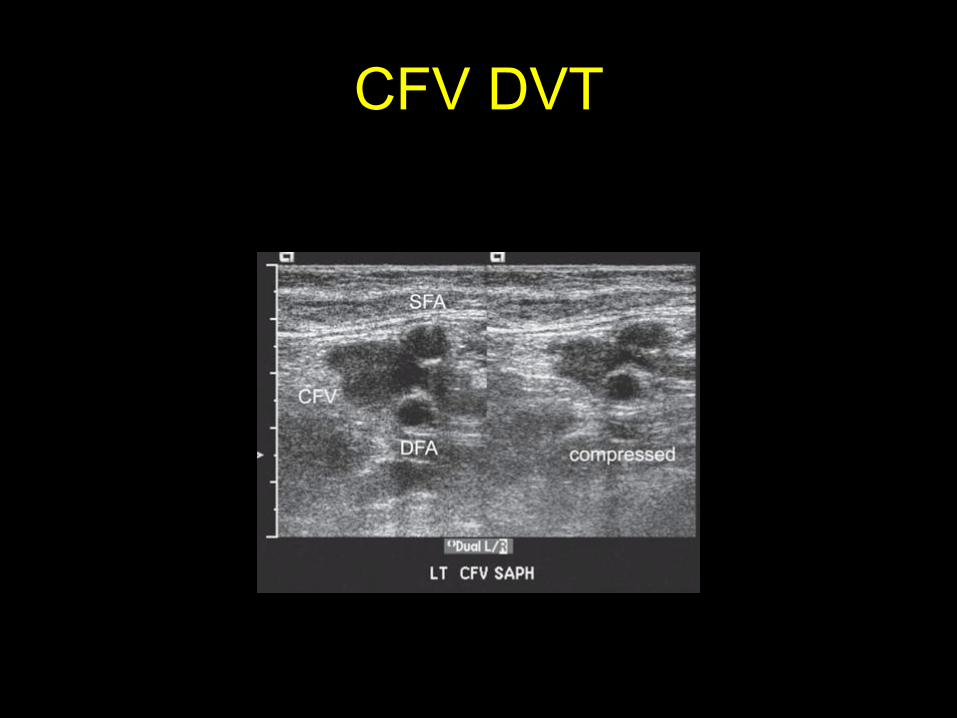
CFV DVT
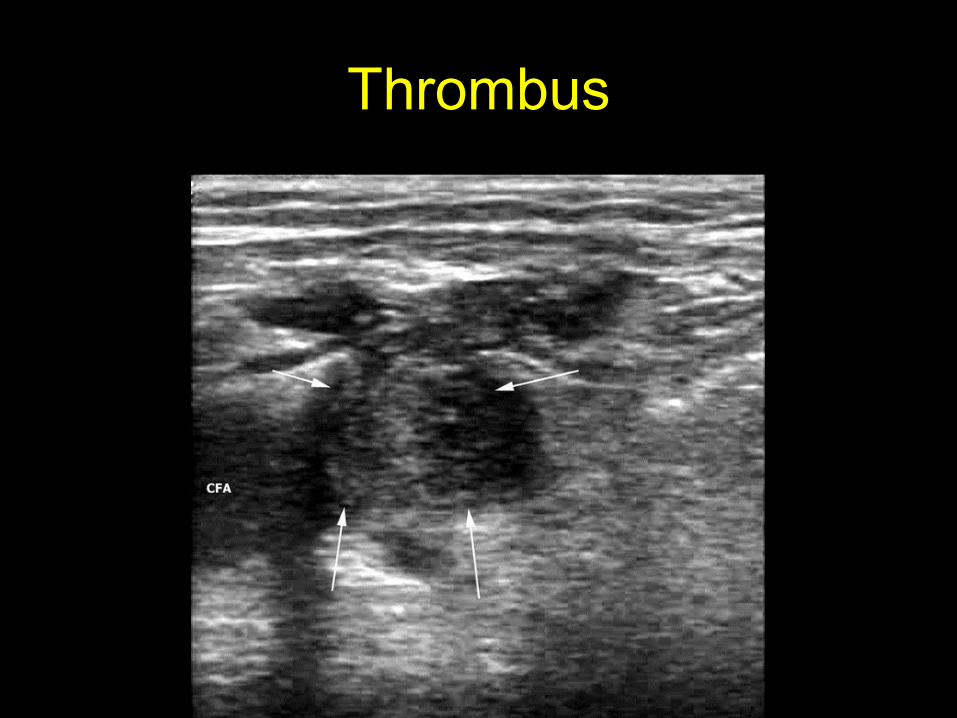
Thrombus
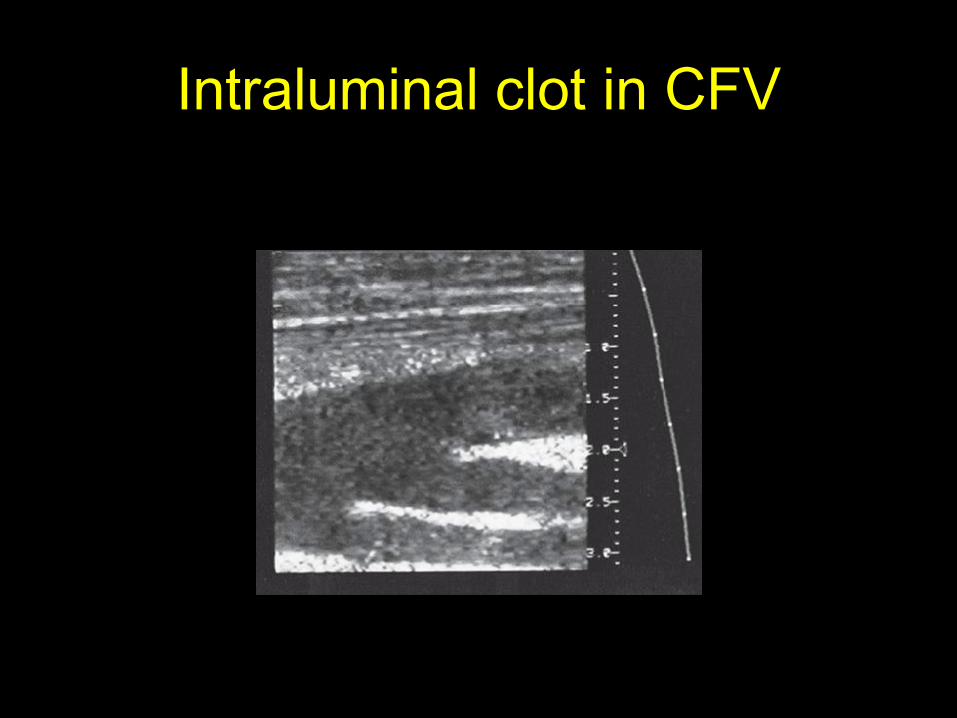
Intraluminal clot in CFV
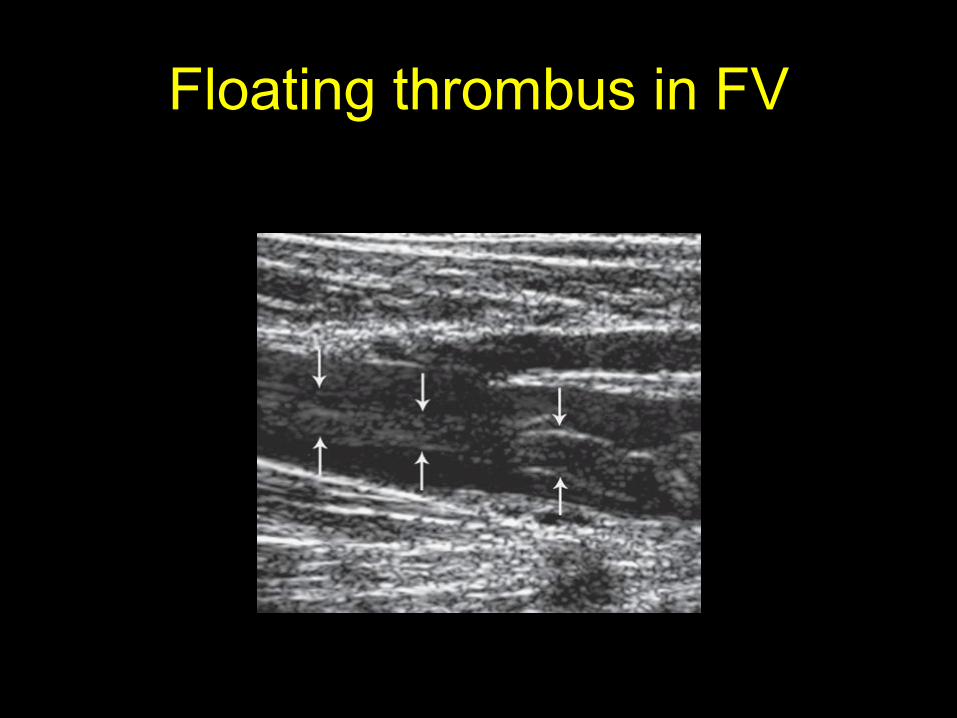
Floating thrombus in FV
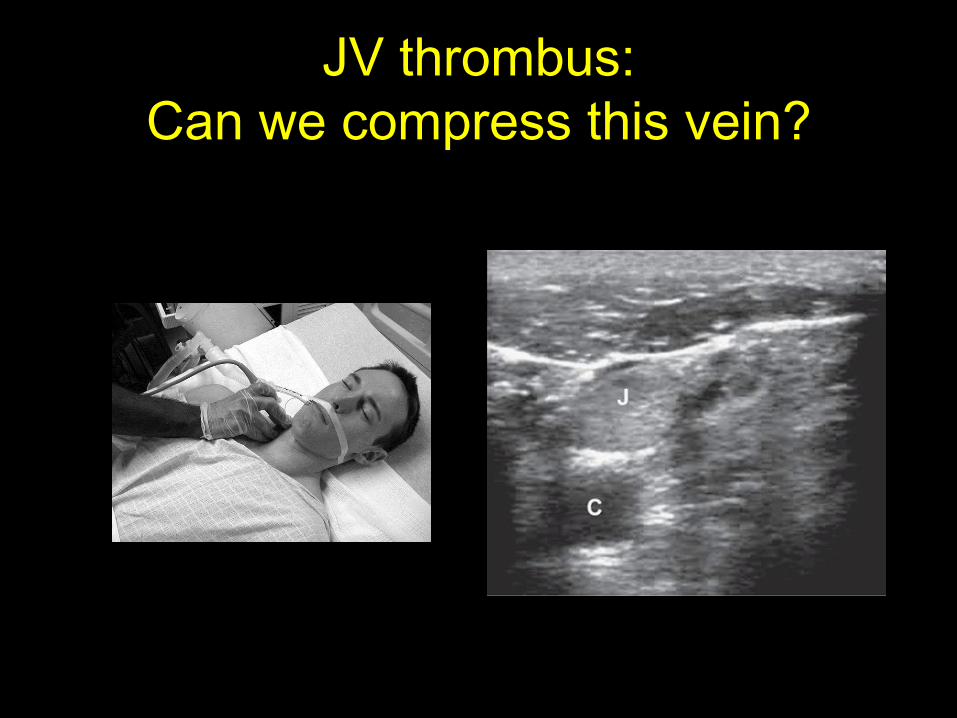
JV thrombus:
Can we compress this vein?
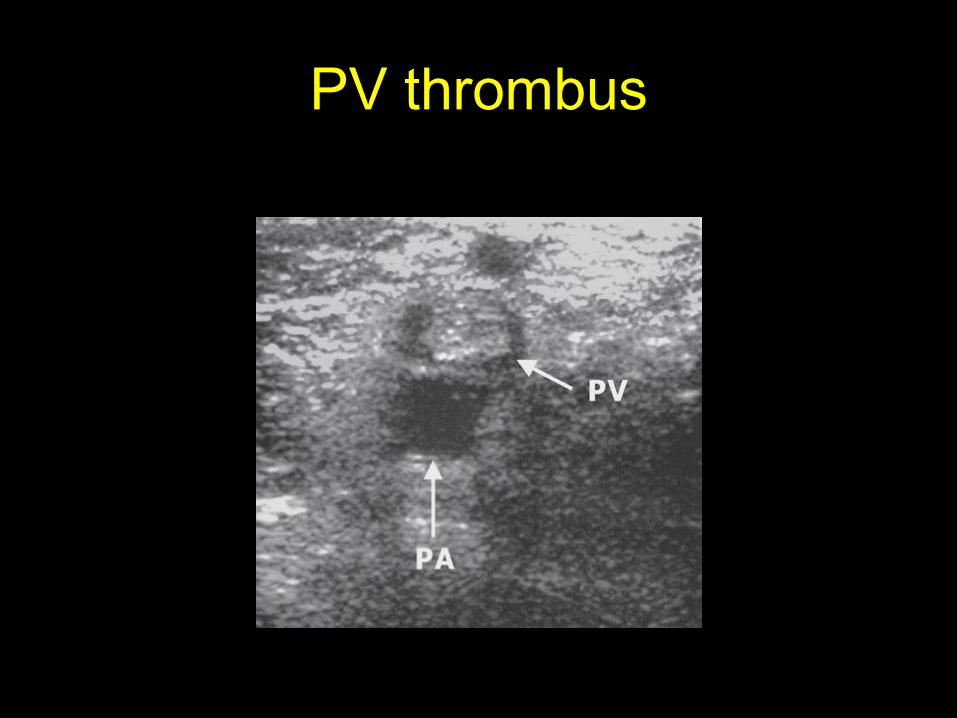
PV thrombus
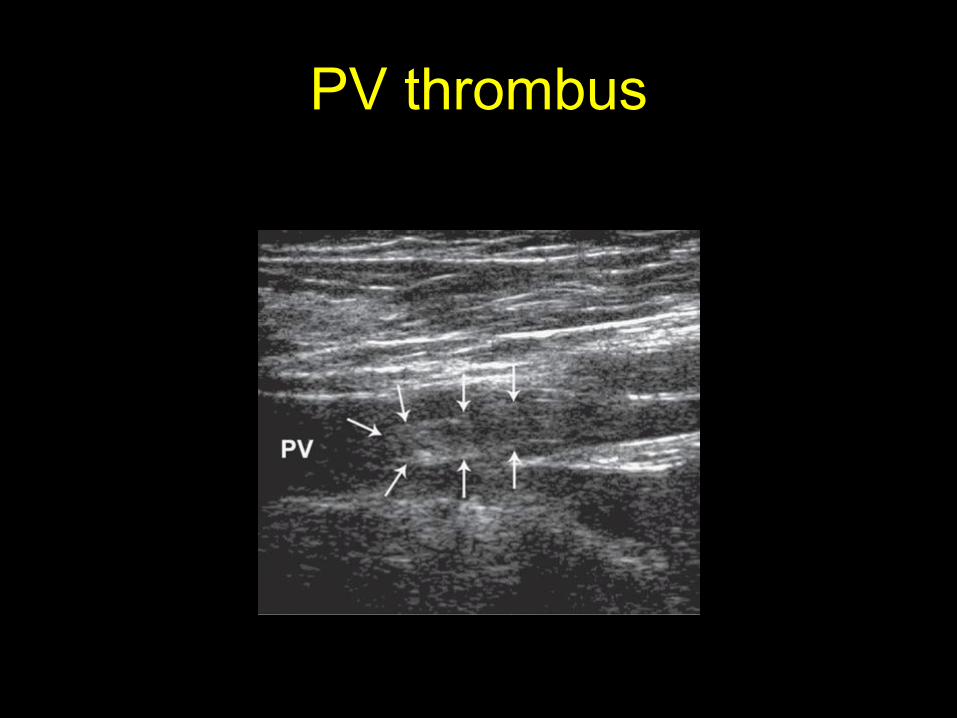
PV thrombus
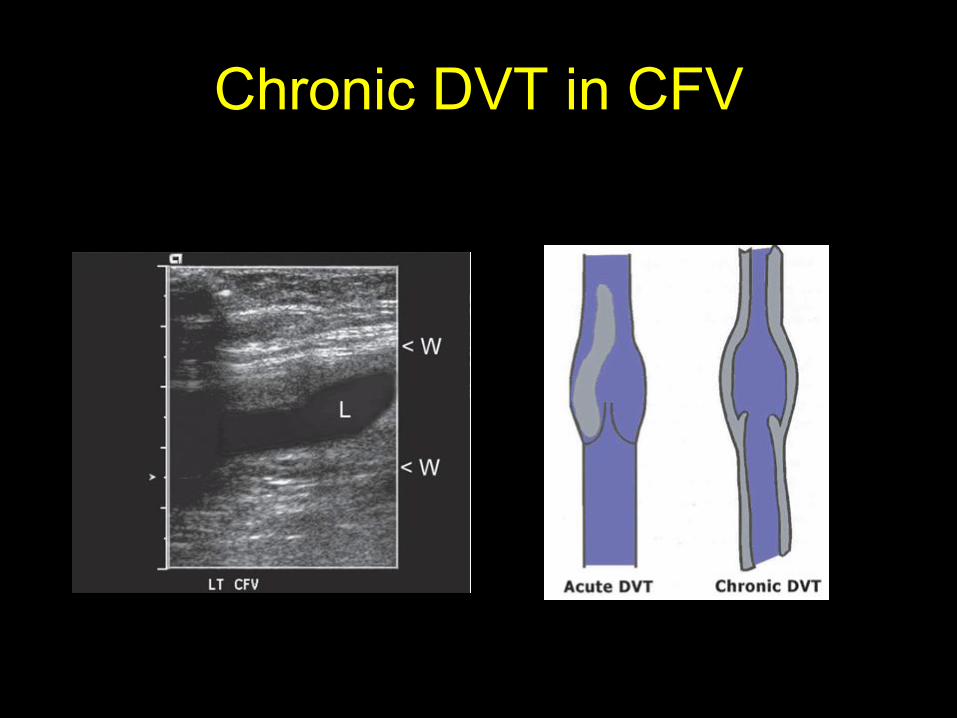
Chronic DVT in CFV
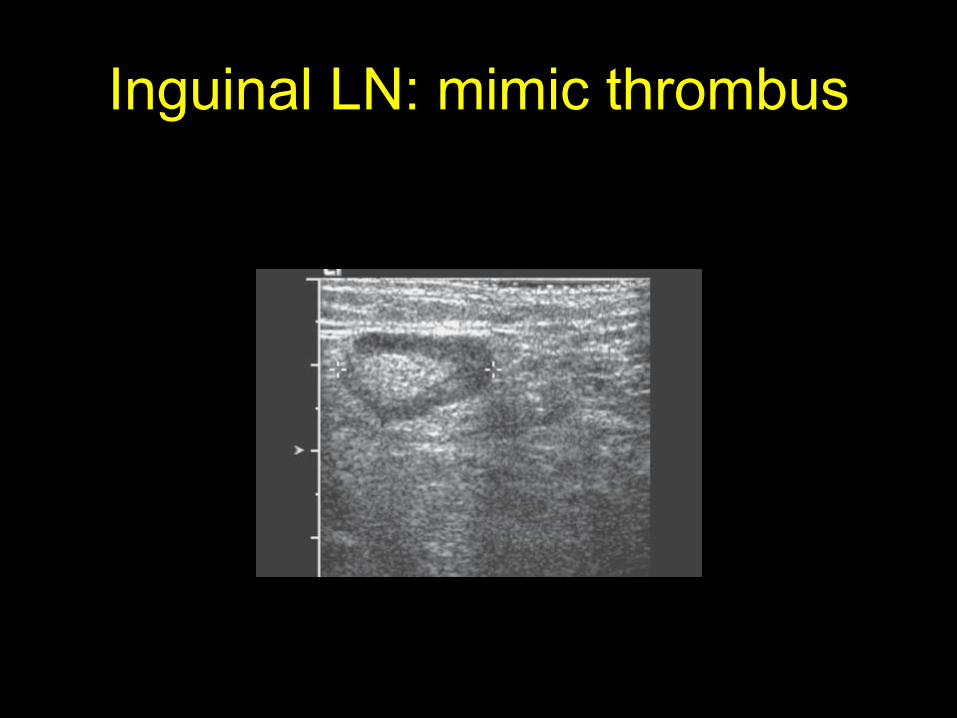
Inguinal LN: mimic thrombus
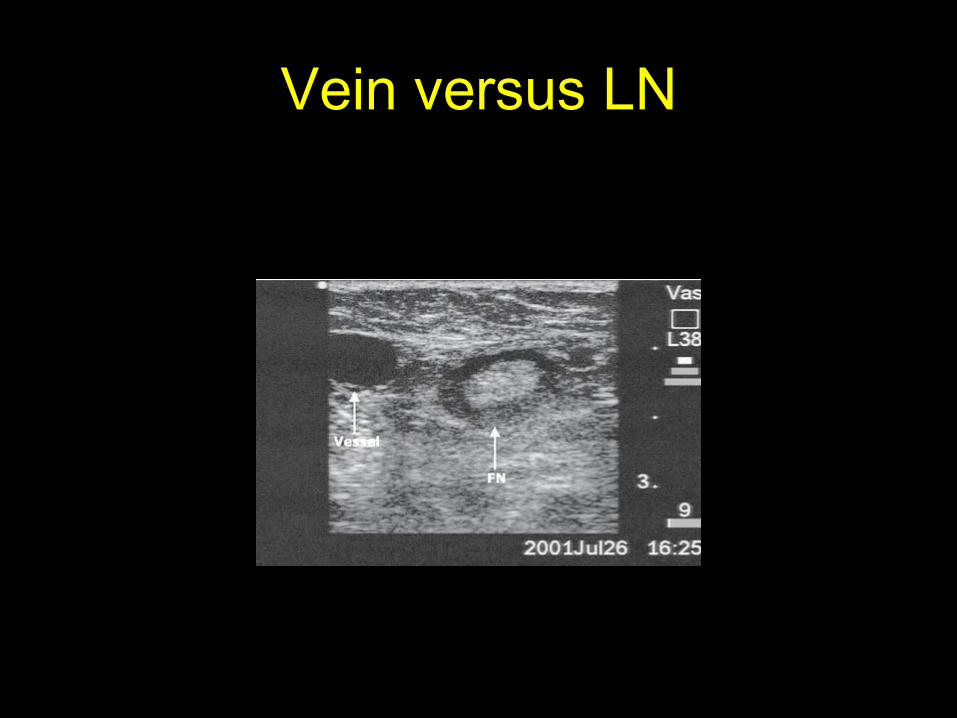
Vein versus LN
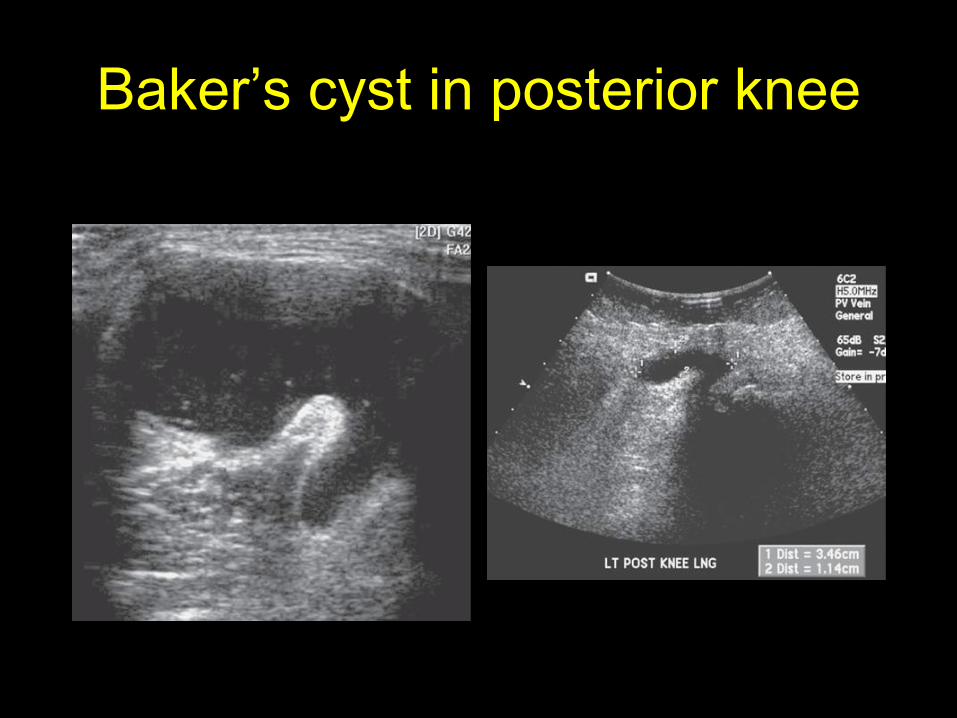
Baker’s cyst in posterior knee
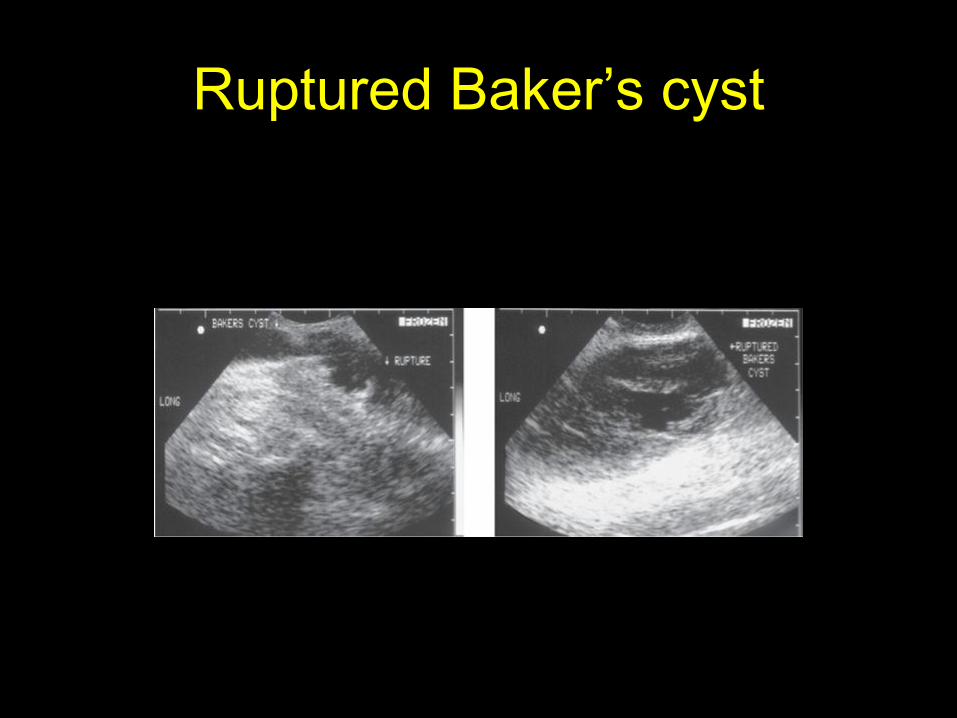
Ruptured Baker’s cyst
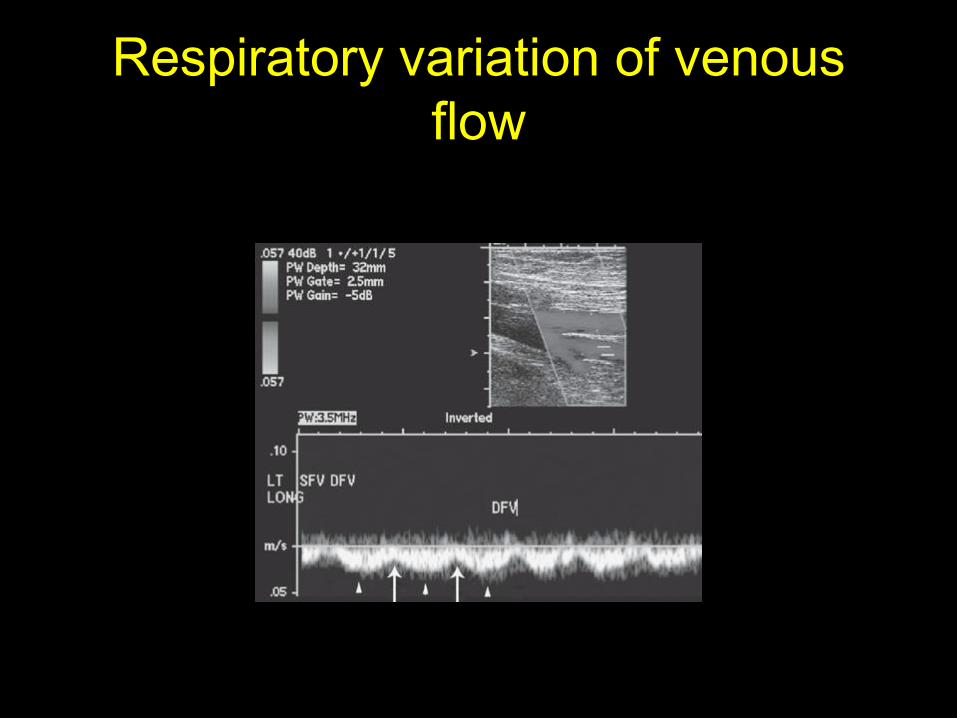
Respiratory variation of venous
flow
Pitfalls
• Contraindication
• Imaging challenging subjects
• Segmental DVT
• Misunderstanding the limitations of ultrasonography
• Mistaking artery for vein
• Femoral lymph nodes mistaken for a DVT
• Pelvic vein thrombosis
• Slow venous blood flow
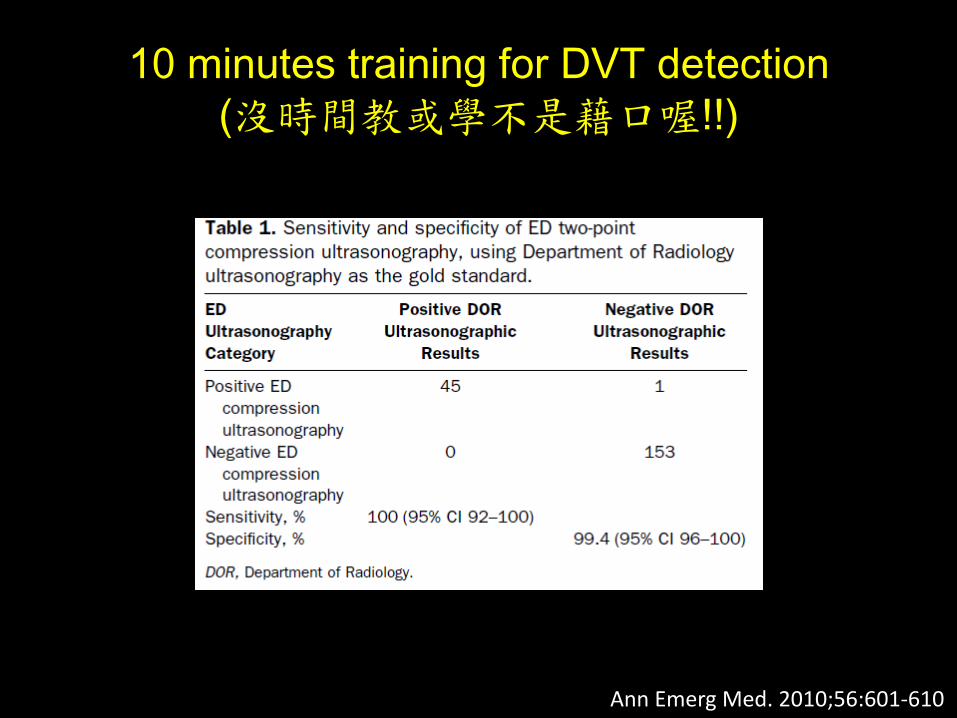
10 minutes training for DVT detection
(沒時間教或學不是藉口喔!!)
Ann Emerg Med. 2010;56:601-610
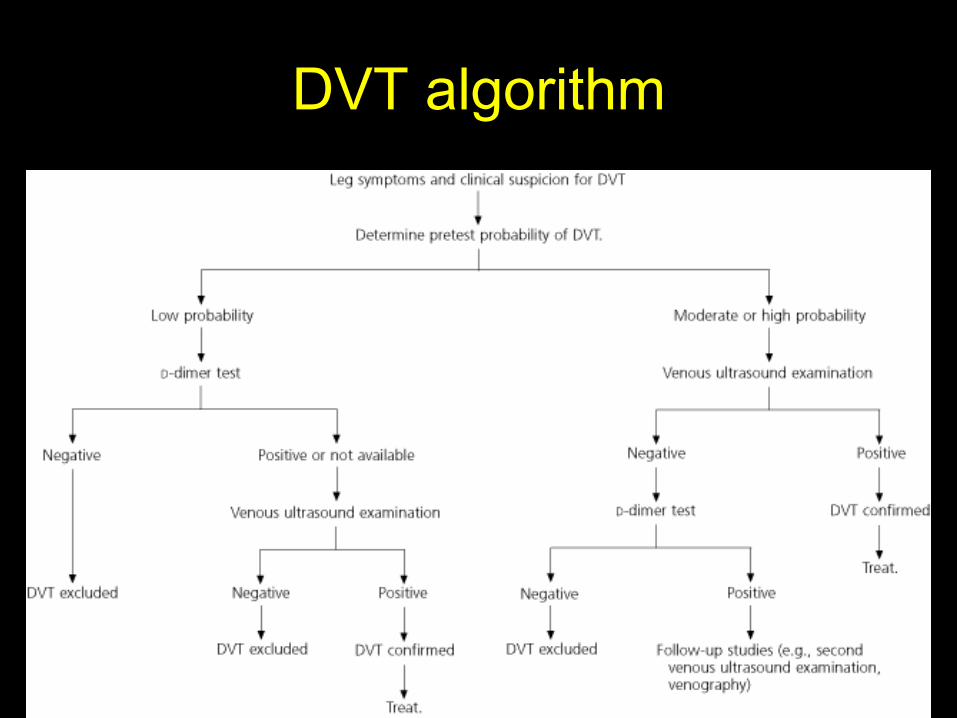
DVT algorithm
Take Home Message
• EUS
– Can tell you the presence or absence of
proximal DVT
– Can’t tell you
• the presence or absence of distal DVT
• the cause of the pain if the US is normal
• Two points compression approach
• Look for complete venous compression